
Abstract
Objective
The study aim was to review existing research on healthcare workers’ safety climate, safety knowledge, and safety motivation as predictors of workers’ safety behaviors. A second aim was to assess existing evidence of multiple spillover effects from workers’ safety climate and safety behaviors to patient safety climate and safety behaviors and vice versa.
Background
Research has focused on patient safety but mainly investigated from the perspective of healthcare staff. A broader model of safety is proposed, where safer healthcare provision is achievable if both workers and patients participate in safety.
Method
A systematic literature search was conducted. A total of 15,663 articles were screened, of which 43 met the inclusion criteria.
Results
The impact of workers’ safety climate could go beyond workers’ safety performance to also include patients’ safety climate, as well as their safety motivation and safety participation. Patient safety participation would, in turn, affect workers’ safety compliance. Such results highlight patients’ central role in healthcare safety for both service providers and users.
Conclusion
This review offers a framework of safety that extends from healthcare workers to patients. It also emphasizes that patient participation can help staff safety performance, reducing the chance of errors, but it needs to be proactively encouraged by healthcare staff.
Applications
The insights can be used to develop interventions that improve both worker and patient safety through collaboration and co-participation. The proposed framework offers ideas and practical implications for healthcare organizations, practitioners, planners and policy makers to consider.
Keywords
Introduction
The most recent data available from the World Health Organization (WHO, 2022) reported that work-related injuries, occupational illnesses and related absenteeism are a significant financial cost for the health sector (around 2% of overall health spending; WHO, 2022). Nevertheless, only a small group (26 out of 195) of WHO Member States have policies and national programs dedicated to safeguarding health workers’ occupational health and safety (WHO, 2022). Safety in healthcare becomes even more important when data on patient safety are added to the above considerations of healthcare workers. Internationally, around 1 in every 10 patients is harmed in health care and more than 3 million deaths occur annually due to unsafe care (Slawomirski & Klazinga, 2022).
The statistics highlight the need to recognize healthcare safety as a global priority by intervening on the leading indicators or predictors of safety outcomes (Jiang et al., 2019), which can be traced back to the organizational environment that both health providers and health users share with regard to safety, often described through the concept of safety climate.
Over the past 40 years, research on workplace safety has shown that an organization’s safety climate is a strong and consistent predictor of safety performance and safety-related outcomes across many industries, including healthcare. Safety climate is defined as employees’ shared perceptions of the organization’s policies, procedures, and practices related to safety (e.g., Zohar, 2003; Zohar, 2010; Zohar & Luria, 2005). According to Zohar and Luria (2005), safety climate reflects socially constructed signals about what behaviors are expected and valued at work. These signals arise from two sources: the policies and actions of top management (organizational safety climate) and the day-to-day practices of supervisors and co-workers (group-level safety climate). Safety climate is well-established as one of the main antecedents of safety performance, which is described as safety behaviors, and it is commonly divided into two components. The first is safety compliance, which refers to following correct and safe procedures, including taking precautions against risks (such as using proper protective equipment). The second is safety participation, which involves proactive and voluntary efforts to create a workplace that supports safety (such as helping co-workers and promoting voluntary safety programs; Neal et al., 2000). The relationship between safety climate and safety compliance and participation has shown to be mediated by the determinants of safety performance, in particular by the knowledge and skills necessary for safety behaviors, and by the motivation of individuals to perform those behaviors (Griffin & Neal, 2000). Safety compliance and participation behavior, in turn, have been demonstrated to predict safety outcomes, which in the healthcare sector refer to those work-related incidents that involve either the healthcare worker (Bernal et al., 2015; Davis & Kotowski, 2015) and/or the patient being treated (e.g., Bae, 2011; Kramer et al., 2016; Tvedt et al., 2014), both attributable to the healthcare worker’s actions.
Current research in the healthcare industry—including literature reviews—has mainly shown that more positive employee safety climates are linked to better patient safety outcomes and higher quality-of-care (e.g., Cook et al., 2016; Goh et al., 2013; Groves, 2014; Lee et al., 2019; Singer et al., 2009, 2013; Weaver et al., 2013). However, the safety and well-being of healthcare workers are also closely connected to the quality-of-care delivered. When healthcare workers experience injury or illness, this can affect their ability to provide care safely and effectively, which may in turn contribute to treatment errors or patient accidents (Green & Griffiths, 2013). For example, if injured or ill, employees tend to be replaced with less experienced staff, or if tasks must be redistributed among the remaining team, this can create additional pressures that may jeopardize both care quality and patient safety (Aiken et al., 2014). Additionally, recent literature has highlighted the need to strengthen both patient and staff safety perspectives, as each contain gaps that warrant further attention (Kilcullen et al., 2022). Therefore, the first contribution of this study is to provide an up-to-date and comprehensive review of the existing literature on predictors and outcomes of safety performance in the healthcare industry, while considering both employees and patient safety accidents, as both outcomes must be factored in to achieve high service quality and safer healthcare.
Further, we seek to advance Griffin and Neal’s (2000) established framework of distal and proximal predictors of workers’ safety performance—namely, safety climate, safety knowledge, and safety motivation—by considering how these elements also relate to the users of healthcare services. We will expand the model to embed patients’ active role as agents of safety within healthcare systems. Much of the initial research on safety has been developed in the manufacturing sector, where the safety agents—that is, “the subjects that perform or are responsible for each safety issue inside the company” (Melía et al., 2008, p. 950)—were traditionally identified as the organizational agents or top management, and the workforce agents, which included supervisors, co-workers, and the individual worker (Meliá et al., 2008). We argue that in the healthcare industry it is necessary to broaden the existing definition of safety agents by including the role of patients, as they can influence, with their participation and involvement in safety initiatives, the other agents’ safety processes, actions, and performance, ultimately contributing to safer outcomes.
Lastly, by integrating patients into the model as safety agents, we propose multiple reciprocal effects, from employees to patients and vice versa. It has been well demonstrated in other sectors how an organization’s positive safety culture and a physically safe workplace for employees will positively affect the service environment and enhance service encounters (Willis et al., 2012), but such a framework has been far less developed in the healthcare sector (Hofmann & Mark, 2006; Lake et al., 2016). More recent studies during the COVID-19 pandemic observed significant reductions in attendance at emergency departments, with concerns that public fear of infection may have contributed to increased morbidity and mortality (Dann et al., 2020; Lazzerini et al., 2020; McDonnell et al., 2020). However, where patients felt that precautions were put in place to protect their safety—via the setting up of an alternate “clean” hospital site or using independent sector for patient testing—they reported high levels of confidence in measures undertaken and that had the greatest impact on their perception of safety (Lee et al., 2021). Taken together, these findings lead us to suggest a spillover effect, or influence, whereby healthcare staff’s safety climate and safety behaviors influence patients’ own safety climate and safety behaviors. We also suggest that an additional and reverse spillover effect exists from patient safety behavior to worker safety behavior. To date, most research in healthcare safety has focused on workers’ safety perceptions and the resulting effects on their patient-related safety performance. Yet a smaller, but increasingly important, body of research has begun to examine patients’ safety perceptions and how these shape their own safety motivation, compliance, and participation in care. The limited studies available show that patients’ perceptions of the safety of their healthcare service—patients’ safety climate—play a key role in their willingness to actively participate in safety and error prevention. This includes actions such as voicing doubts, asking questions, and raising concerns about the safety of their treatment or care plan (e.g., Longtin et al., 2009, 2010). Those research findings align with the rising importance given to patient involvement in the redesign and development of healthcare services across the world because of the potential such participation may have in improving healthcare workers’ safety compliance and related patient safety outcomes (i.e., patient readmissions, infection rates, and medication errors; Andersson & Olheden, 2012; Longtin et al., 2010). Several studies have revealed precisely that patient participation can help achieve safer healthcare by preventing employee practice errors (Zhang et al., 2012), but ambiguity remains about how patients participate in safety initiatives and what conditions influence their decision to engage in such behaviors (Vaismoradi et al., 2015).
