
Abstract
Objective
The aim of this study is to examine the effects of cognitive and physical loads on dynamic and static balance performance of healthy older adults under single-, dual-, and multi-task conditions.
Background
Previous studies on postural control in older adults have generally used dual-task methodology, whereas less attention has been paid to multi-task performance, despite its importance in many daily and occupational activities.
Method
The effects of single versus combined (dual-task and multi-task) cognitive (to speak out the name of the weekdays in a reverse order) and physical (with three levels including handling weights of 1, 2, and 3 kg in each hand) loads on dynamic and static balance performance of 42 older adults (21 males and 21 females) aged ≥60 years were examined. Dynamic and static balance measures were evaluated using the Timed Up and Go (TUG) and stabilometer (sway index) tests, respectively.
Results
The TUG speed of female participants was generally slower than that of male participants. Age had no effect on balance performance measures. Under dual-task conditions, cognitive load decreased the dynamic balance performance, while the physical task levels had no effect. The dual-task conditions had no impact on the static balance performance. The effects of cognitive and physical loads on dynamic balance performance varied under dual- and multi-task conditions.
Conclusion
The findings highlight differences between dual- and multi-task protocols and add to the understanding of balance performance in older adults under cognitive and physical loads.
Application
The present study highlights differences between dual- and multi-task methodologies that need to be considered in future studies of balance and control in older adults.
Introduction
Falls are among the most common and serious problems in older adults (American Geriatrics Society, British Geriatrics Society, & American Academy of Orthopaedic Surgeons Panel On Falls Prevention, 2001; Asghari Jafarabadi et al., 2018; van Iersel et al., 2007). In the United States, there were 24,190 fatal and 3.2 million medically treated nonfatal fall-related injuries among persons aged ≥65 years in 2012 (Burns et al., 2016). Direct medical costs of fall-related injuries were $616.5 million for fatal and $30.3 billion for nonfatal injuries in that year, which increased to $637.5 million and $31.3 billion, respectively, in 2015 (Burns et al., 2016). In addition to physical injury, falls can also have psychological and social consequences such as post-fall anxiety syndrome, fear of falling, and loss of self-confidence and functional independence (Ambrose et al., 2013; American Geriatrics Society, British Geriatrics Society, & American Academy of Orthopaedic Surgeons Panel On Falls Prevention, 2001). The risk of falling and of being seriously injured in a fall increases with age due to physiologic and pathologic changes (Ambrose et al., 2013). With the expected rapid increase in the aging population worldwide, there is a clear need to better understand the factors associated with falls in older adults to develop interventions for fall prevention in this population.
A number of factors can contribute to falls in older adults. Gait and balance impairments have been identified as major risk factors for falling in this population (Ambrose et al., 2013; American Geriatrics Society, British Geriatrics Society, & American Academy of Orthopaedic Surgeons Panel On Falls Prevention, 2001; Deandrea et al., 2010; van Iersel et al., 2007). Older adults have stiffer and less-coordinated gaits than young adults and may be less capable of weight shifting or taking a rapid step to avoid falls when their balance is perturbed (Ambrose et al., 2013). People often do several things simultaneously during standing or walking in daily life and many falls occur during the performance of such simultaneous tasks (van Iersel et al., 2007). This phenomenon can be explained by the fact that performing a secondary task interferes with balance control, probably through divided attention (e.g., ability to carry out more than one task at the same time such as dual tasking; Ambrose et al., 2013; Holtzer et al., 2007). For this, dual-task methodology has been used in a number of studies to understand the principles of postural control (Al-Yahya et al., 2011; Pellecchia, 2003; Smith-Ray et al., 2015; van Iersel et al., 2007).
