
Abstract
Objective:
The study objective was to quantify the movement of hospital bed occupants relative to the bed in typical bed articulations.
Background:
Movement of a patient in bed results in two common adverse events: (a) increase in shear and friction forces between the patient and bed, which are extrinsic pressure ulcer risk factors, and (b) musculoskeletal injuries to nurses, resulting from repositioning patients who have migrated down in bed.
Method:
The study involved 12 participants who lay supine in three hospital beds, which were articulated to common positions. Body movement relative to the bed was quantified with the use of motion capture. Cumulative movement, net displacement, and torso compression (shoulder to trochanter distance) were calculated for different bed types and bed movements.
Results:
Bed design and bed movement had a significant effect on most of the dependent variables. Bed design (e.g., type) influenced cumulative movement by up to 115%, net displacement by up to 70%, and torso compression by about 20%. Bed movement (e.g., knee elevation) reduced cumulative migration by up to 35%.
Conclusion:
The quantification of patient migration provides a metric for evaluating the interaction between body and bed surfaces. Overall, the measures were sensitive to design changes in bed frames, bed articulations, and mattress inflation.
Application:
Documentation of the cumulative movement, net displacement, and torso compression provides hospital bed designers quantifiable measures for reducing migration and potentially shear and friction forces when designing bed frames, bed articulations, and mattresses. Optimization of these metrics may ultimately have an impact on patient and caregiver health.
Introduction
In recent years, insurance companies and Medicare have begun to refuse to pay for adverse medical events that are attributed to the stay in the hospital. Two such adverse events, pressure ulcers and skin tears, have continued to plague hospitals and will potentially increase in prevalence, given the propensity toward heavier and older patients. More than 2.5 million pressure ulcers occur in acute care hospitals in the United States annually, with a cost of $2.2 to $3.6 billion (Graves, Birrell, & Whitby, 2005; Staas & Cioschi, 1991; Whittington & Briones, 2004). Although more than 200 risk factors have been identified for the development of pressure ulcers and skin tears, two major risk factors relate to movement of patient in the bed: friction force and shear force (Byrne & Salzberg, 1996).
As the bed is articulated to raise the head-of-bed (HOB) section or position it into a dining chair, the body of the patient will potentially slide in the bed. Sliding down the bed can produce shear force that causes distortion of the skin and underlying structures (Sterner, Lindholm, Berg, & Startk, 2011). Frictional forces between the skin and mattress are also contributors to stress on the soft tissues of the body (Sterner et al., 2011). As a result of these forces, soft tissues are pulled and deformed, and in the extreme cases, skin tears and pressure ulcers develop. Patient weight may also have a large role in the shear and frictional forces, and with the growing tendency toward more obese and morbidly obese patients, prevalence of skin tears and pressure ulcers may increase (Centers for Disease Control [CDC], 2012). In addition, elderly patients who have thin skin are susceptible to skin tears and pressure ulcers.
Patient movement in bed also contributes to negative health outcomes for nurses in hospitals and long-term care facilities. When a person slides down in bed, a nurse or pair of nurses will reposition the patient by pulling the patient toward the HOB. More than 90% of nurses will be required to reposition one patient during their shift (Cornish & Jones, 2007). Estimates of how often patients are repositioned range from 16 to 19 times per week (Lynch & Freund, 2000) to as much as 10 times per shift (Vasihadou et al., 2008). By far, the preferred method to reposition patients is manually in teams of two with 95% of nurses adopting this method (Engst, Chhokar, Miller, Tate, & Yassi, 2005). The high frequency of manual patient repositioning translates to pain and suffering for nurses, accounting for 27% to 48% of all low-back injuries (Harber et al., 1985; Knibbe & Frielle, 1996; Leighton & Reilly, 1995; Randall, Pories, Pearson, & Drake, 2009) and odds ratios (ORs) between 1.5 and 3.6 (Kjellberg, Lagerström, & Hagberg, 2004; Pompeii, Lipscomb, Schoenfisch, & Dement, 2009; Smedley, Egger, Cooper, & Coggon, 1995). Repositioning has been identified as a leading cause of low-back injuries, being one of the top three riskiest nursing tasks (Hignett, 1996; Kjellberg et al., 2004; Nelson & Baptiste, 2006; Smedley, Inskip, Buckle, Cooper, & Coggon, 2005; Vasihadou, Karvountzis, Soumilas, Roumeliotis, & Theodosopoulou, 2008; Yip, 2001).
Biomechanical analyses confirm that repositioning is detrimental to the spine, with estimates of high peak compression forces ranging from 4,200 N to 13,230 N, as compared with assisting in and out of bed, which produced 4,000 N to 8,900 N (de Looze et al., 1994; Jang et al., 2007; Marras, Davis, Kirking, & Bertsche, 1999; Winkelmolen, Landeweerd, & Drost, 1994). High shear loads were also observed during repositioning tasks, exceeding 1,200 N (Jang et al., 2007; Marras et al., 1999). Others have reported slightly lower compression (2,610 N to 3,180 N) and shear (350 N to 385 N) forces for repositioning (Skotte, Essendrop, Hansen, & Schibye, 2002; Skotte & Fallentin, 2008). Ultimately, manual repositioning of patients results in large spine loads that exceed the maximum recommended compression (3,400 N) and shear (1,000 N) tolerances (McGill, 1997; Waters, Anderson, Garg & Fine, 1993). As patients continue to become increasingly heavier because of the obesity epidemic in the United States (CDC, 2012), the spine loads on the nurse will only increase, and resulting low-back injuries will likely increase. Older nurses who have significant cumulative trauma from performing nursing duties for a work lifetime may be particularly at risk.
Because movement toward the foot of the bed (FOB) presumably contributes to adverse events for both patients and caregivers, bed designs must reduce the migration movement along with the shear and friction forces between patient and bed. To accomplish this, quantitative methods need to be developed to accurately capture how a person moves in the bed. Movement of the patient can arise from articulation of the different sections of the bed or by the patient’s repositioning himself or herself in the bed. The current study provides a quantitative approach to documenting the actual movement of the patient relative to the bed while the bed is articulated. Metrics were developed to provide potential surrogate indicators for the shear and frictional forces between the bed and patient. These metrics can be used to guide designers to optimize the articulation of the bed and mattress inflations.
Method
Study Approach
A laboratory study was performed to evaluate a methodology for determining how patients move in bed during various bed articulations. Movements of the shoulder, trochanter, and ankle relative to the bed frame were measured during two different bed articulations. These movements were used to determine cumulative movement, net displacement, and torso compression during bed articulation. Given the lack of sensors to adequately measure the shear force between the skin and bed mattress, movement of the body in the bed provides a surrogate measure as a quantification of the summation of sliding movement in the bed (e.g., cumulative movement) and net displacement toward the FOB (e.g., ending position after the articulation). The torso compression provided a measure of how much the participant is “scrunched” as a quantification of the distance between the shoulder and trochanter. Torso compression can cause discomfort for a patient and may lead to skin shear or elevated peak pressures at the shoulder and sacrum, which could increase risk of pressure ulcers. The beds were articulated in standard conditions as the “patient” was in a supine position while acting comatose and not adjusting to the bed until after the articulation was completed.