Therefore, our review proposes multiple influences, from healthcare staff safety climate and safety behaviors to patients’ safety climate and safety behaviors and, in turn, from patient’s safety participation back to staff safety compliance. Our proposed framework aligns with existing models of patient safety (see SEIPS 3.0) in emphasizing the need for human-centered healthcare redesign through the involvement of multiple stakeholders and addresses the needs of both patients and healthcare workers (Carayon et al., 2020; Monaca et al., 2020). However, our study also complements and expands on these models in two important ways. First, from a theoretical perspective, it focuses on the psychosocial aspects of safety, particularly the central role of safety perceptions (climates), which are well-established predictors of safety attitudes, safety behaviors, and associated safety outcomes. In doing so, we build on Griffin and Neal’s (2000) framework of distal and proximal predictors—safety climate, safety knowledge, and safety motivation—by broadening its scope so that it accounts for patients’ active involvement in safety, affirming their capacity to shape and strengthen these predictive processes. Second, we highlight the possibility of mutual influences between employee safety and patient safety, proposing a conceptual—and potentially empirical—connection between two domains that have often been treated separately in theoretical (occupational safety vs. medical/clinical safety) and practical contexts (including regulatory and statutory frameworks). Understanding the safety perceptions and behaviors of both users and healthcare professionals encourages a shift from a provider-centered approach towards a collaborative model based on partnerships between patients and healthcare providers.
The specific objectives of this study are therefore to: (1) Review existing research on healthcare workers’ safety climate, knowledge and motivation as predictors of workers’ safety behaviors (both compliance and participation) and of related safety outcomes (both workplace injuries and patient safety indicators attributable to workers’ actions). (2) Identify existing evidence of influence which healthcare workers’ safety predictors and behaviors have on patient safety predictors and behaviors, and the influence patient safety participation has, in turn, on staff safety compliance.
Figure 1 synthetizes the expected theoretical framework. Theoretical framework of this literature review. The arrows indicate paths of expected relationships among the factors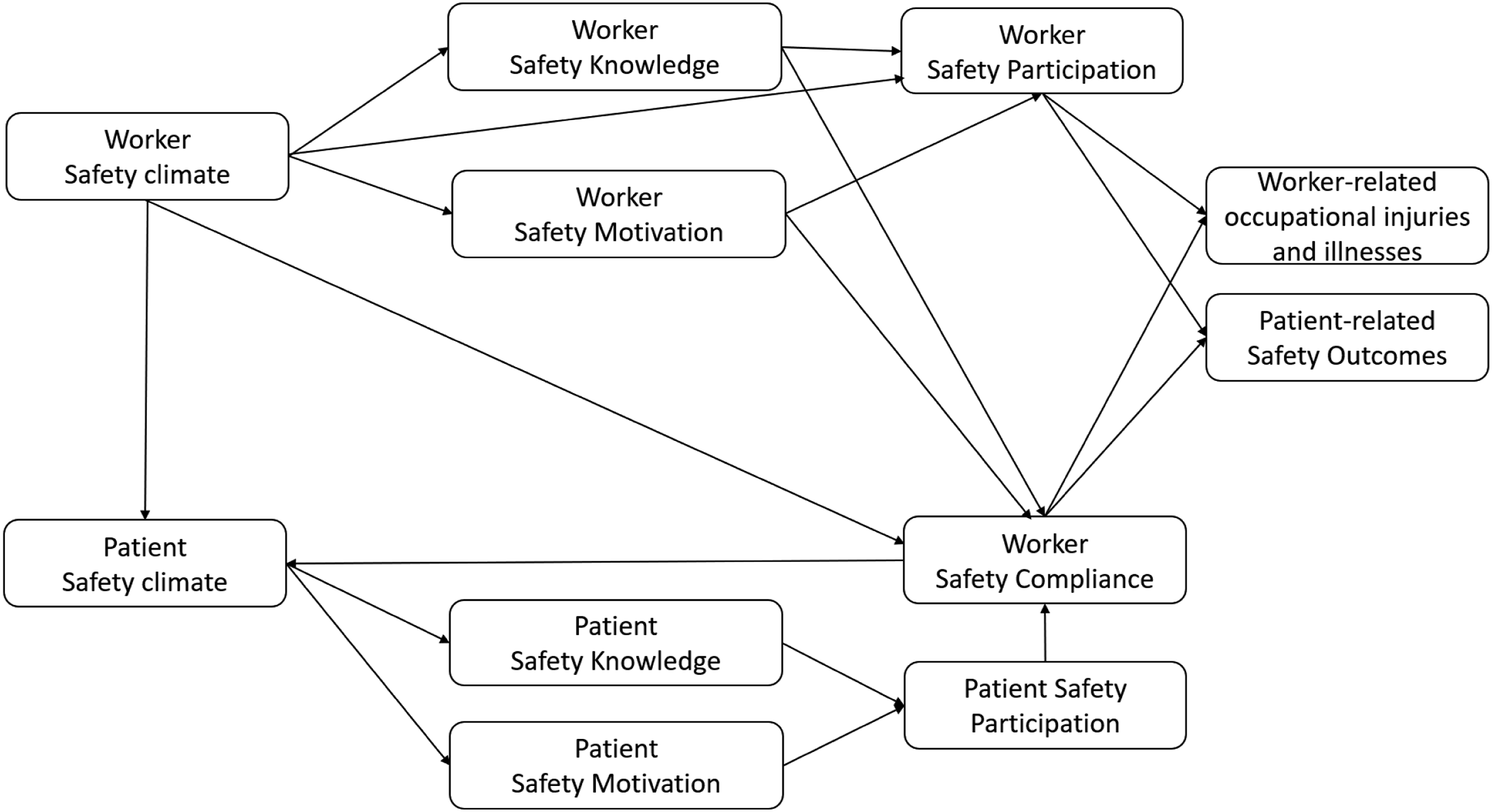
Method
Search Strategy
Our systematic literature review was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Briner & Denyer, 2012; Moher et al., 2010). The literature search was conducted using the following databases: Scopus, Emerald Journals, ABI/INFORM Global, Media Research Centre, Oxford Academic Journals, ProQuest Science database, PubMed, Sage Journals, Wiley online library, and journal finder, Google Scholar. Databases were searched between the time range of the year 2000–2024. This timeframe was determined as healthcare systems have transformed and taken major leaps in terms of complex service arrangements and newer healthcare models since 2000 (Maniatopoulos et al., 2020).