Studies on the interaction between attention and postural control under a dual-task paradigm have yielded conflicting results depending on the task type and difficulty as well as individuals’ age (Berger & Bernard-Demanze, 2011; Lindenberger et al., 2000; Pellecchia, 2003; Springer et al., 2006). Additionally, motor cognitive dual-task performance in previous studies generally involves simultaneous completion of a simple physical/motor task (e.g., walking) and a secondary cognitive task (e.g., counting backward, digit reversal or classification, and presenting word lists for memorization). However, many daily and occupational activities require multi-task performance (e.g., multiple physical and cognitive demands). For instance, people have to lift or carry loads as part of their daily routine or occupation. Currently, there is limited knowledge regarding the effects of carrying loads of different weights on the balance performance of older adults under multi-task conditions. It is important to consider how carrying loads of different weights along with cognitive activity as a measure of multi-task condition impacts the older adults’ balance performance. Research to be conducted on this issue will have important implications in terms of the elderly balance and control under cognitive load (CL) and physical load (PL).
On the basis of the above-mentioned background, the objective of this study was to examine the effects of cognitive (to speak out the name of the weekdays in a reverse order) and physical (with three levels including handling weights of 1, 2, and 3 kg in each hand) loads on dynamic and static balance of a sample of older adults (aged 60 years and over) under single-, dual-, and multi-task conditions.
Materials and Methods
Participants
Study participants consisted of 42 older adults (21 males and 21 females) aged 60 years and over. The required sample size was calculated based on the mean difference as the effect size in the outcomes (e.g., dynamic and static balance measures) and factors (e.g., CL and PL) evaluated in the study, considering a 95% confidence level and a power of 80%. The primary information on the main outcome was obtained from the study by Shumway-Cook et al. (2000). The study participants were selected through random sampling from the elderly who were under the coverage of an aging friendly center located in Tabriz, Iran. The Mini-Mental Status Examination cognitive test was applied for screening of cognitively impaired cases and those volunteers scoring <23 on this test were excluded (Folstein et al., 1975). Other inclusion criteria were being 60 years or older, having no musculoskeletal injury, not using an assistive device for walking, and being able to carry loads (up to a weight of 3 kg in each hand). Participation in the study was on a voluntary basis and the participants were told that they were free to withdraw from the research at any time. Each participant signed a written consent form before participation. The study protocol was reviewed and approved by the ethical review committee of the Tabriz University of Medical Sciences.
Experimental Design
Two dependent variables evaluated in the study were (1) dynamic balance, by using the Timed Up and Go (TUG) test, and (2) static balance, by using a stabilometer. Independent variables were CL and PL as well as gender and age of participants. To perform the CL, each participant was instructed to speak out the name of weekdays in a reverse order as accurately as possible. The names of weekdays were presented randomly to avoid learning/memorization effect (Qu, 2013). The PL had three levels and consisted of handling weights of 1, 2, and 3 kg in each hand (2, 4, and 6 kg in total). This weight limit was chosen to simulate the load carriage in daily life.
Data Collection
Data were collected by using questionnaire, personal interview, and experimental tests (for evaluation of dynamic and static balance performance). Participants were asked to complete a personal information questionnaire before undertaking the experimental tests. The questionnaire included demographic details including age, gender (male, female), education level (primary/secondary, diploma, undergraduate, postgraduate), marital status (single, married), living condition (living with family or alone), and having chronic disease as well as other information such as illness history, sleep condition (asking “How is your sleep in general? good, not good”), and history of falling during the past few months (no, yes). The participants were asked to refrain from physical activity for 24 hr before undertaking the test.
The TUG test was used to measure the dynamic balance of participants. The TUG is a commonly used test in older adults as it is easy to administer and can be completed by the majority of participants (Ambrose et al., 2013). It uses the time required by a participant to rise from a chair, walk 3 m, turn around, walk back to the chair, and sit down. During the tests, the participants were instructed to wear their regular footwear (Ambrose et al., 2013). Each TUG trial was performed once, with a 3-min rest break after each trial. The time taken to complete this test (in seconds) was measured using a stopwatch.