Participants
A total of 12 participants (6 males and 6 females) volunteered to participate in the study. All participants read and signed a consent form approved by the University of Cincinnati’s Institutional Review Board. The participants were recruited into the study on the basis of six weight-height classifications: (a) tall–average weight, (b) tall–overweight, (c) average height–average weight, (d) average height–overweight, (e) short–average weight, and (f) short–overweight. The height categories were defined by below the 25th percentile (males <171 cm, females <157 cm), 26th to 75th percentile (males >171 cm and <180 cm, females >157 cm and <166 cm), and above the 76th percentile (males >180 cm, females >166 cm) for males and females, and overweight was based on the body mass index of normal weight (<25 kg/cm2) and overweight (between 25 kg/cm2 and 30 kg/cm2). Summary of the anthropometric measurements is in Table 1.
Summary of the Anthropometric Measurements
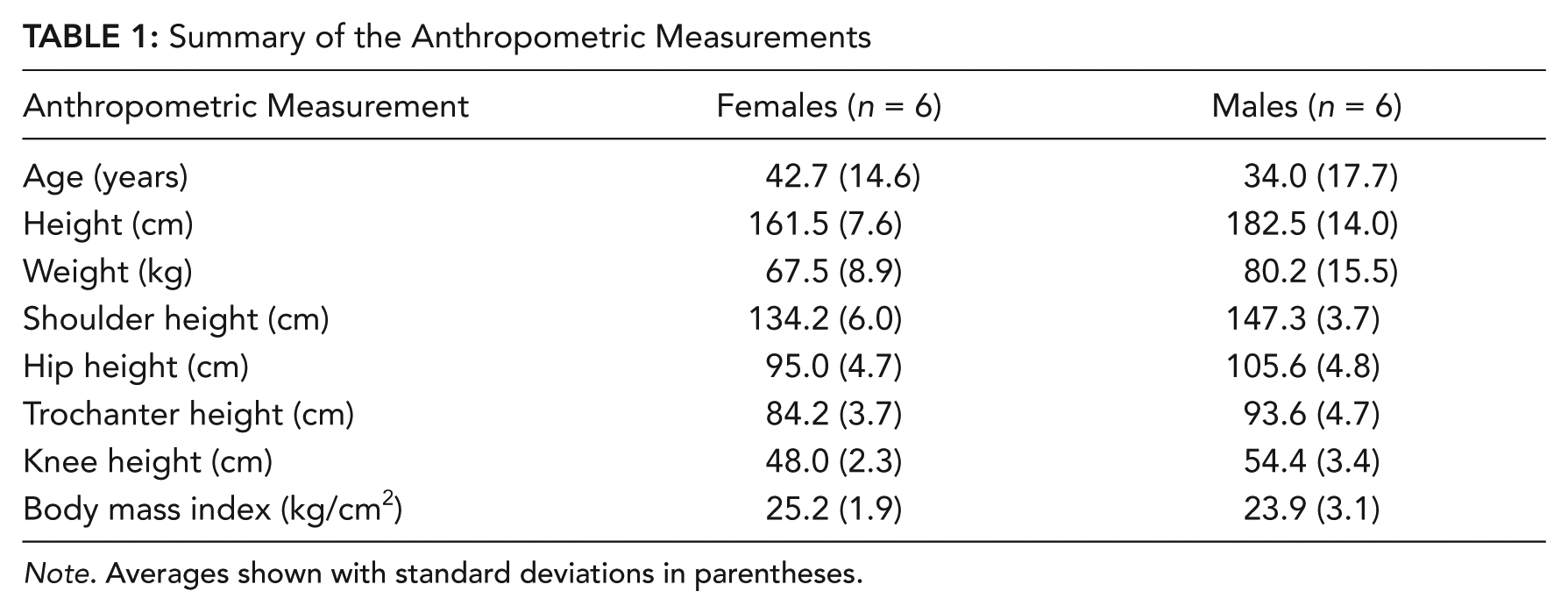
Note. Averages shown with standard deviations in parentheses.
Motion-Capture System
A seven-camera, passive optical motion-capture system (MotionAnalysis, Santa Rosa, CA) quantified the instantaneous 3-dimensional position of seven markers on the body, six markers on the bed frame, and three markers on the surface of the mattress at a sampling rate of 10 Hz. All data were collected, digitized, and analyzed with the use of Cortex software. The body markers were positioned on bony landmarks according to standardized locating procedures for the following body locations of the left side of the body: (a) temple of the head (zygomatic bone approximately 2.5 cm lateral from the midline of the eye), (b) shoulder (on the acromion), (c) elbow (on the lateral epicondyle), (d) hip (on the top of the iliac crest), (e) trochanter (at the center of the greater trochanter), (f) knee (on the lateral femoral epicondyle), and (g) ankle (on the lateral malleolus of the fibula). The bed markers were positioned on the following points of the beds: (a) end of the articulating head section, (b) head of the nonarticulating portion of the frame, (c) pivot point between the seat section and head section, (d) pivot point between seat section and thigh section, (e) pivot between the thigh and foot section, (f) foot of the nonarticulating portion of the frame, (g) surface of mattress in thigh area, (h) surface of mattress in trochanter position, and (i) surface of mattress on head section near shoulder. See Figure 1 for marker position on participant and bed. The markers were 1.3 cm in diameter and attached to the bony landmark with hypoallergenic double-sided adhesive circular washers.

An example of the marker locations for a participant positioned in the bed.
Study Design
The independent variables were bed type, mattress pressure, and knee elevation. Three different bed types were evaluated: Bed 1 was an extended-care bed with a powered air mattress 18 cm thick, Bed 2 was a medical-surgical bed with a powered air mattress 22 cm thick, and Bed 3 was a critical-care bed with a powered air mattress 28 cm thick. For all beds, the frame on which the mattress was placed was comprised of a head, seat, thigh, and foot section. Mattress pressure refers to the air pressure within the mattress with two levels: normal and maximum inflation. Maximum inflation was tested only for Bed 2 and Bed 3, as Bed 1 did not have this option for the mattress. In the normal pressure condition, pressure was adjusted on the basis of patient weight, whereas with maximum inflation, the mattress was filled to a high pressure level (predetermined by manufacturer). Knee elevation was either on or off. The knee elevation was based on the bed articulation of the thigh and foot sections of the bed. For the on condition, the knee raised as the thigh section rotated upward about a pivot between the seat and thigh sections, and the foot section rotated downward about a pivot between the thigh and foot sections (see Figure 2a). For the off condition, the thigh and foot section remained flat throughout the entire articulation (see Figure 2b). Five repetitions were completed for all trials except maximum inflation, for which only two repetitions were completed. The difference in number of repetitions was to limit the time the participant was involved in the study.
