
Abstract
Objective:
This paper systematically reviews the effect of chair backrests and reducing seated hip flexion on low back discomfort (LBD) and trunk muscle activation.
Background:
Prolonged sitting commonly exacerbates low back pain (LBP). Several modifications to seated posture and chair design have been recommended, including using chairs with backrests and chairs that reduce hip flexion.
Method:
Electronic databases were searched by two independent assessors. Part 1 of this review includes 26 studies comparing the effect of sitting with at least two different hip angles. In Part 2, seven studies that compared the effect of sitting with and without a backrest were eligible. Study quality was assessed using the PEDro scale.
Results:
Significant confounding variables and a relatively small number of randomized controlled trials (RCTs) involving people with LBP complicates analysis of the results. There was moderate evidence that chair backrests reduce paraspinal muscle activation, and limited evidence that chair backrests reduce LBD. There was no evidence that chairs involving less hip flexion reduce LBP or LBD, or consistently alter trunk muscle activation. However, participants in several studies subjectively preferred the modified chairs involving less hip flexion.
Conclusion:
The limited evidence to support the use of chairs involving less seated hip flexion, or the effect of a backrest, is consistent with the limited evidence that other isolated chair design features can reduce LBP.
Application:
LBP management is likely to require consideration of several factors in addition to sitting position. Larger RCTs involving people with LBP are required.
Introduction
Low back pain (LBP) is one of the most common musculoskeletal disorders (e.g., Woolf & Pfleger, 2003). Prolonged sitting by itself is not linked to the onset of LBP (Roffey, Wai, Bishop, Kwon, & Dagenais, 2010). However, sitting is commonly reported to increase the symptoms of people with LBP (e.g., Womersley & May, 2006). Consequently, there has been an increasing amount of research investigating sitting posture (e.g., Dankaerts, O’Sullivan, Burnett, & Straker, 2006), and the effect of seating modifications (e.g., Lengsfeld, Konig, Schmelter, & Ziegler, 2007), among people with LBP. Some studies have examined these factors among people with LBP (e.g., O’Sullivan et al., 2006), whereas other studies have examined the onset of low back discomfort (LBD) among pain-free subjects (e.g., Gadge & Innes, 2007).
Using lumbar supports (Williams, Hawley, McKenzie, & Van Wijmen, 1991) or devices (Reinecke, Hazard, & Coleman, 1994) to increase lumbar lordosis have been advocated in the management of LBP for many years. This reflects the fact that both health care professionals (O’Sullivan, O’Sullivan, O’Sullivan, & Dankaerts, 2012) and ergonomic recommendations (Corlett, 2006) favor lordotic sitting postures for the lumbar spine. However, although increasing seated lordosis may reduce LBP in the short term for some individuals (Williams et al., 1991), many patients with LBP already assume lordotic postures that are associated with their symptoms (Dankaerts et al., 2006, O’Sullivan, 2006). Furthermore, lordotic sitting postures are associated with high levels of trunk muscle activation (O’Sullivan, 2006), which may lead to compressive loading, fatigue, and discomfort (Carcone & Keir, 2007; Lander, Korbon, DeGood, & Rowlingson, 1987).
Sitting involves more lumbo-pelvic flexion than standing (Claus, Hides, Moseley, & Hodges, 2009; De Carvalho, Soave, Ross, & Callaghan, 2010; Dunk, Kedgley, Jenkyn, & Callaghan, 2009), due to the greater hip flexion causing posterior pelvic tilt. Sitting postures that maintain lumbar lordosis in sitting are commonly considered advantageous among health care professionals (O’Sullivan, O’Sullivan, et al., 2012; Pynt, Higgs, & Mackay, 2001) and the public (O’Sullivan et al., 2013). Consequently, attempting to reduce seated hip flexion, with a view to maintaining lumbar lordosis, has been proposed (Mandal, 1983). It has been demonstrated that reducing seated hip flexion helps maintain seated lumbar lordosis (Keegan, 1953; Saarni, Nygård, Rimpelä, Nummi, & Kaukiainen, 2007) and that people may prefer to sit with less hip flexion than that usually recommended (Mandal, 1987). However, the effect of reducing hip flexion on trunk muscle activation is unclear with both reduced (e.g., Koskelo, Vuorikari, & Hänninen, 2007) and increased (e.g., Lander et al., 1987) muscle activation reported. In addition, it is unclear how such changes in muscle activation translate into clinically meaningful improvements in LBP. For example, schoolchildren have been shown to prefer chairs involving less hip flexion without such chairs necessarily decreasing pain prevalence or symptoms (Cardon, De Clercq, De Bourdeaudhuij, & Breithecker, 2004; Troussier, 1999).
Another commonly advocated chair modification is the use of a backrest (Carcone & Keir, 2007). Chair backrests have been proposed to promote good spinal posture, while also reducing trunk muscle activation and LBD (Andersson, Jonsson, & Ortengren, 1974; Carcone & Keir, 2007). In addition, using a backrest, especially increasing backrest inclination, has been proposed to reduce intradiscal pressure (Andersson, Ortengren, Nachemson, Elfström, & Broman, 1975). As a result, backrests have become standard in many workplaces. However, it appears that backrests are not always used optimally during common occupational tasks (Vergara & Page, 2000b), and a recent review cast significant doubt on the strength of the relationship between sitting and parameters such as intradiscal pressure (Claus, Hides, Moseley, & Hodges, 2008). Furthermore, although much research has examined the effect of different types of backrest configurations (Ellegast et al., 2012; Groenesteijn et al., 2012), there has been no systematic review on whether using chair backrests actually reduces LBP/LBD, or how they influence trunk muscle activation.
Recent systematic reviews examining factors such as occupational seating have reported mixed results. A systematic review (Driessen et al., 2010) of randomized controlled trials (RCTs) concluded that there was little evidence to support the use of physical ergonomics interventions, including changes in seat design, for LBP or neck pain. In contrast to this, a more recent systematic review (Van Niekerk, Louw, & Hillier, 2012) of seated occupational interventions, which included more varied study designs and examined a broader range of body regions, suggested that there was some evidence of effectiveness. However, many of the included studies in this review (Van Niekerk et al., 2012) were at high risk of bias. Therefore, this systematic review specifically examined the effect of reducing seated hip flexion (Part 1) or providing a chair backrest (Part 2) on trunk muscle activation and/or LBP/LBD.
Method
Overview
The Cochrane and MEDLINE databases were initially searched, revealing no systematic reviews investigating the effect of using a chair backrest or hip angle on trunk muscle activation and/or LBP/LBD. These reviews were registered on the PROSPERO database (registration numbers CRD42012002343 and CRD42012002378; PROSPERO, 2012), and have been reported in accordance with the PRISMA statement (Moher, Liberati, Tetzlaff, & Altman, 2009).
Search Strategy and Inclusion Criteria
Two assessors (KO, MC) independently searched for the presence of an agreed range of keywords in the following databases; MEDLINE, SPORTDiscus, CINAHL, AMED, Academic Search Complete, and Biomedical Reference Collection. The search strategy used four keyword groups relating to (a) sitting, (b) the low back region, (c) muscle activation or discomfort, and (d) either changing hip angle in sitting (Figure 1) or backrests (Figure 2). The specific keywords for each group are detailed in Figures 1 and 2. The abstract had to contain at least one keyword from each group to be considered for these reviews. The four groups of keywords were combined using “AND.” Articles were limited to those involving humans and published in English, with no year limits applied. Only peer-reviewed journal articles were considered. Conference proceedings were excluded because they are not consistently peer reviewed, and often lack sufficient information to adequately assess methodological quality. After removing duplicates, the titles and abstracts that met these criteria were screened for suitability. If it was unclear whether a study was eligible, full-text articles were retrieved. Studies were included if they compared at least two sitting conditions with different seated hip flexion angles for Part 1, or if they compared sitting with a backrest to at least one other sitting condition without a backrest for Part 2. In both reviews, included studies must have measured either LBP, LBD, or the activation of at least one trunk muscle. Studies had to either report quantitative values for muscle activation, LBD, or LBP, or perform statistical comparisons between the sitting conditions to be eligible for inclusion. Studies involving either pain-free participants or people with LBP were eligible. No minimum follow-up period was required, such that single-session comparisons of sitting conditions were eligible. The reference list of each article was also screened for further relevant articles.
