
Abstract
Objective
The objective of this systematic review was to investigate the potential link between cognitive dissonance or its related constructs (emotional dissonance, emotional labor) and musculoskeletal disorders.
Background
The etiology of musculoskeletal disorders is complex, as pain arises from complex interactions among physical, social, and psychological stressors. It is possible that the psychological factor of cognitive dissonance may contribute to the etiology and/or maintenance of musculoskeletal disorders.
Method
MEDLINE, APA PsycInfo, and CINAHL Plus databases were searched for studies investigating cognitive dissonance or its related constructs as exposure(s) of interest and outcomes related to physical health (including, but not limited to, musculoskeletal pain). Risk of bias was assessed using the Appraisal tool for Cross-Sectional Studies (AXIS) tool.
Results
The literature search yielded 7 studies eligible for inclusion. None of the included studies investigated cognitive dissonance directly but instead investigated dissonance-related constructs of emotional dissonance and emotional labor, in which a mismatch between required and felt emotions might elicit a psychological response consistent with the cognitive dissonance state. Moderate effect sizes between dissonance-related constructs and musculoskeletal disorders were noted (OR 1.25–2.22).
Conclusion
There is likely a relationship between the two factors studied. However, as the included studies were cross-sectional in nature, a causal relationship between cognitive dissonance-related constructs and musculoskeletal disorders cannot be inferred. Therefore, future study proposing and validating a causal pathway between these variables is warranted.
Application
Cognitive dissonance and its related constructs may serve as risk factors for musculoskeletal disorders that have not been considered previously.
INTRODUCTION
Musculoskeletal disorders (MSDs) are typically characterized by injuries of the muscles, nerves, tendons, joints, cartilage, and spinal discs and comprise a number of conditions including chronic low back pain, osteoarthritis, tendonitis, and carpal tunnel syndrome (Bernard, 1997). They are highly prevalent in industrialized societies, affecting over 50% of persons in the United States age 18 and over and nearly 75% of persons in the United States age 65 and older (Weinstein et al., 2018). Moreover, with the aging of the United States population, the prevalence of MSDs and economic burden of treating musculoskeletal pain is only expected to rise in coming years. Of all MSDs, the most prevalent and costly include low back and neck pain (Dieleman et al., 2016; Dunning et al., 2010; Fejer et al., 2006). Low back pain has been recognized as the most disabling medical condition known to affect mankind worldwide (Hoy et al., 2014), while the advent of modern technology (computers, smartphones, tablets, etc.) consistent with office work has begun to shift the problem up into the neck as well (Côté et al., 2008).
The etiology of MSDs is highly complex, and it is now accepted that pain arises from complex interactions among physical stressors, social stressors, psychological stressors, individual factors, and genetics (Hartvigsen et al., 2018). Regarding psychological stressors, most prior research has centered on factors including depression, anxiety, fear-avoidance, and pain catastrophizing (Elbinoune et al., 2016; M. M. Gerrits et al., Penninx, 2015; M. M. J. G. Gerrits et al., 2014; Ortego et al., 2016; Pinheiro et al., 2016; Pinheiro et al., 2015). However, it is likely that another psychological factor (i.e., cognitive dissonance) may also contribute to the etiology and/or maintenance of MSDs, especially low back and neck pain.
Over 60 years ago, psychologist Leon Festinger presented the basic tenants of Cognitive Dissonance Theory. In his seminal publication, Festinger suggested that humans strive for psychological consistency and experience discomfort when considering two or more psychologically inconsistent notions (i.e., thoughts, beliefs, values, emotional reactions, behaviors) at the same time (Festinger, 1957). This discomfort, which has since been titled the cognitive dissonance state (CDS), was hypothesized to persist so long as the cognitive inconsistency remains. Just as the experience of hunger is not satiated without food, Festinger suggested that the CDS is not reduced until psychological consistency is restored (Joel Cooper, 2019). Depending on the magnitude of the CDS experienced, humans may need to expend considerable cognitive and behavioral effort to restore cognitive consistency and subsequently reduce their discomfort. This is most often achieved by changing, trivializing, rationalizing, or altering the cognitions or behaviors that led to the CDS in the first place. For example, a smoker who comes to understand that smoking is detrimental to their health may think things such as “the evidence is weak that smoking causes cancer” (change the cognition), “I don’t smoke that much” (trivialize), or “I smoke but I also exercise (rationalize). Alternatively, he/she may choose to quit smoking altogether (alter behavior).
This, of course, is a rather simplified example. In contrast, there are a milieu of environments, many occupationally related, in which the cognitive dissonance state may be experienced more frequently and/or in which the cognitive dissonance state may be more difficult to resolve. In healthcare settings, for example, practitioners who value providing excellent patient care must come to terms with other factors (e.g., competing priorities, limited resources, limited authority) that prevent them from delivering the quality of care they would like to provide (Cronqvist et al., 2001). Similarly, police officers may become caught between “due process” (i.e., innocent until proven guilty) and “tough on crime” (i.e., clean up the streets) mentalities in their day to day work and experience a cognitive dissonance state in instances in which their behavior is too aggressive or not aggressive enough, respectively (Miller et al., 2000). Alternatively, scientists conducting research on laboratory animals may experience a CDS when weighing the potential long-term benefits of their research against the welfare of the animals they must handle and/or harm on a day-to-day basis (Engel et al., 2020). Finally, the most intense of all examples might relate to the military population, in which veterans report having experienced moral injury and a cognitive dissonance state from perpetuating, failing to prevent, or witnessing acts that violate deeply held moral beliefs and expectations (Braitman et al., 2018; Evans et al., 2018).