Search words included and were not limited to “healthcare,” “safety performance,” “perceptions,” “patient perceptions,” “safety motivator,” “safety attitudes,” and “safety culture.” As for the latter, the terms safety culture and safety climate are typically used as synonyms in the health care safety literature, although they present differences (Alabdaly et al., 2024). As safety climate is considered a snapshot of culture which can be more easily measured at a specific point in time, researchers often use safety climate as a proxy measure of safety culture (Morello et al., 2013; Sexton et al., 2006). For those reasons and for the purpose of this review, “safety culture” has been used as an alternative search word to “safety climate.” A full list of all search terms is included in the supplementary material (Table S1).
Eligibility Criteria, Study Selection and Data Extraction
Several eligibility criteria were applied during abstract screening. First, studies had to be conducted in countries with established healthcare systems, whether contributory or state-funded. Although studies conducted in specific countries would mostly be relevant to their own healthcare systems (e.g., Ericsson et al., 2019), the nature of those countries’ healthcare provision is often comparable across contexts, as those systems typically require some form of contribution, which may or may not involve payment through employment (Ingleby et al., 2012). Second, the research had to employ an empirical design, including primary studies or meta-analyses drawing on secondary data. Third, articles not published in English were excluded, and fourth, articles not published in peer-reviewed journals were excluded.
A total of 15,663 articles were identified in the primary search. Based on the title and abstract screening, 72 articles were deemed potentially eligible and retrieved for full-text review. Of these, 15 articles were excluded because they were not relevant to the research questions and 32 articles did not meet the inclusion criteria. 18 additional studies were identified through screening the references of included articles (i.e., pearl-growing method; Ramer, 2005), which led to a total of 43 articles for quality assessment (see Figure 2 for the PRISMA flowchart). PRISMA - flow diagram illustrating the review process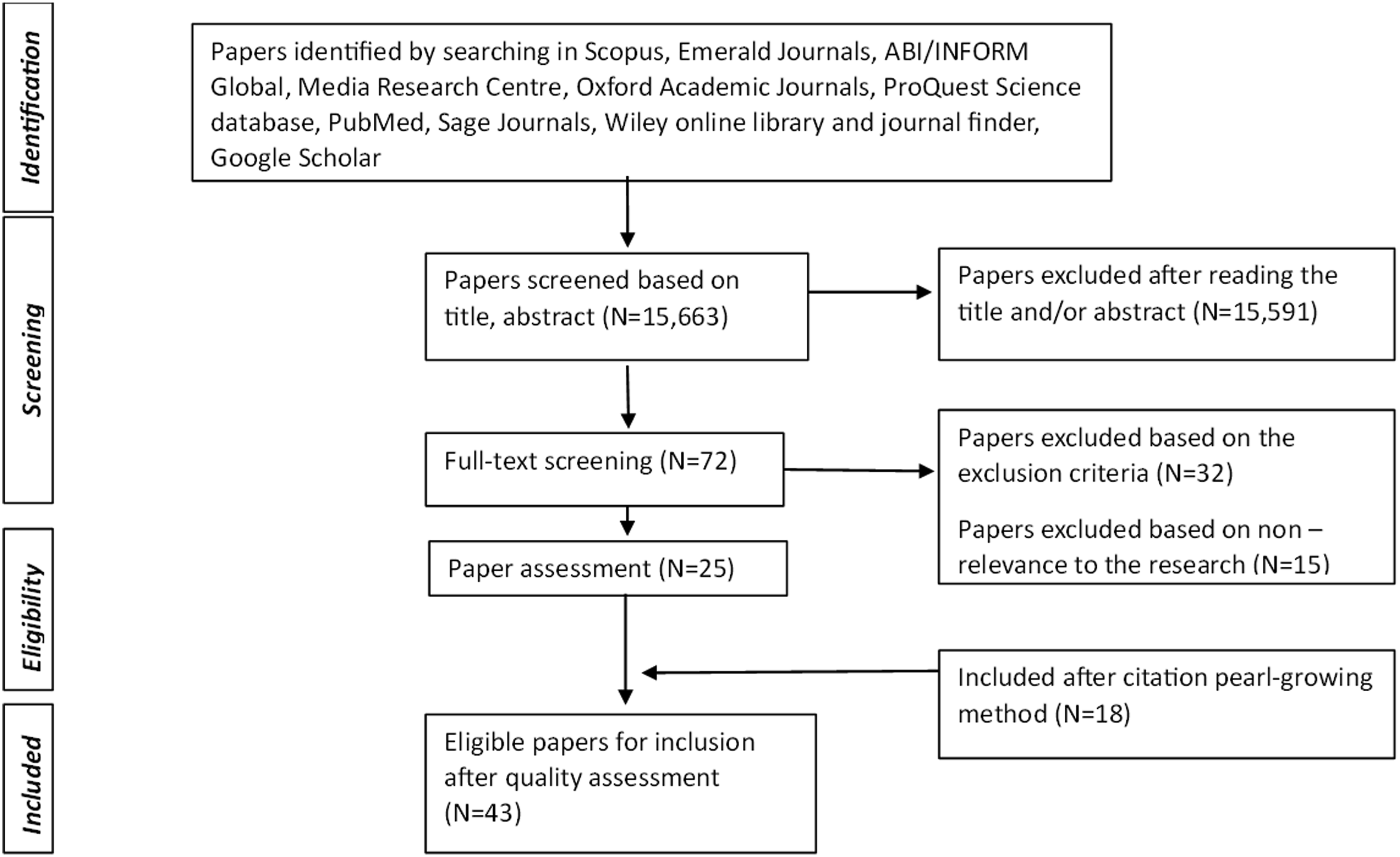
Data on the following criteria were extracted from each article and reported in a spreadsheet: first author’s last name, publication year, country, title, aims, research design and methodology, sample, results. Two reviewers individually appraised the 43 articles using 6 criteria retrieved and adjusted from existing systematic reviews based on the Institute of Work and Health (e.g., Jetha et al., 2024; Skovlund et al., 2025). The criteria assessed risk of bias in study design and objectives, sampling and recruitment procedures, data collection and data analysis (supplementary Table S2). Each article was appraised on a scale between 1 (low quality) and 3 (high quality) across the 6 parameters. A total score was calculated for each article, then divided by the maximum weighted total score and multiplied by 100 to give a percentage score. This percentage score was used to classify each article as either low (50%), medium (50–85%), or high (>85%) quality. All 43 articles were rated either medium or high quality; hence, all of them were included in the review.