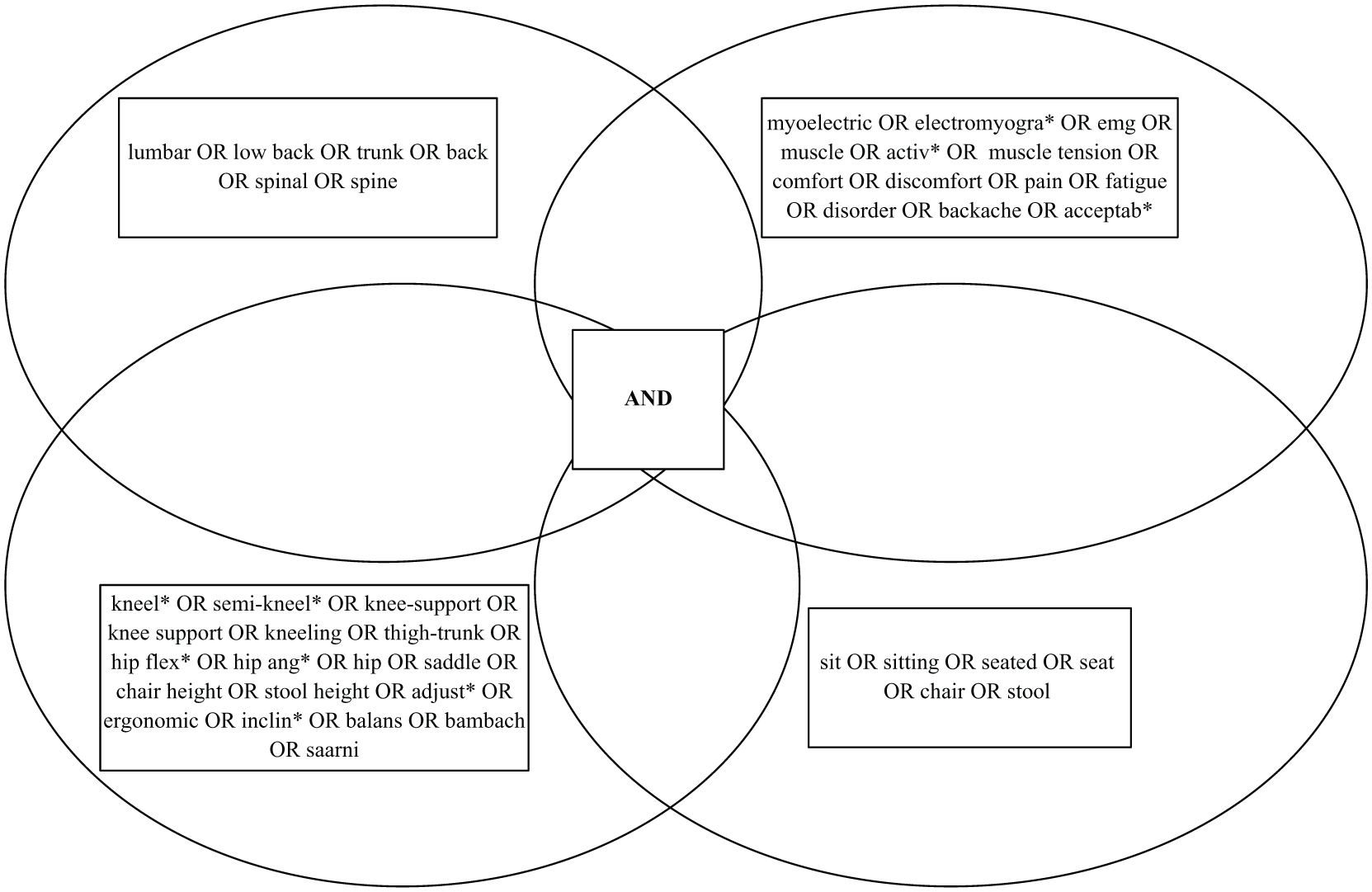
Four keyword groups used in search strategy examining chairs which reduce seated hip flexion.
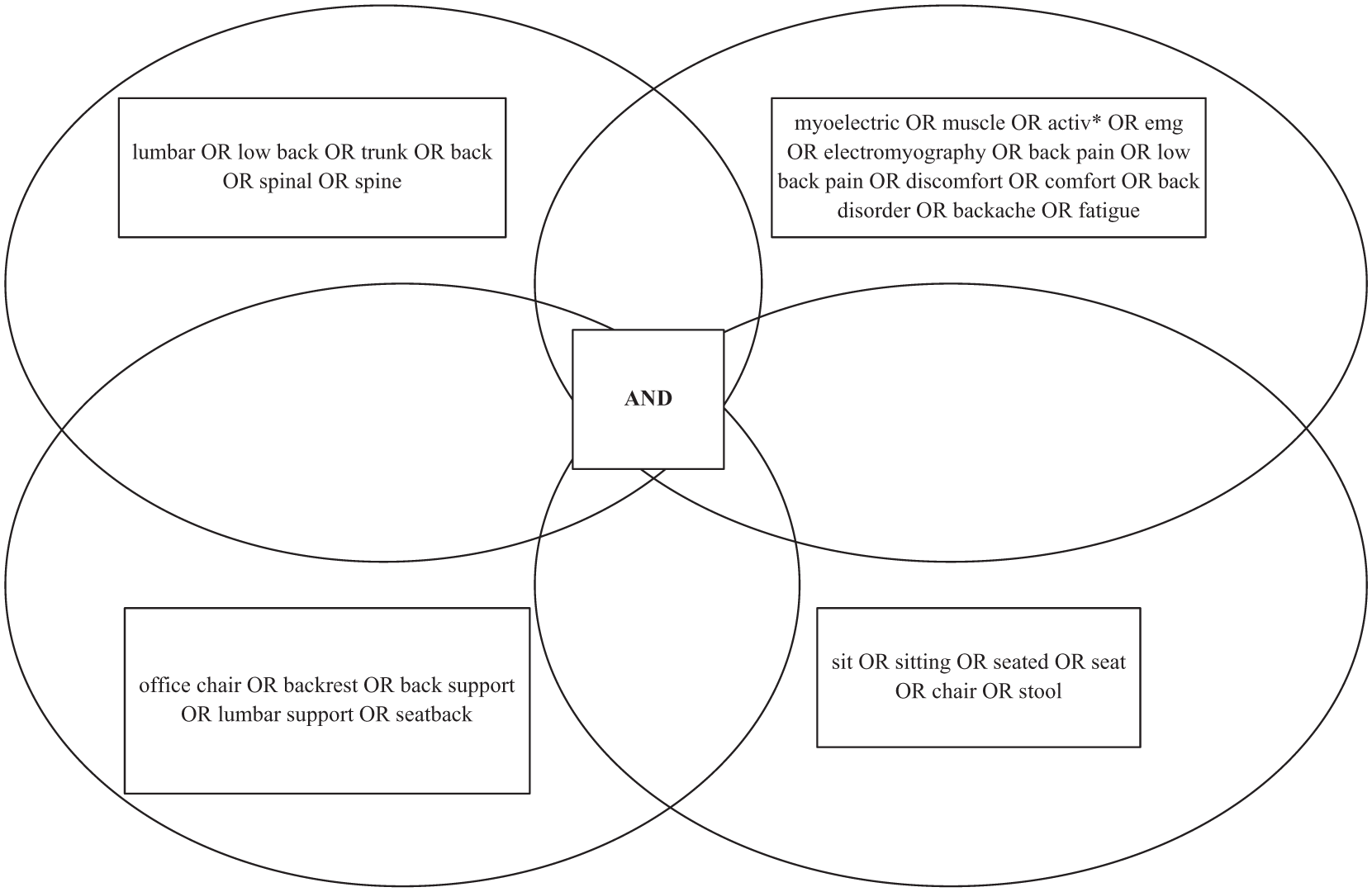
Four keyword groups used in search strategy examining chairs using backrests.
