
Abstract
The gradient in health inequalities reflects a relationship between health and social circumstance demonstrating that health worsens as you move down the socioeconomic scale. Norway’s Public Health Act (PHA) specifically aims to tackle the gradient by addressing the social determinants of health. In this article, we draw on data from 2 studies that investigated how municipalities in Norway deal with these challenges. In doing so, we apply theoretical perspectives, as defined in the Gradient Evaluation Framework (GEF), to analyze the implementation of the PHA at the municipality level. The article aims to describe and analyze how local governments follow the requirements of the act. In doing so, we address the following research questions: Which policies are implemented at the local level to reduce social inequalities in health among families and children? How is intersectoral collaboration carried out, and who is taking part in the collaboration? The article draws on both quantitative survey data from questionnaires sent to all Norwegian municipalities and qualitative interview data in 6 municipalities. The findings show that there is raised awareness of the significance of social determinants among an increased number of municipalities, indicating that the PHA is being implemented according to its objectives.
In many countries of the European Union, considerable gains in population health have been achieved over the last few decades, with citizens now living longer and healthier lives than previous generations. 1 Despite this, however, large inequalities in health status persist between and within countries, with evidence suggesting that these inequalities are increasing.2,3 Moreover, substantive evidence suggests a social gradient in health inequalities (HI), demonstrating that health becomes worse as you move down the socioeconomic scale.4–6
The causes of HI are complex and involve a wide range of factors, which relate to the wider social determinants of health, including living conditions, health-related behaviors, education, occupation and income, health care systems, and health policy. As many inequalities are not simply a matter of chance or choice and are instead influenced strongly by a range of factors, such as the actions of governments (e.g., policy), stakeholders, and communities, this means that they are not necessarily inevitable and can be prevented. 7 Consequently, action to tackle health inequalities through healthy public policy means addressing those factors that are deemed inequitable and preventable and that affect the health of the population unequally. This means that in practice, reducing HI is difficult and has been termed a “wicked” problem, denoting a complex issue with multiple root causes and no simple solution.8–10 Approaches targeting only the most disadvantaged populations are unlikely to be effective in leveling-up the gradient and may even contribute to an increase in HI (for example, due to increased stigmatization). Instead, a gradient approach to policy is arguably required, which necessitates not only a focus on disadvantaged populations but also a focus on the upstream determinants of health inequities (such as income, education, living, and working conditions).
It is likely that low socioeconomic status during childhood may influence adult health status even if an individual has experienced upward social mobility.11,12 This would suggest that efforts to level-up the gradient in health should pay particular attention to children and young people, as interventions at these early stages in the life cycle may well offer the greatest potential of leveling-up the gradient and facilitating long-term positive health outcomes. For instance, welfare policies that aim to provide children and their families with, inter alia, a decent standard of living (e.g., a “living wage”) and access to high-performing schools, may well contribute positively to child health and well-being. In addition, family policy generosity and the child poverty rate are clearly related; countries with more generous family policies tend to have substantially lower child poverty rates. 13
For a number of years, Norway has been ranked at the top of the United Nations’ Health Development Index, which is a summary measure of average achievement in key dimensions of human development. Norway belongs to the “social democratic” welfare regime, characterized by its emphasis on solidarity, universalism, and the redistribution of resources among social groups, mainly through progressive tax systems. 14 However, even though the overall picture of Norway is positive and a Public Health Act (PHA) with a focus on reducing the gradient in health inequalities has been adopted, the country nevertheless has its challenges with a seeming increase of social inequalities in health. 15
Consequently, over the last decade the Norwegian national government has developed a number of specific policies to reduce HI, with leveling up the social gradient by action on the social determinants of health as a core public health objective. 16
The present article aims to describe and analyze how local governments in Norway follow the requirements of the Norwegian 2012 PHA by applying theoretical perspectives as defined in the Gradient Evaluation Framework (GEF). 17 In doing so, we address 2 research questions: How is the concept of social inequality understood and applied? How is the “health in all policies” (HiAP) approach to reducing social inequalities in health among families and children carried out? To address this, first, we present the Norwegian Public Health Act. Second, we present the conceptual foundations and structure of the GEF framework. Third, we present our methods; fourth, we present our results; and lastly, we discuss the findings and draw conclusions.
