
Abstract
Objective
The purpose of this study is to uncover and catalog the various practices for delivering and disseminating clinical performance in various Veterans Affairs (VA) locations and to evaluate their quality against evidence-based models of effective feedback as reported in the literature.
Background
Feedback can enhance clinical performance in subsequent performance episodes. However, evidence is clear that the way in which feedback is delivered determines whether performance is harmed or improved.
Method
We purposively sampled 16 geographically dispersed VA hospitals based on high, low, consistently moderate, and moderately average highly variable performance on a set of 17 outpatient clinical performance measures. We excluded four sites due to insufficient interview data. We interviewed four key personnel from each location (n = 48) to uncover effective and ineffective audit and feedback strategies. Interviews were transcribed and analyzed qualitatively using a framework-based content analysis approach to identify emergent themes.
Results
We identified 102 unique strategies used to deliver feedback. Of these strategies, 64 (62.74%) have been found to be ineffective according to the audit-and-feedback research literature. Comparing features common to effective (e.g., individually tailored, computerized feedback reports) versus ineffective (e.g., large staff meetings) strategies, most ineffective strategies delivered feedback in meetings, whereas strategies receiving the highest effectiveness scores delivered feedback via visually understood reports that did not occur in a group setting.
Conclusions
Findings show that current practices are leveraging largely ineffective feedback strategies. Future research should seek to identify the longitudinal impact of current feedback and audit practices on clinical performance.
Application
Feedback in primary care has little standardization and does not follow available evidence for effective feedback design. Future research in this area is warranted.
Audit and feedback (A&F, providing recipients with periodic summaries of their performance) has become a widely spread quality improvement (QI) tool for changing clinician behavior, and is an important way to guide individuals’ actions and decisions (Institute of Medicine (US) Committee on Quality of Health Care in America, 2000). According to feedback intervention theory (FIT; Kluger & DeNisi, 1996) and its more clinically focused sibling, CP-FIT (Brown et al., 2019), A&F works by providing clinicians with knowledge of their performance results, thus redirecting attention to the details of the task of interest (Dougherty & Conway, 2008). A&F has been used and shown to improve quality of care in a wide variety of healthcare settings; for example, a meta-analysis by Tannenbaum and Cerasoli (2013) found that feedback in the form of debriefs enhances both individual and team performance in subsequent performance sessions by as much as 25%. A&F has also been shown to improve both proximal and distal behaviors that impact quality of care, such as prescribing behavior and diabetes management.
The effectiveness of this QI intervention, however, is highly dependent on the presence of specific design features incorporated into the intervention (Ivers et al., 2012). For example, meta-analytic research indicates that features such as the format (e.g., written), content elements such as correct-solution information, appropriate comparators, data at the correct level of aggregation, and frequent feedback close in time to the behavior being observed yield significantly better results than A&F interventions without such features (Hysong, 2009). Other research also points to the absence of and need for using theory in the design of A&F to create a tool that works best for the given context in question. Together, these point to a portfolio of evidence-based best practices for design and delivery of A&F in clinical settings.
A&F has begun to more explicitly incorporate theory and evidence-based characteristics and features in their design; what is far less known is the extent to which these evidence-based best practices have been translated into everyday practice. To that end, this study aims to describe the types and prevalence of A&F strategies employed in a national sample of Veterans Health Administration (VHA) primary care practices, and assess the extent to which the strategies observed align with evidence-based best practices for A&F as reported in the literature.
Method
Design
Part of a larger study of A&F, this research consists of qualitative, primary analysis of telephone interviews with facility leadership and primary care personnel at 16 U.S. Department of Veterans Affairs Medical Centers (VAMCs), employing a cross-sectional design with purposive sampling guided by preliminary analyses of clinical performance data. Methods for this work have been described extensively elsewhere (Hysong et al., 2012) and are summarized here.
Site Selection
Sites were selected using a purposive stratified approach based on their scores on a profile of 15 outpatient clinical performance measures extracted from VHA’s External Peer Review Program (EPRP) representing five domains: diabetes care (five measures), hypertension care (two measures), immunizations (two measures), cancer screening (three measures), and tobacco use (three measures). EPRP is a nationally abstracted database containing performance data for all VHA medical facilities on over 90 indicators covering access, quality of care, cost-effectiveness, and patient satisfaction domains. Data are abstracted monthly, but reported quarterly, to facility leadership, who then disseminate as they deem necessary. We refer interested readers to our published protocol paper (Hysong et al., 2012) for further details about these measures.