Cognitive dissonance may also be relevant to consider alongside related constructs including emotional labor and emotional dissonance. Emotional labor has been defined as the effort, planning, and control required to express organizationally desired emotions (via an external facial or bodily display) during interpersonal transactions (Andrews et al., 2008; Hülsheger & Schewe, 2011). These organizationally desired emotions may be positive or negative, depending on the context. For example, a call center worker or flight attendant may be expected to convey a warm, enthusiastic demeanor with customers, while a debt collector may be expected to convey an angry or detached demeanor with debtors (Simpson & Stroh, 2004). If organizationally desired emotions are consistent with how an employee genuinely feels in that moment, then their emotional display and experienced thoughts and emotions will be consonant. However, an individual may also need to regulate their behavior, including emotional displays, in ways that are incongruent with their experienced thoughts and emotions. The call center worker or flight attendant in the example above might become frustrated by a customer that is making unreasonable demands with a “the customer is always right” mentality. Conversely, the debt collector might actually be sympathetic toward the debtor’s financial situation. When expressed and experienced emotions are at odds with one another, emotional labor escalates to emotional dissonance. Emotional dissonance may be viewed as analogous to the broader construct of cognitive dissonance described above because emotional responses fall under the umbrella of psychological notions just like thoughts, behaviors, values, and beliefs.
Cognitive dissonance remains one of the most highly studied concepts in social psychology. At this moment in time (July 2021), a PubMed search of “cognitive dissonance” returns nearly 1,300 results. Among these results, studies describe in detail how and why the cognitive dissonance state plays a role in the attitudes and beliefs, preferences and preference changes over time, and behavior (Devine et al., 1999; Izuma et al., 2010; Kitayama et al., 2013). Others describe instances in which the cognitive dissonance state is used as a catalyst for behavioral change, such as to better cope with chronic pain (Gilliam et al., 2013; Leake et al., 1999) or stop smoking (Simmons et al., 2013). It is evident, however, that despite decades of research on the topic, the physical manifestations of the cognitive dissonance state are not well understood, particularly those related to musculoskeletal health outcomes.
Given that the experience of the cognitive dissonance state causes increased physiological arousal (J. Cooper, Zanna, & Taves, 1978; Croyle & Cooper, 1983), global physical changes are also expected to occur during the CDS, consistent with the activation of the sympathetic nervous system. Some of these physical changes have been quantified previously and include changes to the galvanic skin response (GSR) or heart rate (Croyle & Cooper, 1983; Etgen & Rosen, 1993; Losch & Cacioppo, 1990). However, these physiological changes have always been quantified as indicators of the cognitive dissonance state, rather than effectors of other physical changes that could still lie downstream. Therefore, while scientists largely understand how and why the cognitive dissonance state shifts our attitudes, beliefs, and even our behaviors, very little is understood about how the CDS may affect other parts of the body. For example, in addition to the physiological changes mentioned above, human physiological stress response (consistent with sympathetic nervous system activation) has also been associated with biomechanical changes, including increased muscle coactivity, reduced motor unit rotation, and increased muscle fatigue (Bloemsaat et al., 2005; Davis et al., 2002; Marras et al., 2000; Minerbi & Vulfsons, 2018). These are all factors that also subsequently increase the risk that an individual might experience myofascial pain or a musculoskeletal disorder like low back or neck pain, as mentioned above (Dommerholt et al., 2006; Granata & Marras, 1995; Jun et al., 2017; Marras et al., 2001).
Given the evidence presented above, it is hypothesized that cognitive dissonance and related constructs may play a meaningful role in the etiology and/or maintenance of musculoskeletal pain that is not yet well understood. If this is the case, cognitive dissonance could be a key factor to consider alongside other psychological factors that are more commonly studied (e.g., depression, anxiety, pain catastrophizing) relative to musculoskeletal pain. The objective of this systematic review was to summarize existing evidence linking cognitive dissonance (and/or the related constructs of emotional dissonance and emotional labor) to musculoskeletal pain. Given the high prevalence of low back and neck pain among all MSDs, our preference was to include studies with low back or neck pain outcome metrics, though we did not explicitly limit our search to these two body regions. Likewise, given the strong association between work-related exposures and MSDs, our preference was to include studies investigating the CDS in a work-related context, though this was not an explicit criterion for inclusion or exclusion, either (see below).
METHODS
Literature Search Strategy
This systematic review considered articles published through July 2021. The literature search was performed in a systematic manner using the EBSCOhost Research Platform and searched MEDLINE, APA PsycInfo, and CINAHL Plus with Full Text databases. Given the study objective, the literature search sought links between cognitive dissonance or its related constructs (emotional dissonance, emotional labor) and words related to musculoskeletal injuries/pain. Thus, the search term used was (dissonance AND pain) OR (dissonance AND injury) OR (dissonance AND musculoskeletal) OR (“emotional labor” AND pain) OR (“emotional labor” AND injury) OR (“emotional labor” AND musculoskeletal).
Screening and Eligibility Criteria
Duplicate results were removed prior to screening. Then, a three-step approach was performed for screening the literature search results. This three-step process first involved screening titles, then screening abstracts, and finally, retrieving and screening the full text. The reference lists of all the articles for which full text was acquired were also scanned to identify any other eligible sources using this same three-step process.
Studies were considered eligible for inclusion if the article was written or translated into English, if the full text was available, if the population studied was purposefully selected because of their likelihood of experiencing the CDS or a related construct (as defined by the authors of that study), if dissonance or a related construct was tested as an independent variable of interest, and if the study reported on any sort of physical health outcome. Biomechanical measures related to musculoskeletal injuries or musculoskeletal pain were preferred physical health outcomes, but studies with physiological and/or metabolic metrics were included as well. Narrative and systematic reviews were excluded, as were any studies that only examined psychological outcomes or changes to work performance.