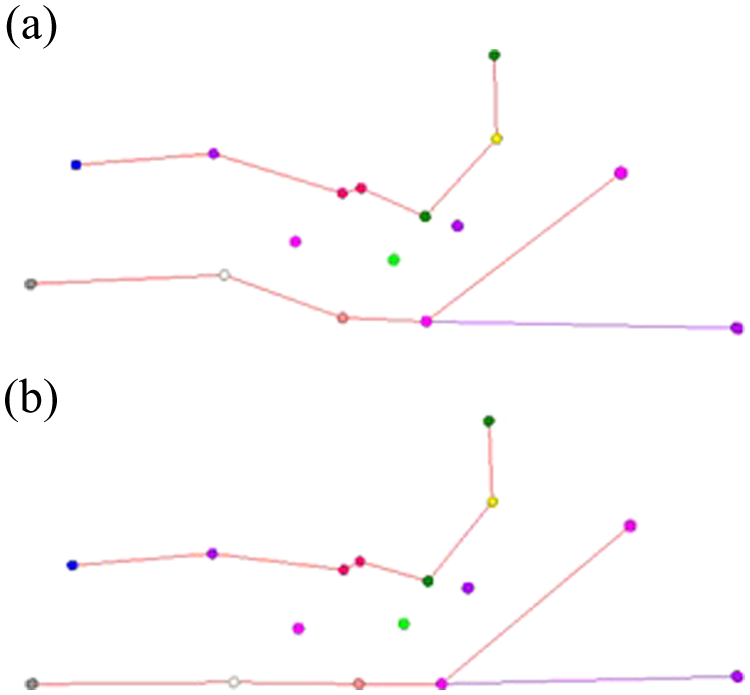
Digitized markers providing a visual of the knee elevation conditions: (a) knee elevation on and (b) knee elevation off.
The dependent variables consisted of net displacement, cumulative movement, and torso compression. For each trial, the instantaneous position of the shoulder, trochanter, and ankle were calculated relative to the head, seat, and foot sections of the bed, respectively. We computed cumulative movement by taking the sum of the absolute value of the incremental changes of the relative position for each targeted body marker (e.g., shoulder, trochanter, and ankle), thus estimating the total movement up and down in the bed (e.g., accounting for positive and negative movement). We calculated the net displacement by comparing the starting position of the targeted body marker with the ending position, quantifying how much movement there was toward the FOB. Positive values represented movement toward the HOB, whereas negative values indicated a movement down toward the FOB. The measurement of torso compression (e.g., scrunching) was developed to identify how much a participant was “balled up” during the articulation. The torso compression was defined as the maximum change in the distance between the shoulder and trochanter markers across the course of a trial.
Procedure
Before each trial, the participant’s trochanter was aligned with markings on the bed, designated by the manufacturer as the proper position of a patient. Two types of articulations were tested: flat to a 45° HOB angle then back to flat (referred to as “0-45-0”) and 30° HOB to dining chair position then back to 30° HOB (referred to as “30-chair-30”). Figure 2 shows the markers for Bed 1 in the 45° position with knee elevation on and off. Each articulation was tested with five replications with the participant being repositioned after each trial. The length of each articulation was approximately 1 min for the single 0-45-0 trials and 1.5 min for the single 30-chair-30 trials. After each trial was started and the peak position (e.g., 45° or chair) was reached, the articulation was immediately reversed until the final position was reached. For Beds 2 and 3, the 30-chair-30 bed articulation was also tested with five replications (see Figure 3 for markers of chair position). The trials were completed in random order for each bed (blocked). Beds were completed in random order across the 12 participants with a counterbalanced method.
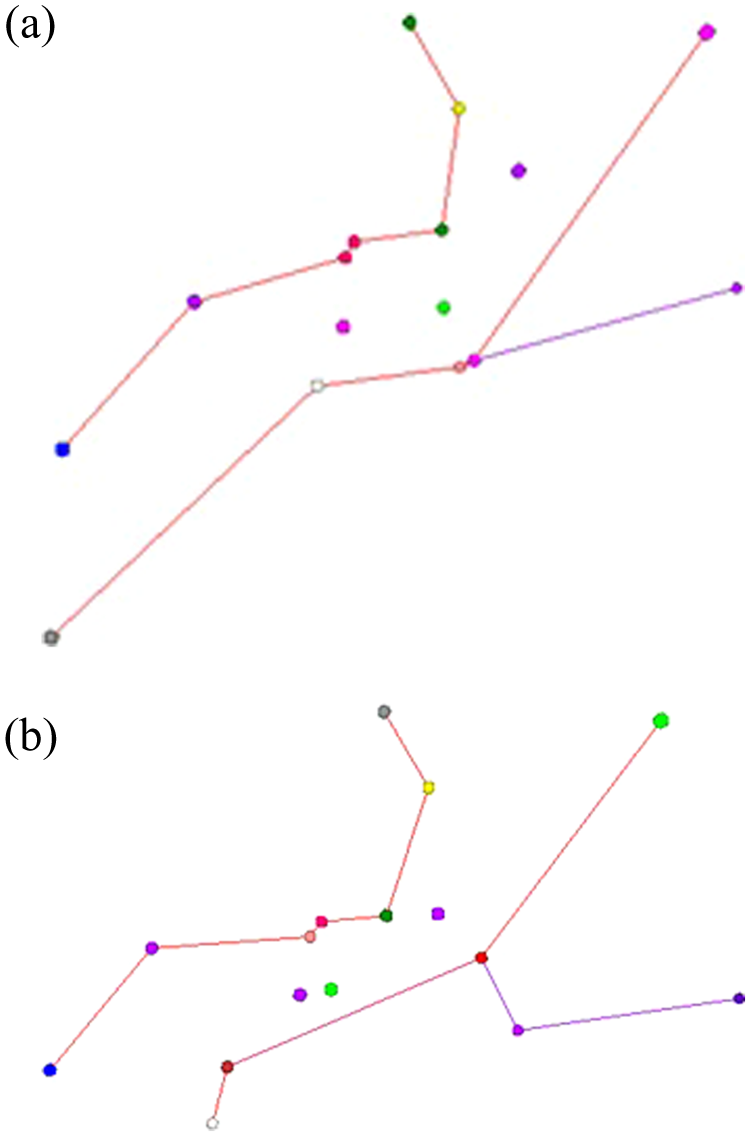
Digitized markers providing visual of the dining chair position for 30-chair-30 bed condition for (a) Bed 2 and (b) Bed 3.