We selected four high-performing, four low-performing, four consistently moderately performing (i.e., those with moderate average performance and the lowest variability across measures), and four moderate, yet highly variably-performing facilities (i.e., those with moderate average performance and the highest variability across measures; Hysong et al., 2012). Sites were selected based on their treatment of chronic and preventive care for two primary reasons: one is so that feedback regarding a specific set of patients can be implemented (e.g., likelihood of opportunity to implement feedback is greater than acute care settings) and the second is that patient acuity may be lower, inducing lower workload and increasing likelihood for learning from feedback to transfer to the work environment (Holton & Baldwin, 2003; Sweller, 1988).
Participants
We interviewed up to four participants at each of 16 geographically dispersed VAMCs, drawn from the following groups: the facility director, the associate chief of staff (ACOS) for primary care, one full-time primary care physician and/or physician extender, and one full-time primary care nurse. Table 1 summarizes which roles were interviewed at each facility.
Site Characteristics and Roles Interviewed at Each Site
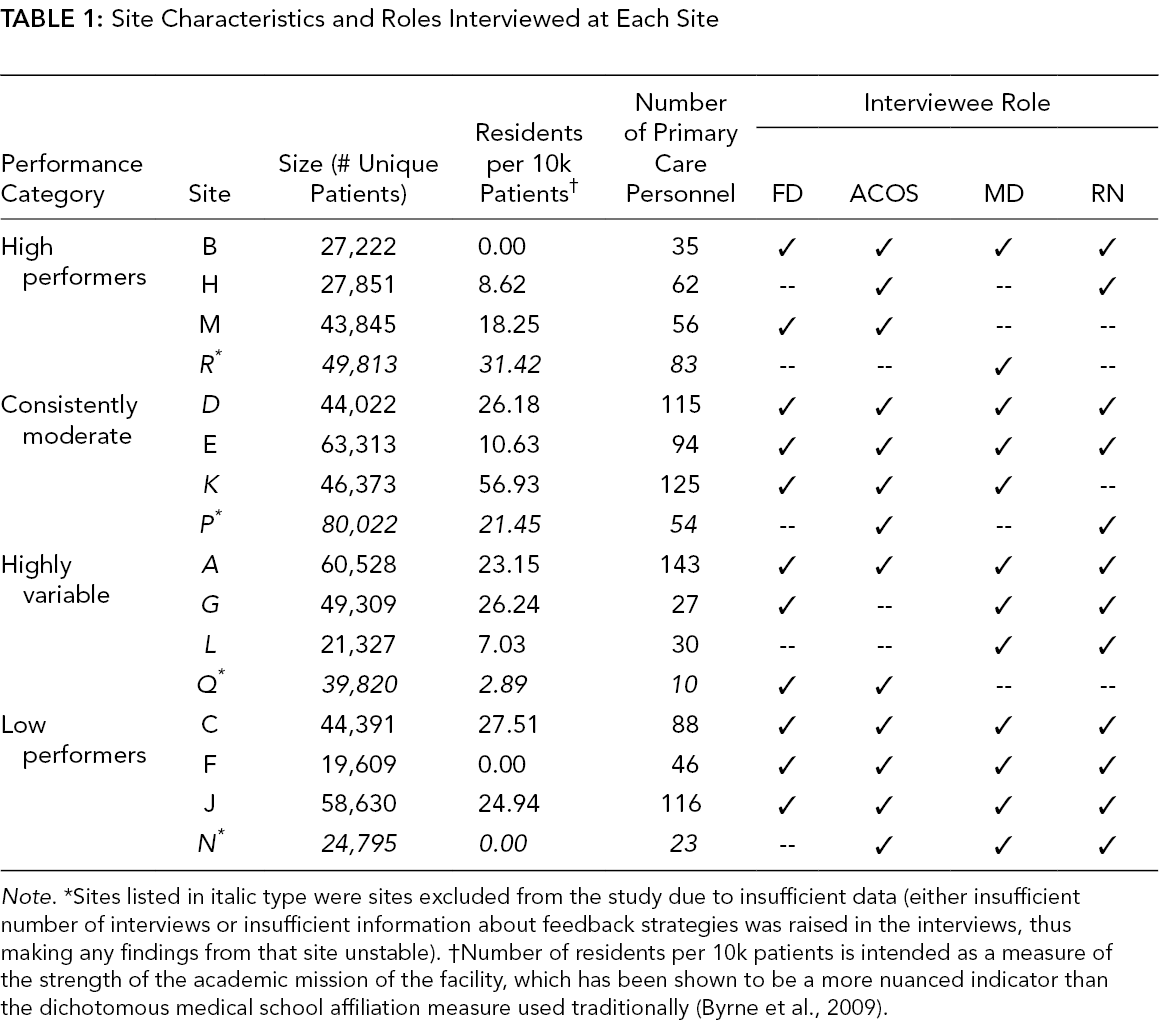
Note. *Sites listed in italic type were sites excluded from the study due to insufficient data (either insufficient number of interviews or insufficient information about feedback strategies was raised in the interviews, thus making any findings from that site unstable). †Number of residents per 10k patients is intended as a measure of the strength of the academic mission of the facility, which has been shown to be a more nuanced indicator than the dichotomous medical school affiliation measure used traditionally (Byrne et al., 2009).
