
Abstract
In 2001, Ireland announced a Primary Care Strategy that has led to the implementation of primary care centers (PCCs) throughout the country. This article examines the nature and extent of private and public sector involvement in establishing the PCC network since 2001. The study is based on a PCC dataset constructed using unpublished data obtained from Ireland’s Health Service Executive (HSE). The dataset includes the date when PCCs became operational and their mode of delivery: public procurement, private lease, or public–private partnership. The results show that 140 PCCs have or will become operational by the end of 2019: 35% (49 PCCs) are public, 55% (77) are leases with private landlords, and 10% (14) are public–private partnerships. Before 2009, PCCs were delivered by traditional public procurement, but since 2009, private delivery methods have been prioritized. In conclusion, the PCC network has been increasingly implemented by relying on the private sector. This results in a more commercialized network subject to financial risks associated with public–private partnerships.
A significant body of international evidence suggests that effective primary care systems are associated with better health, lower total health costs, and more equitable access to health care services,1–3 which has led the World Health Organization (WHO) to call for strengthening primary care systems globally. 4 Primary care systems usually involve a public–private mix of providers and funding sources, which varies from one country to another. 5 In recent years, a number of countries have attempted to reform their primary care systems by providing more space for the private sector and market forces. The objectives include a desire to give more choice to patients while achieving financial savings and efficiency through competition. The type, scale, and speed of these changes are significantly diverse. In England, reforms have sought to improve patients’ choices and stimulate competition between providers by awarding contracts to private companies to provide general practitioner (GP) services.6,7 In Sweden, reforms have involved choice of provider for the population and freedom of establishment for private primary care providers. 8 Australia has witnessed the corporatization of general practices. 9 In China, the ownership (public or private) of primary care facilities varies geographically. 10
Those reforms reflect global trends over the last several decades by which health care systems have been gradually restructured to incorporate private providers, sources of finance, and management principles.11–20 The precise nature of those policies, their causes and impacts vary geographically. Ireland has followed the general trend, as documented by historical and health system surveys,21–23 as well as case studies of acute hospitals,24,25 nursing homes 26 and social care, 27 within a political context favorable to neoliberal privatization.28–34 However, in Ireland and elsewhere, the nature and extent of private sector involvement in the primary care sector remains to be fully documented and understood. In particular, the extent and role of private sector involvement in primary care centers (PCCs) has not been examined systematically. Existing work has focused on the experiences of primary care teams (PCT) members,35,36 including social workers 37 and public health nurses, 38 as well as community participation in primary care. 39 The genesis of the 2001 Strategy and the factors that inhibited the achievement of some of its policy objectives with regard to functioning PCTs have also been examined. 40
This article seeks to address these shortcomings. It asks, what has been the nature and extent of private sector participation in the development of Ireland’s PCC network? While focusing on the PCCs’ source of finance (public or private), various aspects of private sector involvement are also discussed. As will be seen below, the implementation of the PCC network has taken place within a largely private system of primary care delivery. The PCCs constitute an adequate case to study the reform and restructuring of the Irish primary care system. Indeed, the Health Service Executive (HSE) conceives of the PCCs and PCTs as central to the national primary care strategy. 41 The remainder of this section introduces the Irish (primary) health care system in order to contextualize the role and place of PCCs within it.