Results
Characteristics of the Selected Studies
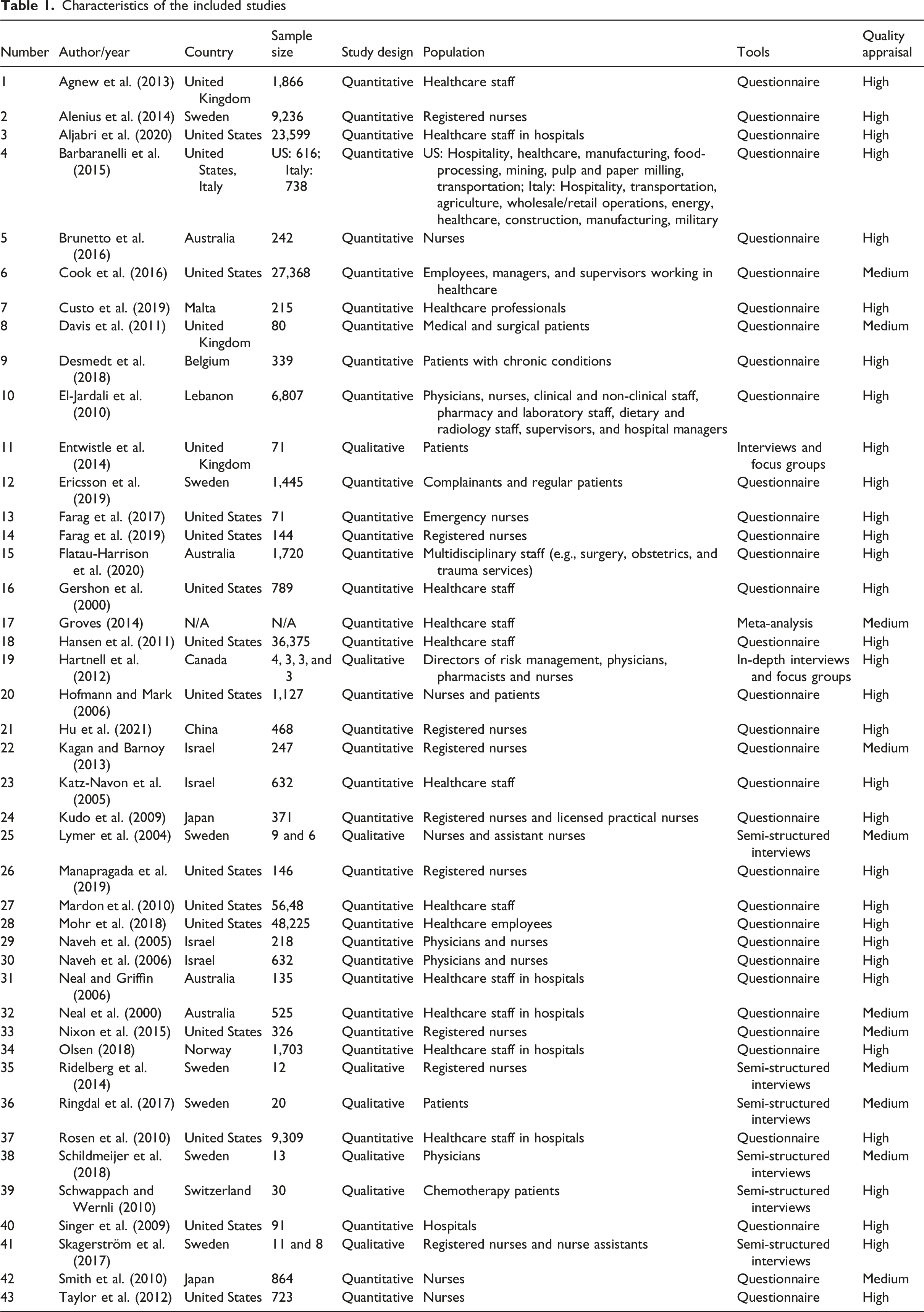
Of the 43 selected articles, 32 were high-quality and 34 studies were using quantitative research design. The included studies were conducted in 14 countries.
37 studies had healthcare staff as participants, 1 of which involved both nurses and patients. The remaining 6 studies had patients as the sole participants (whether primary, acute or chronic care patients).
Characteristics of the included studies
RQ1. HC Workers’ Safety Climate, Safety Performance and Safety Outcomes
Twenty-eight high-quality articles and seven medium-quality articles reported on the perspective of healthcare professionals with regard to their safety climate, their safety performance—including antecedents and components—and/or their safety outcomes (patient and workers accidents and injuries—dependent on workers’ safety behavior). The findings were categorized into three sub-groups, as below.
Worker Safety Climate, Antecedents, and Components of Safety Performance
Staff safety climate was found to be related to their safety motivation (Flatau-Harrison et al., 2020; Kudo et al., 2009); in turn, safety motivation together with safety knowledge was demonstrated to partially mediate the relationship between worker safety climate and their safety compliance and safety participation (Barbaranelli et al., 2015; Neal et al., 2000; Neal & Griffin, 2006). Such partial mediation indicates that safety climate also directly related to safety behaviors, as reported across multiple articles, finding that safety climate (as a whole or in its sub-components) was directly associated with self-reported safety compliance, including employees’ error reporting and prevention of adverse effects to patients (Farag et al., 2017, 2019; Gershon et al., 2000; Hartnell et al., 2012; Kagan & Barnoy, 2013; Lymer et al., 2004; Manapragada et al., 2019; Ridelberg et al., 2014). When safety climate was measured as a first or second-order factor rather than its sub-components, its relationship with safety behavior seemed to be stronger for safety participation rather than for compliance (Neal et al., 2000). Moreover, the effect of safety climate on safety participation seemed to persist over time (Neal & Griffin, 2006).
When safety climate was measured as its sub-factors, those were found to be significantly and directly linked to safety performance antecedents and components. Specifically, employee safety climate factors including safety reporting systems, communications with physicians and nurses’ workload were significantly associated with nurses’ motivation to prevent mistakes (Kudo et al., 2009). Employee safety climate factors including safety communication, management values, safety systems (Manapragada et al., 2019), cleanliness and tidiness of the workspace, managerial support, and absence of work hindrances (Gershon et al., 2000) showed significant positive relationships with safety compliance and overall safety performance (compliance and participation together). Staff increased workload and pace of work, together with supervisors’ knowledge, were identified as additional safety climate factors contributing to workers’ safety compliance (Lymer et al., 2004). Higher management negative attitude and inauthentic commitment to safety were employee safety climate factors identified by frontline staff as barriers to their ability to prevent errors and adverse effects to patients (Ridelberg et al., 2014). Finally, management error feedback, communication, and non-punitive response to error were additional safety climate factors that showed to significantly impact employees’ motivation to report errors (Farag et al., 2017, 2019; Hartnell et al., 2012; Kagan & Barnoy, 2013).
Some studies found unexpected or additional factors to be included in the relationships discussed above. Specifically, it was found that the relationship between safety climate and safety compliance was mediated by other distal factors not taken into consideration in Griffin and Neal’s model (2000), such as hospital unit leadership (Olsen, 2018) and job-related negative affect (Nixon et al., 2015). Additionally, in one article safety compliance was predicted marginally by safety climate dimensions, as the main variance in compliance was explained by employees’ psychological capital (Brunetto et al., 2016).
Worker Safety Climate, Worker Safety Behaviors, and Worker Occupational Safety Outcomes
Employee safety climate significantly and inversely related to work injury rates, whether self-reported (Agnew et al., 2013; Gershon et al., 2000; Smith et al., 2010) or retrieved from official source and archival records (Aljabri et al., 2020; Cook et al., 2016; Hofmann & Mark, 2006; Taylor et al., 2012). Some specific dimensions of safety climate seemed to be significantly related to needlestick and sharps injuries, such as management priority to and active involvement with safety, as well as supervisors correcting unsafe work practices (Smith et al., 2010). Still about those safety climate factors pertaining to the role of higher managers, senior management support to safety training and frequent safety-related feedback were found to be significantly related to workplace exposure incidents (Gershon et al., 2000).