The Norwegian Public Health Act
In January 2012, the Norwegian national government adopted a new Public Health Act (PHA). 18 The purpose of the PHA is to contribute to societal development that promotes public health and reduces social inequalities in health. The act provides a broad basis for the coordination of public health work both horizontally across various sectors and actors as well as vertically between authorities at local, regional, and national level. In the act it is stated that only by integrating health and its social determinants as an aspect of all social and welfare development through a “whole-of-government” approach can good and equitable public health be achieved.
The PHA is explicitly underpinned by the principle of “health in all policies” (HiAP). 19 HiAP is an approach to public policies across different sectors (e.g., education, health, transport, housing, etc.) that systematically takes into account the health implications of such policies to improve population health and reduce health inequity. Intersectoral action is therefore regarded as key to reducing HI. In governance terms, one of the main features of intersectoral action is that it places responsibility for public health work as a whole-of-government responsibility rather than a responsibility of the health sector alone.
In Norway, the PHA has been developed at the national level. Central actors involved in the act’s development have been policymakers from the Directorate for Health who were inspired by the wider international social determinants agenda. 7 Subsequently, when a left-wing government came into office in 2005, a window of opportunity for adopting the policy was created and subsequently capitalized on. 20
The adoption of the PHA gave the Norwegian central government a strong mandate for implementing the policy, and this top-down strategy included mandating the municipalities to integrate the policy into their own plans and budgets. Via the county governor, the national authorities are now able to oversee and audit the municipalities’ implementation of the act. Other national governance tools have included information and guidance to the administrative levels at regional and local levels. A study from 2013 indicated that policymakers at the national level were advocates for the policy, but nevertheless municipalities did not share these ambitious aims. 21
In Norway, municipalities have a dual role: on the one hand, they are agents for the welfare state through their responsibility for implementing national policy goals. On the other hand, municipalities form independent local democratic areas that are able to decide how to use national funding in accordance with local priorities, preferences, and needs.22,23 From 2018, a total of 422 municipalities have the overall responsibility for welfare provision, including services such as preschools, schools, child care, care for the elderly, social support and services, primary health care, culture, agriculture, and the development of local areas, which includes the development of industry and employment. 21 A particular focus is on the local planning system as an important means of ensuring that the overall aims of the policy are being implemented. This means that the broad determinant perspective in the PHA is to be the foundation for local government planning and included in the local master plan (MP). 24 For municipalities, the MP is the basis for all local policies. All local governments must produce an overview of the health status and determinants that influence health and disease in their populations. This overview is required to identify local health challenges and their determinants: it should have a particular focus on social inequalities in health, and it should be the basis for local policymaking. The Norwegian National Public Health Institute (NPHI) has subsequently produced so-called health profiles for all the municipalities. These are available both on the NPHI website and the municipalities’ websites. They include indicators that provide an opportunity for monitoring and addressing the social determinants of health. Municipalities are mandated to use these indicators both in the MP and in the further development of their policies and measures. However, the act also allows the municipalities to adjust the policies to their own context. The relative freedom of the independent municipalities may therefore result in differences in how the policy is being implemented at the local level.