In Ireland, the health care system involves a complex mix of private and public provision and financing.42–44 Health care financing comes predominantly from public sources, but private health insurance and out-of-pocket payments by individuals are also significant. Entitlements to public health services fall into two main categories. Individuals in category I (full medical cardholders) may access free public health services, including outpatient and inpatient hospital care, GP care, and other primary and community care services (however, they must pay a co-payment for prescription items). Individuals in category II must pay the full cost of GP services and primary and community care services but may access public hospital services and prescription medicines at subsidized rates. 45 In 2010, the national average price of a GP consultation was estimated at €51. 46 Also, in 2005, the GP visit card was introduced: individuals who hold one are entitled to free GP consultations but otherwise have the same entitlements as those in category II. Eligibility for medical or GP visit cards is assessed primarily through an income means test, although the cards may be granted on a “discretionary basis” for those whose health needs might cause undue financial hardship. Additionally, the availability of voluntary private health insurance adds a further layer of complexity. Approximately 43% of the population holds private health insurance (2016 data), 47 which provides coverage mainly for private or semi-private acute hospital services. 48
In the Irish primary care system, the private sector plays a relatively important role compared to other Western European countries.22,49 Ireland is the only country in Europe that does not offer universal coverage of primary health care, and the majority of individuals pay privately for primary care. 50 GPs are self-employed and sell their services in a private market, while holding state contracts to supply services to the minority of the population who can access care free of charge (e.g., medical or GP visit cardholders). GPs themselves have typically undertaken investment in GP practices. According to recent estimates, there are 64.4 GPs per 100,000 people in Ireland, significantly lower than the European average of 91 GPs per 100,000. 51
The primary care system faces challenges in terms of access. A comparative study of primary care systems in 31 European countries evaluated access to primary care services in Ireland as “weak” (on a 3-point scale, “strong,” “medium,” “weak”). 52 Recent evidence also suggests that in Ireland, individuals without free primary care or private health insurance are more likely to report an unmet need for health care. 43 Therefore, Irish health professionals associations, GPs, and analysts have stated that the primary care system should be improved,53,54 asserting that the “need for large investments in the primary care infrastructure … is one of the most urgent needs in the entire Irish health care system.”22(p156)
Echoing these calls, a political consensus in favor of introducing free GP care has emerged recently. In 2015, free GP visits for all children under the age of 6 and all adults aged 70 years and older were introduced. 42 In 2017, a cross-political party report, Sláintecare (sláinte means “health” in the Irish language), reiterated the need to improve the primary care system and recommended the implementation of universal GP care. 55 The report also recommended that PCCs be used as “the hub of community diagnostic services so that all patients can access diagnostics in these centres.”55(p24) Although the extent to which Sláintecare will be implemented remains to be seen, putting into effect some of its key recommendations in primary care could fundamentally alter the context in which GPs are employed and investment in PCCs occurs.
In sum, the development of the PCC network has occurred within a largely private primary care system. The PCCs originate from the government’s landmark Primary Care Strategy (hereafter, Strategy), 56 published in 2001. The Strategy suggested that about 400 to 600 PCCs should be established within a decade (by 2011) and that between 600 to 1,000 would be required in total in the longer term. 56 However, in 2010, the HSE revised the total number of PCCs required in the long term down to 542. 41 It is within this context that the 140 PCCs in operation by 2019 should be examined (there were no PCCs before 2001).
The 2001 Strategy recommended to set up one PCT (or, in some cases, several PCTs) within a PCC so that the team could operate under one roof and offer coordinated services to a geographical area of between 3,000 and 7,000 inhabitants. 56 A PCT would include GPs, nurses, midwives, physiotherapists, home help, occupational therapists, social workers, and administrative staff. Moreover, a wider network of health professionals (e.g., a speech therapist, a dietician, a psychologist, a dentist, a chiropodist) would provide groups of several PCTs with additional services. Enrollment would remain voluntary, but all individuals were to be encouraged to enroll with one PCT and with a particular GP within that team (while remaining free to switch to another PCT and GP). PCCs could be either purpose-built or set up in existing infrastructure that would be refurbished. The role of the private and public sector in their establishment was not predetermined, and the government specified that a varying mix of public and private input could be used. 57
Methods
No comprehensive data on PCCs in Ireland have been published. Therefore, data had to be collected and used to construct a systematic PCCs dataset (Table 1). To do so, requests were made to HSE Estates via email and telephone. HSE Estates is the body responsible for the HSE’s infrastructure (properties and facilities). Conversations with HSE officials clarified certain aspects of the collected raw data. Data requested and obtained from HSE Estates include a list of all existing PCCs as of the end of 2018 as well as PCCs planned for delivery in 2019. For each PCC, the following information was obtained: its geographical location, the year that it became operational, and its delivery mode (public procurement, lease, or public–private partnership [PPP]).
