
Abstract
Objective:
The purpose of this study was to determine maximum forces during syringe use for different grips found in the field.
Background:
Prolonged syringe use in chemotherapy drug delivery is associated with pain and injury in nurses and technicians.
Method:
Twenty healthy female hospital workers generated isometric maximum voluntary force using a 30 cc syringe with four pinch grips (chuck, chuck variation, thenar, two-handed). Both dominant and nondominant hands were used with the syringe plunger fixed in wide (8.3 cm) and narrow (2.5 cm) grip spans. Participants were encouraged to position the apparatus in the most comfortable position and exert a maximal effort for 5 seconds.
Results:
Significant interaction effects were found: Grip Span × Pinch Type, Hand × Pinch Type, and Grip Span × Hand × Pinch Type (p < .05). The results demonstrated that the thenar (103.6 ± 22.9 N) and two-handed (104.7 ± 17.1 N) pinches produced the highest forces.
Conclusion:
Thenar and two-handed pinch grips may be the preferred pinch type to lower the relative efforts required to use a syringe and may be one strategy to assist with reduction of musculoskeletal disorder risk associated with syringe use.
Application:
Determining maximal syringe press forces allows workers and ergonomists to develop better strategies for managing the cumulative loads during drug delivery and mixing.
Introduction
The ability to use the thumb to grasp and manipulate objects is important in hand function for activities of daily living (Goehler & Murray, 2010). The thumb is capable of producing high pinch forces; however, force requirements for pinching tasks in the occupational setting may exceed the capacity of some workers, thereby increasing the risk of musculoskeletal injury (Nussbaum & Johnson, 2002; Viikari-Juntura & Silverstein, 1999). This is of prime concern with syringe use in hospitals. Prolonged gripping and pressing during syringe use is observed in the daily activities of nurses, pharmacists, and other jobs that require mixing and/or administering medication or fluids. Chemotherapy nurses are required to manually administer (“push”) chemotherapy medication via syringe at slow rates of 1 to 2 ml/minute continuously for up to 30 minutes. Sustained manual delivery is required to gently and cautiously inject the potent medication. In addition, pharmacy technicians manually mix the drugs using syringes to draw the drugs from vials and inject them into IV lines and bags repetitively for up to 90 minutes.
Pinch force, wrist posture, and repetition have been shown to contribute to musculoskeletal disorders (MSD) of the hand and wrist (Viikari-Juntura & Silverstein, 1999), such as carpal tunnel syndrome, De Quervain’s tenosynovitis, and tendinitis. Previous research has investigated the relation of strength with respect to wrist position (Imrhan, 1991), repetition (Snook, Ciriello, & Webster, 1999), pinch grip type (Imrhan & Sundararajan, 1992), and grip span (Shivers, Mirka, & Kaber, 2002). To date, there are no published data on pinch strength associated with syringe use. Acquiring information about the relationship between grip span, hand, and pinch grip type would be beneficial in developing risk-reducing strategies. The purpose of this study was to obtain maximal pinch forces using various pinch grip types associated with operating a syringe for use in future syringe-based studies.