Assessment of Methodological Quality
Methodological quality was rated independently by two assessors (KO, MC) using the Physiotherapy Evidence Database (PEDro) scale (http://www.pedro.org.au). The PEDro scale is a reliable (Maher, Sherrington, Herbert, Moseley, & Elkins, 2003) and valid (de Morton, 2009) method of assessing trial quality, based on the Delphi criteria (Verhagen et al., 1998). This scale investigates the internal validity of a study and contains 11 criteria, 10 of which are scored. When it was unclear whether a study met the PEDro criteria, the original authors were emailed for clarity, to enhance the accuracy and rigor of the reviews. Regarding the “baseline comparability” criterion, studies must typically describe a measure of disorder severity. Although this cannot be applied among pain-free participants, points for this criterion were automatically awarded for crossover design studies, despite there being no measure of “severity” available, in line with a recent systematic review (O’Sullivan, O’Keeffe, O’Sullivan, O’Sullivan, & Dankaerts, 2012). Regarding the “point estimates and variability” criterion, points were awarded if such data were provided for either muscle activation and/or LBP/LBD. In the event of disagreement between the two raters for an individual study, a consensus decision was reached. The quality was classified as “high” (≥6/10), “fair” (4–5/10), or “poor” (<4/10), according to PEDro scores (Ye, Kalichman, Spittle, Dobson, & Bennell, 2011), to aid interpretation of study quality in the event of inconsistent findings. An a priori decision was made to exclude studies rated as “poor,” in line with a recent systematic review (O’Sullivan, O’Keeffe, et al., 2012). In addition, the overall quality of the studies was evaluated under the headings of bias, confounding factors, strength of the results, and clinical applicability, similar to a recent systematic review (O’Sullivan, O’Keeffe, et al., 2012).
Data Extraction and Synthesis
Data regarding each study were extracted and cross-checked by two assessors (KO, MC). This included data on (a) sample size, (b) participant sex, (c) participant age, (d) sitting conditions, (e) study protocol, (f) muscles analyzed, (g) pain or discomfort measurement, (h) inclusion/exclusion criteria, and (i) the main results (Table 1). Significant differences in the outcome measures used for both muscle activation and LBP/LBD, as well as the comparison sitting conditions used, did not allow for pooled analysis of the data.
Description of Studies Included in the Review

Note. Age expressed as mean unless otherwise stated. BB, biceps brachii; BF, biceps femoris; BPD, body part discomfort scale; CES, cervical erector spinae; C1/4/6, cervical vertebral levels; DE, deltoid; emg, electromyography; EO, external oblique; F, female; GA, gastrocnemius; GCR, general comfort rating scale; IO, internal oblique; LBD, low back discomfort; LBP, low back pain; LD, latissimus dorsi; LES, lumbar erector spinae; L1/2/3/4/5, lumbar vertebral levels; M, male; N/A, not assessed; NF, neck flexor (Sternocleidomastoid); NS, not stated; RA, rectus abdominis; RCT, randomized controlled trial; RF, rectus femoris; SOL, soleus; ST, superior trapezius; TA, tibialis anterior; TES, thoracic erector spinae; T4/5/6/9/10, thoracic vertebral levels; VAS, visual analogue scale.
Results
Study 1: Effect of Reducing Seated Hip Flexion
Identification of studies
The results of the search strategy are outlined in Figure 3. The electronic search returned 1,080 potentially relevant studies, which was reduced to 849 after removing duplicates. After screening these titles and abstracts, 19 potentially relevant studies were identified. After reviewing the full-text of these studies, 14 studies met the inclusion and exclusion criteria. Searching the reference lists of these articles added another 15 studies. Three studies were rated as “poor” quality on the PEDro scale and were excluded. Therefore, the final number of articles included in this review was 26 (Table 1). Five studies were clinical trials with a follow-up period. The remaining 21 studies were crossover studies, or used similar designs such as a single system repeated baseline study (Gadge & Innes, 2007) and studies comparing “old” and “new” seating designs (Aagaard-Hansen & Storr-Paulsen, 1995). In all, 21 studies examined LBP or LBD, 11 examined trunk muscle activation, with 6 studies examining both (Table 1). Only 7 studies included participants with LBP.
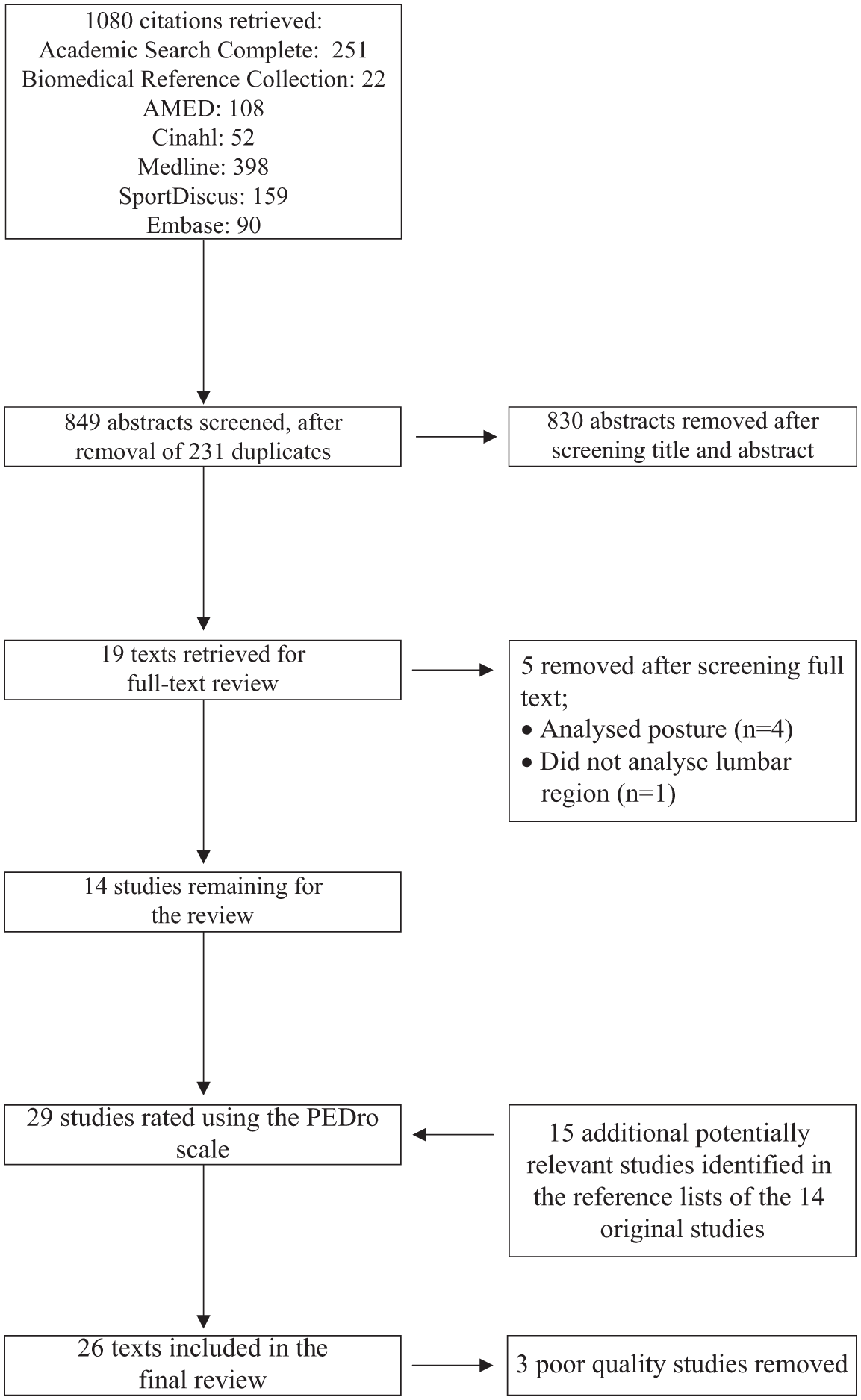
Flow chart indicating study selection procedure for chairs which reduce seated hip flexion.