Primary Care Centers in Ireland.

Abbreviations: HSE, Health Service Executive; PCC, primary care center; PPP, public–private partnership.
Public – PCC established through traditional public procurement. Lease – the HSE leases space in privately owned PCCs. PPP – PCC built and managed via public–private partnership.
Several caveats should be mentioned about these HSE data. First, 25 PCCs were established in the early years of the Strategy for which the HSE could not provide a precise year when they became operational – the HSE only specifies that they became operational before 2008. All these 25 PCCs are public (HSE owned). Table 1 lists these PCCs as becoming operational before 2008 (“<2008”). For the purposes of the discussion below that examines the varying significance of public and private delivery modes over time (Figure 1), these 25 PCCs were allocated evenly to the years between 2003 and 2007 (in other words, it was assumed that 5 of these PCCs became operational every year between 2003 and 2007). Using 2003 as the earliest year at which such PCCs would have been established was motivated by the fact that there is no indication that any PCC were established before 2003 – the first PCC for which a precise date is available is 2003 (the Virginia PCC, see Table 1), and it is only in October 2002 that the Department of Health provided funding for 10 pilot sites where PCCs could potentially be established. 22
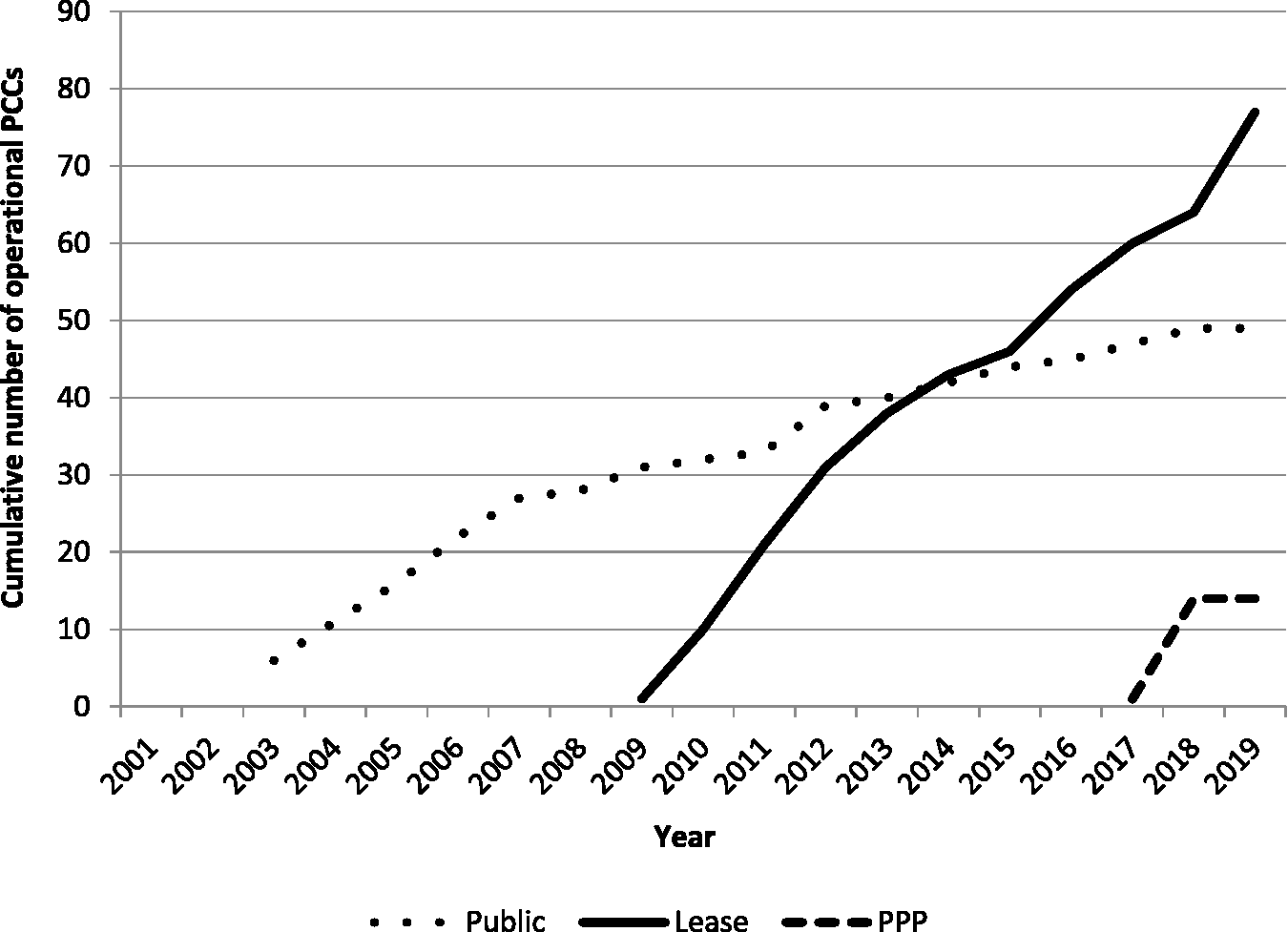
Cumulative number of primary care centers operational by mode of delivery, 2001–2019. Source: Table 1.
Second, the dataset indicates that the first PCC delivered through a lease with a private landlord was established in 2009 (Letterkenny PCC). However, readers familiar with the Irish PCC network may note that there were reports of leased PCC projects before 2009. In particular, in 2005, a businessman called Fergus Hoban had announced plans to develop up to 60 “primary care facilities” in the country. 22 However, these plans were not fully realized due to Ireland’s property crash of 2008–2010. Only a few of these facilities were built (e.g., the Mulhuddart primary care center), but the HSE does not include them under the Primary Care Strategy and in the list provided to this author because the facilities were substandard and the leases agreed with the HSE were short-term and not standardized. For example, GPs were not required for leased PCCs before 2009, whereas the presence of GPs is essential and central to existing PCCs. Moreover, under the Primary Care Strategy, leased PCCs all have standard 25-year leases, and it is these that are considered in this article.