A purpose-built stabilometer (Danesh Salar Iranian Co., Tehran, Iran) was used to measure the static balance. This type of stabilometer has been shown to be valid and reliable in measuring static balance (Mosadegh et al., 2017). Measurements were taken while the participants were standing on both feet on the stabilometer platform (40 × 40 cm). Participants were instructed to stand in an upright standing posture on the stabilometer platform for 30 s with eyes open. They were instructed to stand with their feet flat and look at a point that was in front of their eyes during each trial. The stabilometer sway index (SM.SI in %), which is the numerical value of the standard deviation of the distance the participant moved away from the center of balance (Larcom, 2013), was used as a measure of static balance in this study. Three repetitions of static balance measurements were made for each test condition (with a 20-s rest break between successive measurements), and their average value was used for subsequent analysis.
Procedure
On arrival, participants were given instructions about the aims and procedures of the study. The test equipment was then introduced and any questions were answered by the investigator. All participants were familiarized with the stabilometer and TUG tests by practicing them before undertaking the actual tests. Each participant performed 16 different experimental conditions as follows: 2 single tasks (TUG test and stabilometer test), 8 dual-task conditions (TUGCL, TUG2kg, TUG4kg, TUG6kg, stabilometerCL, stabilometer2kg, stabilometer4kg, and stabilometer6kg), and 6 multi-task conditions (TUGCL+2kg, TUGCL+4kg, TUGCL+6kg, stabilometerCL+2kg, stabilometerCL+4kg, and stabilometerCL+6kg). The order in which the two tests (TUG and stabilometer) were presented was randomized across participants. The order of presentation of the loads (cognitive and physical) was also randomized between the participants. The participants were given no feedback regarding their performance during the trials. Data were collected between 9:00 and 12:00 a.m. in a lab environment. The experimental tests were carried out during a single session and took approximately 1 hr to complete for each participant.
Statistical Analysis