Crossover studies
Eight studies compared forward inclined kneeler chairs to at least one office chair with a flat seat pan (hip angle approximately 90°). Six of these eight studies used the same brand of armless kneeler chair (Balans kneeler chair), whereas three of them compared sitting to a flat seat pan that also had a backrest. Lander et al. (1987) reported that cervical erector spinae (CES) and lumbar erector spinae (LES) activation were significantly higher on the Balans kneeler chair than on an armless seat with a flat seat pan and backrest. In addition, the chair with the flat seat pan and backrest was reported as more comfortable on a 0 to 10 visual analogue scale (VAS). Bennett, Gillis, Portney, Romanow, and Sanchez (1989) reported no significant differences in LES activation while sitting on two armless seats with a flat seat pan and a backrest with the Balans kneeler chair. Cram and Vinitzky (1995) compared paraspinal activation (CES, thoracic erector spinae [TES], LES) on three different chairs: the Balans kneeler chair, a chair with a flat seat pan and backrest, and using the Back Up, which is a chair accessory providing pelvic support. LES activation was again significantly higher on the Balans chair than on the flat seat pan with a backrest. However, this study did not specify if the chairs featured an armrest or whether participants were able to lean on the desk while writing for 10 minutes, which could confound results. Two other studies analyzed only discomfort and not muscle activation. Bendix, Jensen, and Bendix (1988) reported no statistically significant differences between sitting on a Balans chair and an armless tiltable chair. Similarly, this study did not state if participants leaned on the desk during the tasks. Bishu, Hallbeck, Riley, and Stentz (1991) reported that the Balans kneeler chair was less comfortable (measured by a discomfort questionnaire rated 0–5) than two other conventional sitting conditions with a flat seat pan. Although one of the conventional chairs in this study had armrests, it was not stated if participants were instructed to use them. Finally, and in contrast to the other five studies examining the same kneeler chair, Soderberg, Blanco, Cosentino, and Kurdelmeier (1986) reported that a kneeler chair at two different forward inclinations was preferred to a conventional chair with a flat seat pan. Furthermore, paraspinal activation (CES, TES, LES) was significantly lower on the kneeler chair. The conventional chair had armrests but participants could not use them and rested their wrists lightly on the computer keyboard to assist standardization. The other two studies of kneeler chairs used different brands, and combined the kneeler chair with sloping desks. Marschall, Harrington, and Steele (1995) compared a traditional workstation with a kneeler chair combined with sloping desks among schoolchildren. Neither chair featured armrests. Latissimus dorsi (LD) activity was significantly decreased on the kneeler chair and participants preferred this workstation. Finally, Bridger (1988) reported greater comfort when sitting for 20 minutes using a kneeler chair compared to a conventional office chair, especially when the kneeler chair was combined with a sloping desk. This study did not state whether chairs featured armrests which could confound results.
Thirteen studies examined the effect of varying seat pan inclination, or seat height, or both on trunk muscle activation, LBP or LBD. Bendix and Biering-Sørensen (1983) reported no difference in discomfort on four different seats—a flat seat pan and three forward inclined seats whose height increased in line with increasing forward seat pan inclination. Bendix (1984) reported no significant difference in acceptability between three seats of varying inclination and mobility whose participants were instructed to rest their elbows on the table. In contrast, Bendix, Jessen, and Winkel (1986) reported significantly greater acceptability for an armless, forward inclined higher seat compared to an armless, low, backward inclined seat. Bendix, Winkel, and Jessen (1985) observed that LES activation was not significantly different between three armless seats of varying inclination and mobility in a two-part study. Although the tiltable chair was significantly more acceptable in a short laboratory study, this difference was not statistically significant in the longer field study. Winkel and Bendix (1986) reported no difference in LES or calf muscle activation between a low, backward inclined seat, and two higher seats that were forward inclined or freely tiltable. This study did not state whether chairs featured armrests or whether participants were instructed to lean on the table while completing the tasks. Another study by the same research group (Jensen & Bendix, 1992) also reported no significant difference in preference between three armless seats of varying inclination and mobility. Subjects in this study were instructed to sit as they pleased. Naqvi (1994) assessed discomfort every five minutes during 15 minutes of sitting on four different armless seats—a flat seat pan and three forward inclined seats. LBD increased significantly with increasing forward inclination beyond 5° and after 10 minutes of sitting. However, because both neck discomfort and overall discomfort were significantly lower at 10° than 5°, they recommended different angles of inclination for each spinal region. Van der Heide, Otten, van Eykern, and Hadders-Algra (2003) demonstrated that mean TES activation was significantly increased with a backward inclined seat pan, whereas LES onset activation was significantly delayed with a backward inclined seat pan. The authors did not specify if the seats featured armrests. Inclining the seat pan forward to varying degrees by sitting on three different wedges (10°, 20°, and 30°) was investigated in one study (Wu, Miyamoto, & Noro, 1998). In this series of three experiments, pain-free participants rated the use of a wedge positively in terms of the stability it provided, and the way they perceived it placed load on their spine and pelvis. However, the level of discomfort (rated on a 5-point scale) was increased with wedges which reduced hip flexion by 20° or 30°, whereas the level of discomfort using a 10° wedge was no better than using no wedge. Similarly, it was not stated if the seat featured armrests. Yu, Keyserling, and Chaffin (1988) modified seven sitting variables including seat height and seat inclination. They reported significantly less overall and localized body discomfort with a lower seat than with a higher seat. There were no significant differences during seat forward inclination, and no significant differences in LES activation or LES fatigue with varying seat height or seat inclination.
The final three crossover studies simply controlled the degree of hip flexion in sitting. Hardage, Gildersleeve, and Rugh (1983) compared TES and LES activation while sitting with and without a backrest at three different hip angles. Despite some evidence of an interaction between hip angle and the presence of a backrest in sitting, there was no significant difference in paraspinal muscle activation between seats with different hip flexion angles. Gadge and Innes (2007) compared discomfort levels between an armless conventional chair with a flat seat pan and a Bambach armless saddle seat. It was not stated if participants were instructed to rest their elbows or whether the assessor monitored use of the table. Both LBD and overall body discomfort (OBD) increased more slowly on the Bambach seat, however discomfort was higher for the hips and buttocks when sitting on the Bambach seat. Michel and Helander (1994) reported that people with LBP reported significantly less LBD using an armless sit–stand chair than a conventional armless chair. However, pain-free participants reported less LBD on the conventional chair. Overall, buttock discomfort was significantly greater in the sit–stand chair.