Procedure
Participants were interviewed individually for 1 h by a research team member at a mutually agreed upon time; interviews were audio-recorded with the participant’s consent. Participants answered questions about (a) the types of EPRP information they receive, (b) the types of quality/clinical performance information they actively seek out, (c) opinions and attitudes about the utility of EPRP data (with specific emphasis on the role of targets), (d) how they use the information they receive and/or seek out, and (e) any additional sources of information or strategies they might use to improve the facility performance.
Data Analysis
Interview recordings were transcribed and analyzed using techniques adapted from grounded theory (Strauss & Corbin, 1988) and content analysis (Weber, 1990) using Atlas.ti, a qualitative analysis (Hwang, 2008) software program.
Strategy domains, dissemination methods, and prevalence
Each unique strategy for providing feedback found in interviews was assigned a code to observe its prevalence in the data. As several individual feedback strategies were uncovered, we further grouped strategies by the dissemination mechanisms through which feedback was delivered: computerized delivery, written reports, meetings, and conversations. Dissemination method(s) offer detail on how performance measures are delivered to providers when they do receive said feedback. The most frequently used strategies may not align with best practices and most effective strategies; thereby, we also identified the most frequently used strategies to provide contextualized guidance for enhancing A&F strategies.
Alignment with evidence-based best practice
Finally, to assess how well a given strategy followed evidence-based best practices, each feedback strategy was evaluated against each of the feedback cues (characteristics) demonstrated by previous research to either improve or hinder feedback effectiveness (Hysong et al., 2006; Kluger & DeNisi, 1996). We calculated a “feedback richness score” for each strategy derived from guidelines produced by Kluger and DeNisi (1996)’s (1996) FIT in combination with Hysong et al.’s (2006) principles for effective feedback by subtracting the number of characteristics that hinder feedback effectiveness (ineffective cues) from the number of characteristics that improve feedback effectiveness (effective cues; please see Supplemental Material 1).
Results
Strategy Domains and Prevalence
We found 102 feedback strategies used by our sample of sites; we further identified four primary delivery types through which feedback (i.e., computerized delivery [n = 1], reports [n = 12], meetings [n = 23], and conversations [n = 13]; please see Supplemental Material 2).