Data Extraction
A standardized data extraction form was used to acquire all the same basic information on eligible studies. This included information about the: 1. Study Type: epidemiological, laboratory-based, field-based 2. Population: sample size, occupation, gender, age, work experience (where reported) 3. Exposure Details (dissonance-related construct) 4. Relevant Outcome Details (physical health outcomes) 5. Other Predictors or Outcomes Reported.
Then, the results of each of the included studies were examined, with special attention paid to results that provided evidence for or against a link between cognitive dissonance, emotional dissonance, or emotional labor and musculoskeletal complaints, consistent with the study objective. Given that most studies were cross-sectional in nature, the primary summary measures were point prevalence estimates, odds ratios, and correlations.
Assessment of Bias
AXIS Risk of Bias Tool as Described by Downes et al. (2016).
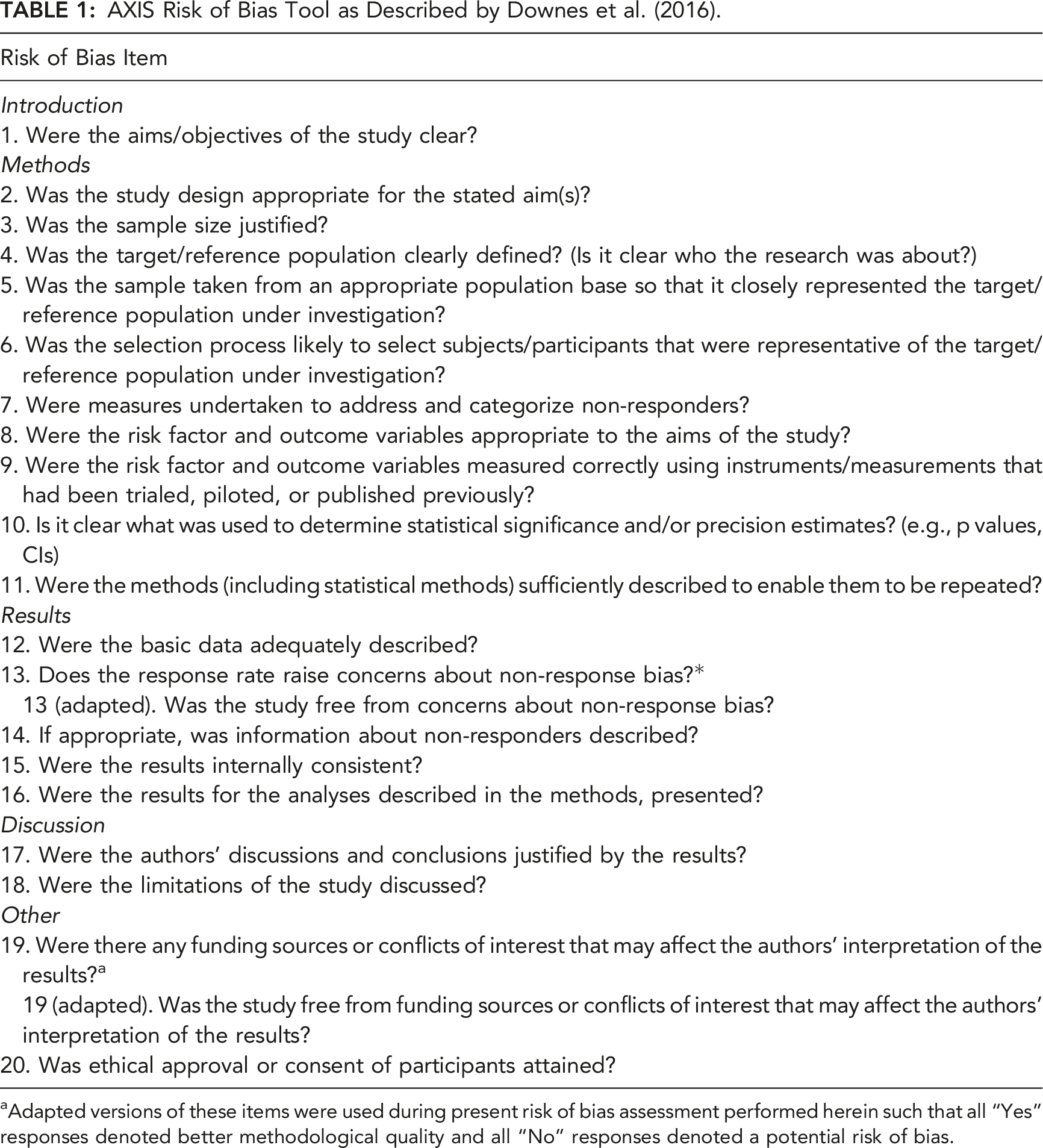
aAdapted versions of these items were used during present risk of bias assessment performed herein such that all “Yes” responses denoted better methodological quality and all “No” responses denoted a potential risk of bias.
