
Abstract
The objective of this study was to analyse whether variables associated with emergency services (ES) use in Spain have changed in the period 2006–2011 using a comparative analysis of the 2006 and 2011 Spanish National Health Surveys. The measure of association was the prevalence ratio with its 95% confidence interval, obtained by Poisson regression with robust variance. We studied interactions between the explanatory variables for ES use and year and subsequently performed a stratified analysis by year. ES use declined by 2.1% in 2011. Most emergency care (approximately 60% in both surveys) was provided in public hospitals. Between 2006 and 2011, ES use increased by 9% in women (p for interaction = 0.008) [ref. men], 3% in persons with poor mental health (p for interaction = 0.072) [ref. good mental health], and 8% in individuals with limitations on activities of daily living (p for interaction = 0.006) [ref. no limitations]. The change in the effect of the variables sex, mental health, and limitations on activities of daily living on use of ES (2006 and 2011) is not explained by either demographic characteristics or individual socioeconomic indicators. These results could be associated with macroeconomic and structural changes occurring during the period 2006–2011.
In recent decades, the demand for emergency health care in Europe has increased continuously, at both hospital and outpatient levels.1,2 In Spain, use of emergency services (ES) increased by 18.5% between 1987 and 2006, with the frequency of ES use in the adult population reaching 29.5%3,4 in 2006. This increase in ES use has been associated with demographic and structural changes, such as aging of the population, higher prevalence of chronic diseases, and difficulties in accessing primary care.5,6 The steady increase in ES use has been the object of study and debate, given its implications for both individuals and society. Although emergency care is an essential part of health care, it should be used judiciously. Emergency care can interfere with the provision of primary care; inappropriate use may hamper health care workers’ rapid response in life-threatening situations and, ultimately, represents a significant economic burden on the health care system. 7
The Spanish health care system provides universal access to ES regardless of socioeconomic status or place of residence. 8 Medical assistance in ES is universal in Spain for anyone requiring emergency care.
In Spain, access to health care for the immigrant population is regulated by Organic Law 4/2000. 9 According to this law, legal immigrants, as well as all illegal immigrants inscribed in a municipal register and all immigrant children and pregnant women, have the right to health care in the same conditions as the Spanish population. Illegal immigrants not inscribed in a municipal register have access only to emergency care
Multiple studies have discussed factors that influence access to health services, specifically the ES. One of the more widely used theoretical frameworks is the behavioral model of Ronald M. Andersen. 10 This framework distinguishes between population factors (predisposing, enabling, and need) and the environment or external environment (consisting of the health care system along with the political and legal framework of society). These factors are seen as determinants of personal health behaviors (e.g., smoking, diet, personal care) and use of services. These behaviors lead to objective and subjective use of services and user satisfaction results.
Among the most commonly studied indicators as determinants of ES use relate to socioeconomic level. Unemployment, low income, and belonging to the occupational class of manual workers have been identified as risk factors associated with ES use, at both individual and contextual levels.11,12 Recently published studies in Spain 13 show that living in a municipality with higher unemployment increases the probability that individuals will use hospital ES, independent of their socioeconomic level.
This is an important issue given the economic crisis that has affected Europe since 2008, which has been characterized by increased unemployment, inequality, and poverty and by implementation of structural changes that have affected the distribution of public resources in health. Between 2008 and 2011 the unemployment rate in Spain rose from 11.2% to 21.3% 14 and the index of economic poverty increased by 60%; this increase ranged between 15% and 102% across Spanish regions 15 and public expenditures on health decreased by 5.7% between 2009 and 2012.16,17
Few studies to date have examined how the economic crisis affects the use of health services. A recently published study by Lusardi and colleagues 18 analyzes how the crisis affects the use of routine primary care visits in the United States, England, Canada, France, and Germany. The results show that use of non-emergency primary care decreases with increasing poverty 18 and that this decrease is more pronounced in countries with higher co-pays per visit and/or medical prescription. In line with these results, visits to primary care physicians in Spain declined during the period 2006–2011 among the native population, but remained stable in the immigrant population. 19 The authors hypothesize that these results may reflect that seeking care entails not only out-of-pocket expenses, but also costs of time away from work or job hunting.