Third, the above 2 caveats suggest that it would be possible to construct a slightly different dataset if, say, one was to vary certain definitional elements of a PCC. However, an additional advantage of using this article’s dataset is that it conforms to official pronouncements by the HSE, the Department of Health, and Ministers of Health, who obtain their information from HSE Estates, which is the official repository of data on the PCC network. This has the advantage of making it possible for readers to directly compare this paper’s data to official statements about progress and developments in the PCC network. 58
Results
Table 1 presents the data collected on every PCC established since 2001 as well as those that will become operational in 2019. Of the 140 PCCs, 49 are public (built through traditional procurement), 77 are operated through a lease, and 14 were established through PPP.
One key difference between these modes of delivery is the source of finance for capital expenditure: public PCCs are built through public finance, whereas leased PCCs and PCCs established through PPP are built through private finance. Also, in all delivery modes, GPs occupy the PCC premises and operate privately. More specifically (for details, see Mrowka 59 ): (1) the public model is a conventional model of public procurement whereby the government procures public infrastructure funded by the exchequer. Construction firms build the PCC under contract with the government, which has a relatively large degree of control over the building design. When the premises are built, the HSE owns the PCC and assumes responsibility for its maintenance and operation. (2) In the lease model, a private landlord owns the PCC and leases space to both the HSE and private health companies, typically through a 25-year lease. HSE and private health professionals thus work side by side. The facilities may have been purpose-built or already existing, and the government has less input on its design and specifications. (3) In the PPP model, a private company is responsible for designing, building, financing, and maintaining a PCC for a contract period of 25 years. The private company raises all necessary finance to build the facility, through a combination of debt (e.g., bank loans) and equity. When the PCC becomes operational, the HSE formally owns the facility and land on which it is located, but the private company operates and maintains the facility through a licensing agreement with the HSE. The HSE pays a monthly “unitary charge” to the private company for the duration of the contract (25 years) as compensation for construction work and maintenance of the facility. During that time, the HSE occupies floor space in the PCC. The HSE and other health professionals occupying the facility (e.g., GPs) are responsible for clinical operations, while the private company is responsible for building management and maintenance. At the end of the 25-year period, in theory, the HSE intends to take control of the facilities and the private company would leave the project, although this has not happened yet because PCCs delivered through PPP have not yet reached the end of the 25-year licensing period.