Intervention studies
Five studies examined the effect of these chairs over a period of time greater than one day. An RCT by Wang et al. (2008) compared the effect of a curved seat pan to both (a) a flat seat pan and (b) a placebo group receiving only miscellaneous items (footrest, small table-top storage box, side table, lamp, and reading glasses). Although both armless “intervention” chairs reduced back and hip pain over a four month period, the curved seat pan did not actually reduce back and hip pain as much as the flat seat pan. The final four studies examined the effect of incorporating these seats into an ergonomically designed workstation including a sloping desk. All used schoolchildren as the population of interest. All seats were armless. An RCT by Linton, Hellsing, Halme, and Åkerstedt (1994) compared the effect of a traditional workstation with an ergonomic workstation over a six month period. The intervention group reported a significant reduction in the incidence of LBP on a dichotomous (yes/no) scale. Comfort was also rated higher among the intervention group. However, the actual frequency of LBP, headache, neck pain, and overall musculoskeletal pain was not significantly different between groups at follow-up. The reduction in LBP incidence occurred without any change in actual spinal posture. Another RCT (Aagaard-Hansen & Storr-Paulsen, 1995) examined the effect of changing seat height and inclination, desk slope, or both. Combining a forward inclined, higher seat, and adjustable sloping desk was subjectively preferred overall to (a) a traditional flat seat pan and desk and (b) a flat seat pan and an adjustable sloping desk. However, there was no significant difference in the frequency of reported LBP. A nonrandomized clinical trial (Koskelo et al., 2007) compared a forward inclined seat combined with an adjustable sloped desk to standard furniture. Reducing seated hip flexion decreased trapezius and LES muscle activation, and was associated with better satisfaction scores at 2-year follow-up. The incidence of neck and shoulder pain decreased in both groups, especially in the group who sat in less hip flexion. However, there was no significant difference in the incidence of LBP or headache between the groups at follow-up. Finally, another nonrandomized clinical trial (Saarni et al., 2009) compared the use of saddle-type chairs and adjustable desks to a control group still using their usual chairs and desks. The ergonomic workstations were preferred in the first year, but not in the second year. In addition, no significant differences in seated posture or trunk mobility were observed between the two groups.
In conclusion, the use of chairs that reduce seated hip flexion appears to be associated with increased paraspinal muscle activation and/or increased discomfort. However, this is likely to be partly explained by other differences between the sitting conditions studied. This includes the use of a backrest or a sloping desk, which appear to ameliorate the negatives of forward inclined chairs (Bridger, 1988; Marschall et al., 1995; Soderberg et al., 1986) to the extent that reducing seated hip flexion in itself does not influence LBP, LBD, or trunk muscle activation.
Study 2: Effect of Providing a Backrest
Identification of studies
The results of the search strategy are outlined in Figure 4. The electronic search returned 386 potentially relevant papers, which was reduced to 275 after removing duplicates. After screening these titles and abstracts, 16 potentially relevant articles were identified. After reviewing these 16 full-text articles, only 7 of them met the inclusion and exclusion criteria. Searching the reference lists of these articles did not add any further articles. All seven eligible studies were rated as “fair” to “high” quality and were included in the review. Therefore, the final number of articles included in this review was seven. All seven studies were crossover design studies, with one (Kingma & van Dieen, 2009) involving testing on two separate days. All seven studies examined trunk muscle activation, whereas two of them (Gregory, Dunk, & Callaghan, 2006; Lander et al., 1987) also examined LBD. Only one study (Cram & Vinitzky, 1995) included both pain-free participants and people with LBP, with the remainder examining only pain-free participants.
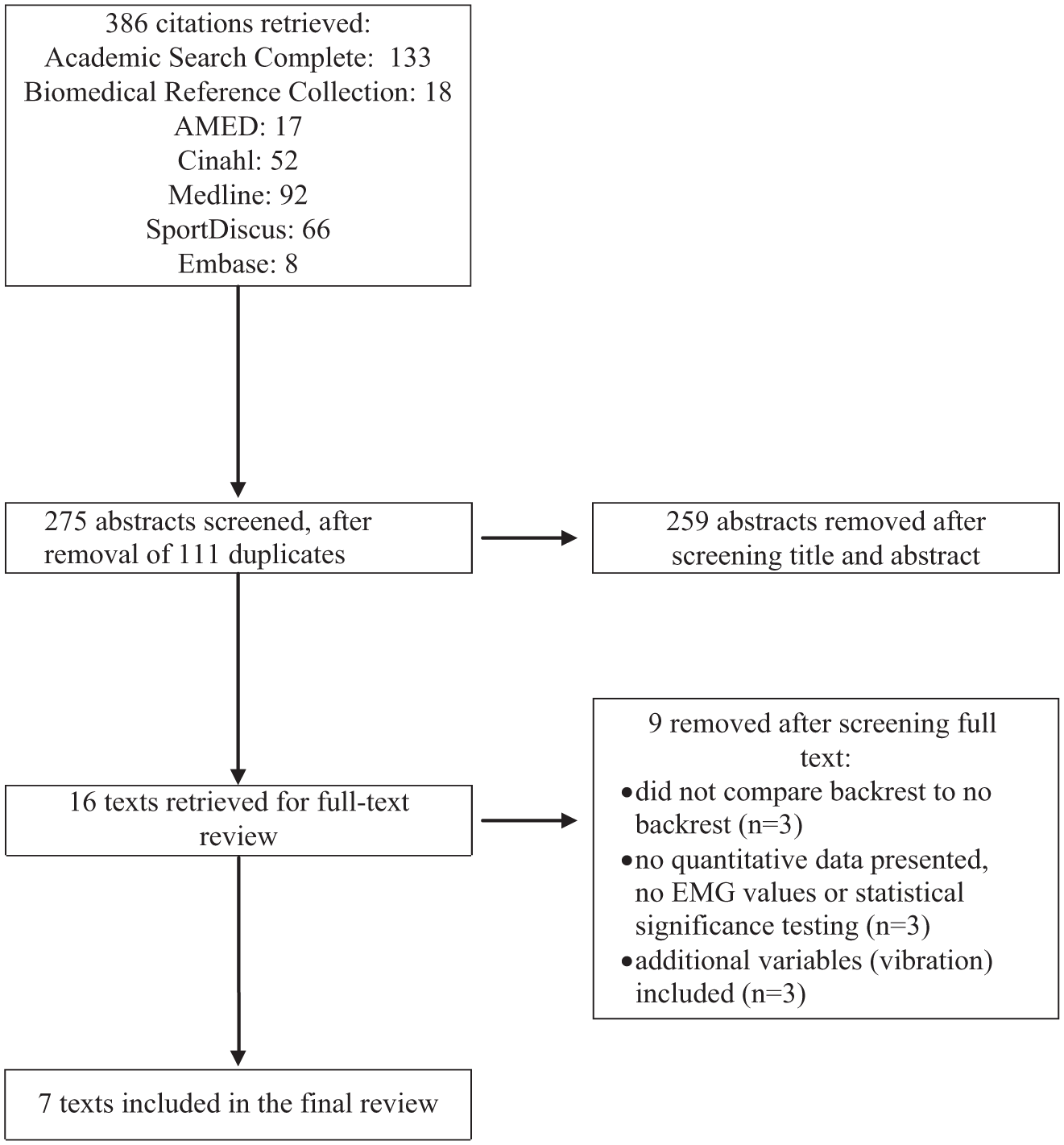
Flow chart indicating study selection procedure for chairs using backrests.
Description of results
Four studies have already been described in Part 1 of this review, as they met the inclusion criteria for both systematic reviews (Bennett et al., 1989; Cram & Vinitzky, 1995; Hardage et al., 1983; Lander et al., 1987).