Method
Participants
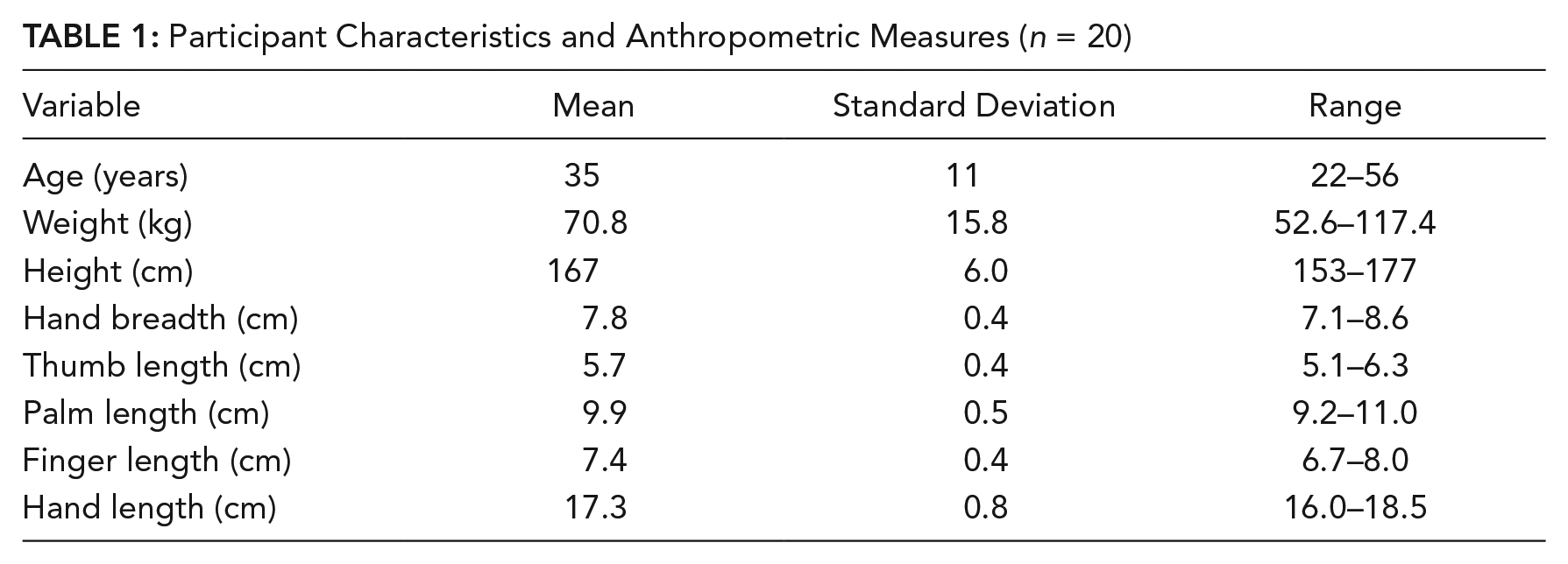
Twenty healthy female workers participated in this study (characteristics in Table 1). Participants reported good health and no previous upper limb pain or musculoskeletal disorders in the prior 6 months and were recruited from the administrative offices of the hospital. This study was approved by the McMaster University Hamilton Health Sciences/Faculty of Health Sciences Research Ethics Board. All participants provided written informed consent.
Participant Characteristics and Anthropometric Measures (n = 20)
Procedure
Anthropometric measurements were taken, including height, mass, and hand size (hand breadth, thumb length, palm length, finger length, and hand length using digital calipers) (Table 1). Participants produced maximal isometric forces on the plunger of a standard 30 ml syringe using four common pinch grip types at two plunger lengths, which effectively created two grip spans. Static forces were measured using a digital force gauge (M5-200, Mark-10 Corporation, Copiague, NY, USA) attached to the distal end of a 30 ml syringe with a 2.54 cm (1”) diameter plunger and flanges of approximately 0.64 × 0.64 cm (0.25” × 0.25”) (BD Luer-Lok Sterile Syringes, Franklin Lakes, NJ, USA). Participants were seated in a chair adjusted with feet flat and thighs parallel to the floor. The force gauge–syringe setup was mounted on a tripod adjusted to knee height and modified for comfort by each participant. The tilt angle of the syringe was not constrained.
Four syringe pinch grip types commonly used in the field were tested (Figure 1). The four grip types were: (a) chuck pinch—index and middle finger pads placed on syringe base with thumb pad on syringe plunger; (b) chuck pinch variation—middle and ring finger pads placed on the syringe base with thumb pad on the syringe plunger; (c) thenar pinch—index and middle finger pads on the syringe base with thenar eminence pressing on syringe plunger; and (d) two-handed pinch—index finger pads on syringe base with the tips facing each other with both thumb pads on syringe plunger.