Figure 1 presents the chronological evolution of the PCC network since 2001. Of the 140 PCCs that are operational or planned for 2019, 35% (49 PCCs) are public, 55% (77) are delivered through lease, and 10% (14) are delivered through PPP. It can be seen that in the early years of the Strategy (before 2009), PCCs were delivered by traditional public procurement – 28 in total were delivered between 2001 and 2008. However, since 2009, private delivery methods (lease and PPP) have been prioritized. Between 2009 and 2019, 112 PCCs were or will be established: 77 through leases, 14 through PPP, and 21 through public procurement.
Discussion
The previous section described the development of the PCC network since 2001 and showed that modes of delivery using private sources of capital expenditure have been prioritized in recent years. This section aims, first, to outline the factors that have motivated this strategy, and second, to discuss some of the potential consequences of this development path.
Reasons for Private Sector Participation
There are several reasons why the 2001 Strategy ultimately was implemented with significant private sector involvement, particularly to finance capital expenditures to build the PCCs. First, private sector participation in the development of the PCC network was always an option considered by policymakers. Indeed, the 2001 Strategy stated that “the role of public–private partnerships and other options will be explored” to establish the PCC network. 56 In 2005, Minister for Health Mary Harney voiced support for private options to deliver primary care facilities. 22 In 2008, the HSE requested expressions of interest from developers to deliver a number of PCCs and agreed on leases for these facilities, and the first became operational in 2009 and 2010 (see Table 1). 60
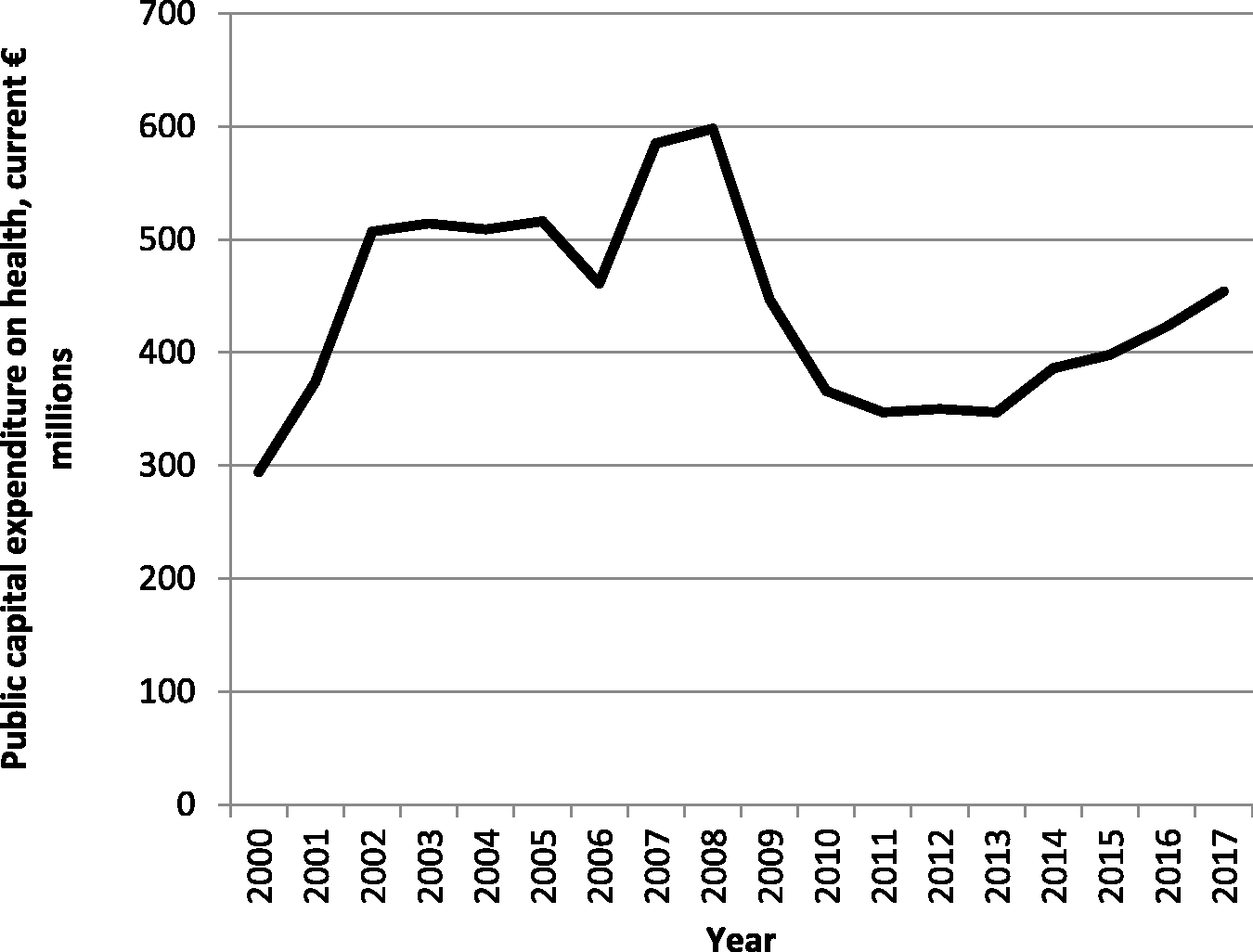
Second, in response to the 2008–2009 financial crisis, Ireland, following other European countries, implemented a program of fiscal consolidation in 2008–2014, during which public capital spending was curtailed significantly (Figure 2). Total public capital spending on health decreased from €598 million in 2008 to €447 million in 2009, reaching its nadir in 2011 (€347 million). This constrained public capital spending on PCCs through traditional procurement.