Two studies compared sitting with a backrest to sitting on an exercise ball. In one study (Gregory et al., 2006), the chair with a backrest involved significantly lower activation of TES, and significantly lower LBD and OBD. In the other study comparing to sitting on an exercise ball (Kingma & van Dieen, 2009), using a backrest was associated with lower LES mean activation, lower variation in activation of LES, and lower LES muscle fatigue. This study did not assess discomfort, although they reported that participants experienced less LBD and upper back discomfort when using the backrest during pilot testing. Finally, using a ball-shaped backrest at three different heights was compared to not using a backrest (Yoo et al., 2008). The effect of the backrest varied according to its height, suggesting that it may be clinically relevant to choose backrest height based on an individual’s height (spinal length) and region(s) of discomfort. It is important to acknowledge that the results of these two studies could be related to differences in mobility between the chairs, and not just the presence of a backrest, although a recent systematic review suggests dynamic sitting has little effect on LBP/LBD (O’Sullivan, O’Keeffe, et al., 2012).
In conclusion, the use of a backrest appears to reduce paraspinal muscle activation according to the height it is positioned at, most commonly the lower lumbar spine. The decrease in paraspinal activation is likely due to external support being provided by the backrest, which spares the muscles from needing to provide active support. This also appears to lead to a decrease in LBD, though the lack of RCTs involving people with LBP limits strong conclusions on this point.
Critical Appraisal
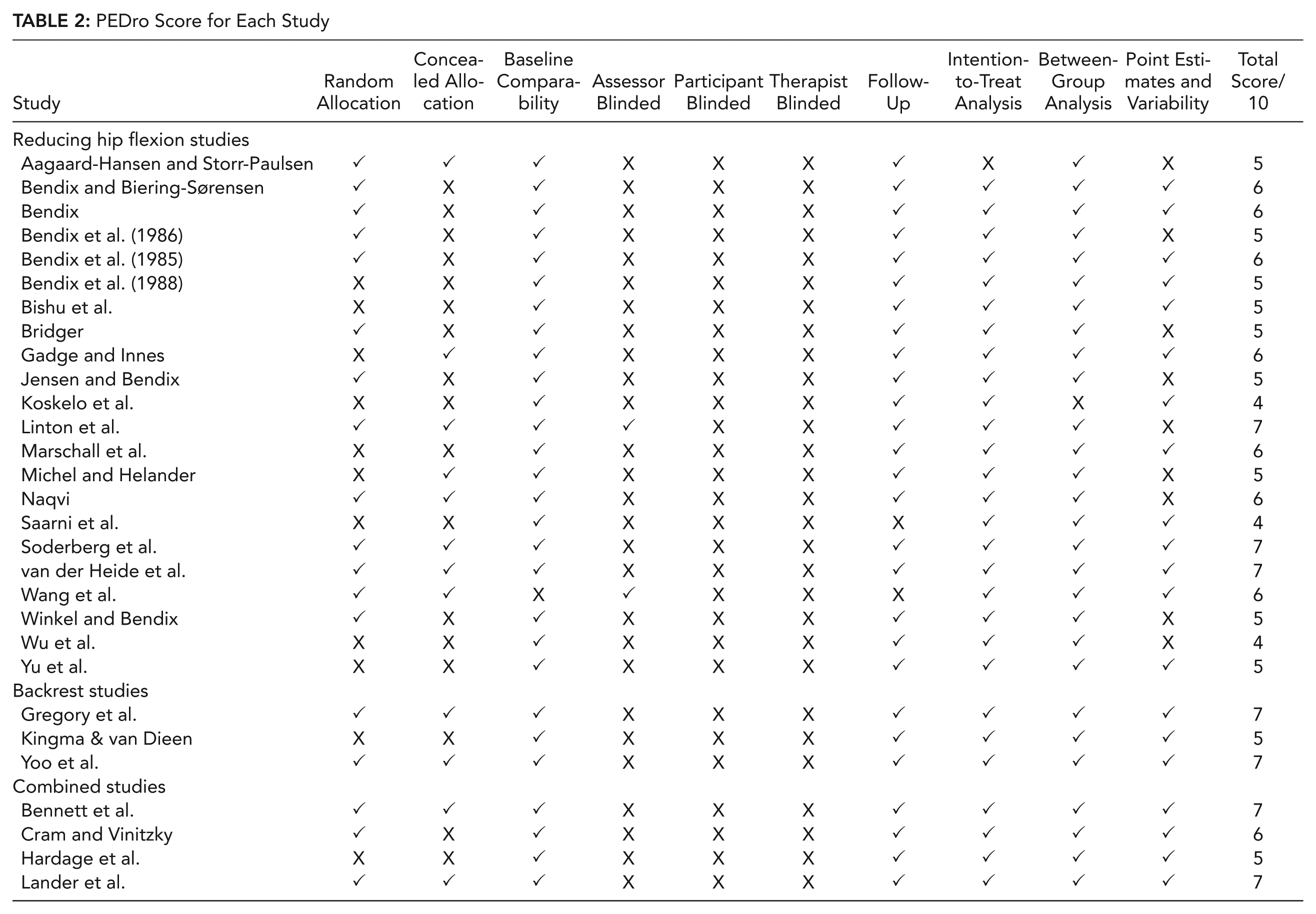
The detailed methodology of each included study is provided in Table 1. Table 2 illustrates that all included studies were rated as fair (4–5/10) to high (≥6–10/10) quality, with all studies except three (Koskelo et al., 2007; Saarni et al., 2009; Wu et al., 1998) scoring in the range of 5–7/10. This section briefly summarizes the key methodological concerns regarding all studies included.
PEDro Score for Each Study
Bias
Randomization was acceptable in most studies, although the precise method of randomization (e.g., computer-generated or by selecting allocation from an opaque envelope) was not always stated. Although several studies allocated participants in a counterbalanced order instead, this is not a major cause for concern in crossover or repeated measures design studies. Concealment of allocation was performed in most, but not all studies. All crossover studies clearly had similar groups at baseline, however one study (Wang et al., 2008) did not demonstrate comparability of groups at baseline. Only two studies reported blinded assessors (Linton et al., 1994; Wang et al., 2008). Blinding of therapists and participants is difficult to achieve in such studies, although some studies (Aagaard-Hansen & Storr-Paulsen, 1995; Wang et al., 2008) used several intervention chairs to partially address participant bias. Limited information was provided about inclusion/exclusion criteria overall, increasing the potential for selection bias. No study mentioned using a random recruitment strategy which decreases the generalizability of results. A range of participant ages and sex were included.
Confounders
Some significant confounding variables were present in several studies. Considering the review on reducing seated hip flexion first, several studies did not control for the presence of a backrest (Koskelo et al., 2007; Saarni et al., 2009) or the height and slope of the desk used (Koskelo et al., 2007; Linton et al., 1994; Saarni et al., 2009) between sitting conditions. Furthermore, despite the fact that changing seat pan inclination alters the pressure on a backrest (Bendix et al., 1985), the vast majority of studies did not investigate if backrest pressure varied between sitting conditions. In some studies, the size of the seat pan (Wang et al., 2008) or the size and inclination of the backrest (Gadge & Innes, 2007) varied considerably between the flat and inclined seats. In some studies, neither the inclination of the intervention seat nor its effect on hip angle was reported, and was not available from the authors when contacted (Aagaard-Hansen & Storr-Paulsen, 1995; Linton et al., 1994). In fact, it was not always clear if the modified chair design would have a major effect on the seated hip flexion angle (Wang et al., 2008).
For the review on chair backrests, it is again clear that several studies did not control for other factors which differed between the sitting conditions (other than the presence of a backrest) and which could affect the findings. This includes comparing to an exercise ball that involved greater movement, and comparing to a kneeler chair that not alone had no backrest, but also involved far less hip flexion. The presence of these confounders reflects the fact that the chair with the backrest was often the control sitting condition in these studies. No study reported any objective method of checking that participants actually used the backrest when sitting in the backrest condition, which could confound the results (Vergara & Page, 2000a).