Additionally, one article revealed high safety performance (compliance and participation as combined) to negatively predict employees’ injuries over time (Neal & Griffin, 2006).
Worker Safety Climate, Worker Safety Performance, and Patient-Related Safety Outcomes
Strong evidence was found to support the relationship between employee safety climate (whether general or patient-specific) and a wide range of patient safety indicators attributable to employees’ actions, including medication errors, in-hospital complications, and adverse effects (Agnew et al., 2013; Alenius et al., 2014; Custo et al., 2019; El-Jardali et al., 2010; Groves, 2014; Hansen et al., 2011; Hofmann & Mark, 2006; Hu et al., 2021; Katz-Navon et al., 2005; Mardon et al., 2010; Mohr et al., 2018; Naveh et al., 2005, 2006; Rosen et al., 2010; Singer et al., 2009; Taylor et al., 2012). Some studies focused on specific safety climate dimensions rather than measuring a second-order safety climate factor. Those safety climate dimensions that showed to be significantly related to patient safety indicators were respectively: workers’ perceptions of staffing levels and managerial commitment (Agnew et al., 2013), staffing levels and good relationships nurse-physicians (Alenius et al., 2014), managerial safety practices (Custo et al., 2019), communication openness, feedback and communication about errors, and non-punitive response to error (El-Jardali et al., 2010). Two articles reported that employee perceptions of suitable safety procedures and frequent and clear information flow reduced patient treatment errors (Naveh et al., 2006), but only when managers practiced safety and prioritized safety within their unit (Naveh et al., 2005).
Three studies investigated hospital safety culture rather than climate, and in one of them safety culture dimensions of espoused safety values directly related to safety outcomes (including self-reported patient accidents), whereas the practiced values related to such outcomes through employee safety performance (not specifying whether compliance or participation, or both; Hu et al., 2021). The two remaining studies reported non-significant relationships between safety culture and a range of patient safety outcomes, whether those were considered separately—that is, pressure ulcers, falls, medication errors, nurse-sensitive outcomes, and post-operative outcomes—or as a composite measure (Groves, 2014; Rosen et al., 2010).
RQ2. Spillover Effects From Worker to Patient to Worker
Six high-quality and three medium-quality articles focused on possible spillover effects from employees to patient safety climate, safety behaviors and safety outcomes; of those, six articles recruited patients as participants, whereas two articles involved staff only. Lastly, one article involved both HC providers and users, and it was also mentioned in the previous results section, as its findings cover both our research questions.
In detail, there was no explicit definition of a patient’s safety climate, as studies investigated specific dimensions pertaining to patients’ perceptions of their healthcare provider with regard to the priority and value given to safety, without explicitly defining those perceptions as climate. For instance, one article tested and found that patient perceptions of nurse responsiveness to patients’ symptoms was significantly and positively related to staff safety climate at the unit level, and this was the only study, to the best of the authors’ knowledge, to have explicitly investigated staff and patient safety perceptions at the same time with possible spillover effect from staff to patients (Hofmann & Mark, 2006).
Other dimensions of patient safety climate involved patients’ perceived communication between their healthcare professionals, which seemed to lead to more patient incidents when such communication was insufficient (Desmedt et al., 2018). Patients have found to experience harm also because of inadequate listening from or feeling ignored by their healthcare practitioner in two further articles (Ericsson et al., 2019; Ringdal et al., 2017).
The remaining studies targeted determinants and contributors of patients’ safety participation—namely, patient safety motivation, and in doing so they highlighted a range of factors that largely involved the healthcare staff, such as their behaviors and attitudes, and the quality of their relationship with patients. Patients’ perceptions of the communication with and from healthcare staff seemed to represent a determinant not only of patient accidents and harm, but also of patients’ motivation to participate in their own safety and of their subsequent participation behavior (intended as voicing their doubts and concern to their HC providers; Entwistle et al., 2014; Schildmeijer et al., 2018; Schwappach & Wernli, 2010; Skagerström et al., 2017). The communication and interactional aspects between patient and healthcare staff were found to be the main determinants of patient motivation to participate according to staff as well; patients needed to be adequately informed about matters related to their health and safety, they needed to receive no conflicting information, and staff needed to make sure that information was understood correctly and trusted by patients, in order for the latter to be willing to get involved in health and safety-related matters (Entwistle et al., 2014; Ringdal et al., 2017; Schildmeijer et al., 2018; Skagerström et al., 2017). Additionally, doctors and nurses’ encouragement were found to be of paramount importance in enhancing patients’ motivation to ask challenging questions and to flag any safety problems or errors; patients appeared to be more willing to ask general and factual questions about their healthcare management, but were reluctant to challenge their HC professional, for example they would not be willing to ask their doctors/nurses if they had washed their hands before starting the visit/procedure for fear of causing offense, being dismissed or labeled as “difficult” (Davis et al., 2011; Entwistle et al., 2014). However, authentic encouragement from HC professionals was the main influential factor on patient likelihood to speak up, hence of their safety participation (Davis et al., 2011; Entwistle et al., 2014).
One article underlined that patients who felt safe and knowledgeable about what was happening to them were, in turn, feeling more empowered, hence more motivated to participate, and this led to higher participation behavior (Ringdal et al., 2017).
Finally, both staff and patients believed their participation contributed to support better staff compliance, namely, that it contributed to less patient harm and safer healthcare (Ericsson et al., 2019; Schwappach & Wernli, 2010).
Discussion
This section sequentially addresses two research questions based on the analysis of the presented results, concluding with a discussion of the limitations found in the review and opportunities for future research.
The first aim of this literature review was to understand whether healthcare workers’ safety climate predicted their knowledge and motivation to behave safely and, in turn, their safety behaviors (compliance and participation) and safety outcomes (both workplace injuries and patient safety indicators attributable to healthcare staff behaviors).
The review has confirmed the theoretical framework suggested by Griffin and Neal (2000) as found across other industries, that both components of safety performance (compliance and participation) are predicted by their antecedent (safety climate) and determinants (safety knowledge and safety motivation), with the determinants partially mediating between safety climate and safety performance components (Neal et al., 2000). The above relationships can be explained according to the social exchange theory (Blau, 1964) and expectancy-valence theory (Vroom, 1964). When employees feel that their organization cares about their well-being, they develop a sense of obligation to reciprocate by engaging in behaviors that benefit the organization, including higher compliance (Hofmann & Morgeson, 1999) and proactive engagement in non-mandatory safety activities (which are considered a form of citizenship activities; see Neal & Griffin, 2006; Tsui et al., 1997). Expectancy-valence theory as applied to safety posits that employees are motivated to adhere to safety protocols and engage in safety activities if they believe these actions will lead to desirable outcomes (Zohar, 2003). Interestingly, safety participation seems to further strengthen safety compliance, by increasing workers’ willingness to act in a safe manner, thus creating a positive lagged effect of their safety participation to their safety compliance via their safety motivation (Neal & Griffin, 2006). One possible reason is that individuals who engage in voluntary safety initiatives often receive positive reinforcement and encouragement, which motivates them to continue these activities. Hence, an organization’s safety climate would have an important long-lasting influence in ensuring adherence to procedures, but it would have an even more significant role in promoting employees’ active commitment to and involvement in safety through increasing their motivation to behave safely (Clarke, 2006).