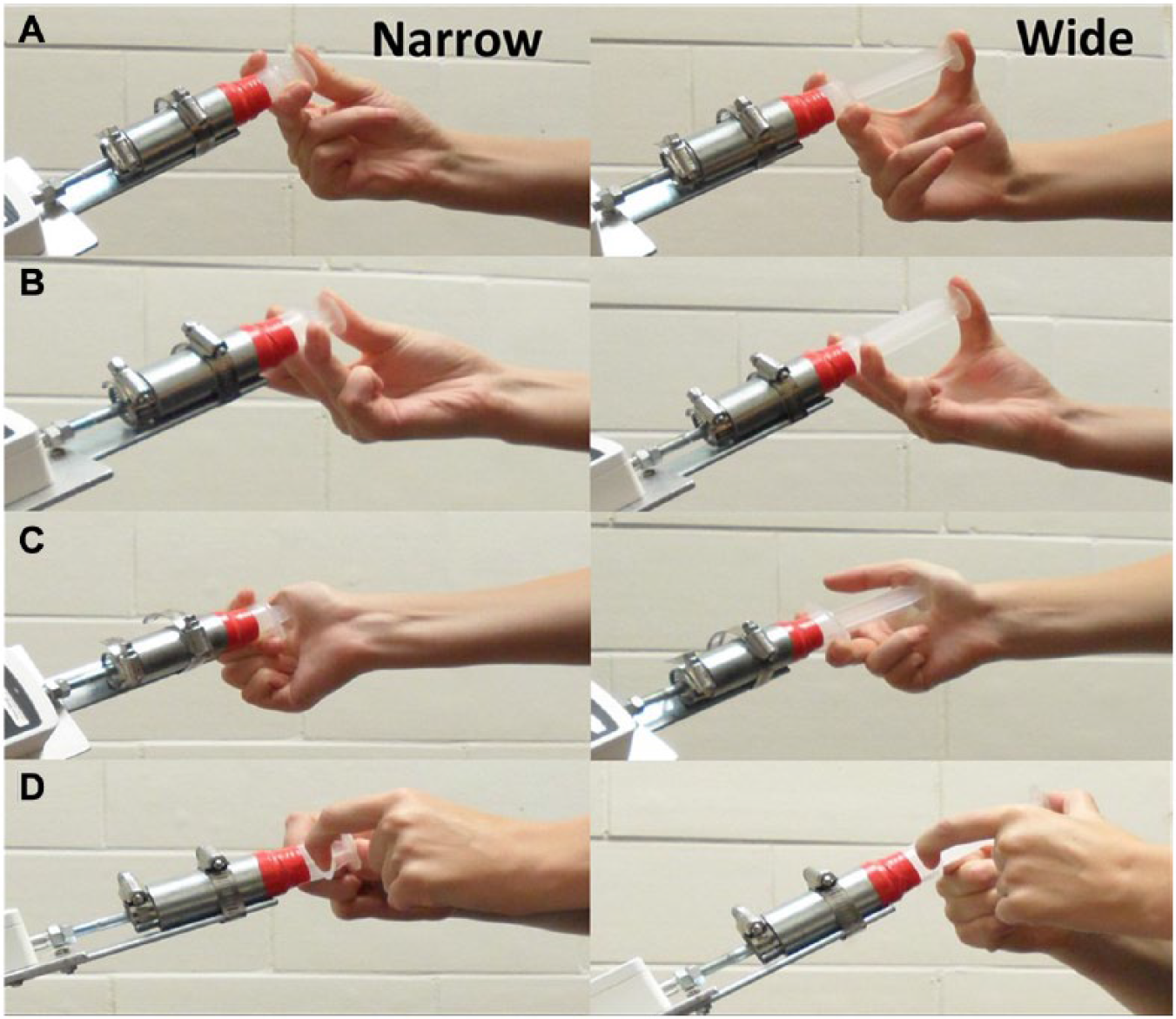
Pinch grip types with a (left) narrow and (right) wide grip span. (A) Chuck pinch. (B) Chuck pinch variation. (C) Thenar pinch. (D) Two-handed pinch.
Participants were shown photographs, given instructions, and given time to practice each pinch grip type. In each trial, the plunger was pressed maximally for 5 seconds. Verbal encouragement was given during the trials to help promote maximal exertion. A one-minute rest was given between trials with additional rest provided if the participant reported symptoms of fatigue. Each grip was performed twice, and the peak force was recorded. A third trial was performed if the first two trials differed by more than 15%. Conditions were blocked by grip span (wide or narrow), alternating the starting grip span between each participant. Both hand and pinch grip type order were randomized. Thus, each pinch grip was used with both dominant and nondominant hands in both wide (8.3 cm) and narrow (2.5 cm) grip spans to simulate full and near empty syringe conditions. A tripod-mounted digital camera recorded hand and wrist posture during each trial.