In both reviews, the duration of sitting exposures, and the use of rest periods between them, varied considerably between studies (Table 1), although these were similar between sitting conditions in all studies that mentioned these details. Similarly, some studies performed testing on separate days to avoid fatigue, however greater error in calculating muscle activation occurs between different days (Dankaerts, O’Sullivan, Burnett, Straker, & Danneels, 2004). Although the tasks performed varied between studies, within each study tasks were standardized in each sitting condition, to control for task variation affecting the results (Groenesteijn et al., 2012).
In both reviews, several studies did not control for the presence of armrests. Only two studies (Bendix, 1984; Soderberg et al., 1986) specifically stated that participants had to rest their elbows in front of them. Seven studies (Bridger, 1988; Cram & Vinitzky, 1995; Hardage et al., 1983; van der Heide et al., 2003; Winkel & Bendix, 1986; Wu et al., 1998; Yu et al., 1988) did not state whether seats featured armrests which could confound results. All other studies featured armless seats, however they did not monitor or report if participants were forward leaning onto a surface such as a table, which could confound results (Soderberg et al., 1986).
Strength of results
None of the included studies in either of the two reviews calculated their sample size based on a-priori power calculations, and many may have been underpowered to detect differences between sitting conditions. Appropriate methods of statistical analysis were used in nearly all studies. Only a small number of studies included a considerable number of dropouts, and suitable intention-to-treat analysis was used in most of these studies reducing the risk of attrition bias. The sample size among studies in the review of seated hip flexion angles ranged from two to 293, with an overall sample of 986 participants included. The sample size among studies in the review of chair backrests ranged from 10 to 24, with an overall sample of 131 participants included. The review on chair backrests found no randomized controlled trial (RCT) or longitudinal studies with a follow-up period, preventing any attempt to identify if using a chair backrest reduces LBP incidence or severity in the medium term.
Clinical applicability
Only seven studies across both reviews included participants with LBP, with little detail provided on their level of functional disability which limits its clinical applicability. In laboratory-based studies, participants were usually asked to perform simulated functional or occupational tasks to enhance clinical applicability. Only five studies examined the effect of reducing seated hip flexion over a prolonged period of time. However, some of these studies (Koskelo et al., 2007; Saarni et al., 2009) had long follow-up periods of approximately 2 years. Four of these five follow-up studies examined schoolchildren, which may not reflect the nature, or intensity, of LBP reported by adult populations. Several different scales to analyze LBP and LBD were used, preventing pooled analysis of the data. Some studies simply asked participants about their subjective preference, which is less clinically relevant. There were also large variations in the trunk muscles analyzed between studies (Table 1). Even when studies analyzed the same muscles, variations regarding electrode placement and the type of muscle activation analysis performed did not allow for pooled analysis of the data.
Discussion
The results of both systematic reviews will be discussed for muscle activation and discomfort separately.
Muscle Activation
Muscle activation on chairs that reduce seated hip flexion
The use of kneeler chairs was associated with increased paraspinal muscle activation and/or increased discomfort in five of the eight studies that investigated them. In these five studies the control sitting condition offered participants a backrest whereas the kneeler chair did not, which is likely to partly explain the difference between the sitting conditions. This is further highlighted by the fact that the three studies that reported at least some benefit from kneeler chairs ensured that the presence or absence of a backrest was consistent between the sitting conditions compared (Bridger, 1988; Marschall et al., 1995; Soderberg et al., 1986). In addition, two of the three studies which reported some benefit from a kneeler chair, combined it with a sloping desk, which may also have contributed to the benefit (Bridger, 1988; Marschall et al., 1995). Therefore, it would appear that kneeler chairs actually increase paraspinal muscle activation and/or discomfort, unless they have a backrest or are integrated into a wider ergonomic workstation with sloping desks, when they may actually reduce paraspinal muscle activation and are preferred by participants. The increase in discomfort associated with these chairs when they do not have a backrest suggest that paraspinal muscle activation increases in the absence of external support being provided by the backrest, leading to unnecessarily high levels of muscle activation being needed to provide active support. No study examined the use of kneeler chairs prospectively.
The 13 crossover studies which reduced seated hip flexion through changing the seat height, using tilted seat pans, or combining these features, revealed more consistent results, reflecting the fact that 12 of these studies controlled for confounding variables such as the presence of a backrest and the use of sloping desks. None of these 13 studies demonstrated unequivocal advantages for reducing seated hip flexion.
Muscle activation on chairs with backrests
Five of the seven studies in the backrest review reported that using a backrest significantly reduced LES muscle activation (Cram & Vinitzky, 1995; Hardage et al., 1983; Kingma & van Dieen, 2009; Lander et al., 1987; Yoo et al., 2008). A backrest had minimal effects on the other trunk muscles studied. The effect of the backrest appears to differ according to its position, with the paraspinal muscles at the height of the backrest being the most likely to be decreased (Yoo et al., 2008). The decrease in LES activation is likely due to external support being provided by the backrest, which spares the muscles from needing to provide active support.
Sitting Discomfort
Discomfort on chairs that reduce seated hip flexion
One study (Gadge & Innes, 2007) reported less LBD and OBD among pain-free participants when using a saddle chair with a backrest, but this was offset by an increase in buttock discomfort. Another study reported reduced LBD when sitting in less hip flexion among people with LBP (Michel & Helander, 1994), however pain-free participants reported greater discomfort using this chair. Finally, some limited evidence to support the use of reducing seated hip flexion was observed in two studies that reported a reduction in the activation of some paraspinal muscles (van der Heide et al., 2003) and enhanced subjective acceptability compared to a freely tiltable chair (Bendix et al., 1986). However, most of the crossover design studies reported no difference in LBP or LBD when seated hip flexion was slightly reduced (Bendix, 1984; Bendix & Biering-Sørensen, 1983; Bendix et al., 1985; Hardage et al., 1983; Jensen & Bendix, 1992; Winkel & Bendix, 1986; Wu et al., 1998). In fact, several studies (Bendix & Biering-Sørensen, 1983; Bendix et al., 1988; Naqvi, 1994; Wu et al., 1998) noted that reducing hip flexion to a much larger degree actually increased discomfort. One study (Yu et al., 1988) actually reported greater discomfort when seated hip flexion was reduced. However, the hip angles compared were 105° and 135°, probably reflecting the previous point that very large decreases in hip flexion appear to increase discomfort. Finally, although using ergonomic workstations including saddle-type chairs was preferred during the first year of a 2-year study (Saarni et al., 2009), this preference was lost in the second year. It is clear therefore that although some studies subjectively preferred chairs with reduced hip flexion, the majority of studies that examined discomfort demonstrated increased discomfort levels, particularly if large changes in hip flexion occurred.
Discomfort on chairs with backrests
The only two studies (Gregory et al., 2006; Lander et al., 1987) which specifically examined the effect of a backrest on sitting discomfort favored using a backrest. One other study (Kingma & van Dieen, 2009) did not specifically measure discomfort, but also reported increased participant comfort using a backrest during pilot testing. None of these three studies included people with LBP.