This suggests that interventions and training to enhance workers’ safety compliance should aim at improving especially their safety knowledge and their safety motivation (Neal et al., 2000); interventions to enhance safety participation should be targeting the organization safety climate, particularly when the goal is to achieve long term effects and beyond improving adherence to mandatory procedures.
Results also suggest to management how to motivate employees so as to get them actively involved with safety initiatives through changing the work environment—for instance, through management and supervisor’s corrective and non-punitive response to mistakes, which would make workers less afraid to report errors—rather than blaming and punishing workers for lack of compliance (Farag et al., 2019; Neal & Griffin, 2006).
The review of the studies on worker and patient safety outcomes found that both appear to have common contributing factors attributable to workers’ safety climate (Flin, 2007), which leads us to confirm the importance of improving workers' safety climate to reduce both worker and patient injuries, with the consideration that lower occupational injuries can contribute to achieve better quality and safer healthcare. Similar safety climate dimensions were indeed identified as the main responsible—directly or indirectly through safety performance—of both types of outcomes, with almost twice the amount of evidence for patient safety as compared to the number of articles on worker occupational injuries and illnesses. Above all, management commitment and managerial involvement with safety (e.g., through support to employee safety training), supervisors’ safety practices (including correcting others’ unsafe work behaviors) and open, frequent and clear safety communication, including regular safety-related feedback and an environment that is supportive of learning from errors were, above all, demonstrated to predict both workers’ injuries and incidents, and patient errors, complications and adverse effects (e.g., see Agnew et al., 2013; El-Jardali et al., 2010; Gershon et al., 2000; Naveh et al., 2005; 2006; Smith et al., 2010).
Those results mirror what was found across other industry settings, in particular the role of management active involvement in determining workplace safety climate and outcomes, as leaders would send key signals about the relative priority of safety in comparison to other competing demands (e.g., productivity; Nixon et al., 2015). Because of the multilevel nature of safety climate, for those messages to be effective beyond rhetoric, the importance given to safety has to be enacted at every level, starting from higher management espoused and supervisors’ practiced commitment to safety. This means that higher-level managers and direct unit leaders have an irreplaceable role, the former to influence the priority given to safety through decision making (e.g., budgets, including staffing adequacy and support to safety training); the latter, to translate that commitment into work procedures and communication loops that are clear, open, and aligned with the advocated safety policies, in order to engage work units in safe behaviors, resulting in safer outcomes for them and their patients (Aljabri et al., 2020; Olsen, 2018).
Additionally, we found that self-reported safety performance acted as a partial mediator between workers’ safety climate—on one side—and worker and patient safety outcomes—on the other side—as reported in two separate studies (Hu et al., 2021; Neal & Griffin, 2006). This has to be tested further in future empirical research, but the existing evidence showed that self-report measures of safety behavior might have predictive validity toward objective safety measurements. Moreover, it calls for future research to treat and test safety compliance and safety participation as empirically distinct from each other, and potentially producing different effects (Neal & Griffin, 2006).
The second aim of this literature review was to identify possible spillover effects that healthcare workers’ safety climate and safety behaviors have on patients’ safety climate and behaviors and, in turn, possible spillover effects from patient safety participation behavior to employee safety compliance behavior. We found good evidence, although very limited in number, as only 9 of the 43 reviewed articles took into consideration patients’ perspectives and perceptions of safety when using healthcare services. As reported in the results section, employee safety climate and safety behaviors showed to be related to patients’ own perceptions of the importance and priority their healthcare provider gave to safety—that is, how safely they have been treated as patients.
The results of our second research question support our view that Griffin and Neal’s (2000) model of workplace safety is also applicable to healthcare service environments. Additionally, they corroborate our proposal that patients are safety agents of their own healthcare, in a manner similar to their healthcare providers. It can be argued indeed that patients collect information from the organizational environment to shape their own perceptions of safety and, to some extent, in doing so they mirror staff perceptions of safety. For instance, our findings suggest that in work settings, open and authentic communication about safety priorities, together with non-punitive feedback from top management and supervisors, motivates healthcare staff towards safer behaviors and outcomes (Manapragada et al., 2019; Ringdal et al., 2017). Similarly, our findings also suggest that effective and clear communication and feedback between carers—and between staff and patients—in a comfortable environment where patients are encouraged and empowered to ask questions without fear of being demeaned, rejected, or perceived as challenging hierarchical knowledge, makes patients feel they are being treated safely, enhances their safety knowledge, and consequently makes them more willing to participate in the safety aspects of their healthcare management (Ringdal et al., 2017; Skagerström et al., 2017). Those dimensions echo existing questionnaires developed to assess patient safety culture, where similar key factors comprise the different facets of patient safety perceptions (e.g., see the PaPSC scale from Monaca et al., 2020). As shown for workers, and together with safety motivation, patient’s safety knowledge depends on patient’s safety climate dimension of perceived communication from and information provided by healthcare staff; such knowledge would constitute “the basis of patient participation” (Larsson et al., 2011, p. 5), as it would make patients more confident in making informed decisions about their treatments (Larsson et al., 2007), and this would lead to higher patient safety participation (Ringdal et al., 2017). Patient safety knowledge should hence be enacted by HC staff, through assessing and enhancing patients’ understanding of their care management plan (McTier et al., 2014).
The potential spillover effect from workers to patients found in this review would resemble what has been established by research across other service industries, where employee safety is also positively associated with customer/user satisfaction, and service users would be unsatisfied with service encounters if they sensed a negative company safety climate, thus showing how perceptions of workplace dynamics spill into the service environment (Willis et al., 2012). Although user satisfaction was not the aim of this study, various dimensions of care related to safety have been identified when exploring patients’ safety perceptions. Those dimensions seemed to be broader than the traditional risk-based views adopted by HC staff (Scott et al., 2012) and seem to be closely linked to the quality-of-care that patients experience and satisfaction with the care received, which would contribute to how safe or unsafe patients may feel within the healthcare settings (e.g., Kenward et al., 2017; Larsson et al., 2011). The social exchange theory can help explaining not only the relationship between employee safety climate, safety motivation, and safety behavior, but also the spillover effect from employees to patient; when health service users feel supported, cared for, and treated safely, they will exhibit positive and proactive attitudes and behaviors towards their interactions, thereby producing beneficial outcomes for the organization (Sierra & McQuitty, 2005), such as signaling or reminding staff about safety procedures through voicing their doubts and concerns.
Additionally, patient perceptions of staff workload have too been identified as hindrances to patient motivation to participate, as well as high staff workload and pace of work have been found to be associated to lower staff compliance (e.g., Entwistle et al., 2014; Kudo et al., 2009; Lymer et al., 2004); this highlights that perceived employees’ workload is an important dimension of both workers and patients’ safety climate, although relating to different components of their safety performance. Although no studies were found on patient safety climate, safety knowledge, and safety motivation as impacting patient safety compliance, it is reasonable to expect that better understanding of medications and treatment protocols for patients would lead to better patient compliance as well, as indicated by previous research displaying significant associations between poor patient-reported experiences while in the hospital and low patient compliance with medication instructions after discharge and increased recovery time (Beach et al., 2006; Svensson et al., 2000).