RESULTS
Study Selection
As shown in Figure 1, the search yielded 315 results. After removing 78 duplicates, 237 titles were screened for eligibility. Ultimately, after also screening 36 abstracts and 15 full texts, seven studies were selected consistent with the inclusion/exclusion criteria. Reviewing the references of the fifteen full texts did not yield any additional studies for inclusion. Flowchart of the study selection process.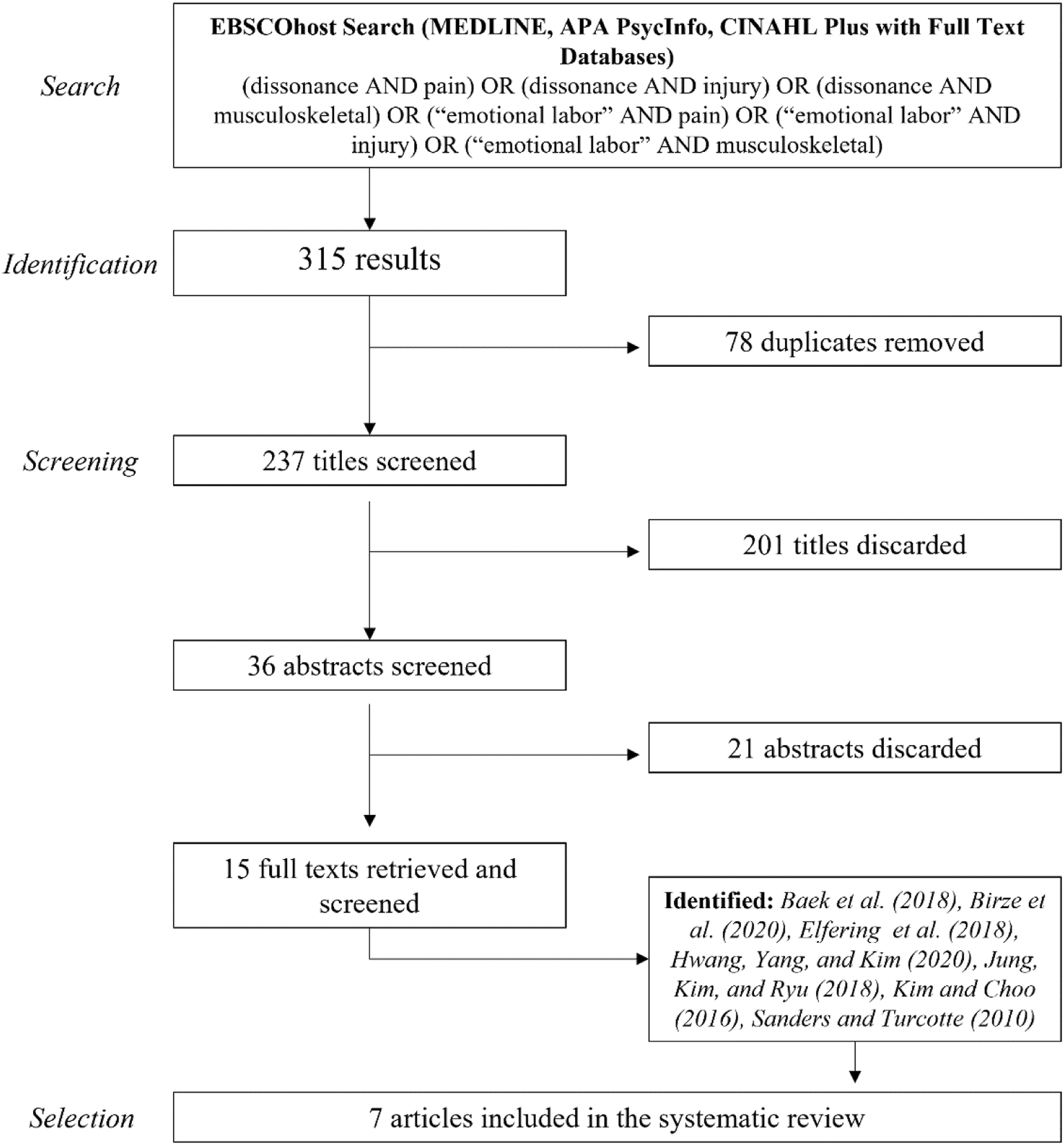
Characteristics of the Studies
Descriptions of the Seven Included Studies.
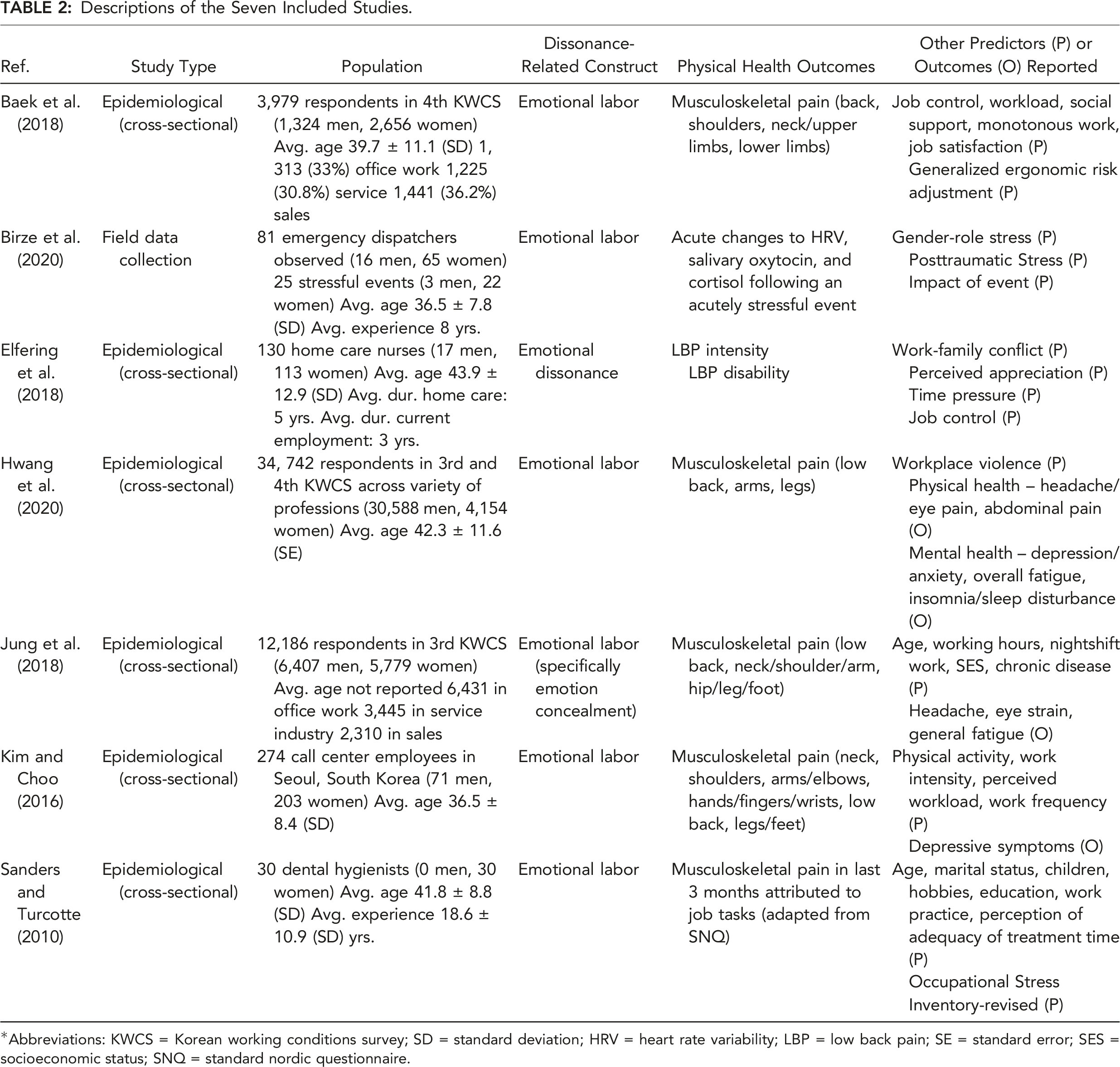
*Abbreviations: KWCS = Korean working conditions survey; SD = standard deviation; HRV = heart rate variability; LBP = low back pain; SE = standard error; SES = socioeconomic status; SNQ = standard nordic questionnaire.