With regard to the use of ES, a study by Hughes and Khaliq 20 found that that a one-point increase in the national unemployment rate produced an increase in the use of both hospital and outpatient ES. 20 In Spain, García Subirats and colleagues 19 reported that ES use did not change between 2006 and 2012 in either the native or immigrant population. However, we do not know whether the effect of the variables associated with the use of ES has changed during this period of economic crisis, which is the main objective of our work—the change in these determinants. It is important to know whether or not social inequalities in health services use in Spain have changed during the period of economic crisis. Based on the foregoing, the objective of this study was to analyze whether the variables associated with ES use in Spain changed during the period 2006–2011.
Methods
Study Design and Data Source
This was an observational, cross-sectional study of data from the Spanish National Health Surveys in 2006 (SNHS2006) 4 and 2011 (SNHS2011). 21 These surveys were carried out by the National Institute of Statistics in collaboration with the Ministry of Health, Social Services, and Equality, and they include the non-institutionalized adult population (age 15 years or older in SNHS2011 [21.007] and 16 years or older in SNHS2006 [29.478]). Stratified, multistage sampling was used. The first-stage units were census sections, the second-stage units were housing units, and the third-stage units were individuals. People whose last hospitalization was for a birth (643:403 in SNHS2006 and 240 in SNHS2011), and those aged 15 years in SNHS2011 (122), were excluded from the analysis.
The Spanish Hospital Morbidity Survey in 2011 says that 76.2% of hospital admissions (public and private) related to pregnancy, childbirth and/or postnatal care were admitted for ES. 22 Because use of ES includes the last 12 months, women whose last entry in this period was for childbirth are excluded; otherwise, results might be reflecting the increase or decrease of birth in this period. 23 This is especially important in times of crisis, like the present, when a drop in the birth rate has been observed.
Variables
The dependent variable analyzed was use of ES in the last 12 months, based on the question “In the last 12 months, have you had to use any emergency service for some problem or illness?” Taking as reference Andersen’s model of access to health care systems, 9 the independent variables were structured as follows.
Predisposing Factors
Age, coded as 16–34 years/35–64 years/65 years and over; sex (man/woman); and place of origin 24 (country of birth), grouped into six categories: Spain/High-Income Countries (Western Europe, Central Europe, United States, Canada, and Australia)/Eastern Europe/Africa/Asia/Latin America. To define these categories, we considered geographic proximity criteria, economic criteria, cultural proximity, and size categories, which have been used in other studies. 24 For further analytical study, we recoded into four categories: Spain/High-Income Countries/Eastern Europe–Africa–Asia, and Latin America; highest educational level completed; employment status, coded as employed/unemployed/not seeking work; and social class. The categories of social class have been drawn from the proposal made by the Working Group Determinants of the Spanish Society of Epidemiology, where social class is assigned according to occupation of the person interviewed.25,26 To enable data comparability between both surveys, we coded the variable social class as non-manual workers (social class I, II, and III) and manual workers (social class IV, V, and VI).25,26
Factors Related to the Need for Care
Self-perceived health status in the last 12 months, coded as positive (very good or good) and negative (fair, poor, or very poor). Adult mental health, referring to the past few weeks, was assessed by the GHQ-12 questionnaire, using a cut-off score of 3. 27 The number of chronic diseases diagnosed by a physician in the last 12 months was coded as none/one or two/three or more diseases. Finally, information was collected on limitations in the activities of daily living (yes/no).