Data Analysis
For each of the three one-handed postures, the mean peak force of all participants was evaluated using a 2 (grip span) × 2 (hand) × 3 (pinch grip type) repeated measures ANOVA (SPSS v 17.0; IBM Corporation, Armonk, NY, USA). To include the two-handed pinch grip, a 2 (grip span) × 4 (pinch grip type) repeated measures ANOVA was performed including the mean peak force between dominant and nondominant hands. Significant effects were followed up using Tukey’s honest significant difference (HSD) test. To examine the relationships between strength and anthropometric measures, Pearson product moment correlations were performed. An α level of 0.05 was used for all tests.
Results
There were significant main effects for all variables in the one-handed grips (grip, span, and hand). The dominant hand was significantly stronger than the nondominant hand, and the narrow grip was significantly stronger than the wide grip. The thenar grip was stronger than the chuck pinch, which was stronger than the variation of the chuck pinch (p < .05) (Table 2). The two-handed pinch was significantly stronger than the chuck and chuck variation pinches but not the thenar pinch (p < .05). The mean maximum forces may be found in Table 2.
Descriptive Statistics of Mean Peak Force (N) With Respect to Pinch Grip Type, Hand, and Grip Span (n = 20)
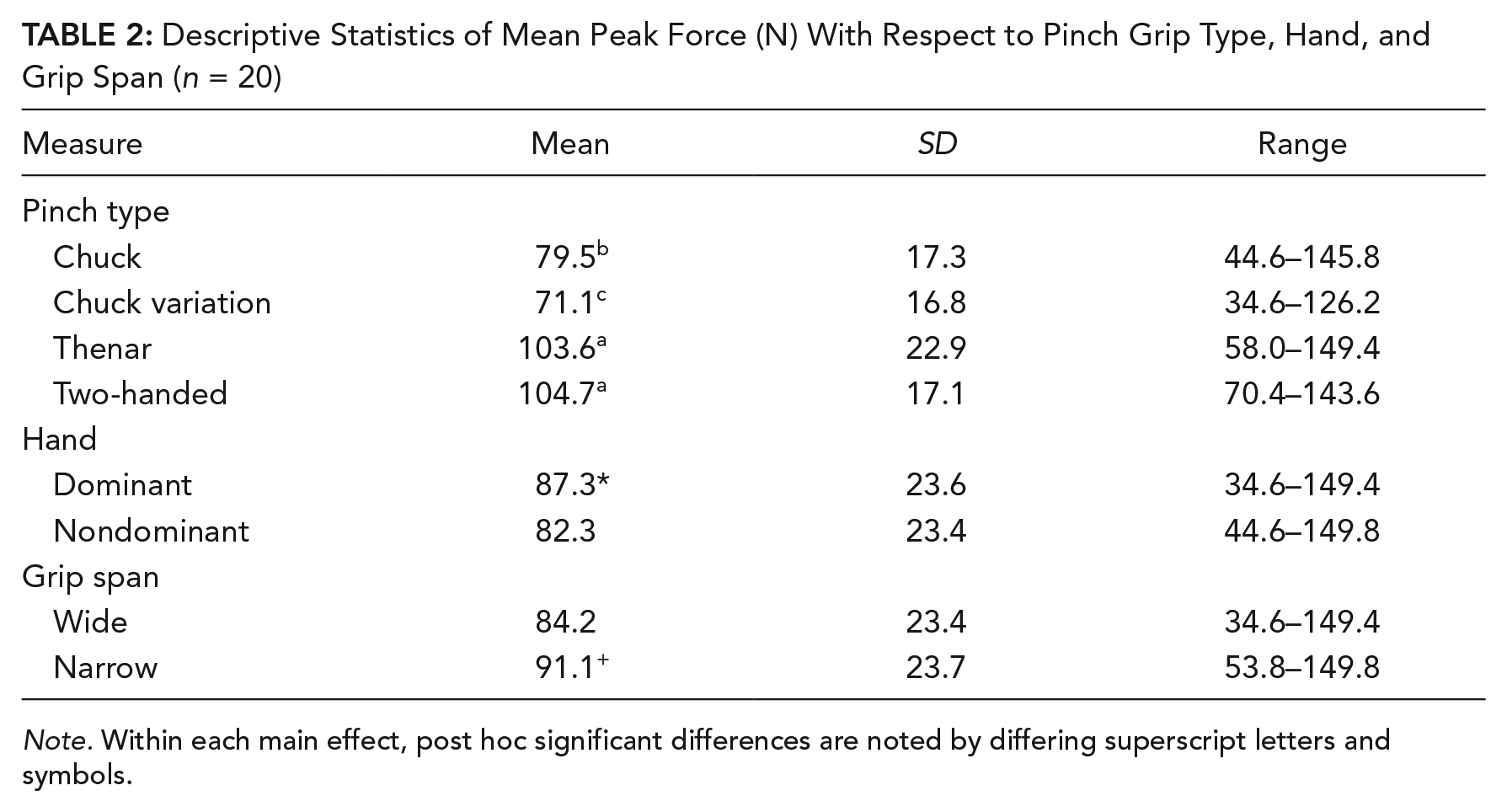
Note. Within each main effect, post hoc significant differences are noted by differing superscript letters and symbols.