Statistical Analyses
Because Bed 1 had limited functions, such as no dining chair and maximum inflate, analyses for the 0-45-0 conditions with and without knee elevation were analyzed for all three beds, whereas the maximum inflation and 30-chair-30 conditions were analyzed only for Bed 2 and Bed 3. A repeated-measures ANOVA was completed on each dependent variable to identify whether there were significant effects of bed type and knee elevation. A simpler ANOVA was completed to analyze mattress inflation that included bed type and included only the first two trials of the regular inflation and the two trials of maximum inflation (both had knee elevation on). Additional analyses were completed to compare dependent variables for the dining chair articulations for Bed 2 and Bed 3. Descriptive statistics (means and standard deviations) were computed for all of the outcome variables. Post hoc analyses in the form of Tukey standardized honest difference were conducted whereby significant effects were identified to determine the source of the differences between conditions.
Results
Raising HOB (0-45-0) Articulation
Overall, the three beds performed slightly differently in the simple raise-the-HOB articulation. The cumulative movement for the shoulder, trochanter, and ankle were all significantly affected by the bed type and knee elevation (p < .0001). No statistically significant interactions were found for any of the cumulative movement outcomes. Figure 4 shows the mean cumulative movement for the interaction between the bed type and knee elevation. The general trend was that Bed 1 had the greatest cumulative movement in the shoulder (approximately 7 cm or 60% more, p < .05), whereas Bed 3 produced more cumulative movement in the trochanter (approximately 15 cm or 115% more, p < .05) and ankle (approximately 12 cm or 100%, p < .05). Knee elevation (e.g., on condition) decreased the cumulative movement of the trochanter by 2 cm to 5 cm (17% to 47%) and ankle by 4 cm to 7 cm (13% to 77%) but increased the cumulative movement in the shoulder by 1 cm to 3 cm (7% to 18%).
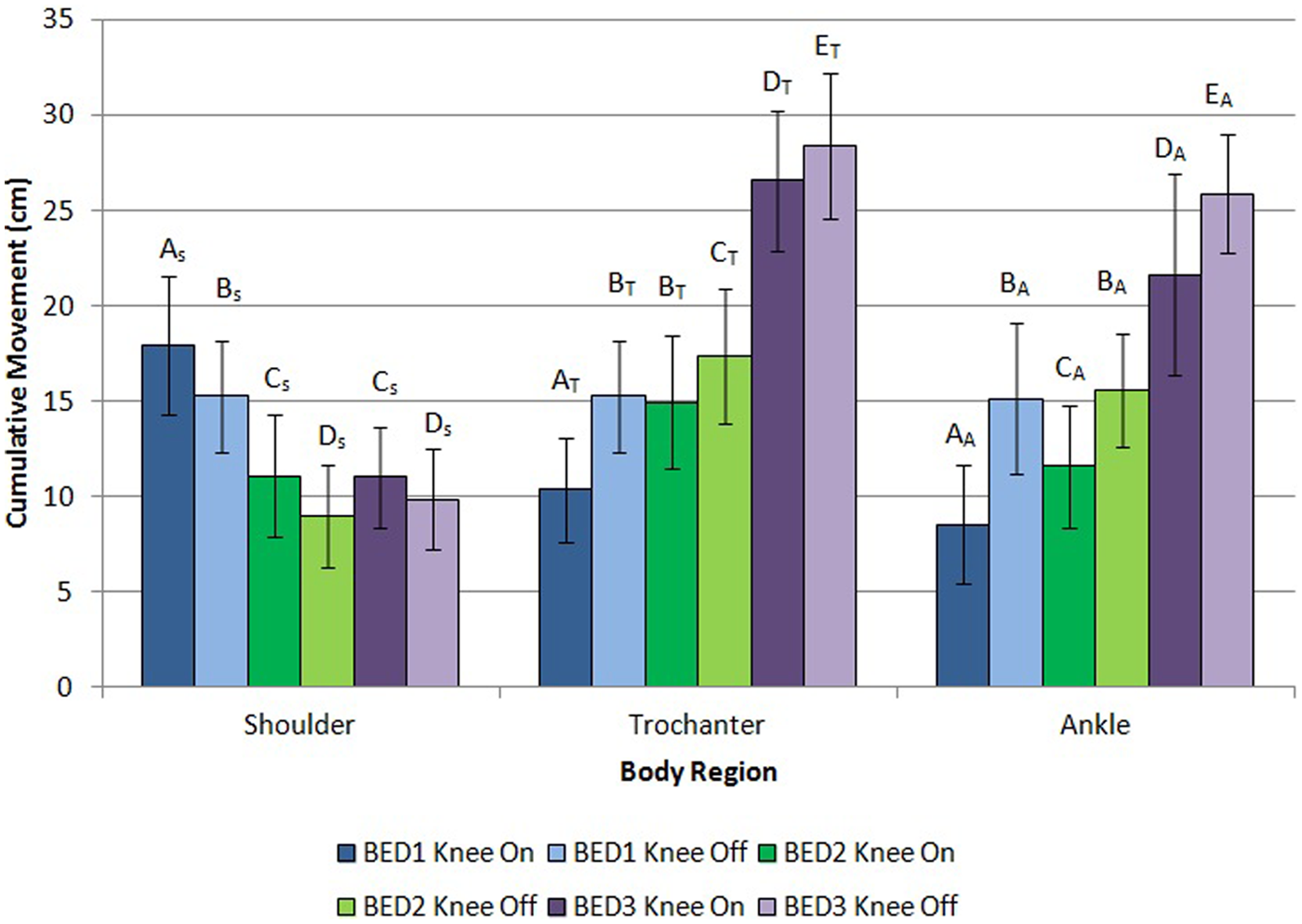
Cumulative movement for shoulder, trochanter, and ankle as a function of bed type and knee elevation (on, knee raises during articulation; off, knee remains flat during entire articulation) during the articulation from flat to 45° to flat (0-45-0). Error bars are standard deviations. Different alpha characters denote significant differences.
The net displacement was significantly (p < .05) affected by bed type but not by the knee movement (Figure 5). In a single articulation, the participant slid down the bed by nearly 2 cm for Bed 1 and Bed 2 in the shoulder and ankle but slightly less in the trochanter (nearly 1.5 cm). Net displacements for Bed 1 and Bed 2 at the shoulder, trochanter, and ankle were very similar and were not statistically different (p > .05). In all body regions, net displacement for Bed 3 was significantly greater than for Bed 1 and Bed 2, with mean net displacements being 35%, 72%, and 70% greater for the shoulder, trochanter, and ankle, respectively. For all of the beds, movement at the end of the articulation was toward the FOB. No interactions were found to be significant for net displacement variables.