Third, the recent use of PPP to develop 14 PCCs was motivated by the European Union’s and Irish government’s renewed support for PPP schemes in 2012. 62 In July 2012, the Irish government announced a €2.25 billion Infrastructure Stimulus Package, including €115 million allocated to PCCs, 63 of which €70 million would be provided by a 25-year loan from the European Investment Bank. 64 The 14 PCCs delivered are products of this investment plan.
Fourth, global investors have recently entered the Irish PCC market because it offers relatively high profit opportunities. 65 The fact that the HSE rents space in PCCs from landlords through long leases (25 years) results in stable revenue streams, which is appealing to investors. 66 The renewed government and European Investment Bank commitment to developing PCCs, exemplified by the 14 PCCs bundle delivered through PPP, also provides a political and economic context supportive of a growing PCC network.65 Moreover, the government has recently pledged to develop more PCCs as part of its national development plan Project Ireland 2040, 58 which is positive for investors.
Potential Consequences
The PCC network has been developed using a mix of public and private delivery modes. However, over the last few years, leased and PPP facilities have been prioritized. This section discusses some of the potential consequences of this development strategy.
First, there is an extensive literature on the privatization and commercialization of health care and the potentially negative consequences on the quality of care when commercial incentives conflict with care delivery.11–14 To what extent are PCCs subject to those trends? This article suggests the following preliminary and tentative conclusions. The HSE manages public PCCs, and no private companies operate on their premises (only the GPs practicing on the premises are self-employed private providers, as are the large majority of GPs in Ireland). Commercial incentives that would affect PCC operation can thus be assumed to be relatively small. In PCCs delivered through PPP, the HSE is responsible for all clinical governance, and no health care private companies operate on the premises (only the PCC’s GPs are self-employed private providers). Private companies only play a role in building management. 67 Therefore, the main impacts associated with private sector involvement are fiscal (see below).