Conceptual Foundations and the Structure of the GEF
The GEF4,17,25,26 is a European action-oriented policy tool aimed at technical policy experts in (modern) public health working at the European member state level (Figure 1). The framework aims to facilitate evaluation of policy actions for their current or future use in terms of their “gradient friendliness.” In particular, this means each policy’s potential to level-up the gradient in HI by addressing the social determinants of health. The GEF conceptual model sets the formulation, implementation, monitoring, and evaluation of policies and their related actions firmly within the well-established policy cycle. Although some have challenged the policy cycle for being unresponsive, simplistic, and unrealistic, it is nevertheless also generally accepted as being a useful heuristic and iterative device for understanding the lifecycle of a policy, especially when evaluating complex policy actions. 27
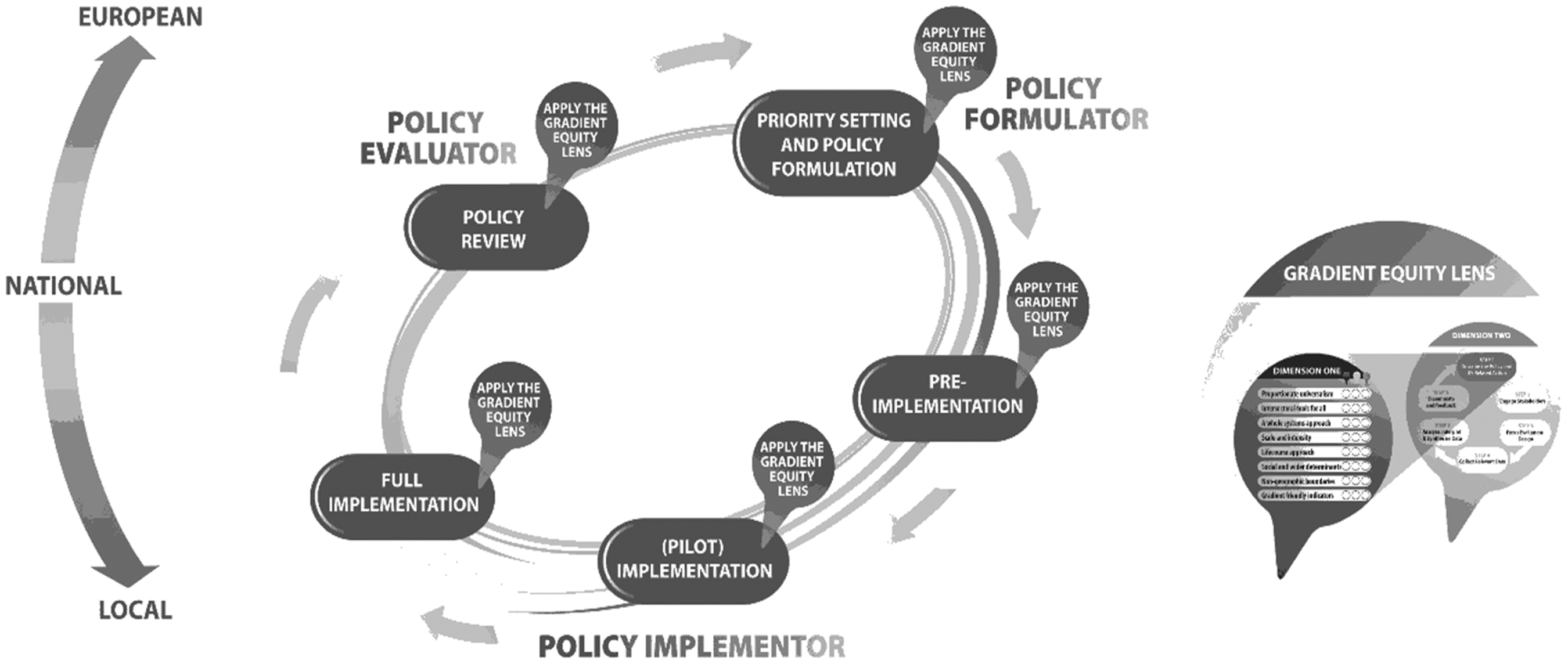
Gradient Evaluation Framework (reproduced from Davies and Sherriff, 17 with permission from the University of Brighton).