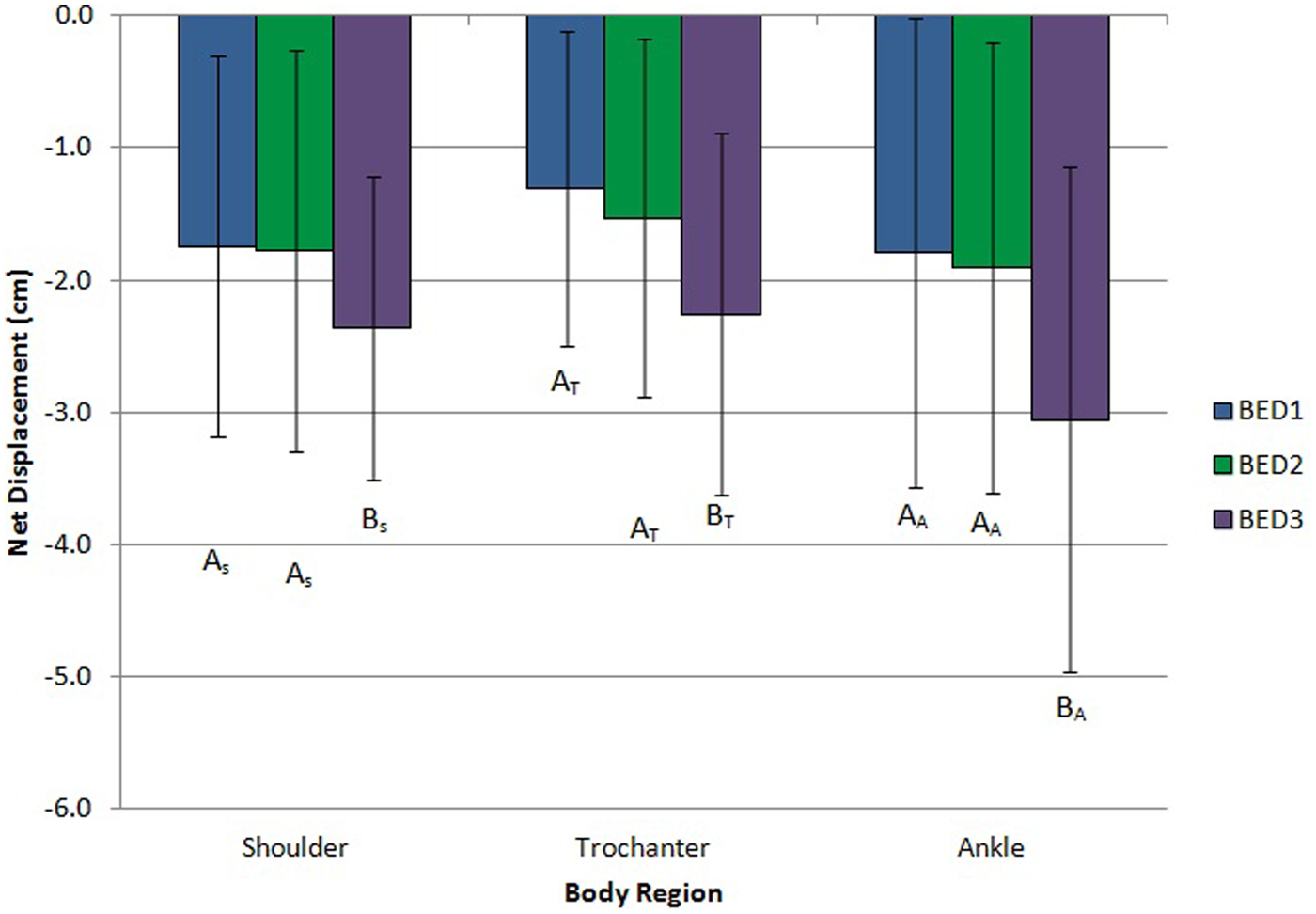
Net displacement for shoulder, trochanter, and ankle as a function of bed type during the articulation from flat to 45° to flat (0-45-0). Error bars are standard deviations. Different alpha characters denote significant differences.
In Figure 6, a different trend was measured for the torso compression whereby Bed 1 had the largest values, Bed 3 had the smallest, and Bed 2 was in the middle (p < .05). Torso compression was approximately 20% less in Bed 3 than in Bed 2 and 11% less in Bed 2 than in Bed 1. In general, the distance between the shoulder and trochanter was shortened by a distance ranging from 5.5 cm to 7 cm and represents significant torso compression. Again, no statistically significant interactions were found for torso compression.
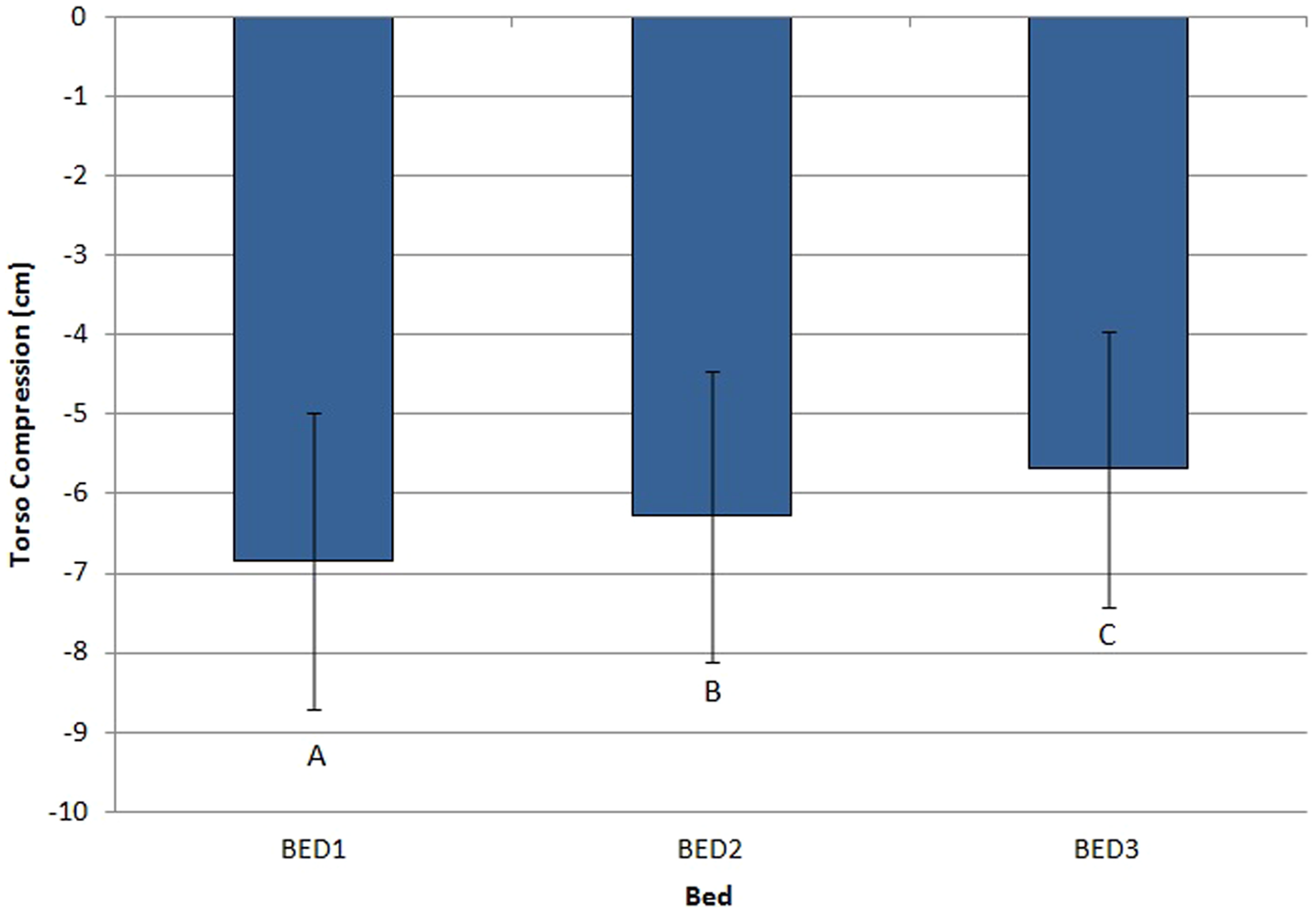
Torso compression as a function of bed type during the articulation from flat to 45° to flat (0-45-0). Error bars are standard deviations. Different alpha characters denote significant differences.