All seven studies investigated dissonance-related concepts as potential predictors of poor outcomes in the context of work-related exposures and outcomes. Together, the population represented by these seven articles is large and heterogeneous. Occupations studied included home health care nurses (Elfering et al., 2018), emergency dispatch workers (Birze et al., 2020), call center employees (Kim & Choo, 2016), dental hygienists (Sanders & Turcotte, 2010), and more. The three studies with the largest study populations relied on data gathered from the Korean Working Conditions Survey (KWCS), which is conducted periodically among workers over 15 years of age in Korea by pen and paper interviewing and captures multiple facets of work, from physical to psychosocial (Baek et al., 2018; Hwang et al., 2020; Jung et al., 2018). In addition, the gender makeup of the populations studied was heavily skewed in most of the studies. The study by Hwang et al. (2020) recruited predominately male subjects (88% of study population), while other studies (Baek et al., 2018; Birze et al., 2020; Elfering et al., 2018; Kim & Choo, 2016; Sanders & Turcotte, 2010) recruited predominately female subjects (66–100% of study population). The only study with approximately the same number of male and female subjects was that by Jung et al. (2018), comprised of 6407 (52.5%) males and 5779 (47.5%) females. Where reported, the mean age of the subjects recruited across the seven studies ranged between 36.5 and 43.9 years, which is expected to accurately represent the working population.
Broadly, “cognitive dissonance” was not the exposure/independent variable of interest in any of the included studies. Instead, Elfering et al. (2018) investigated the construct of emotional dissonance, while the other six studies investigated the construct of emotional labor. Methods used to quantify these dissonance-related constructs varied from study to study. Elfering et al. (2018) measured emotional dissonance using four items from the Frankfurt Emotion Work Scales (Zapf et al., 1999). Likewise, two studies (Birze et al., 2020; Kim & Choo, 2016) quantified emotional labor using the Emotional Labor Scale originally developed by Brotheridge and Lee (2003), and Hwang et al. (2020) and Jung et al. (2018) used Likert-style questionnaires to measure emotional labor by asking about hiding emotions during work ranging between “always” and “never.” Finally, Sanders and Turcotte (2010) used thirteen items from the Job Content Questionnaire (Karasek et al., 1998) in addition to thirteen more questions that addressed emotional labor specific to dental hygiene practice. In contrast, the study by Baek et al. (2018) assessed a population comprised of individuals whose job requires that they hide their feelings while dealing directly with people who are not employees at their workplace (termed emotional laborers) and simply provided prevalence estimates of musculoskeletal disorders within that population. This study also assessed the effects of more traditional psychosocial factors (job control, workload, social support, etc.) and their effects on musculoskeletal pain.
Finally, in terms of study outcomes, only one study focused specifically on low back pain or low back pain-related disability as outcome measures (Elfering et al., 2018). Instead, five of seven studies quantified musculoskeletal pain across multiple body regions (Baek et al., 2018; Hwang et al., 2020; Jung et al., 2018; Kim & Choo, 2016; Sanders & Turcotte, 2010). The last study by Birze et al. (2020) examined physiological measures associated with long-term health outcomes, including saliva oxytocin and cortisol levels and heart rate variability (HRV).
Study Findings
Relevant Results of Included Studies.