Consideration of Confounding Variables
As previously stated, the presence of several significant confounders in many studies warrants some caution in interpreting these findings. Nevertheless, it is possible to at least partly interpret the contribution of such confounders to the results. For example, a recent systematic review (O’Sullivan, O’Keeffe, et al., 2012) suggests that dynamic sitting does not significantly influence LBP or LBD. Consequently, the most likely reason for differences observed in the two dynamic comparisons (Gregory et al., 2006; Kingma & van Dieen, 2009) was the presence of a backrest rather than differences in mobility. It is more difficult to determine the confounding influence of hip angle when interpreting the effect of using a backrest. The single study that did actually control for hip angle between chairs with and without a backrest (Hardage et al., 1983) reported no difference in muscle activation between three different hip angles. Similarly, although the kneeler chair design typically increased paraspinal activation (Bennett et al., 1989; Cram & Vinitzky, 1995; Lander et al., 1987), other studies (e.g., Koskelo et al., 2007) have reported decreased paraspinal activation using other chair designs with less seated hip flexion. Variations in the degree of forward trunk lean between studies may also be relevant, as this could also influence paraspinal muscle activation if not monitored closely. This may explain why the differences between chairs in one of the studies were smaller during forward lean tasks than during sitting (Bennett et al., 1989). This overlaps with the fact that none of the included studies measured how much pressure was placed on the backrest, or whether in fact it was used by participants (Vergara & Page, 2000a). Another common potential confounder was that studies (e.g., Bridger, 1988; Cram & Vinitzky, 1995; Hardage et al., 1983; van der Heide et al., 2003; Winkel & Bendix, 1986; Wu et al., 1998; Yu et al., 1988) did not always state whether seats featured armrests or not. Finally, it appears the effect of a backrest is closely related to its location (Yoo et al., 2008), which may explain some of the variation between studies. Notwithstanding these confounding factors, the results demonstrate moderate evidence that chair backrests reduce paraspinal muscle activation, and limited evidence that chair backrests reduce LBD. For chairs involving less hip flexion, the increased LBP/LBD reported in many studies probably reflects the confounding effect of not providing a backrest in the intervention chair. Therefore, for chairs involving less seated hip flexion the results demonstrate no evidence that they reduce LBP or LBD, or consistently alter trunk muscle activation.
Implications
This relatively limited supporting evidence to support the use of chairs involving less seated hip flexion or backrests is consistent with the limited evidence that other chair design features in isolation reduce LBP (Driessen et al., 2010, O’Sullivan, O’Keeffe, et al., 2012). This reflects the multidimensional nature of LBP where not just biomechanical and ergonomics factors, but also psychosocial (Carroll, Cassidy, & Côté, 2004; Jarvik et al., 2005; Main, Foster, & Buchbinder, 2010; Mitchell et al., 2010; Ramond et al., 2011), lifestyle (Chiu et al., 2005; Onen, Alloui, Gross, Eschallier, & Dubray, 2001), genetic (Battié, Videman, & Parent, 2004; Reichborn-Kjennerud et al., 2002), and neurophysiological (Apkarian, Baliki, & Geha, 2009; Wand et al., 2011) factors may be involved (O’Sullivan, 2012). Therefore, any unidimensional biomechanical or ergonomic approach to managing LBP is likely to be of limited effectiveness in isolation. Considering that people with LBP have previously been shown to have greater difficulty relaxing their trunk muscles than people without LBP (Geisser et al., 2005), using a backrest to reduce muscle activation may be of benefit to people with LBP. Another important consideration is the need to discriminate between participant ratings of preference in the short term compared to clinically meaningful changes in LBP/LBD in the long term. Participants in several studies subjectively preferred the chairs involving less hip flexion, but these chairs typically did not result in reductions in LBP/LBD. It may be that simply changing spinal loading, and/or the novelty associated with a new chair design, explains these short-term positive perceptions without actually having a meaningful impact on LBP. All of the studies included in these reviews prescribe the same change in sitting to all participants. This is not consistent with clinical practice, and does not reflect well documented individual variations in posture and movement patterns among people with LBP (Dankaerts et al., 2006; Dankaerts et al., 2009). For example, two recent studies published after short listing for these systematic reviews was complete suggest that matching chair prescription to the individual presentations of people with LBP may be more effective than generic prescriptions that adopt a one-size-fits-all approach (Curran, Dankaerts, O’Sullivan, O’Sullivan, & O’Sullivan, 2014; O’Keeffe, Dankaerts, O’Sullivan, O’Sullivan, & O’Sullivan, 2013). We believe that if changes in chair design are to have a more significant impact on LBP it will be through matching the seating prescription to the individual, their specific demands at work or home, and/or linking it with other barriers to recovery from LBP across the biopsychosocial spectrum.
Limitations
The main limitations of these reviews are that significant differences in the outcome measure used, the participants included, and the comparison sitting conditions did not allow for pooled analysis of the data. There were very few RCT designs including people with LBP, and most tended to involve only very short-term follow-up of participants. Larger RCTs involving people with LBP, with suitable blinding, less confounding variables, and involving a long-term follow-up period, are required to fully confirm the findings of this review. Given the tendency for novel chair designs to differ in several ways (e.g., backrest presence and/or orientation, seat pan angle and motion, lower limb position; O’Sullivan et al., 2012a, 2012b), studies that identify the specific utility of each design feature may be useful. Many of the included studies were quite old, with specific design features which were unclear. The uncertainty as to whether armrests were used or not in several of the studies may have influenced the findings. Further research is required to shed light on whether the acceptability of specific chair designs is affected by the duration of sitting studied.
Conclusion
These two reviews included a total of 29 studies investigating the effect of backrests and reduced seated hip flexion on sitting discomfort or trunk muscle activation. Significant confounding variables existed, and only a small number of RCTs involving people with LBP were found. There was moderate evidence that chair backrests reduce paraspinal muscle activation, and limited evidence that chair backrests reduce LBD. Despite participants in several studies subjectively preferring chairs involving less hip flexion, there was no evidence that these chairs reduce LBP or LBD, or consistently alter trunk muscle activation.
The limited evidence to support the use of chairs involving less seated hip flexion, or the effect of a backrest, is consistent with the limited evidence that other isolated chair design features can reduce LBP.
Key points
The effect of a chair backrest and reducing seated hip flexion on low back pain (LBP)/low back discomfort (LBD) and trunk muscle activation was systematically reviewed.
Many studies included several confounding variables, and only a small number of RCTs involving people with LBP were found, which complicated analysis of the results.
There was moderate evidence from seven studies that chair backrests reduce paraspinal muscle activation, and limited evidence that chair backrests reduce LBD.
Despite participants in several studies subjectively preferring chairs involving less hip flexion, there was no evidence that these chairs reduce LBP or LBD, or consistently alter trunk muscle activation.
The limited evidence to support the use of chairs involving less seated hip flexion, or the effect of a backrest, is consistent with the limited evidence that other isolated chair design features can reduce LBP.
Footnotes
Acknowledgements
KO was supported by a fellowship from the Health Research Board of Ireland. Thanks to Mary O’Keeffe and John Hurley for comments on the draft manuscript. Some of the authors are currently involved in studies using a chair that involves sitting in less hip flexion (![]() ), and that is used in the management of low back pain. Those studies are partially funded by the manufacturers of the chair. The authors do not feel this has in any way affected this systematic review, but are disclosing this fact to enhance transparency. None of the authors have any stake/shares in this, or any other specific chair design.
), and that is used in the management of low back pain. Those studies are partially funded by the manufacturers of the chair. The authors do not feel this has in any way affected this systematic review, but are disclosing this fact to enhance transparency. None of the authors have any stake/shares in this, or any other specific chair design.
Máire Curran is a physiotherapist working in clinical practice. She earned her BSc (Hons) in physiotherapy from the University of Limerick, Ireland in 2013.
Leonard O’Sullivan is a senior lecturer in the Department of Design and Manufacturing Technology at the University of Limerick, Ireland. He earned his PhD in ergonomics from the University of Limerick in 2002.
Peter O’Sullivan is professor of musculoskeletal physiotherapy at Curtin University, Perth, Australia. He earned his PhD in physiotherapy from Curtin University in 1998.
Wim Dankaerts is a professor at the University of Leuven, Belgium. He earned his PhD in physiotherapy from Curtin University in 2005.
Kieran O’Sullivan is a physiotherapy lecturer in the Department of Clinical Therapies at the University of Limerick, Ireland. He earned his PhD in physiotherapy from the University of Limerick in 2012.