While the specific core components of the policy cycle vary, in GEF it comprises 5 core elements: priority setting and policy formulation; pre-implementation; (pilot) implementation; full implementation; and policy review. In GEF, the stages of the cycle are interdependent; they do not need to operate in a linear or incremental way, and evaluation can apply at each stage, as appropriate to the policy action context and stage of development under consideration.
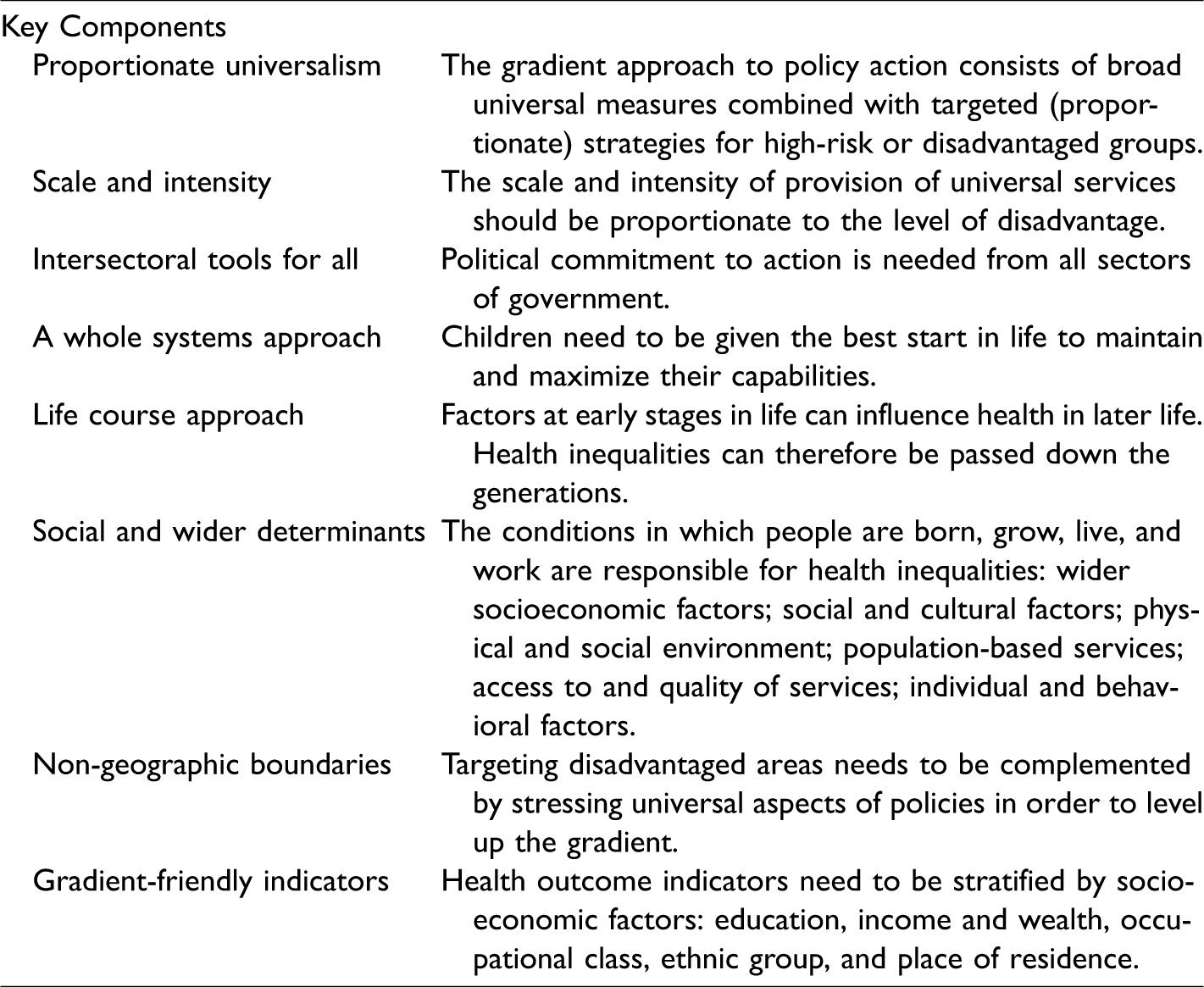
A core part of the framework is the Gradient Equity Lens (GEL), which can be applied iteratively and flexibly to facilitate appropriate evaluation of policy actions at each stage of the preferred policy cycle. This GEL comprises 2 key interrelated dimensions that together provide a gradient perspective on evaluating policies and their related actions. The GEL includes 8 key areas which form a checklist of key components deemed important to underpin the design and evaluation of effective policy actions (proposed or in place) in terms of their potential to be gradient-friendly, i.e., to level-up the gradient in health inequalities by addressing the social determinants of health that affect children, young people, and their families (Table 1).