Raising HOB Articulation With Maximum Inflate of Mattress for Bed 2 and Bed 3
Increased mattress pressure produced approximately 1 cm more of shoulder net displacement and a 13% to 17% (2- to 3-cm) increase in the cumulative movement in the shoulder, trochanter, and ankle (significant at p < .002). The mattress inflation effect was not dependent on the bed type (p > .05).
Dining Chair (30-Chair-30) Articulation for Bed 2 and Bed 3
Figure 7 shows that Bed 3 had significantly (p < .001) more cumulative sliding in the shoulder (11 cm greater or 68%) and trochanter (13 cm greater or 108%) as compared with Bed 2. Bed 3 also had significantly (p < .001) more net displacement in the trochanter (more than 1 cm greater or 40%) than Bed 2. For the dining chair articulation, motion was not estimated for the ankle because the angle of the foot section in the dining chair position of Bed 3 was close enough to vertical that the ankle routinely left contact with the bed. As a result, Bed 2 and Bed 3 could not be compared for net displacement and cumulative movement at the ankle. Although net displacement and cumulative sliding were lower in Bed 2 than Bed 3, torso compression was greatest for Bed 2, with almost 1 cm (approximately 17%) less distance between shoulder and trochanter than Bed 3 (p < .001).
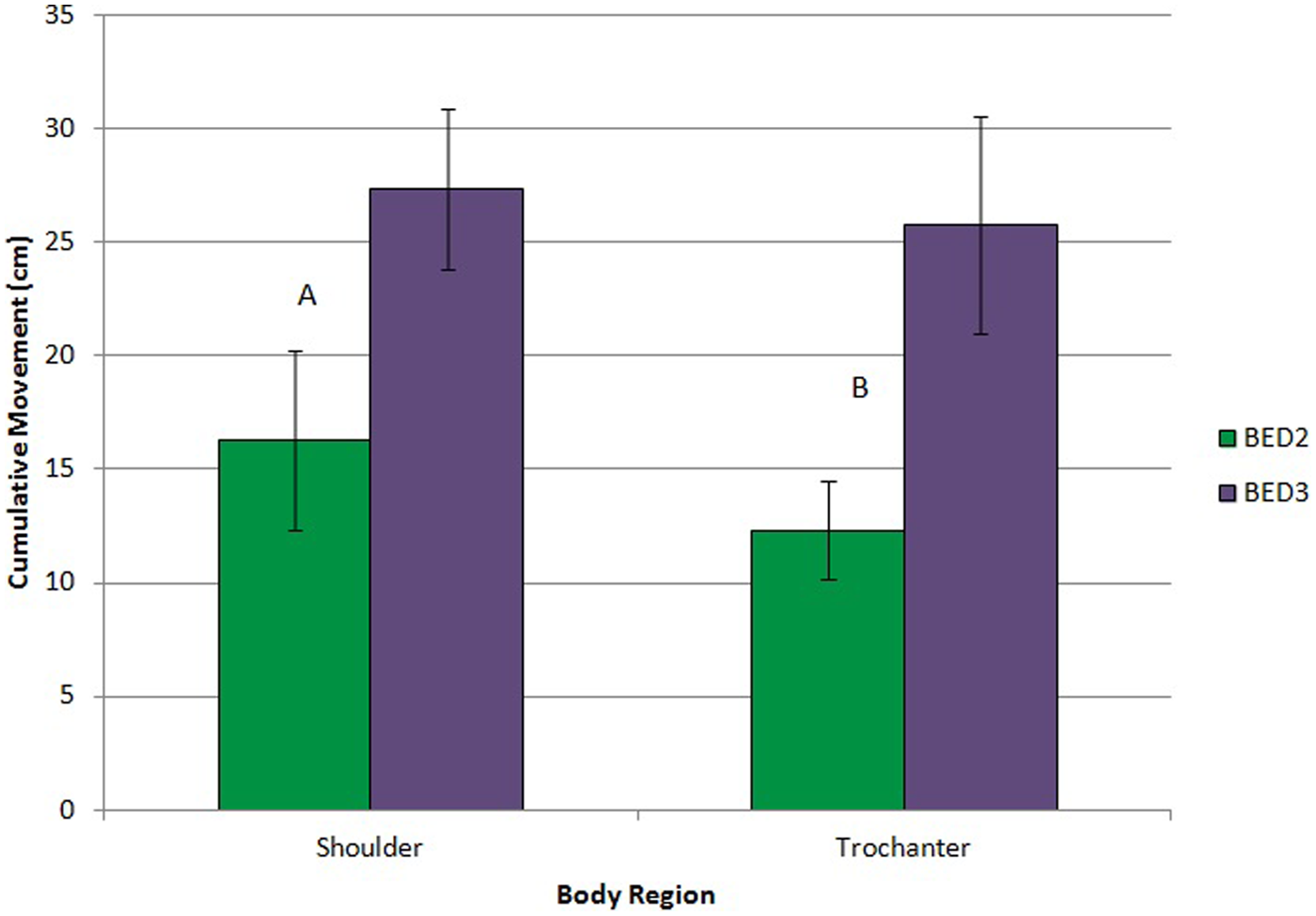
Cumulative movement for shoulder and trochanter as a function of bed type during the articulation from 30° to dining chair to 30° (30-chair-30). Error bars are standard deviations. Different alpha characters denote significant differences.