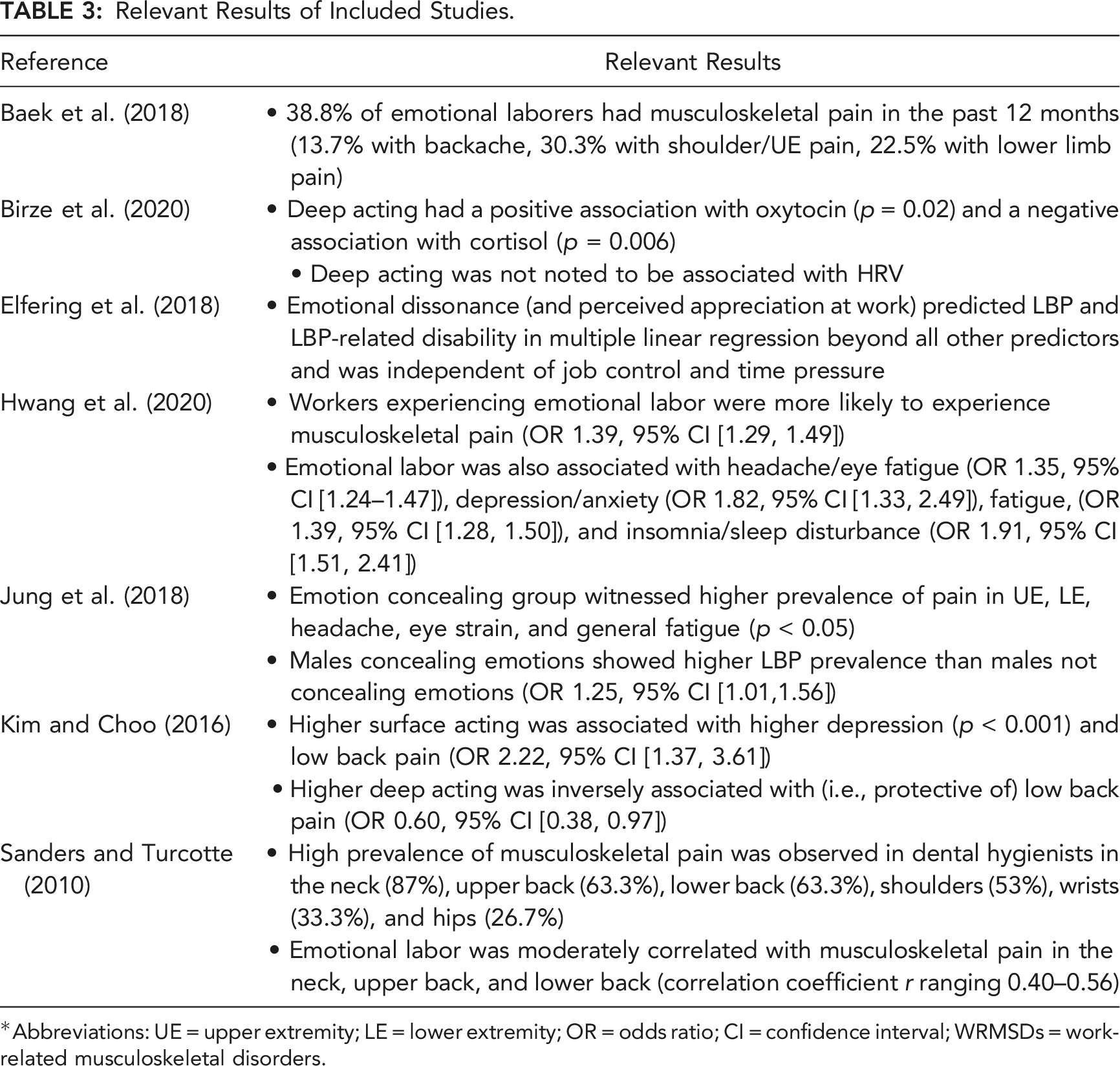
*Abbreviations: UE = upper extremity; LE = lower extremity; OR = odds ratio; CI = confidence interval; WRMSDs = work-related musculoskeletal disorders.
A few of the included studies distinguished between “surface acting” and “deep acting” during emotional labor. In surface acting, individuals put on a “mask” and adjust their emotional response by suppressing, amplifying, or faking their emotions. In contrast, in deep acting, individuals try to align required and true feelings such that genuine emotional displays are put forth (Hülsheger & Schewe, 2011). Due to the larger mismatch between required and felt emotions during surface acting, individuals are far more likely to experience emotional dissonance with a surface acting strategy than with a deep acting strategy. This expectation was also reflected in the results presented herein. Physiologically, Birze et al. (2020) noted that deep acting has a positive association with oxytocin and negative association with cortisol, suggesting a reduced stress response. Biomechanically, Kim and Choo (2016) noted that deep acting may actually be protective against low back pain (OR 0.60, 95% CI 0.38–0.97), whereas higher amounts of surface acting was associated with a higher prevalence of low back pain (OR 2.22, 95% CI 1.37–3.61).
Risk of Bias
Risk of Bias Assessment for Included Studies.