The GEL can be applied to all the phases of the policy cycle, and in the present article, the GEL is adapted as a conceptual framework to study the implementation of the Norwegian PHA.
The Gradient Equity Lens (Davies and Sherriff 25 ).
Methods and Data
This article is based on data generated from 2 studies comprising 3 surveys as well as qualitative interviews with policymakers. A baseline survey was conducted in 2011 a few months before the PHA was implemented. In 2011, there were 430 municipalities and 15 partly self-governing urban districts of Oslo. An online questionnaire was sent to the chief executive officers (CEOs) of all municipalities and urban districts, who then either answered the survey themselves or delegated it to an appropriate civil servant. A total of 361 municipalities and urban districts filled in the questionnaire, giving a response rate of 87%. The smallest and most geographically remote municipalities were the ones that in most cases did not respond to the survey request. 28 The second survey was carried out in spring 2014. As with the first, the questionnaire was sent to the CEOs of the municipalities and urban districts of Oslo; 269 municipalities responded to the whole questionnaire, while an additional 40 municipalities responded to parts of it. The response rate was thus between 61% and 77%. Once again, the smallest and most remote municipalities did not respond. The third survey was carried out in 2017. It had a slightly different purpose but included several of the same questions as the 2 former surveys.
All surveys included questions on if and how public health had been included in the municipal planning system, which areas of public health had been prioritized in the municipality, which specific groups had policies been developed for, whether or not intersectoral working groups for health promotion had been established, whether a public health coordinator (PHC) had been employed, and where in the municipal organization the PHC was employed. The 2014 survey was essentially a further elaborated version of the initial 2011 baseline survey, covering specific questions regarding the implementation of the PHA, especially with regard to planning procedures. 29 Subsequently, some questions were asked only in the 2014 questionnaire. The 2017 survey had a broader perspective, but some of the questions from the 2014 survey were included. 30
In addition, individual interviews were conducted with policymakers from 6 municipalities. The municipalities were sampled strategically, and the main inclusion criteria were that municipalities had already started the process of implementing the HiAP principles and were actively addressing HI. Consequently, based on the 2011 survey, municipalities that were ostensibly in the process of implementing the PHA were selected. Additional criteria included size of municipality (some large, medium, and small) and inclusion of both urban and rural municipalities. In each municipality, between 6 and 8 informants were interviewed. The municipalities selected had different organizational models, and therefore the relevant informants varied to some extent. In general, political and administrative leaders and leaders of different sectors or units were interviewed along with public health coordinators. The aim of this article is not to compare the municipalities; instead, the survey data is intended to provide a broad picture of the general situation regarding implementation of the PHA, while the interview data and quotes aim to present a more in-depth and nuanced picture. Both studies received ethical approval from the Norwegian Data Protection Official for Research.
Results
Proportionate Universalism/Scale and Intensity
The concept of proportionate universalism was initially formulated by Marmot as a strategy that might reduce the steepness of the social gradient in health. 6 Proportionate universalism proposes that any actions to address the social gradient must be universal, but with a scale and an intensity that is proportionate to the level of disadvantage. Proportionate universalism is also a principle represented in the PHA.