Discussion
Hospital bed designers have struggled for years to control the migration of the patient as well as shear and friction forces placed on the body of the patient as a bed articulates into different positions. The current study aimed to develop the methodology and metrics that designers can use to evaluate the interaction of the bed frame, mattress surface, and patient body. We developed three primary metrics: (a) net displacement, (b) cumulative movement, and (c) torso compression. Net displacement captures the final migration of the body for the shoulder, trochanter, and ankle. Cumulative movement provides a measure of the entire movement of the body regions throughout the articulation. Torso compression provides an indication of the “scrunching” pressure on the body as a measure of the distance between the shoulder and trochanter. These metrics provide potential surrogate measurements for friction and shear forces between the patient and the bed or for how frequently a caregiver will be required to reposition a patient up in the bed.
We selected three bed designs along with different mattress pressures and knee elevation articulations to demonstrate how different bed design components affect the metrics. The first metric, net displacement, produced a consistent trend, with Bed 3 producing the greatest migration toward the FOB for all three body regions. However, for all the beds, the “patient” moved approximately 2 cm down in the bed in one 0-45-0 articulation and 3 cm to 4 cm down in the bed for 30-chair-30. Small deviations were also quantified between the specific body regions (e.g., shoulder vs. ankle vs. trochanter), potentially resulting from minor differences in individual body postures and movement relative to specific bed sections. In other words, a given body region moves relative to a given bed section and thus may have different relative migrations. The mattress may also have influenced the movement of the participant, as all three bed mattresses contained air bladders. The surface of the air mattress may shift depending on how the air within the mattress is distributed.
To explore the influence of the mattress compliance, we placed three markers on the mattress in the head section, thigh section, and foot section of the bed. Movement of the mattress accounted for 10% to 20% of the net displacement values and 15% to 50% of the cumulative movement. The mattress movement had the largest impact on the cumulative movement of the trochanter (40% to 52%). Obviously, the mattress pressure and potential design (e.g., bladder construction) has a role in how the participant migrated down the bed. The movement trends of the body relative to the mattress were observed to be similar to those of the body relative to the bed, although on a smaller scale. Since caregivers likely key on the visual position of the person relative to the bed, these trends were reported.
Cumulative movement, the second metric, provided a slightly different picture for the beds whereby Bed 1 had the most sliding movement in the shoulders and Bed 3 produced the most in the trochanter and ankle. Bed design and mattress composition certainly affected the movements, with significant differences for bed type, maximum inflation, and knee elevation. Bed 3 resulted in double the amount of cumulative movement of Bed 1 or Bed 2 during the 0-45-0 conditions.
It is interesting that Bed 3 generally produced the most net displacement and cumulative movement but resulted in the least cumulative movement in the shoulder region. A clue to explaining this conflicting result may lie in the finding that Bed 3 has the lowest torso compression for all of the bed types. It is possible that when the HOB section is raised to 45° on Bed 3, the shoulder is not scrunched and remains close to the starting position, whereas the lower body slides farther to the FOB. When Bed 3 is lowered back to flat, the shoulder must then slide down to meet the lower half of the body, which would explain why the Bed 3 net displacement of the shoulder is comparable to the net displacement of the trochanter and ankle. For Bed 1 and Bed 2, when the HOB is raised to 45°, the shoulder slides up the bed, which causes the torso to experience more scrunching. As Bed 1 and Bed 2 are lowered back to flat, the shoulder slides back down to meet the lower half of the body. The additional shoulder movement up and then back down could explain why Bed 1 and Bed 2 resulted in greater cumulative shoulder movement and greater torso compression than did Bed 3.
By having lower torso compression (third metric) during the articulations, Bed 3 appears to cause less “balling up” of the participant and may have lower forces between the bed and his or her body. So although there is more sliding movement and ultimate displacement for Bed 3, the user may feel less tension during the articulation. Lower torso compression values may also be an indication of the shear and friction forces, since to push shoulders toward the trochanter, force has to be applied by the bed to the upper body (e.g., pushed toward the FOB) and lower body (e.g., pushed to the HOB). Whether the torso compression is linked to the feeling of balling up or forces between bed and body, smaller values would likely be linked to better comfort. The smaller torso compression values in combination with greater cumulative movement for Bed 3 may indicate that the user may move more freely over the mattress with less friction and shear forces.
Other Considerations
There are several other considerations that should be kept in mind when interpreting the study results. First, although the quantification method provides documentation of the bony structures, soft tissues may move differently as a result of increased friction and shear forces. As a result, some error could occur in understanding the movement of soft tissues—adipose tissue and skin. In obese and morbidly obese individuals, it is possible that the soft tissues would behave differently as compared with the motion of bony landmarks observed in this study. The individual’s excess weight could cause increased compression of the tissues, potentially creating more shear and friction forces between the individual and bed surface, and thus movement during the articulations could be altered. Although in this study we did explore effects on overweight individuals, we did not include obese or morbidly obese individuals. Some evidence of the impact was found by comparing overweight with normal-weight individuals. Over-weight individuals had larger net displacements (by approximately 0.5 cm for all body regions), whereas the cumulative movement was lower for the shoulder (approximately 3 cm) but higher for trochanter and ankle (approximately 1 cm and 1.2 cm, respectively). The torso compression was also greater for overweight participants (approximately 0.5 cm).
Second, although single bed articulations provide useful information about the patient’s movement in bed, in a traditional health care setting, a patient would likely experience many articulations throughout the day, potentially magnifying the results. For each bed, a separate set of three consecutive articulations was completed without repositioning the participant in an attempt to give some indication of how a patient would move across a longer duration, when several articulations would occur. As seen in Figure 8, the majority of sliding movement toward the FOB occurred during the first articulation (Bed 1, approximately 85%; Bed 2, 75%; Bed 3, 61%). However, in almost every case, downward sliding continued (to a lesser extent) during the following two articulations. With continued sliding, it is likely that a nurse would reposition the patient toward the HOB, and then the sliding downward cycle would be repeated as the bed continues to be articulated. This cycle would potentially increase the risk of shear and friction forces to the patient and the risk of a patient-handling injury to the nurse.