According to our results, encouraging patients’ active participation (including voicing safety concerns) appears to occur through proactive communication, education and encouragement provided by HC staff, and it can be considered a form of employee extra-role or safety participation behavior. Such behavior is important for patients to feel motivated to contribute and, ultimately, to actively participate in their own safety. It would be important for future research to test this model empirically. Those findings underscore that patient involvement with safety can only occur where HC professionals are keen on encouraging patients to get involved and will largely require operational actions to be taken by HC workers at an interpersonal level during routine healthcare delivery (Howe, 2006). Hence, patient participation in safety seems unlikely in instances where HC workers are not interested in promoting patient input (Longtin et al., 2010). This also means that workers’ safety participation could have an equally important role, if not more important than workers’ safety compliance in shaping patient safety climate. More importantly and unexpectedly, worker safety participation displayed to be crucial in impacting patient motivation to participate to safety, and it thereby calls for a redefinition and expansion of the construct of safety participation when applied to workers in healthcare, given it also involves proactively encouraging and promoting patient safety. See Figure 3 for the authors’ reviewed theoretical framework, following the findings from this review. Theoretical framework resulting from the review of literature; dotted arrows indicate new emerging relationships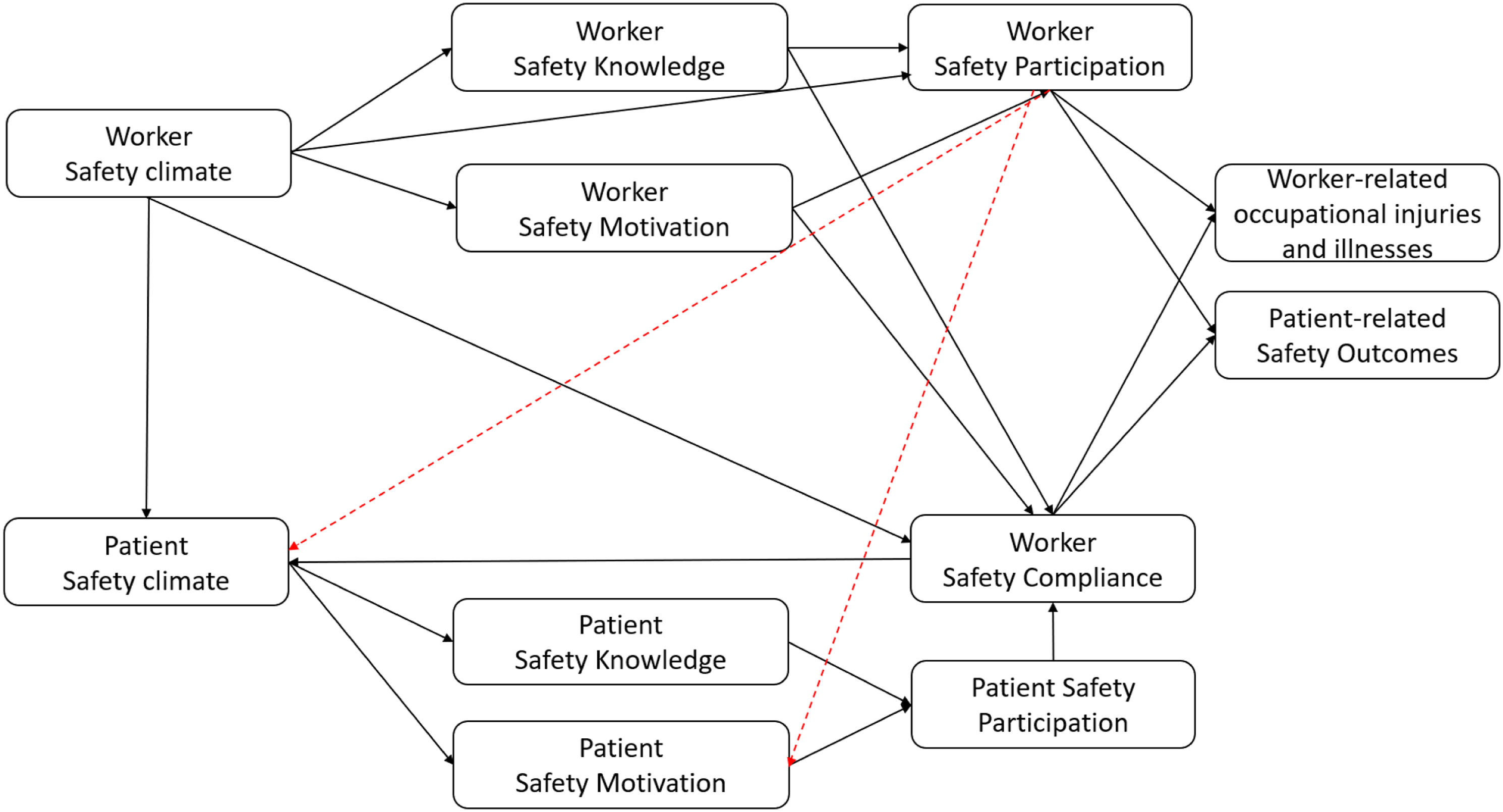
A further spillover effect would exist, as seen in the results section, by two high-quality studies, which found that both nurses and patients reported that, by taking an active part in their care, patients would contribute to lower harm and staff errors (Olsen, 2018; Schwappach & Wernli, 2010). Such result aligned with the suggestions made by various authors, that healthcare systems are shifting away from a provider-centered approach to embrace a patient-centered one, where the emphasis is on promoting collaboration between patients, families, and HC professionals in order to achieve a safer healthcare (Doherty & Stavropoulou, 2012; Sahlström et al., 2018; Vaismoradi et al., 2015). However, given the evidence found on this relationship is small (only two articles), future research should test through longitudinal designs whether patient safety participation has positive influence on workers’ safety compliance and on related patient safety outcomes.
Limitations, Future Research and Implications
The use of standard inclusion criteria might lead to overlooking studies that are not published in peer-reviewed journals, hence excluding grey literature sources which may provide valuable perspectives and limit biases (Paez, 2017). However, to ensure validity, the authors decided to use a rating system for the assessment of the quality of evidence based on the criteria established by the Institute of Work and Health (see supplementary material S2).
Additionally, our review did not differentiate between developing and developed countries, as it included only countries that have established healthcare systems based on some form of contribution. Studies that focused primarily on home-workers, such as primary care and those healthcare services that moved to telephone/online consultation since the pandemic have not been included in this study; future research should explore workers and patients’ safety perceptions, predictors, and components of safety performance in telemedicine contexts.
Also, the studies included in our literature review were based also or solely on self-reported data, which may have been influenced by respondents’ social desirability. As King and Bruner (2000) suggest, social desirability bias is more likely to occur when participants respond to socially sensitive questions (e.g., questions about the level of care provided by healthcare workers to patients). This could obscure the true relationships between the investigated variables, creating artificial relationships between them. However, ensuring participants’ anonymity and confidentiality of their data has been demonstrated to increase honesty in their responses, reducing the risk of social desirability bias (Fernandes & Randall, 1992). Additionally, self-report data is acceptable when it measures affective experiences or individual’s perceptions, such as the variables of interest in this study (Maurer & Tarulli, 1994; McEnrue, 1989; Spector, 1994).