In the 2014 questionnaire, we asked if the municipalities had developed an overview of the health situation, including HI. Thirty-nine percent of municipalities reported that they had made such an overview, while 48% reported that they were only just starting the process. In 2017 there had been a major increase, as 85% reported that they had made this overview.
The 2017 survey also indicates that municipalities have started to consider equal allocation of resources in their planning documents and decision making.
From the individual interviews, officials working as public health coordinators particularly were found to have a high awareness of the principles of the PHA, and some of them have captured the gradient thinking, illustrated by the following quote: I belong to those who think Michael Marmot has been reasoning sensibly about this, and I believe the social determinants and the basic conditions for development of society are the most important. (K2)
In 2017, the question was posed somewhat differently, asking about concrete areas covering social living conditions, such as housing, education, and employment and income. These areas still hold a relatively low priority: for example, 36% of the municipalities report that they were giving priority to issues like employment and income. In contrast, 58% report that they prioritize individual measures concerning mental health in children and adolescents. 31 Part of the explanation for this priority is the national government’s priority of mental health among adolescents and children and the support to municipalities on this issue. 31
When asked in the surveys whether the municipalities prioritized universal measures, 16% answered yes in 2011, while in 2014 the number had increased to 43% (2011, n = 303; 2014, n = 250). This question was not included in the 2017 survey.
The individual interviews also found support for these principles: I believe it is valuable to reach everyone, but I believe that some of our offers should be directed at disadvantaged groups. (H1) To me this is first and foremost about vulnerable families who have a history—unemployment and dependency on social welfare often continue over generations. (K5)
A Whole System Approach/Intersectoral Tools for All
The Norwegian PHA demands a whole system approach to addressing HI. The responsibility for public health lies with the municipality leadership, which includes the mayor, the CEO, and their administration. The whole system approach is further reflected in the PHA demand that public health must be included in the local municipal MP. Based on the MP, action plans should be developed, committing the local governments to address HI challenges. In the 2014 and 2017 surveys, municipalities were asked if they had established intersectoral working groups and which sectors were members of such groups. In 2014, 62% of the municipalities reported having established such groups. In 2017, the number had increased to 72%.
Regarding sectors participating most often, approximately 50% of the participants come from the local child health centers; this had increased to 71% in 2017. The cultural sector included sports (67% and 56%), schools (75% and 72%), and kindergartens (50% and 60%). An interesting point is that the kindergartens seem to participate more in intersectoral working groups in 2017 than they did in 2014 and 2011.
To ensure implementation, it is important that public health is anchored at the executive level in the municipalities, where budgets are made and policies developed. Furthermore, in the Norwegian system, the municipal planning process is important for the development of policies and measures, and thus the planning departments play an important role in the policymaking process. In 2014, 68% of the municipalities’ CEO staff participated in intersectoral working groups, representing an increase from 22% in 2011. In 2017 the number had decreased to 56%. However, participation from the planning departments had increased. In 2011, it was 16%; in 2014, participation had increased to 65%; and in 2017, 56% of the municipalities reported that the planning department was participating in intersectoral working groups. In the interviews, informants described this positive development, which is illustrated in the following quote: It has developed from being a responsibility for the health sector to a field that is a responsibility for the central leadership and then developed to concrete measures. (M1) Generally, the public health field is still too much influenced by the health and social sectors. We have been working overtime to anchor it more broadly and we have moved a bit on the way. (K2)
Life Course Approach
In the 2011 survey, municipalities were asked which institutions they believed could reduce social inequalities. Municipal health centers are a universal service offered to all families. They are responsible for vaccination programs and for following up on children’s and families’ health and well-being. Forty-three percent believed that these health centers reduced social inequalities, while only 27% believed that schools could play this role. In 2014 and 2017, municipalities were asked a general question in terms of whether they were capable of reducing social inequalities: in 2014, 83% said yes; and in 2017, this number had increased to 95%. However, it seems that the efforts are mainly related to the services they are responsible for, rather than looking across administrative levels and sectors. Particularly, child health centers and kindergartens seem to be arenas for efforts to reduce inequalities among children.