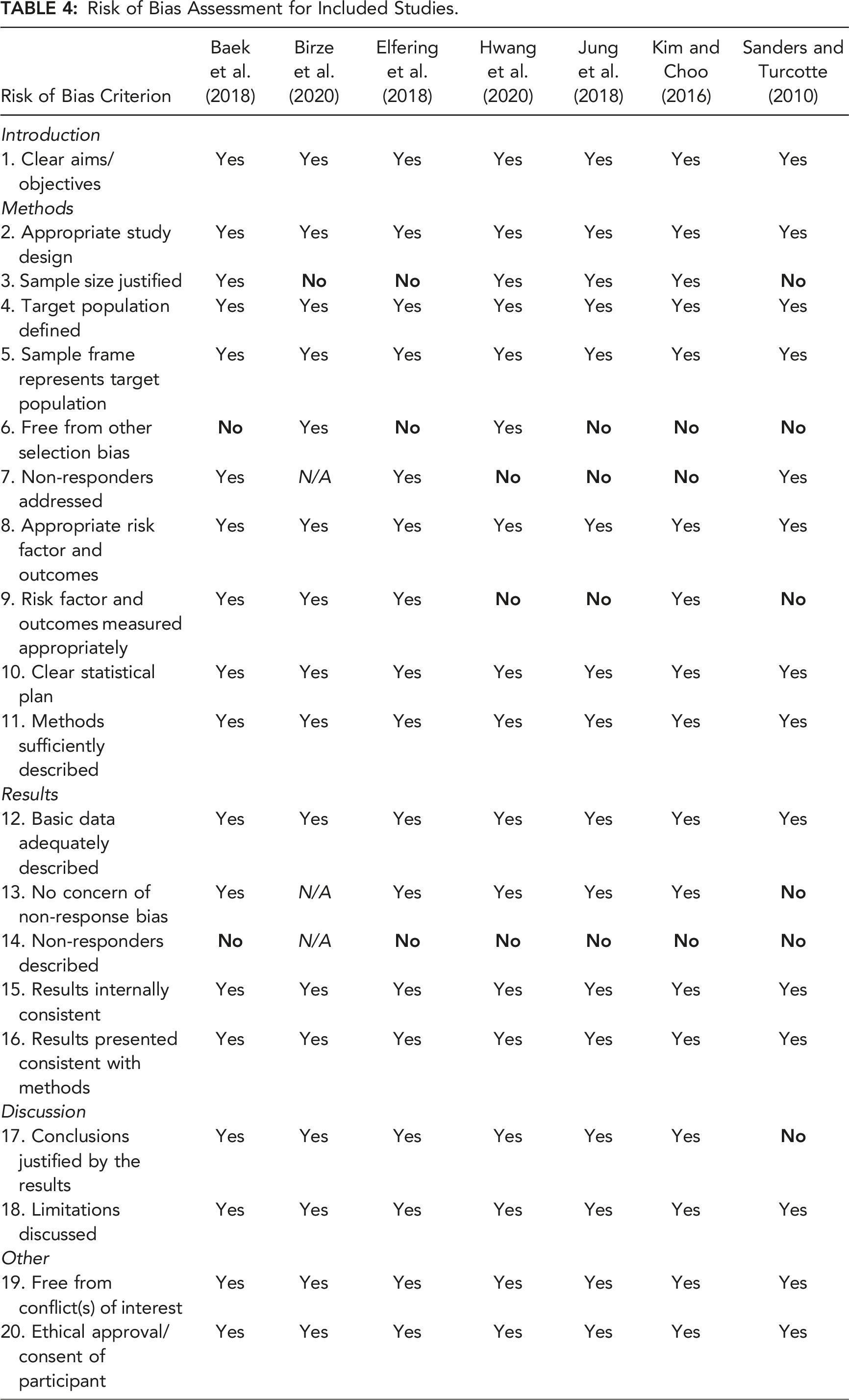
Other selection biases noted were study specific. For example, instead of statistically controlling for physical work exposures, Jung et al. (2018) excluded workers in jobs that were high in physical work demands. Sanders and Turcotte (2010) excluded part time employees, which also significantly reduced their available sample size. Finally, Kim and Choo (2016) excluded call center workers who had been on the job for less than 1 year, even though these employees are more likely to use surface acting techniques than deep acting techniques at work given their inexperience.
One additional risk of bias was noted across three of the included studies, wherein the reliability of the exposure metrics can be called into question. Though piloted on a handful of subjects, the validity and reliability of the dental hygiene portion of the emotional labor questionnaire implemented by Sanders and Turcotte (2010) was not quantified. Likewise, Hwang et al. (2020) used two items from the Korean Working Conditions Survey item on “work situations” to assess emotional labor levels, and Jung et al. (2018) assessed emotional labor with a single questionnaire item asking, “Do you have to hide your emotions during your worktime?” It is unclear whether these metrics were piloted or if their internal reliability were ever quantified. In contrast, most of the other studies included herein reported Cronbach’s α values for their exposure and outcome metrics that were generally at an acceptable level (>0.7) (Birze et al., 2020; Elfering et al., 2018; Kim & Choo, 2016).
Discussion
With the advent of the biopsychosocial model of pain, it was recognized that musculoskeletal disorders like low back and neck pain arise from complex interactions among physical factors, psychological factors, social factors, individual factors, and genetic factors (Hartvigsen et al., 2018). The contributions of psychological factors including anxiety and depression have been extensively studied relative to musculoskeletal disorder causation previously (Elbinoune et al., 2016; M. M. Gerrits et al., 2015; M. M. J. G. Gerrits et al., 2014; Ortego et al., 2016; Pinheiro et al., 2016; Pinheiro et al., 2015). However, given that the CDS increases sympathetic nervous system activation and that these physiological changes may be associated with a higher risk for physical injury, it was hypothesized that the cognitive dissonance state may, too, play a meaningful role in the etiology and maintenance of musculoskeletal pain. Together, the studies that were found provide preliminary evidence that there may be a link between these factors.
Our initial literature search yielded a multitude of study results (237 unique titles), which were narrowed down to the seven publications included herein. Many of these initial search results discussed changes to performance as a result of experiencing the CDS at work, such as the degradation of patient care resulting the CDS in healthcare settings (Cronqvist et al., 2001; de Vries & Timmins, 2017; Harvey et al., 2020; Hülsheger & Schewe, 2011). However, there were no studies that investigated a direct link between cognitive dissonance and musculoskeletal pain.
Nonetheless, the inclusion of related constructs including emotional dissonance and emotional labor in this systematic review did provide some useful results. Emotional labor represents the effort, planning, and control required to express organizationally desired emotion during interpersonal transactions (Andrews et al., 2008). These organizationally desired emotions can be congruent or incongruent with an individual’s internal thoughts and emotions, and when incongruent, emotional dissonance may be experienced. In the included studies, jobs including emotional labor were associated with either a high prevalence of musculoskeletal disorders across all body regions (Baek et al., 2018) or increased odds (odds ratios ranging between 1.25 and 2.22) of experiencing musculoskeletal pain (Elfering et al., 2018; Hwang et al., 2020; Jung et al., 2018; Kim & Choo, 2016). Jobs high in emotional labor were also associated with increased odds of experiencing other adverse events including headache/eye fatigue, depression/anxiety, and insomnia/sleep disturbance (Hwang et al., 2020).