Data analysis was performed with the SPSS v.23 (IBM Corp., Armonk, NY, USA). A mixed model analysis of variance (mixed model ANOVA) with repeated measures design was used for evaluation of the main effects of CL and PL as well as gender and age and their interaction on the dependent variables of the dynamic and static balance performance measures. In this model, the parameters were estimated by restricted maximal likelihood method and covariance structure was selected as compound symmetry based on Akaike’s Information Criteria. This was followed by Sidak’s post hoc tests on adjusted means to explore the effects in more detail. p < .05 was considered as significant level for all statistical tests.
Results
Demographic D ata
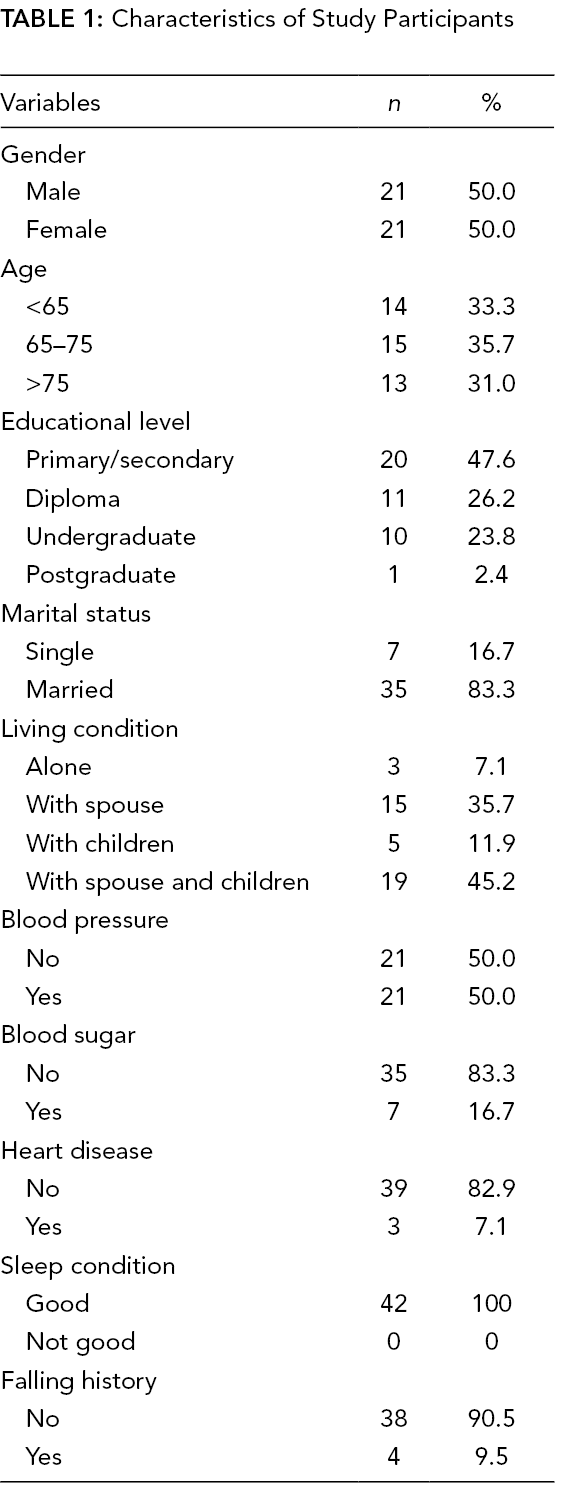
The demographic details of the study participants are presented in Table 1. Their age ranged from 60 to 85 years (mean = 69.2 years; SD = 13.6 years). The majority of participants were married (83.3%). Among them, 47.6% had a primary/secondary degree, 26.2% had a diploma, and 23.8% had an undergraduate degree. Only 7.1% of them reported that they live on their own, while the rest lived with their spouse (35.7%), children (11.9%), or both (45.2%). Their major health problem was blood pressure (50%) and the majority of them (90.5%) indicated that they had no history of falling.
Characteristics of Study Participants
Gender and Age Effects
The ANOVA results showed significant differences between males and females in terms of the TUG performance (p < .05), but not the stabilometer index. The TUG speed of female participants (mean = 10.2 s; SD = 2.0 s) was slower than that of male participants (mean = 9.3 s; SD = 1.3 s). The results showed no significant difference in the TUG and sway index scores in terms of the age of participants. No significant interaction was found between gender and age in relation to balance performance measures.
Dynamic Balance Performance
The results of mixed model ANOVA (Table 2) showed significant differences among tasks for dynamic balance performance (p < .001). The mean time to complete the TUG in different test conditions ranged from 8.8 to 11.1 s. According to Sidak’s post hoc test, the mean time for the single-task TUG (8.8 s) was significantly faster than the TUGCL (9.5 s) condition. The mean completion time for the TUGCL (9.5 s) was significantly faster than those for the TUGCL+4kg (10.7 s) and TUGCL+6kg (11.1 s) conditions. The mean times required to complete the single-task TUG (8.8 s), TUG2kg (9.0 s), TUG4kg (9.2 s), and TUG6kg (9.3 s) were significantly faster than those for the TUGCL+2kg (9.9 s), TUGCL+4kg (10.7 s) and TUGCL+6kg (11.1 s) conditions.