In the interviews, many of the respondents expressed awareness of the life course approach and emphasized the need for services for families and children: We take care of them at birth. We try to influence them from the first day. I think the municipality has a responsibility to follow through the transitions in the education system, from day care to secondary school. (M1) We see that it often is inherited. If you come from a family with low socioeconomic status, you follow in the footsteps of your parents regarding activities and education, and they follow that path. (M7)
Social and Wider Determinants
The Norwegian PHA mainly addresses the social determinants of health and pays relatively less attention to individual lifestyle factors. Despite this, many municipalities surprisingly continue to focus predominantly on individual lifestyles, such as physical activity and diet. Indeed, the 2014 survey showed that 71% of municipalities still prioritized lifestyle issues. This is an increase from 2011, when the number was 34%. In the 2017 survey, the respondents were asked what they saw as the main challenge in public health. Mental health problems were ranked highest (62%).
Given the focus of the PHA, it would be expected that addressing the social determinants would be much higher on the agendas of municipalities. In contrast, the municipalities taking part in the qualitative interviews seemed to reflect more about the social determinants. Education is one issue that was raised by several informants: I believe the most important in reducing social inequalities is simply education. If people get a platform and get an education, that’s what it takes to reduce inequity. (F7) But it is also very political, and I think that has not been problematized enough. When we tried to include the wider social determinants in our local plan, everybody agreed, but in practice we don’t have a political regime that necessarily thinks that this is a good policy—so it is not being followed up in practice. (K4)
Non-Geographic Boundaries
There are regional variations in how the social gradient relates to mortality. 6 A policy addressing only socially deprived areas will have limited potential to reduce the social gradient. Our surveys show that larger Norwegian municipalities in 2011 prioritized living conditions while smaller ones tended to prioritize lifestyle issues. As shown above, the 2014 and 2017 surveys indicate that an increasing number of municipalities prioritize living conditions in their public health policies. Still, it appears to be a theme mostly for the larger municipalities.
Based on our interviews, there also seems to be a difference between smaller and larger municipalities regarding the priority of the HI. In one city, informants working within public health and the social services regarded the situation as worrying: If you take a cynical approach; if they live in a certain part of town, have not completed secondary education, and smoke, then they don’t have many prospects. (K4) In the long term, you will have a new generation of children and young people who will attend good schools in stimulating surroundings that will encourage them to take an education. This could lead to more social equality, which will also help them to make healthy choices. (K4)
Gradient-Friendly Indicators
In general, policy objectives, including targets and outcomes, need to be able to capture the fact that social inequity in health forms a gradient across society. However, social determinants of health and causal factors require additional analysis, as the most important determinants of health may differ between socioeconomic groups. 17
It is of course very important that indicators have been developed and made available for each municipality, providing the opportunity to address the social gradient. Without such indicators, many of the aspects of health inequalities remain invisible. The share of municipalities that have developed an overview of the health situation has increased by more than 50% from 2014 to 2017. In 2017, 70% of the municipalities reported that the overview has formed the basis for local priorities in their planning, and 68% also reported that the priorities of services is based on findings from the overview. This indicates that if municipalities have made an overview, they will use it as presupposed in policy documents.
Discussion
The Norwegian Public Health Policy is unique in Europe in overtly addressing the social determinants of health. An overall aim is to level the social gradient in health by adopting a HiAP approach, and the local level is key to implementing these policies.
Even though the issues of HI and HiAP have been on the political agenda for a number of years in Norway, it was only when the PHA was adopted in 2012 that the municipalities were mandated to include these themes in their policies, plans, and practices. In general, there was a development from 2011 through 2017, where the act was being increasingly integrated in the municipalities. In the following, we will follow the GEF in our discussion of the findings.