Most Frequently Occurring Feedback Strategies
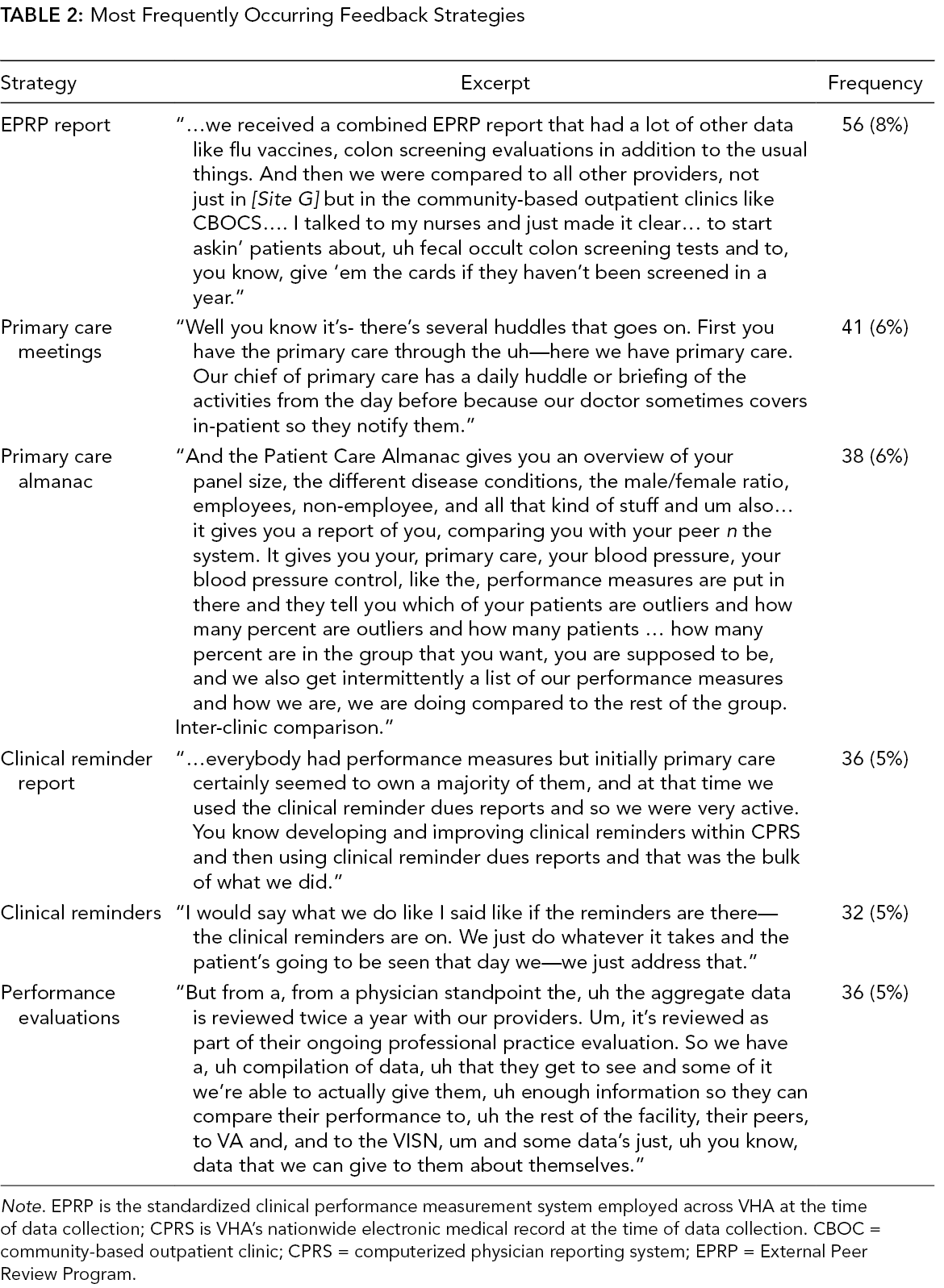
Note. EPRP is the standardized clinical performance measurement system employed across VHA at the time of data collection; CPRS is VHA’s nationwide electronic medical record at the time of data collection. CBOC = community-based outpatient clinic; CPRS = computerized physician reporting system; EPRP = External Peer Review Program.
Alignment With Evidence-Based Best Practice
Feedback strategies receiving the highest richness score(s), all of which received a richness score of 2 (out of a possible 10), disseminate information to clinic staff through use of visual means. Among these, clinical reminder report poster(s) (defined as a poster displayed where clinical staff members can see it that displays data on clinically relevant metrics derived from data available through the clinical reminders) and provision of relevant reports of performance on EPRP measures. EPRP reports providing feedback at the individual and clinic level are considered to be higher in richness than other means of providing EPRP reports. Conversely, several excerpts demonstrating low quality, ineffective strategies emerged from the data. The strategies receiving the lowest richness score include providing feedback to individuals during primary care nurse meetings (richness score of −6) and delivering feedback during meetings with providers who fall below par on the current clinical EPRP measures (richness score of −4). Other low-quality and seemingly less effective strategies emerging from the data include disseminating feedback during morning meetings (richness score of −2) and delivery of feedback during performance measure meetings (richness score of –3). Most ineffective strategies delivered feedback in meetings, whereas strategies receiving the highest richness score(s) did not occur in a group setting (i.e., individually); further, most effective strategies delivered feedback via visually understood reports that did not occur in a group setting (Table 3).