Enabling Factors
Health coverage was coded in four categories for the analytical study. Responders were asked to specify the type of health insurance they had; we re-codified the possible answers with a maximum two per person as follows: public coverage (national health system and mutual insurance companies benefiting from the social security state), private (individual or company private insurance and mutual state benefiting from private insurance), mixed (when the answer was to either), and other situations. Social support, which was measured with the Duke-UNC questionnaire, using a cut-off score of 32, 28 was coded as low or normal support.
Health Behavior Indicators
(1) Lifestyle: smoking (smokes/does not smoke); (2) ES use: frequency of use of ES in the last 12 months. Responders were asked for the times they had to use an ES in the past 12 months; we re-codified the possible answers into three categories: once, twice, or three or more times. Regarding the most recent ES use, the type of ES was coded as: public hospital/public non-hospital ES/private service/other. The person who requested emergency care was coded as: patient’s own initiative, physician referral, or unknown.
Analysis
We first performed a descriptive study of each survey. We calculated the distribution of the independent variables by ES use in the last 12 months. The association of the dependent variable with the independent variables was estimated by the Chi-square test (Wald). For the analytical study, we first combined the two surveys (2006 and 2011) into a single database and included the variable year of survey to estimate if ES use differed between 2006 and 2011. We then studied the association between ES use and the previously described covariables. The measure of association was the prevalence ratio (PR) with its 95% confidence interval (CI), obtained by Poisson regression with robust variance. After the univariate analysis, a multivariate analysis was carried out using forward selection for inclusion of variables. To estimate if the effect of the covariables on ES use differed between years, we analyzed possible interactions of the explanatory variables with the variable year. A value of p ≤ 0.1 in the test of interaction (Wald Chi-square) was considered statistically significant. Given the presence of multiple interactions, we then performed a stratified analysis by year, using the model previously described. Increases, in case the interactions are significant, are calculated as follows: [(PR2011 − PR2006)/PR2006]*100.
The weighting coefficients included in the surveys were taken into account in both studies. The statistical programs used were STATA13 and SPSS19.
Results
After excluding persons aged 15 from the SNHS2011 survey and women whose last ES use was to give birth, the subsamples analyzed were made up of 29,075 persons in SNHS 2006 and 20,645 persons in SNHS2011.