Emotional labor strategies are often classified as either surface acting or deep acting. In surface acting, individuals put on a “mask,” as they suppress felt emotions and amplify organizationally required emotions. In contrast, in deep acting, individuals try to truly align their felt and required emotions. Placing these strategies in context with Cognitive Dissonance Theory, surface acting represents a state that is likely to be high in emotional dissonance, whereas deep acting represents a state in which emotional dissonance is likely to have been resolved. The decision to separate surface from deep acting among some of the included studies provides some useful information regarding the potential for a dose-response relationship between the dissonance-related exposure of emotional labor and outcomes including musculoskeletal pain and physiology. If a relationship between dissonance-related concepts and musculoskeletal symptoms exists, it can therefore be expected that higher levels of surface acting would be positively associated with musculoskeletal pain symptoms, whereas the relationship would disappear with higher levels of deep acting because cognitive/emotional dissonance would have been resolved with this approach. This hypothesized relationship was confirmed in the included studies. For example, Kim and Choo (2016) noted that surface acting was associated with a higher prevalence of low back pain (OR 2.22). Interestingly, instead of there being no relationship between deep acting and musculoskeletal pain (OR approximating 1.0), deep acting was actually protective of against low back pain (OR 0.60). This protective effect may be mediated by physiological changes that occur during deep acting and manifest themselves biomechanically, as Birze et al. (2020) noted that deep acting has a positive association with oxytocin and negative association with cortisol.
The risk of bias assessment conducted for the included studies suggests that selection bias was likely across several of the included studies based on their inclusion/exclusion criteria or the characteristics of the non-respondents. The authors anticipate that the true effect size between exposure (i.e., emotional dissonance or emotional labor) and outcome (i.e., musculoskeletal symptoms) was underestimated across the studies included herein. For example, there was a potential healthy-worker effect in the study by Elfering et al. (2018). Likewise, Jung et al. (2018) excluded jobs that were high in physical work demand while Kim and Choo (2016) excluded workers with less than a year of experience in call center work. Both high physical work demand (Bernard, 1997; Hoogendoorn et al., 1999) and inexperience on the job (Alnaser, 2007; Anderson & Oakman, 2016; Chany et al., 2006; Marras et al., 2006) have previously been shown to be associated with a higher prevalence of work-related musculoskeletal injuries. The more appropriate strategy may have been to include these individuals and treat both as potential confounders in a multivariate regression.
There are some limitations worth mentioning in the context of results presented herein First off, our review protocol was not formally registered. Additionally, a small number of articles were eligible for inclusion in the systematic review, and none of the included studies directly assessed cognitive dissonance as an exposure of interest. Instead, conclusions have been drawn from related constructs, including emotional dissonance and emotional labor. The small number of included studies could have resulted from overly narrow eligibility criteria. However, based on the large percentage of studies that were excluded during screening of the titles and abstracts, the authors believe that it is more likely that the relative lack of included studies is simply from the fact that very few researchers have considered the potential relationship between dissonance and musculoskeletal injury to date.
Three of the studies relied on data collected from either the third or fourth Korean Working Conditions survey, while Kim and Choo (2016) collected data on call center operators in South Korea. Thus, the results presented herein are highly representative of those in Korean culture. This is worth noting because the magnitude of the cognitive dissonance state depends on cultural norms and expectations (Harmon-Jones et al., 2009; Stone & Cooper, 2001). Additionally, the fact that much of the data was derived from the KWCS also introduces the possibility that subjects included in the study by Hwang et al. (2020) (third and fourth KWCS) were double-counted and also included in the study by Baek et al. (2018) (fourth KWCS) and/or the study by Jung et al. (2018) (third KWCS).
Finally, of the seven studies that were ultimately included, six were epidemiological studies that relied on cross-sectional designs. These studies rely on prevalence, rather than incidence measures, and they only provide associations between exposure and outcome at a snapshot in time. Thus, causality cannot be inferred from this type of study design. Additionally, even though consistent results were observed across all the included studies, the overarching “level of evidence” that can be inferred from these studies is also limited (van Poppel et al., 1997). Finally, while these results suggest that an association might exist, future work is still needed to propose and test an actual causal pathway linking these variables.
Conclusion
This systematic review summarized existing evidence on the potential link between dissonance-related constructs (i.e., emotional dissonance, emotional labor) and musculoskeletal disorders. Although none of the selected studies investigated the rather broad construct of cognitive dissonance, the seven included studies investigated dissonance-related constructs of emotional dissonance and emotional labor, in which a mismatch between required and felt emotions might elicit a psychological and arousal state consistent with the cognitive dissonance state. Moderate effect sizes between emotional labor and musculoskeletal disorders were observed (OR 1.25–2.22), with no contradictory findings. Moreover, emotional dissonance predicted low back pain and low back pain-related disability beyond all other psychosocial predictors. Thus, as hypothesized, we conclude that there is a likely relationship between dissonance-related constructs and musculoskeletal disorders like low back and neck pain. However, given that most of the included studies were cross-sectional in nature, a causal relationship between these two constructs cannot be inferred directly. Additionally, none of the studies included within this systematic review provide any suggestions for a detailed causal pathway between these variables. A causal pathway linking cognitive dissonance and musculoskeletal pain should therefore be proposed, tested, and revised (as needed) in future work.
Key Points
The psychological construct of cognitive dissonance may be related to musculoskeletal injury, but there are currently no studies that formally examine this relationship. Several studies included herein did investigate the relationship between cognitive dissonance-related constructs of emotional labor and emotional dissonance. Moderate effect sizes between dissonance-related constructs and musculoskeletal disorders were noted (OR 1.25–2.22). The studies included herein were cross-sectional in nature, so a causal relationship between cognitive dissonance-related constructs and musculoskeletal disorders cannot be inferred. Therefore, the relationship between cognitive dissonance and musculoskeletal disorders warrants future research.