On the other hand, private entities and market forces play a more important role in PCCs operated through lease. These facilities often include private for-profit health care companies on their premises along with HSE health professionals and self-employed GPs. These may include commercial pharmacies, diagnostics firms that provide scans and tests, and specialized doctors (consultants) who work for private for-profit hospitals, among others. For-profit operators may negatively affect the quality and cost of services delivered, as scholars have shown for the hospital and nursing home sectors.13,14 In particular, the HSE has acknowledged the problem of pharmacy co-location in PCCs because it may lead to “patients being subjected to inappropriate and unnecessary treatments for the economic benefit (either directly or indirectly) of the parties owning the facilities” as well as to a loss of pharmacy choice for patients.68(p16) For similar reasons, the Pharmaceutical Society of Ireland stated that the co-location of pharmacies with GP units could lead to “the adoption of unprofessional work practices,” which “is not in the best interest of public health.”69(p6) Further research would be necessary to examine more systematically those potential consequences.
Second, the recent emphasis on PPP delivers short-term benefits to the exchequer but also poses longer-term financial risks. The main advantage of PPP to the state is that most of the private borrowing tied to the project is off-balance sheet for national accounts purposes. 70 Therefore, this arrangement results in lower amounts of recorded government debt in the short term. It is thus beneficial to the state because it can generate investment in capital projects when it does not have sufficient capital budgets. Reimbursement costs are spread over time and easier to manage on an annual basis. This strategy proved useful in recent years due to the challenging fiscal environment in which the Irish government has operated. 62
However, over the duration of the 25-year contract, cumulative annual payments by the government risk exceeding the costs of direct government procurement. Indeed, a recent major report calculated that in the United Kingdom total PPP costs are about 40% higher than traditional procurement. 70 Moreover, reviews of the European experience with PPP in the health sector concluded that performance has been “mixed” and has “not met expectations for achieving greater efficiencies at lower costs.”71(p.146),72 Reviews of the Irish experience have also concluded that PPP schemes have frequently proved more costly to the state than expected.73,74 The additional costs arise because private borrowing interest rates are higher than government borrowing interest rates, a portion of the total project costs are absorbed by profits to the private company, while the state must pay insurance costs, external advisers, as well as management and administration fees. In theory, these costs could be outweighed by higher quality projects or efficiency savings, but little empirical evidence supports this claim.70,75
Conclusions
Ireland’s primary care system, and in particular, the services offered by GPs, are in many respects private. It is within this context that the establishment of PCCs has proceeded over the last decade. Private sources of finance for capital expenditures have been prioritized, and thus the growth of PPP and leased facilities has outpaced the construction of PCCs financed by public capital expenditures. Leased PCCs have also involved private for-profit firms on their premises to deliver certain health care services. In this respect, Ireland has followed global trends in which health systems rely on private finance and market mechanisms to a larger extent than previously.
Three main sets of issues should be addressed in further research. First, in recent years, the PCC network has been expanded by relying mostly on PPP and leases as modes of delivery. This has alleviated budgetary pressures; however, in the longer-term, financial costs could turn out to be higher than they would have been under conventional public procurement. Assessing precisely the financial benefits and downsides of this strategy will be an important task for health researchers and economists.
Second, the current and further use of leases to run PCCs means that potential conflicts between market forces and clinical best practice should be described and analyzed precisely in order to reduce them where possible. Tighter government regulations, for example, could alleviate those problems. However, the first step should be to identify the practices that could prove problematic.
Third, trends in large multinational and domestic investments in the primary care market should be documented systematically. Analysts expect further transactions in the short-to-medium term. The growth and evolving patterns of investment should be described and understood precisely because they have the potential to restructure and transform the existing PCC network and primary care system. For example, what are global investors’ precise goals and objectives, and how are they different from domestic, smaller-scale landlords?
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.