A three-way interaction between Pinch Grip Type × Hand × Grip Span was found for pinch force, F(2, 38) = 4.7, p < .01 (Figure 2). This was primarily due to a greater maximum force in the wide (111.1 ± 19.2 N) versus the narrow (102.2 ± 22.6 N) dominant hand thenar grip while there was no difference in the nondominant hand (wide, 100.9 ± 21.7 N; narrow, 100.2 ± 27.5 N). All other grip types had greater forces in the narrow grip or no significant difference (Figure 2). Thenar grip force was significantly greater than both the chuck and chuck variation grips for both hands and both grip spans. In the dominant hand, the chuck pinch produced significantly greater force than the chuck variation pinch in both the wide (77.0 ± 12.8 N vs. 66.9 ± 13.9 N, respectively) and narrow grip spans (89.4 ± 19.5 N vs. 77.0 ± 18.8 N, respectively). In the nondominant hand, chuck pinch force was greater (71.8 ± 15.6 N in the wide grip, 80.0 ± 16.7 N in the narrow grip) than the chuck variation pinch (64.1 ± 15.1 N in the wide grip, 77.1 ± 15.4 N in the narrow grip). There were no significant differences between forces produced using chuck or thenar pinches in either grip span in the nondominant hand.
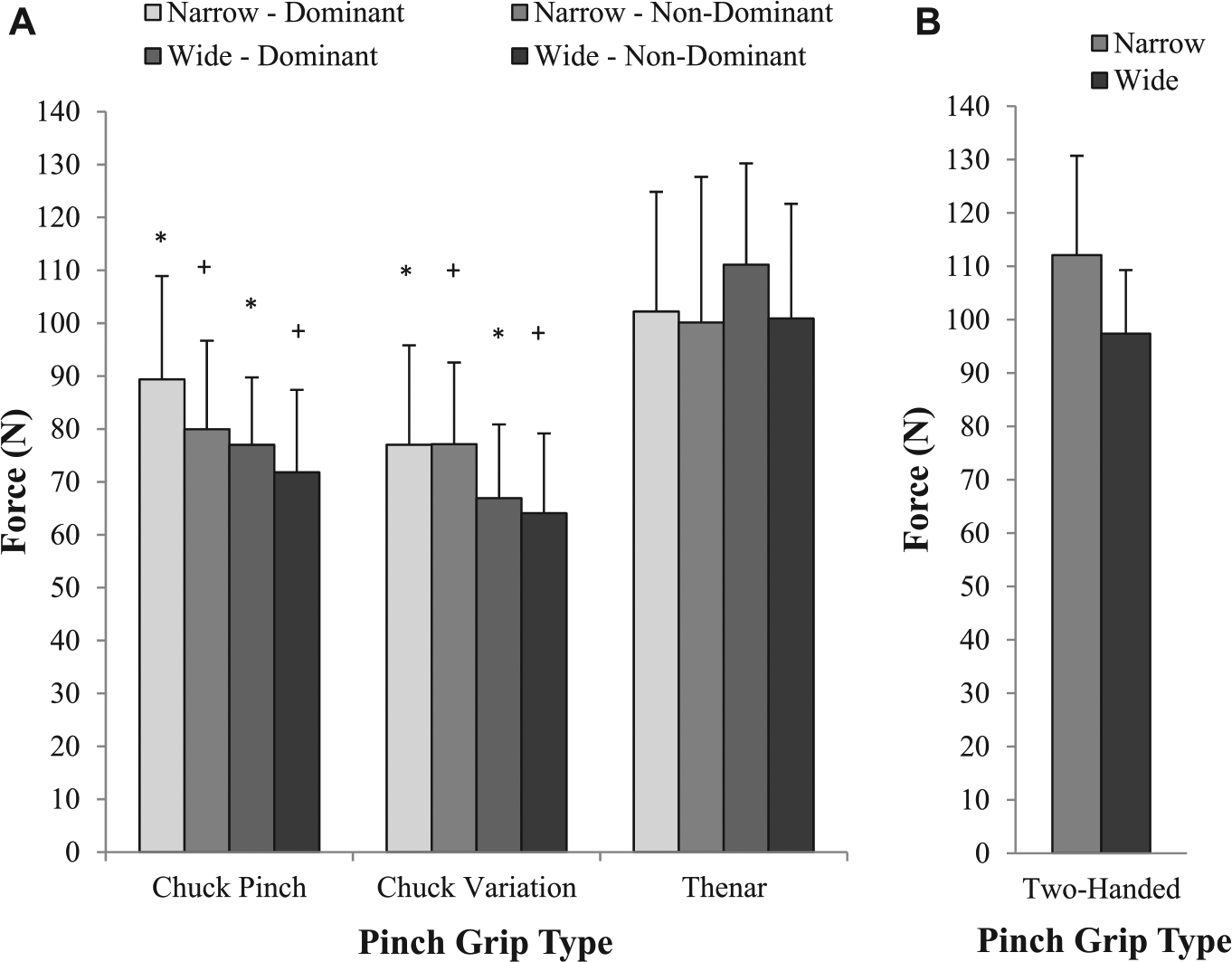
Mean maximal pinch grip force (N) with standard deviation for all postures. (A) Three pinch grip types using both dominant and nondominant hands as well as narrow and wide grip spans. (B) Two-handed pinch using narrow and wide grip spans. The * designates this grip was significantly different (p < .05) from the