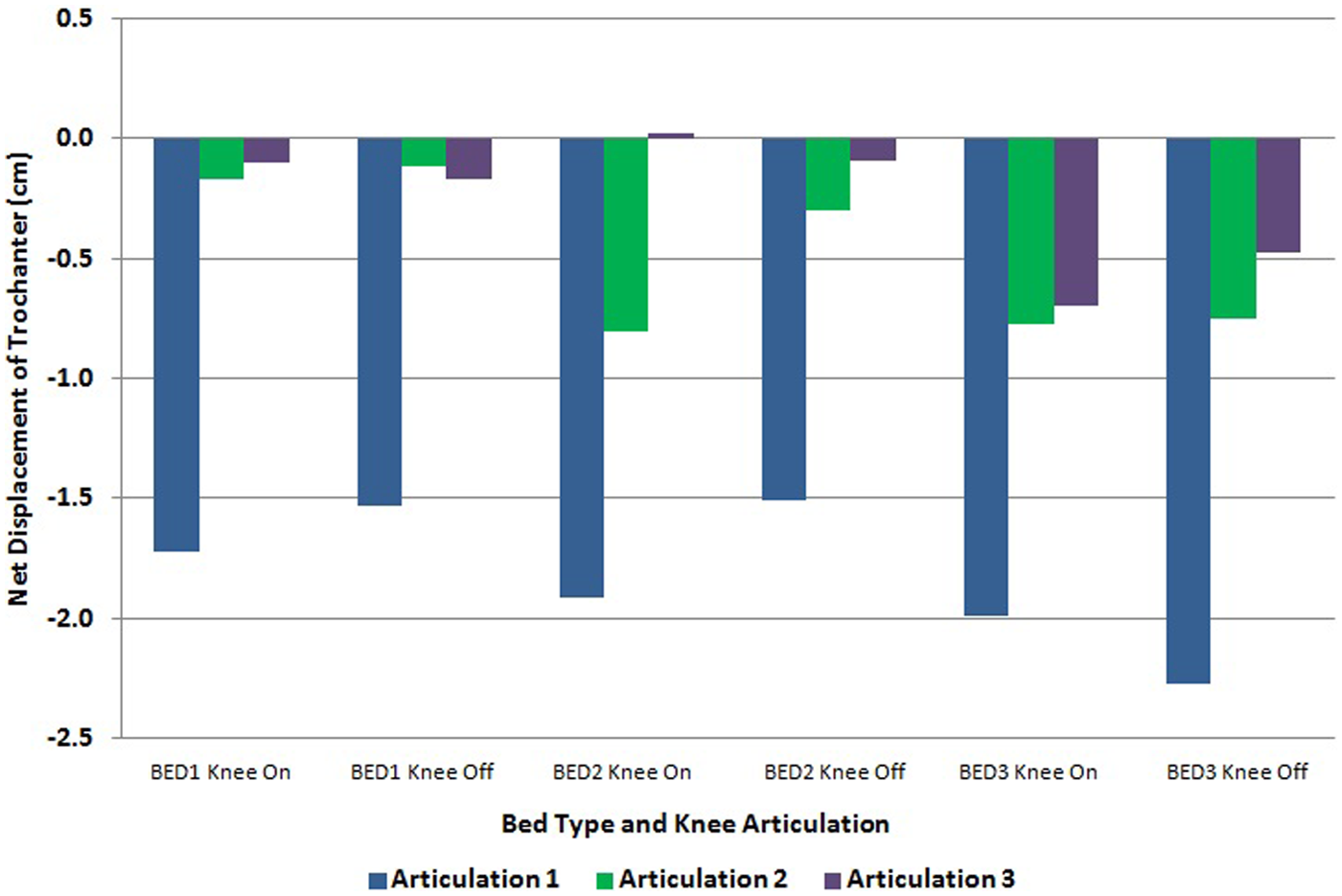
Net displacement of trochanter for three repeated articulations without repositioning of the participant between articulations (averaged across all the participants).
Third, only a limited number of bed articulation positions were investigated in this study. Although they were representative of normal positions patients would use in a health care setting, patients would likely be placed in numerous other positions throughout the day. In addition to a limited number of test positions, a limited participant population was tested with respect to ability and situational awareness. All participants were asked to act “comatose” during the trials and not readjust until after the end of the trial. Although some patients would truly be in a comatose condition, others would likely be able to readjust their position themselves or “squirm” to relieve the pressure points. How well patients naturally readjust themselves to a position that minimizes the friction and shear forces and whether the readjustments contribute to the migration are unknown.
Fourth, although the participant numbers were limited, the current study evaluated individuals of a wide variety of heights and weights to provide a preliminary understanding of how individual characteristics affect how a person moves in bed. Although the data presented focused on overall group results, there were trends with respect to differences between gender and weight groups (as noted earlier). When comparing males with females, we found that males had more net displacement in the shoulders (approximately 0.5 cm) and ankles (approximately 0.4 cm) but less cumulative movement in shoulder and trochanter (approximately 0.5 cm). Males also had greater torso compression than females (approximately 0.9 cm). These findings indicate that hospital designers will need to consider that a “one-size-fits all” approach may not be effective.
Conclusion
The current study provided a framework for hospital bed designers to quantitatively assess the migration of patients as a bed is articulated. Net displacement, cumulative movement, and torso compression offer three distinct metrics of patient migration. On the basis of the three metrics, all three hospital beds demonstrated strengths and weaknesses, suggesting that there may be opportunity for refinement in future designs. Hospital bed designers can now use these quantitative metrics to design and evaluate frame articulation and mattress designs. The optimal design will minimize net displacement and cumulative movement while not translating the lack of movement to torso compression. An optimal hospital bed would reduce the likelihood that the patient will migrate to the FOB, requiring a nurse to move him or her and increasing risk of a low-back injury. The optimal bed design would also likely reduce the risk to the patient for pressure ulcers and skin tears. However, minimizing all three metrics may not be achievable since these metrics may actually be competing constraints (e.g., less cumulative movement may result in more torso compression). Additionally, researchers will need to better delineate the complex relationship between the three metrics and potential adverse events. Ultimately, these metrics may lead to bed designs that will reduce the epidemic levels of pressure ulcers in patients and patient-handling injuries in nurses.
Key Points
Patient migration in hospital beds can lead to risk factors for adverse events, such as pressure ulcers, skin tears, and caregiver injury during patient repositioning.
Three metrics were developed to quantitatively evaluate patient migration in hospital beds of varying designs during different bed articulations.
All bed designs had strengths and weaknesses, with the metrics showing sensitivity to design of bed frames, articulations, and mattress inflation.
The developed metrics provide quantitative measures for designers to use to optimize bed design, which may ultimately affect patient and caregiver health.
Footnotes
Acknowledgements
Funding was provided by Hill-Rom, Inc., for participant incentives. Neal Wiggermann and Rachel Williamson work for Hill-Rom, and Rachel owns stock in the company. Neither is involved in the direct sale of any Hill-Rom product; they are involved only from an engineering aspect, so there will be no direct financial benefit to them from this study.
Susan E. Kotowski is an assistant professor at the University of Cincinnati in the College of Allied Health Sciences. She is also director of the Gait and Movement Analysis Lab. She received her PhD in occupational ergonomics and safety from the University of Cincinnati College of Medicine. She is also a Certified Professional Ergonomist.
Kermit G. Davis is an associate professor at the University of Cincinnati in the College of Medicine, Department of Environmental Health, where he also directs the Low Back Biomechanics and Workplace Stress Laboratory. He received his PhD in occupational ergonomics from The Ohio State University, College of Engineering, Department of Industrial and Systems Engineering. He is a Certified Professional Ergonomist.
Neal Wiggermann is an advanced biomedical ergonomics engineer at Hill-Rom, Inc., where he is also in charge of the ergonomics test laboratory. He received his PhD from the Department of Industrial and Operations Engineering at the University of Michigan.
Rachel Williamson works for Hill-Rom, Inc., where she is the director of Global Surfaces Engineering.