Description of Spanish National Health Surveys in 2006 and 2011. a

Without childbirths (n = 643).
Variables Describing Use of Emergency Services. Spanish National Health Surveys, 2006 and 2011 a .
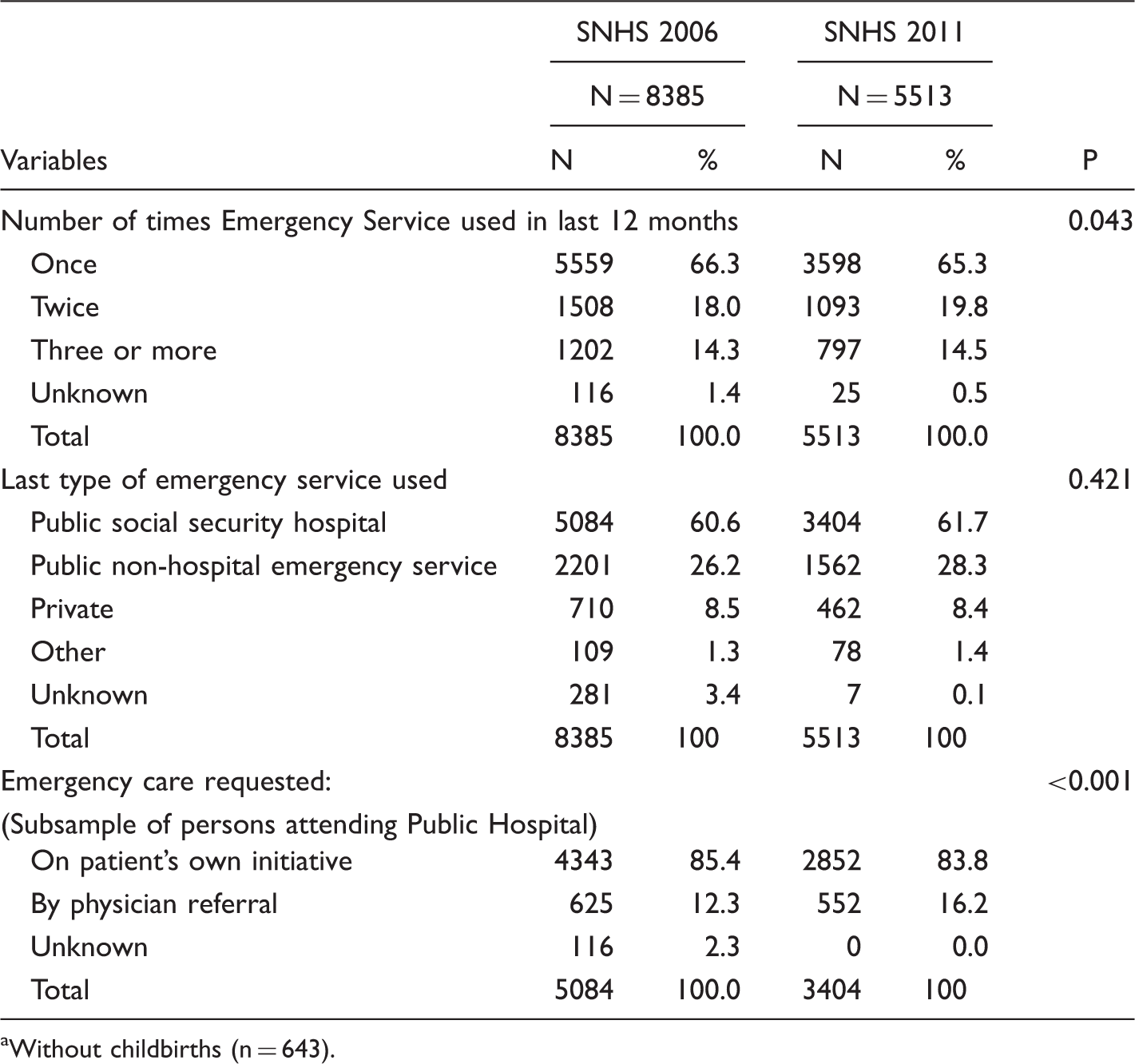
Without childbirths (n = 643).
Variables Associated with Emergency Services Use in the Last 12 Months, 2006 and 2011. Multivariate Analysis by Poisson Regression With Robust Variance.

Prevalence of Emergency Services use by each explanatory variable.
PR: Prevalence ratio. Values adjusted for variables included in the model and for Autonomous Community (region) of residence.
Includes vocational training.
Discussion
The use of ES in Spain decreased by 2.1% between 2006 and 2011, although this decline can be explained by sociodemographic changes and changes in the health status of the population. Regarding the effect of variables associated with the use of health services between 2006 and 2011, ES use increased significantly in women compared to men, in persons with poor mental health vs good mental health, and in persons with ADL limitations compared to those without such limitations.
The fact that, after eliminating the effect of sociodemographic characteristics and health status of the population, ES use in Spain remained stable between 2006 and 2011 signifies a break in the upward trend in ES use registered in the health surveys in Spain in the period 1987–2006. 3 Given that this phenomenon is not explained by changes in individual characteristics of the Spanish population, it may be associated with structural variables related to the macroeconomic context, although this hypothesis is not supported by the scientific evidence found to date. In this regard, the recently published study of Hughes and Khaliq 20 found an association between the national unemployment rate and increased use of ES at the individual level. In the same line, a study in Spain has shown that increases in the municipal unemployment rate increase the use of hospital ES. 16
Women’s use of ES remained practically the same between 2006 and 2011 (29.7% vs. 28.6%) whereas men’s ES use declined from 27.9% to 24.7%. This decline in men may be related with a decrease in the number of accidents produced during periods of economic crisis, as several authors have reported.29,30 Unemployment reduces the risk of accidents in or while commuting to the workplace; in addition, declining income reduces the amount of road travel and, consequently, the probability of suffering an accident. 31 Another possible explanation could related to better access to primary care in this population group. In this regard, the decrease in the use of hospital ES on one’s own initiative (from 85.3% to 83.8%) would support this hypothesis.