thenar and chuck variation pinches in its respective grip and hand dominance condition. The + indicates there was only a statistically significant difference between the respective condition and the thenar pinch (no significant difference between chuck and chuck variation pinch). The two-handed pinch was not included in the ANOVA but is shown for comparison.
The 2 (grip span) × 4 (pinch grip type) repeated measures ANOVA revealed a significant main effect of grip type, F(3, 57) = 75.9, p < .0005, with the two-handed pinch force (104.7 ± 17.1 N) and thenar pinch (103.6 ± 22.9 N) being significantly higher than the chuck pinch (79.5 ± 17.3 N) and chuck pinch variation (71.1 ± 16.8 N) (Figure 3). An additional main effect existed for grip span, with the wide grip producing significantly lower forces than the narrow grip (84.2 ± 23.4 N, compared to 91.3 ± 23.7 N, respectively). Post hoc testing revealed significantly lower forces in all grips in the wide span condition compared to the narrow span condition, except for in the thenar grip.
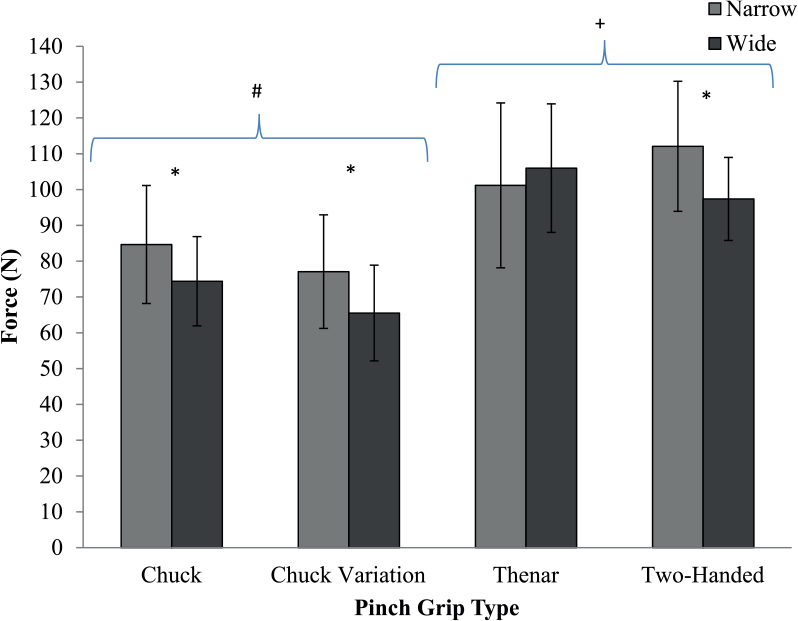
Mean maximal pinch grip force (N) with standard deviations of all pinch grip types in both wide and narrow grip spans. The thenar pinch had higher forces in the wide span while all other pinch grip types had greater force in the narrow span (p < .05). The * indicates there was a statistically significant difference between wide and narrow grip spans for this grip type, whereas the + indicates that these grips were significantly different from grips denoted by #.