Strategy Categorizations and Richness Scores
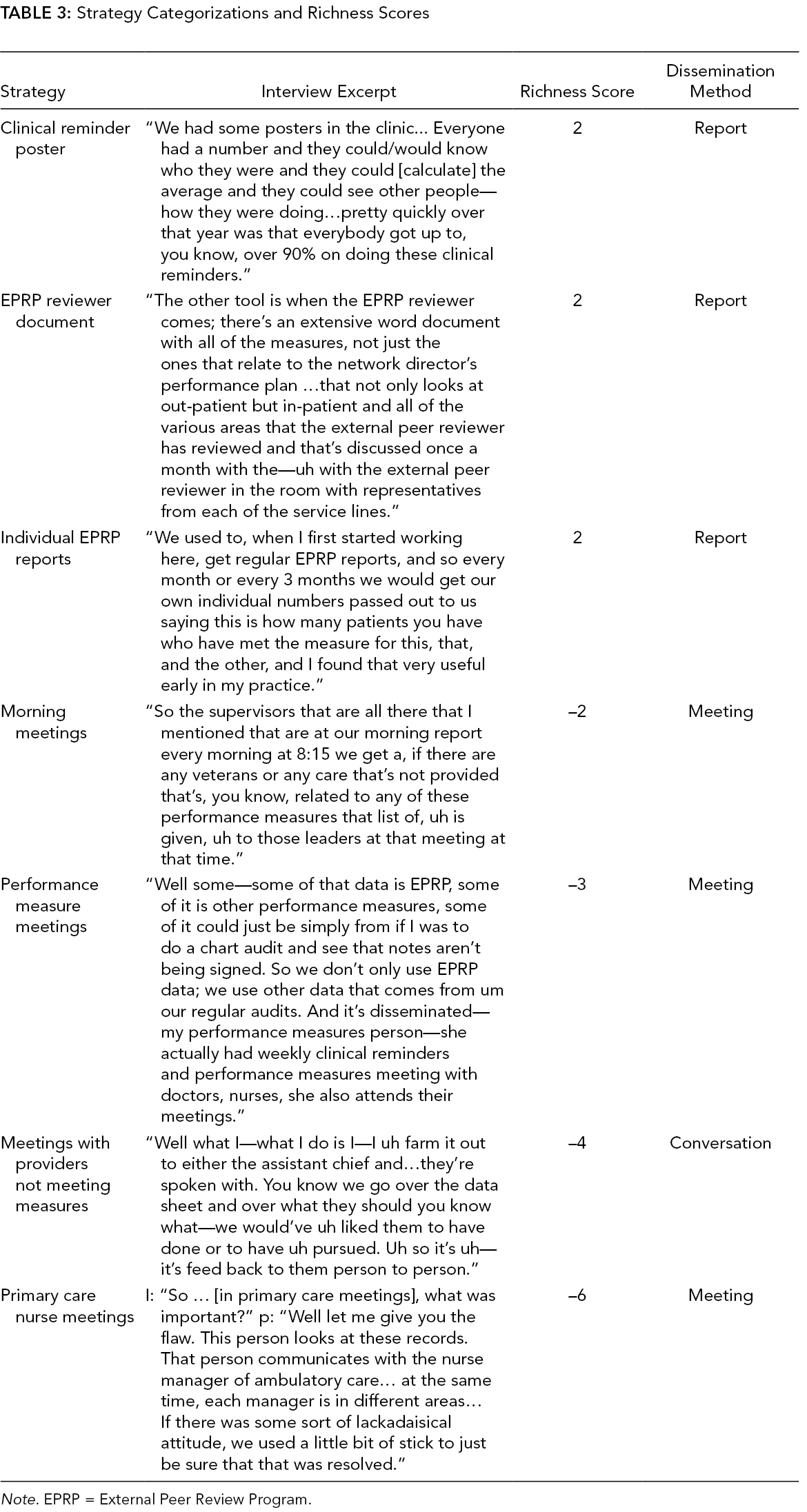
Note. EPRP = External Peer Review Program.