Descriptive Statistics and ANOVA Results for Evaluation of the Effects of Cognitive and Physical Activities on the Dynamic and Static Balance
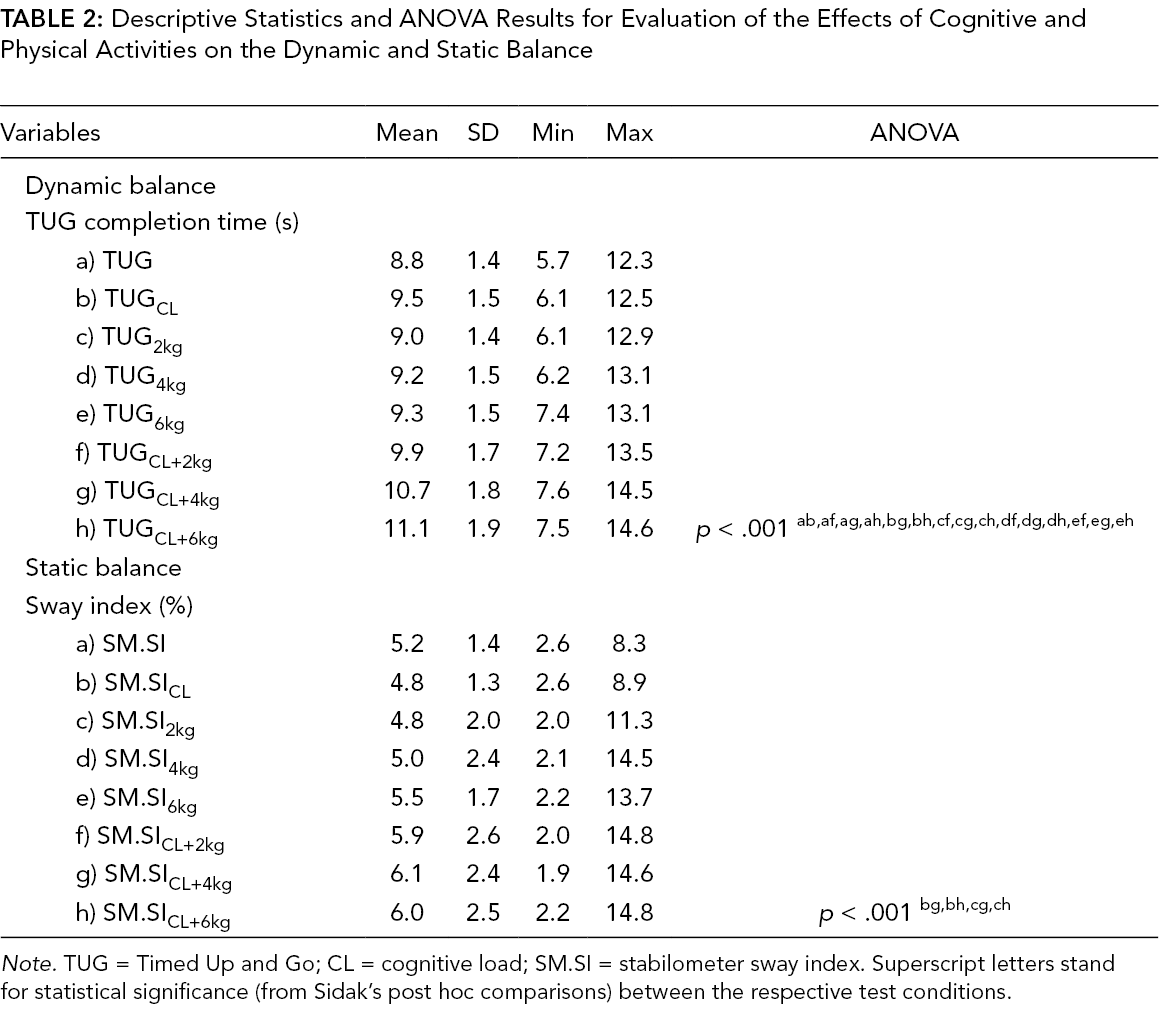
Note. TUG = Timed Up and Go; CL = cognitive load; SM.SI = stabilometer sway index. Superscript letters stand for statistical significance (from Sidak’s post hoc comparisons) between the respective test conditions.