While several correlations with force were statistically significant, explained variance ranged between about 20% and 30%. Moderate correlations with force were found in the following: (a) height and nondominant chuck variation pinch with a wide span (r = 0.481), (b) weight and nondominant chuck pinch with a narrow span (r = 0.458), and (c) dominant hand length and dominant chuck pinch with a narrow span (r = 0.444). Also, when looking at hand length, the forces associated with the dominant thenar (wide span), chuck, and chuck variation pinch grips (narrow span) were moderately correlated with nondominant hand length (r = 0.512, 0.536, and 0.535, respectively).
Discussion
This study determined the maximum forces generated on a 30 ml syringe plunger using four pinch grip types and may assist ergonomists in determining relative workload as well as joint forces. The thenar (103.6 ± 22.9 N) and two-handed (104.7 ± 17.1 N) pinch grips produced greater forces than the chuck (79.5 ± 17.3 N) and chuck variation (71.1 ± 16.8 N) pinch grips (Figure 2). Therefore, using thenar or two-handed techniques under submaximal work conditions would require a significantly lower relative force and effort, suggesting that these postures may be best during repetitive and prolonged syringe use. However, sustained and repetitive use of similar postures even at low force levels can lead to an increased risk for MSD (Bernard et al., 1997). The grips tested, and others that may be used in the field, likely result in pressure points and wrist postures that have detrimental effects on blood flow. As a result, workers frequently choose to alternate between hand use and various postures to avoid discomfort during sustained and repetitive tasks. Individual anthropometry and strength likely play a role in these choices, although this was not borne out in the current study. The dominant arm has been found to be more susceptible to MSD than the nondominant arm (Shiri,Varonen, Haliovaara, & Viikari-Juntura, 2007), suggesting differences in exposure to physical load factors between hands. Force differences between dominant and nondominant hands were only observed in the chuck pinch (Figure 2), where the force generated by the dominant hand (83.2 ± 16.2 N) was greater than the nondominant (75.9 ± 16.2 N) hand. Therefore, it is assumed that hand dexterity may play a greater role in this particular grip type. In addition, the chuck pinch may be used more frequently; thus, skill level may be associated with the type of pinch used and the force generated.
Regardless of hand, the thenar pinch was the only pinch grip type that had higher forces in the wide span (106.6 ± 21.2 N). All other pinches had an increase in force in the narrow span with the two-handed pinch having the highest force (112.1 ± 18.6 N). This could suggest that the thenar pinch may be best to use when the syringe is mostly full or at the start of a treatment and that use of the two-handed pinch would be best once the syringe is nearly empty or at the end of the treatment. This strategy may promote a lower relative effort throughout the push and decrease the risk of fatigue and consequently, injury.
A note of caution arises with repeated use of the thenar pinch. This pinch involves compression on the thenar eminence and thus the recumbent branch of the median nerve, which may increase the risk of injury to the surrounding tissues. Often, the choice of pinch grip used in the field is influenced by the object gripped and the task performed (Imrhan & Sundararajan, 1992), in this instance, a syringe. As a result, the two-handed pinch may be the best option since it produces greater force while avoiding the compression of important nerve structures. However, as suggested in tool design, increasing the size of the contact surface area, placing padding on the contact surface, and limiting total exposure time may avoid such point compression of this area and allow the thenar pinch to be beneficial for tasks requiring a brief increase in force requirements (Fransson-Hall & Kilbom, 1993).
Of further note is the force difference observed between the one-handed pinch and the two-handed pinch. One may expect that the force should double when using both hands. The results illustrate that this did not occur and may indicate the possibility of force sharing between both hands. If both hands share the same force, then a decrease in relative force for each hand occurs. It is also important to consider that the one-handed pinch used both the index and middle finger while the two-handed pinch was constrained to using only the index finger, which may have also influenced the force generated.