Strategy Dissemination
For added guidance and perspective, we analyzed overall effective versus ineffective strategies as categorized by their dissemination methods. Among these dissemination methods, ineffective strategies had a broad range of dissemination methods, including information regarding A&F delivered via meetings (n = 17), conversations (n = 9), reports (n = 5), and computer interface (n = 1). In the more effective dissemination strategies, feedback was typically delivered to recipients via reports (n = 7), meetings (n = 6), and conversations (n = 5). No significant differences in dissemination method prevalence were noted between ineffective and effective strategy types (χ2 = 3.66, p = .30).
Discussion
In this paper, we sought to describe the types and prevalence of A&F strategies employed in a national sample of VHA primary care practices and assess the extent to which the strategies observed align with evidence-based best practices for A&F. We found great variability in the quality and frequency of feedback strategies across sites and found that the feedback strategies employed by most sites exhibited characteristics shown in the literature to make feedback less rather than more effective (Kluger & DeNisi, 1998). Although feedback strategies appear to vary widely, the low utilization of feedback strategies recommended by the scientific literature suggests a need for improvement in the manner in which feedback is delivered in healthcare settings.
This paper contributes to outpatient QI in a number of ways. First, it sheds light on the strategies leveraged in providing feedback in a particular clinical care context (i.e., outpatient care) and provides an indication of the quality and potential effectiveness of strategies employed. For instance, whereas feedback delivered (particularly to low performing care providers) in a group setting received the lowest richness scores, it is also one of the most frequently leveraged methods for providing individual-level feedback on clinical performance (Pedersen et al., 2018). Group meetings may pose a convenient opportunity to provide feedback to providers considering logistics and scheduling. However, most meetings were largely ineffective as a platform for feedback dissemination as receiving negative feedback in the presence of colleagues and peers may spike perceived judgment from fear, enhancing self-focus while receiving feedback on performance (Kluger & DeNisi, 1996, 1998). Interestingly, not all meetings to share feedback were the same. Feedback disseminated via individualized meetings arranged between supervisors and subordinates to discuss objective measures provided tangible evidence as to the current state and a forum free from peer influence or shame as a means to discuss necessary improvements. Reports and dashboards customized to individual provider needs are considered effective for similar reasons, as well as providing opportunity for future review and reference by the clinician. Effectiveness of such reports and feedback meetings can be increased by providing correct-solution information (e.g., providing reminders of preferred evidence-based medications for hypertension displayed alongside hypertension control metrics, or as part of the discussion),
Implications
Findings from this study attest to the quality of the feedback commonly delivered to primary care personnel. This study contributes a deeper knowledge of the current practices used in outpatient settings to disseminate and deliver clinical performance feedback, and how such strategies may be more or less aligned with evidence-based best practices as found in models of effective feedback in the literature. Interestingly, trends across facilities appear to show the uptake of anxiety-provoking feedback techniques, such as providing feedback in front of superiors or colleagues or focusing heavily on negative performance outcomes. Given self-focus and added stress, the literature on A&F suggests these strategies as being largely ineffective (Hughes et al., 2016; Kluger & DeNisi, 1998). Further, the most frequently used strategies do not appear to align with the best practices (Ivers, Grimshaw, et al., 2014; Ivers, Sales, et al., 2014); namely, meetings and use of computer interfaces appear to trump the methods used to disseminate clinical performance to primary care clinicians. Finally, although use of a computer interface to disseminate information may be convenient, more should be done to understand its impact on learner gains from feedback delivered in this manner.
Findings from this paper also contribute to evidence-based practice in team-based settings. While clinical reminders and feedback delivered electronically (e.g., via computer interface) require few added resources and can deliver performance information directly to a learner, the future of healthcare is delivered in teams. For instance, during the completion of this study, VHA outpatient care transitioned to a formalized team-based approach to delivering care in their adaptation of the Joint Commission’s Patient-Centered Medical Home Model (PCMH), Patient-Aligned Care Teams (PACTs). A&F strategies (e.g., debriefs) are critical to healthcare team performance (Gregory et al., 2021; Tannenbaum & Cerasoli, 2013) so that team members, whose work often overlaps considerably (Best et al., 2006), can learn from previous performance episodes. Identifying pertinent A&F practices to outpatient care teams may require unique considerations and as such is another avenue for future research.