Static Balance Performance
The ANOVA results also showed significant differences among tasks for static balance performance (p < .001; Table 2). The mean values of SM.SI in different test conditions ranged from 4.8% to 6.1%. The post hoc test indicated that SM.SICL (4.8%) and SM.SI2kg (4.8%) were significantly lower than SM.SICL+4kg (6.1%) and SM.SICL+6kg (6.0%) conditions. No other significant differences were found between test conditions.
Discussion
Previous research on postural control in older adults has generally used dual-task methodology, whereas much less attention has been paid to multi-task performance, despite its importance in many daily and occupational activities in this population. The main objective of the present study was to examine the effects of CL and PL on dynamic and static balance performance of older adults under single-, dual- and multi-task conditions. The main findings of the study were that the addition of a secondary CL decreased the dynamic balance performance, while the dual-task conditions had no influence on the static balance performance. The pattern of CL and PL effects on dynamic balance performance was also varied under dual- and multi-task conditions. The dynamic balance (assessed by the TUG test) of females was worse than that of males, while there was no significant difference in balance performance measures in terms of the age of participants. It is possible that gender differences in TUG performance might result from anthropometric variations (e.g., shorter stature or leg length in females rather than males), although this possibility needs further investigation. The findings can help to better understand the factors influencing balance and control in older adults under CL and PL.
With regard to the effects of dual tasks, it was found that the CL had a deleterious effect on the dynamic balance performance, while the effects of various levels of PL were not significant. The addition of a secondary CL increased the TUG completion time by 9%, while the corresponding values for three levels of PL ranged from 2% to 5%. This is not in agreement with the findings of Shumway-Cook et al. (2000), who reported that both cognitive and manual secondary tasks were predictors of falls in older adults. In fact, the manual task used in the study by Shumway-Cook et al. (2000) included carrying a full cup of water, which was mainly a measure of upper-extremity motor task, rather than being a physical one used in the present research, and this may explain the difference in their results from ours. Our findings suggest that CLs would affect dynamic balance more than PLs under dual-task conditions. Nevertheless, our findings support the results of the study by van Iersel et al. (2007) who evaluated the effect of different cognitive dual tasks on balance during walking in physically fit elderly people and found an increase in body sway under cognitive dual-task conditions compared to during walking without dual tasks. Additionally, none of the dual tasks in our study influenced the static balance performance of the participants. In one attempt, Pellecchia (2003) conducted a study to determine whether postural sway varies with the difficulty of a concurrent unrelated cognitive task. The author evaluated postural sway under four experimental conditions, including (in order of increasing difficulty) quiet standing, standing combined with digit reversal, standing and 2-bit classification, and standing and counting backward by 3s. She found that attentional demands of the cognitive task influenced postural sway, with the most difficult cognitive task having the greatest impact. The higher difficulty levels of cognitive tasks in that study compared to our study may explain the differences in the results. Nevertheless, the present study highlights the importance of physical aspects (e.g., varying levels of PL combined with CL) in multi-task conditions as one of the factors influencing the balance performance.
According to our findings, the dynamic balance (evaluated using the TUG test) was generally more affected by the study variables than did the static balance measure (evaluated by the sway index of the stabilometer test) under dual-task conditions. More specifically, when it comes to the dynamic balance, it seems that cognitive demand is more problematic than PL in this population. This is of particular interest since cognitive functioning plays an important role in gait and balance (Al-Yahya et al., 2011; Smith-Ray et al., 2015), and as noted earlier it is one of the contributing factors to falls in older adults. Considering the fact that fall injuries are one of the leading causes of health problems among the elderly worldwide, these findings can be used to develop appropriate injury surveillance and prevention programs. The findings clearly suggest that, as far as the dual tasks are concerned, careful attention should be paid to the cognitive status of the older adults in fall prevention programs. In this regard, several investigators have proposed the benefits of cognitive training programs as one of the possible interventions to improve balance and gait, thereby reducing falls in older adults (Li et al., 2010; Smith-Ray et al., 2015).