Despite those limitations, our review opens new opportunities for future research. Firstly, the necessity to consider the role and influence of other safety agents in the healthcare industry, beyond the top management and supervisors, which seems to be overstudied in this sector. For instance, this review demonstrated the role patients have as safety agents, beyond the organizational and workforce ones, proposing a model of patient safety largely specular to the workers’, with similar relationships between antecedents, determinants, performance and outcomes of safety. Future research should also assess the role of other safety agents in their impact on safety behaviors, for example, the role of the team (i.e., peers), since the group-level climate is shaped not only by the actions of supervisors but also by the group itself, because social norms showed to impact safety behaviors (e.g., Fugas et al., 2011; Zohar & Luria, 2005). This supports what was already established by Chiaburu and Harrison (2008) about the importance for research to simultaneously examine influences from different social agents (coworkers, supervisors, organization) when it comes to employees’ safety behaviors and outcomes (Cook et al., 2016). Yet, the role of coworkers seems to be largely unstudied in the literature on safety in healthcare and across other sectors (Fugas et al., 2012).
Further, our review draws unprecedented attention on spillover effects from healthcare staff safety to healthcare user safety, and from the latter to worker’ safety compliance. Although we presented larger evidence for workers influencing patient safety rather than the opposite, both directions need to be assessed further and with robust longitudinal designs, by testing possible lagged effects healthcare workers’ safety participation has on patient safety participation, and the impact this, in turn, might have on staff safety compliance and related patient safety outcomes depending on staff (i.e., medication errors, fall, and infection rates). Moreover, only two articles tested both workers and patients injuries within the same study and as dependent on workers’ safety climate (Agnew et al., 2013; Hofmann & Mark, 2006), but they did not investigate a direct relationship between workers and patients’ safety outcomes. Future research should therefore assess whether workers’ injuries and illnesses can predict workers’ safety and service performance, subsequently impacting patient safety indicators (Green & Griffiths, 2013).
Based on the results of the review, it would be important to consider how some individual (i.e., patient-related, such as socio-demographic variables and worker related, such as personality and attitudes), organizational (staff shortages and workloads), and relational (staff-patient communication and rapport) variables can intervene in the theorized model of safety predictors and outcomes.
From a theoretical perspective, this review contributes to broadening the definition of safety participation when it comes to healthcare workers as compared to other industries. As safety participation is voluntary and entails extra effort beyond the requirements of the job role, this seems to have wider significance for healthcare providers, encompassing their initiative to educate patients on safety-related aspects of their healthcare management and treatments, and to encourage patients voicing their concerns about those. Future research will therefore need to take into consideration a broader definition of safety participation for healthcare workers, and how efforts and interventions to create safer work environments may also look at involving patients.
More widely, this review contributes to further theorizing safety participation from a co-creation lens, whereby patients (users) are recognized not merely as recipients of care but as active knowledge creators. As advocated by Papautsky and Patterson (2021), patients play a vital role in clinical spaces by possessing and sharing unique insights; without their contribution the health picture is incomplete.
The role that adult patients and care partners play in fragmented healthcare systems is being increasingly acknowledged. Recent evidence (Wust et al., 2024) highlights how patients function as both information conduits and knowledge brokers, facilitating the delivery of high-quality and safe care. Despite this, a persistent challenge remains: many healthcare professionals continue to view patient knowledge as limited or narrowly defined, leading to reluctance in involving users in service design and delivery. This underscores the need to develop more nuanced perspectives and foster trust between professionals and users (Fledderus et al., 2013).
Building trust through the co-production of public service elements requires more than simply encouraging participation. It requires reversing traditional power dynamics, enabling patients to articulate their needs and priorities regarding the safety of their healthcare management, and incorporating and adjusting to the patient’s voice at every step (NIHR, 2021). Our review frames these interactions as central to advancing safety participation.
The contribution of this review is particularly relevant for healthcare planners and public policymakers, given the healthcare sector continues to lag behind other industries (e.g., aviation and construction) in cultivating robust safety climates and participatory safety practices. Hospitals must undertake significant reforms to align with the standards of high-reliability organizations in those sectors (Gaba et al., 2003).
An important practical implication identified in this review involves getting healthcare executives involved and committed in developing action learning tools and guidelines to be implemented by frontline staff when conducting patient safety meetings, with feedback mechanisms that inform executive decision making. This involves working collaboratively with employees and the patient community, engaging them in a process of co-design and co-development of such resources. It also requires following best-practice guidance for patient and public involvement (e.g., Health Service Executive (HSE). (n.d.)), drawing on the lived expertise of patient groups and networks. In addition, it entails developing a plan to involve these groups throughout the entire project lifecycle, and identifying and prioritizing individuals who may be vulnerable, discriminated against, marginalized, or otherwise lacking power (NIHR, 2024).
Ultimately, our proposed framework adds to the growing body of literature that underscores the importance of safety culture and climate in healthcare improvement. It also responds to calls for greater conceptual clarity and refinement of definitions and dimensions within this domain (see Halligan & Zecevic, 2011; Papautsky & Patterson, 2021).
Concluding Remarks
This review proposes a framework of safety that extends from healthcare employees to include patients as safety agents, highlighting that workers and patients safety outcomes may have the same origin as attributable to employee safety climate. This study provides an expanded model of safety, where reciprocal spillover effects from workers to patients and from patients back to workers are added to the existing knowledge on safety predictors in healthcare settings. Finally, it underlines the central role staff and patient safety participation—considered as a specific type of citizenship behavior—may have on reducing staff errors and achieving safer healthcare.
Key Points
• Patients are safety agents of the healthcare system, at the same level as organizational (top management) and workforce agents • Proximal and distal antecedents of safety behaviors are the same for healthcare workers and patients; therefore, patient safety climate determines their safety knowledge, safety motivation, and safety behaviors, as it is for workers. • A spillover effect may exist from workers’ safety climate and safety participation to patient safety climate and safety motivation, ultimately impacting patient safety participation behavior. • A further spillover effect may exist from patient safety participation to workers’ safety compliance. This means that patient participation in safety can contribute to lowering patient accidents, medications and treatment errors due to workers’ actions. However, for this to happen, workers proactive encouragement to patients’ input is fundamental. • The construct and meaning of safety participation in healthcare is broader than in other industries, as it involves for staff to promote patient safety through authentic encouragement within clear communication flows and positive interactions with patients, and for patients to co-create safer health services through their active involvement.
Supplemental Material
Supplemental Material -Safety Climate and Safety Behavior and Outcomes: A Comprehensive Systematic Review in Healthcare From the Perspective of Staff and Patients
Supplemental Material for Safety Climate and Safety Behavior and Outcomes: A Comprehensive Systematic Review in Healthcare From the Perspective of Staff and Patients by Anna Paolillo, Ally Memon, and Vittorio Edoardo Scuderi in Human Factors
Footnotes
Ethical Considerations
Ethical approval from the participants is not required because this study is a systematic review based on published studies.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.