Limitations
Although this study is helpful for uncovering practices for delivering clinical performance feedback within VA centers, it is not without limitations. First, we are unable to speak to the impact that a site’s given feedback practices may directly or indirectly have on their clinical performance data; namely, as the studies originally classified as high or low performers were not consistent across time in performance, we were unable to quantify the impact of feedback strategies on performance of a clinic. This may be due to the fact that as strategies varied across and within sites, performance may have fluctuated accordingly over time, making it impossible to link a specific strategy to performance changes (Byrne et al., 2009). Second, although our study aimed, by design, to examine facility-level differences in feedback strategies, new research suggests that variability in clinical performance is more prevalent, and more amenable to change, at the within-facility level. Future research should be directed at a lower level of analysis than that reported here.
Conclusions/Future Directions
Nearly two-thirds of clinical performance strategies currently in use by facilities in our sample are inconsistent with best practices for delivery of A&F. Findings speak to the variety of A&F practices used within the VHA outpatient setting. Future work should examine the effect of these strategies on specific and meaningful clinical performance indices longitudinally and examine A&F practices for outpatient care teams.
Key Points
Audit and feedback interventions are pivotal to fostering learning in health systems.
The quality, variety, and frequency of strategies used to deliver clinical performance feedback in primary care settings vary greatly, at both high- and low-performing VHA facilities.
Our findings suggest that several strategies leveraged for delivering feedback to primary care clinicians were linked to low quality.
Future research should examine impact of specific feedback delivery strategies on clinical performance improvement in individual and team-based healthcare settings.
Supplemental Material
Online supplementary file 1 - Supplemental material for Prevalence of Effective Audit-and-Feedback Practices in Primary Care Settings: A Qualitative Examination Within Veterans Health Administration
Supplemental material, Online supplementary file 1, for Prevalence of Effective Audit-and-Feedback Practices in Primary Care Settings: A Qualitative Examination Within Veterans Health Administration by Sylvia J. Hysong, Richard SoRelle and Ashley M. Hughes in Human Factors: The Journal of Human Factors and Ergonomics Society
Supplemental Material
Online supplementary file 2 - Supplemental material for Prevalence of Effective Audit-and-Feedback Practices in Primary Care Settings: A Qualitative Examination Within Veterans Health Administration
Supplemental material, online supplementary file 2, for Prevalence of Effective Audit-and-Feedback Practices in Primary Care Settings: A Qualitative Examination Within Veterans Health Administration by Sylvia J. Hysong, Richard SoRelle and Ashley M. Hughes in Human Factors: The Journal of Human Factors and Ergonomics Society
Footnotes
Acknowledgments
We would like to thank Kristen Broussard-Smitham, Melisssa Knox, and Thach Tran for their assistance with data collection and analysis for this study. The research reported here was supported by the US Department of Veterans Affairs Health Services Research and Development Service (grant nos. IIR 09–095, CD2-07-0181) and partly supported by the facilities and resources of the VA Center for Innovations in Quality, Effectiveness and Safety (CIN 13-413). Elements of this work were previously presented at the Annual Research Meeting of Academy Health, on Sunday, June 26, 2016. This study was reviewed and approved by the Baylor College of Medicine Institutional Review Board (IRB), protocol #H-20386.
Author(s) Note
The author(s) of this article are U.S. government employees and created the article within the scope of their employment. As a work of the U.S. federal government, the content of the article is in the public domain.
Supplemental Material
The online supplemental material is available with the manuscript on the HF website.
Author Biographies
Sylvia J. Hysong is a lead research health scientist at the Center of Innovations in Quality, Effectiveness and Safety (IQuESt) at the Michael E. DeBakey VA Medical Center and professor at Baylor College of Medicine. Her research interests include primary health care as a work environment, performance measurement and feedback systems, and care coordination in primary care settings.
Richard SoRelle is a research coordinator and health science specialist at the Center for Innovations in Quality, Effectiveness, and Safety (IQuESt) at the Michael E. DeBakey VA Medical Center. His research interests include qualitative social research and health services research and development within primary care settings.
Ashley M. Hughes is an assistant professor in the Department of Biomedical and Health Information Sciences at the University of Illinois at Chicago and a research health scientist at the Center of Innovations for Chronic, Complex Healthcare (CINCCH) at the Edward Hines JR VA Medical Center. She received her PhD in Applied Experimental Human Factors Psychology in 2016 from the University of Central Florida.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.