With regard to mental health, our results show no changes in the prevalence of poor mental health in Spain between 2006 and 2011. However, the use of ES decreased among both persons with good mental health (from 25.9% to 23.6%) and those with poor mental health (from 43.3% to 41.9%). Our results corroborate the study carried out by Wittchen and colleagues 32 in European countries; after conducting a systematic review, these authors concluded there were no changes in the prevalence of mental illness in Europe in the period 2005–2010 32 and that the demand for care for mental health problems even declined. 33 In contrast to these results, a study carried out in Spain in a primary care setting reported an increased prevalence of mental illness in both men and women during the period 2006–2011. This increase was accompanied by a greater demand for health care for these disorders. 34 In this regard, the fact that neither our study nor that of Wittchen and colleagues 32 were conducted in the framework of primary care, but rather represent the adult general population, could be behind these discrepancies.
A result not described to date is the fact that the association between mental health and ES use was 3% higher in 2011 than in 2006. It is possible that the evolution or presentation of mental illness was more severe in 2011 than in 2006, which would increase the magnitude of this association. In this regard, the rise in suicides in both Spain and other Mediterranean countries,35–37 as well as the increased use of toxic substances,35,38 could support this hypothesis.
With respect to ADL limitations, it is important to note that this is the only population group in which ES use increased in the period 2006–2011 (from 50.1% to 53.2%). Furthermore, the magnitude of the association between having vs not having ADL limitations 39 and ES use increased by 8%. This could be due either to more serious health problems limiting ADL in 2011 than in 2006 40 or to increased waiting time for primary care consultations. 41 In this regard, some studies have shown that decreased waiting time in primary care decreases ES use. 42 On the other hand, although occupational status cannot explain these results because this variable is included in the regression models, worsening occupational conditions could explain them in part.43–46 Poorer working conditions and job instability, as well as economic burdens on families in much of the Spanish population in the economic crisis, could promote the need to respond quickly to problems that limit activity and, therefore, their greater use of ES, as Segura’s study seems to suggest. 47
When interpreting the results of this study, its limitations must be kept in mind. The information collected in the survey is self-reported, which could introduce a recall or social desirability bias. With regard to the study design, because it is cross-sectional, we cannot assume causality in the observed associations because we do not know the time interval between the cause and the effect. Some explanatory variables for ES use, such as living with a partner or reproductive history, could not be included because they were collected differently in the two surveys. Likewise, information on income level was not available at the time of this analysis.
Information about household tasks and caring for disabled family has been included in a different way in the SNHS2006 and in the SNHS2011, so these variables could not be included in the analysis. Similarly, the surveys did not include information about the type of employment contract that people had.
Conclusions and Recommendations
Use of ES has not varied in the period 2006–2011, which represents a break in the upward trend in ES use registered in the Spanish National Health Surveys in the period 1987–2006. Poor mental health, limitations in ADLs, and gender are predictors of ES use that increased in magnitude between 2006 and 2011.
Given that these effects are independent of the individual-level variables associated with ES use, these changes might be explained by a differential impact of political and social policies on different social groups. Knowing the factors that affect the use of health services is a key element in the design of health policies, because changes in these may affect the budget estimates of public funding, planning of the portfolio of services, considerations of equity in access to health services by all groups in the society, and the sustainability of the health system itself.
Footnotes
Acknowledgment
CIBER of Epidemiology and Public Health (CIBERESP), Spain.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article.