One of the major contributions of the present study is to report the effects of multi-task condition on balance performance of older adults. As shown in this study, both dynamic and static balance measures were more influenced by multi-tasks (f, g, and h conditions in Table 2) than by other test conditions. When performing the multi-tasks, a decrease in the dynamic balance performance was observed as the level of PL increased. The time required to complete the TUGCL+2kg, TUGCL+4kg, and TUGCL+6kg conditions was increased by 12%, 21%, and 26%, respectively, compared to the single-task TUG. This is despite the fact that various levels of PL under dual-task conditions had no effect on the dynamic balance performance. Taken together, these findings may suggest that the effects of CL/PL on dynamic balance performance may vary greatly under dual- and multi-task conditions. These findings highlight the combined effects of CL and PL during multi-task performance, which may not be apparent under dual-task conditions. It seems that multi-task protocols may provide a more realistic insight into the effects of CL and PL on balance performance than dual-task methods. These findings clearly indicate how increasing the task difficulty (in terms of PL) can lead to impaired balance performance in older adults. It therefore appears that the risk of falling in older adults may be increased while performing a multi-task compared to when doing a dual task. This is perhaps not surprising as the multi-task condition imposes combined cognitive and physical demands on the individuals as compared to performing single or even dual cognitive or physical tasks.
The results presented here regarding the effects of CL and PL on the balance performance of older adults are based on experimental conditions that were examined in this study, and therefore the findings may not be generalizable to the population at large. For instance, the CL had only a single level of difficulty unlike the PL. Thus, it would seem advisable in future research to consider the effects of various levels of CL. Additionally, the use of TUG in this study confirmed the value of this test in assessing dynamic balance in elderly participants. Other studies have also shown that doing a dual task affects people’s balance and concluded that TUG with dual task can be considered as a good measure to evaluate balance and risk of falling in the elderly (Laessoe et al., 2008; Lundin-Olsson et al., 1998; Shumway-Cook et al., 2000). These findings can have important clinical implications. In this regard, Shumway-Cook et al. (2000) concluded that older adults who take longer than 14 s to complete the TUG have a high risk for falls. However, the time values may vary greatly depending on variability in measures, methodologies, and individuals, and therefore uniform protocols or criteria may be required. Therefore, further research is required to generalize the findings.
Conclusions
The findings of this study add to the understanding of the effects of performing single-, dual-, and multi-task conditions on dynamic and static balance performance of older adults. The results showed significant impact of gender, but not age, on the dynamic balance performance. Under dual-task conditions, only CL influenced the dynamic balance performance, while the PL levels had no effect. The dual-task conditions had no effect on the static balance performance. The effects of CL and PL on dynamic balance performance varied under dual- and multi-task conditions, which highlight the differences between the two protocols.
Key Points
Addition of a secondary CL decreased dynamic balance performance, while dual-task conditions had no influence on static balance performance.
Effects of CL and PL on dynamic balance performance varied under dual- and multi-task conditions.
The dynamic balance of females was worse than that of males, while age had no effect on balance performance measures.
Footnotes
Author Biographies
Hamid Allahverdipour is a professor and academic member of the Health Education & Promotion Department in Tabriz University of Medical Sciences, Iran, and holds a PhD in health education from Tarbiat Modarres University, 2001. His research focuses on a number of health-related topics including geriatrics health.
Iman Dianat is a professor and academic member of the Occupational Health and Ergonomics Department in Tabriz University of Medical Sciences, Iran, and holds a PhD in ergonomics from the University of Nottingham, 2009.
Galavizh Mameh holds an MSc in elderly health from the Department of Health Education & Promotion in Tabriz University of Medical Sciences, 2018.
Mohammad Asghari Jafarabadi is a professor and academic member of the Biostatistics & Epidemiology Department in Tabriz University of Medical Sciences, Iran, and holds a PhD in biostatistics from Tarbiat Modarres University, 2010.