Wrist postures were captured for each pinch type, and it was found that even though participants were encouraged to position the syringe using neutral wrist postures and as comfortable as possible, deviated, flexed, and extended wrist postures were still observed. This may indicate that neutral wrist posture may not be the most comfortable for maximum strength generation. It may also suggest that users may have reduced ability to maintain a neutral wrist posture during maximum static grip exertions compared to submaximal exertions. Our previous work with gripping found that to maximum grip forces were similar between a neutral and extended wrist but reduced greatly with flexion. At lower force levels, this effect was reduced (Mogk & Keir, 2003). The use of an extended wrist while applying force also has consequences to the median nerve due to increased pressure in the carpal tunnel (Keir, Bach, Hudes, & Rempel, 2007; Keir, Bach, & Rempel, 1998). It is important to note that while wrist postures were not analyzed, the use of neutral posture is encouraged, especially understanding that majority of work tasks require lower relative forces. Therefore, the ability for the individual to control the wrist posture along with choice of pinch grip is possible and subsequently reduces the risk of MSDs.
There are a few limitations to this study. While we used a fixed force transducer to measure static press forces, the maximal forces obtained should be considered representative of the very slow push rates (1–2 ml/minute). It is also important to consider that liquids are incompressible, thus the “feel” of the test was similar to starting a press or when there is a blockage in the line. Second, we used administrative workers who were not accustomed to operating a syringe. This combined with a relatively small sample size limits our ability to generalize the findings to all trained workers. In addition, individual differences may contribute to the selection of the most comfortable grip type. Maximal pinch force could not be predicted very accurately from anthropometric dimensions. Despite a few statistically significant correlations, anthropometric data did not provide strong associations with pinch grip type, hand dominance, or grip span. Finally, we based the four grip types on those observed from a limited number of workers, thus other types may be adopted in the field.
Conclusion
Thenar and two-handed pinch grips generated the greatest forces. The forces determined in this study can be used in future studies to analyze the proportion of strength required during syringe work, which in turn can assist in determination of risk reduction strategies in the field. Of these strategies, one may suggest potential preferred pinch grips when increased forces are required during syringe use.
Key Points
Prolonged syringe use in chemotherapy drug delivery and mixing is associated with pain and injury in nurses and technicians.
Twenty healthy female hospital workers produced isometric maximum voluntary forces with four syringe grips (chuck, chuck variation, thenar, two-handed) in wide (8.3 cm) and narrow (2.5 cm) grip spans.
Thenar and two-handed pinch grips had the highest maximal forces.
Using thenar and two-handed pinch grips may lower the relative effort required to use a syringe and may help reduce musculoskeletal disorder risk.
Footnotes
Acknowledgements
This study was supported with grants from the Natural Sciences and Engineering Research Council of Canada (NSERC DG No. 217382) and the Centre for Research Expertise for the Prevention of Musculoskeletal Disorders (CRE-MSD).
Victoria MacDonald received a HBK (2004) and BA (2004) in psychology from Lakehead University and MSc (2014) in kinesiology from McMaster University. Her research interests center around work-related musculoskeletal disorders of the upper limb as it relates to the hand efforts and syringe tasks completed by chemotherapy nurses and pharmacy assistants.
Katherine Wilson received her bachelor of science in kinesiology (honours co-op) at the University of Waterloo and completed her MSc in biomechanics at McMaster University in the Department of Kinesiology. Katherine is currently the research manager of the concussion centre within the Bloorview Research Institute at the Holland Bloorview Kids Rehabilitation Hospital.
Michael W. L. Sonne is a MITACS postdoctoral fellow at McMaster University in the Department of Kinesiology. Michael completed his master’s (2010) and bachelor’s of human kinetics (2007) degrees at the University of Windsor and received his PhD from McMaster University in ergonomics and occupational biomechanics in 2014. His primary research focus is on the assessment and prediction of muscle fatigue in the workplace.
Peter J. Keir is a professor in the Department of Kinesiology at McMaster University in Hamilton, Ontario. He received his PhD from the University of Waterloo in 1995. His research examines upper extremity mechanics and function using EMG, imaging, and modeling to determine the mechanisms of work-related musculoskeletal disorders, with an emphasis on carpal tunnel syndrome and muscle-related injuries of the arm and hand.