Informants support the idea that policies should be universal but that targeted measures should be available for disadvantaged families. This support for both universal and targeted measures may be interpreted as a proportionate universalistic strategy. 6 Implicitly it is, since proportionate universalism reflects the Nordic welfare state model. Many measures are universal, and this is the basis for distribution of health and welfare services. However, it cannot be concluded that the municipalities are aware of the principle of proportionate universalism to reduce HI and level the social gradient in the context of the PHA in the Norwegian municipalities. The social differences in Norway are increasing, 32 and universal welfare measures are crucial to reduce these. As policymakers are establishing the policies and making priorities, it seems vital that they share this understanding. When HI are explicitly discussed, the focus is on marginalized groups.
Regarding A whole systems approach/intersectoral tools for all, there seems to be an increased integration across municipal sectors. An increasing number of municipalities have established intersectoral working groups, and the municipal leadership also seems to pay an increasingly important role. One point to be made is that the working groups are anchored in the administrative structure representing sectors responsible for the implementation of the act. This may promote implementation since it demands a commitment from all sectors.
The life course approach is well integrated in Norwegian municipalities since they are responsible for services for families and children. There seems to be an increased awareness that day care, education, and leisure time activities play an important part in reducing social inequalities.
In Norway, like in many other countries, social inequalities are widest in the largest cities, and positive and negative health factors are clustered in different parts of the cities. 15 The situation in the larger cities illustrates dilemmas in the development of policies to level the social gradient. Several programs have been developed to improve living conditions in poor areas. Seldom, however, are housing policies discussed in the context of the social and wider determinants.
While some policies and measures are being developed, mainly in the sectors working with disadvantaged groups and areas, policy measures that address the root causes, i.e., the social determinants, are not being developed. Even though many of these root causes would demand national policy measures, the municipalities have the authority to develop housing policies and recreational areas via the municipal land use plan. In many municipalities, the planning of housing has been left to private developers, and as real estate prices rise, building of affordable housing is very limited.
Norwegian municipalities have been provided with gradient-friendly indicators in the health profiles provided. These indicators provide an opportunity for monitoring and addressing the social determinants of health. Municipalities are mandated to use these indicators, both in the MP and the further development of policies and measures. Most municipalities have now developed the required overviews of the health situation in their municipality.
Conclusions
An increased awareness seems to be developing that municipal services such as day care, education, and leisure time activities play an important part in reducing social inequalities.
In the decentralized Norwegian governance system, municipalities have a relatively high degree of freedom to make priorities, both politically and economically. The PHA includes mostly “soft” governing tools, in terms of audits and different types of support, i.e., courses and seminars for policymakers. Economic support is available, not via budgets but in terms of projects and other time-limited funding. This may be problematic in the long-term implementation and may give a signal that the act is not so important. 33 On the other hand, there is room for local adjustments of the policy, which also call for bottom-up approaches, and an integration in the municipality based on local interests, which is important for implementing a whole-of-government approach.34,35
Another important discussion is the limits of local policymaking. Overall priorities, for example, in fiscal or education policies, are made at the national level. It adds to the point that reducing HI is a wicked issue with contesting definitions and priorities that need whole-of-government action. Reducing HI is both complex and lacking in political consensus. By leaving the main responsibility to the municipalities, the actual solutions are left to the local government to handle, while many of the solutions are to be found at other levels and even other sectors of society.
Footnotes
Compliance With Ethical Standards
Ethics approval and consent to participate. Both studies received ethical approval from the Norwegian Data Protection Official for Research. For the quantitative study, consent was implicitly assumed by return of completed questionnaires. For the interview study, all participants provided informed consent.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship,and/or publication of this article: The research presented in this paper was funded by the Norwegian Research Council as part of the projects: “Addressing the social determinants of health: Multilevel governance of policies aimed at families with children” (Project no. 213841/H10) and “Evaluation of the Coordination Reform: Impact of the reform on health promotion and disease prevention in municipalities” (Project no. 229628).