
Abstract
We conducted a systematic review and meta-analysis to assess differences in risk-adjusted mortality rates between for-profit (FP) and not-for-profit (NFP) hemodialysis facilities. We searched 10 databases for studies published between January 2001 to December 2019 that compared mortality at private hemodialysis facilities. We included observational studies directly comparing adjusted mortality rates between FP and NFP private hemodialysis providers in any language or country. We excluded evaluations of dialysis facilities that changed their profit status, studies with overlapping data, and studies that failed to adjust for patient age and some measure of clinical severity. Pairs of reviewers independently screened all titles and abstracts and the full text of potentially eligible studies, abstracted data, and assessed risk of bias, resolving disagreement by discussion. We included nine observational studies of hemodialysis facilities representing 1,163,144 patient-years. In pooled random-effects meta-analysis, the odds ratio of mortality in FP relative to NFP facilities was 1.07 (95% CI 1.04–1.11). Patients at FP hemodialysis facilities have 7 percent greater odds of death annually than patients with similar risk profiles at NFP facilities. Approximately 3,800 excess deaths might be averted annually if U.S. FP hemodialysis operators matched NFP mortality rates.
Private for-profit (FP) health care institutions provide a significant proportion of patient care in the United States. Dialysis care for people with end-stage renal disease (ESRD) is delivered largely by FP facilities: 91 percent of all free-standing facilities are for-profit, dominated by two FP firms. 1
Research dating back to the 1980s has addressed the outcomes of patients treated at private FP facilities versus not-for-profits (NFPs).2,3 FP facilities may have incentives to maximize efficiency by developing innovative strategies for patient care, thereby improving patients’ outcomes. On the other hand, FP facilities face tax burdens and obligations to owners and shareholders that may provide incentives to limit resources devoted to patient care and jeopardize optimal care and patient outcomes.
A 2002 meta-analysis examining FP and NFP dialysis center outcomes found higher risk-adjusted mortality rates at FP dialysis centers. 4 In the more than 15 years since that meta-analysis was conducted, dialysis centers have undergone considerable corporate consolidation. 5 We therefore reviewed and analyzed studies addressing the impact of FP versus NFP ownership on risk-adjusted mortality in U.S. dialysis centers.
Methods
Search Strategy
Our search criteria was similar to that of the 2002 systematic review for dialysis centers,4,6 which was considered to be comprehensive of the literature through 2001. A health sciences information specialist (R.C.) experienced in systematic review led development of the search strategy as well as a similar search comparing private FP vs. NFP hospitals (published elsewhere). Peer Review of Electronic Search Strategies (PRESS) evaluated the search strategy using a standardized checklist developed by the Canadian Agency for Drugs and Technologies in Health. 7 Feedback improved the free-text component of the search, enhancing sensitivity by ending words with a wildcard to capture all permutations, and specificity by requiring the pairing of key words. This review was pre-registered on PROSPERO (CRD42018085430). Our search included publications from January 2001–December 2019 in the following 10 databases: MEDLINE, HealthStar, EMBASE, PubMed, Cochrane Library, Web of Science, Proquest Dissertations and theses, ProQuest Business Premium Collection, Econlit, and CINAHL. (Online Appendix 1 presents the detailed search strategy.) We also conducted a manual review of citations from existing systematic reviews and contacted topic experts for further references.
Eligibility Criteria
We included published and unpublished observational studies that directly compared mortality rates between private FP and private NFP dialysis facilities without language or geographic restrictions.
We excluded evaluations of dialysis facilities that converted from one profit status to another (e.g., from NFP to FP); studies in which the patient population was a subset of a larger population from an already included study; studies with overlapping data (i.e., studies with data from the same source with overlapping data collection periods [in such instances, we included studies with the larger sample size]); and studies that did not adjust for patient age and some measure of clinical severity.
Screening Citations and Extracting Data
Pairs of reviewers, who participated in a calibration exercise to ensure optimal understanding, conducted eligibility screening independently and in duplicate. Articles deemed potentially eligible at title and abstract screening underwent full-text screening. For those that proved eligible on full-text evaluation, reviewers extracted in duplicate the following data: sampling method, case mix, type of institution, dates when data collection was initiated and completed, duration of follow-up, number of facilities and patients evaluated, mortality rate estimate with confidence intervals and p-values, whether analysis accounted for facility clustering and/or instrumental variables, and prognostic factors for which the analyses adjusted. Disagreements between the two reviewers that persisted after discussion were resolved by a third reviewer.
When more than one outcome option was reported, we applied the following hierarchy: longer duration of follow-up over shorter and optimally adjusted models over under- or over-adjustment (we considered studies over-adjusted if authors included features reflecting profit status in their models, e.g., nurse staffing ratios). All extractions were double-checked by one of the coauthors (S.D. or R.M.). We contacted 11 authors of papers with possible relevant unpublished data; 10 responded, and one was able to provide data that was ultimately included in this study.
Risk of Bias and Quality of Evidence
Two reviewers independently assessed risk of bias across eight domains: selection bias, exposure to intervention, outcome measurements both at the start and end of trial, assessment of prognostic features, appropriate adjustment of prognostic imbalances, adequacy of follow-up, and similarity of intervention between groups. 8 Disagreement that persisted after discussion was resolved by a third reviewer. Studies were defined as low risk of bias if six of the eight assessed domains of bias were definitely or probably addressed, at moderate risk of bias if four or five domains were addressed, and at high risk if fewer than four domains of bias were addressed. We used the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology to assess the quality of evidence 9 and funnel plots to visually evaluate publication bias.
Analysis
The majority of studies reported relevant FP vs. NFP comparisons using odds ratios. We converted all other measures of association into odds ratios. Online Appendix 2 describes how odds ratios were calculated for studies with different mortality metrics.
We planned pre-specified subgroup analyses to determine whether effect magnitude or direction varied based on certain characteristics, requiring at least three studies in each subgroup to proceed with subgroup analysis. Dialysis subgroups included: (a) hospital-based vs. free-standing facilities, (b) whether studies accounted for FP market share, (c) whether studies adjusted for covariates that were likely causally related to FP vs. NFP status, (d) the method of risk calculation, and (e) whether the study included pre-1984 data.
Role of the Funding Source
This study was supported by the Department of Medicine and the Vice Provost’s Office at McMaster University. The funders had no role in the study’s design, conduct, or reporting.
Results
The systematic search for dialysis studies identified 3,021 citations. After removal of duplicate studies, 2,137 records were eligible for screening by titles and abstracts (see Figure 1 for PRISMA diagram).
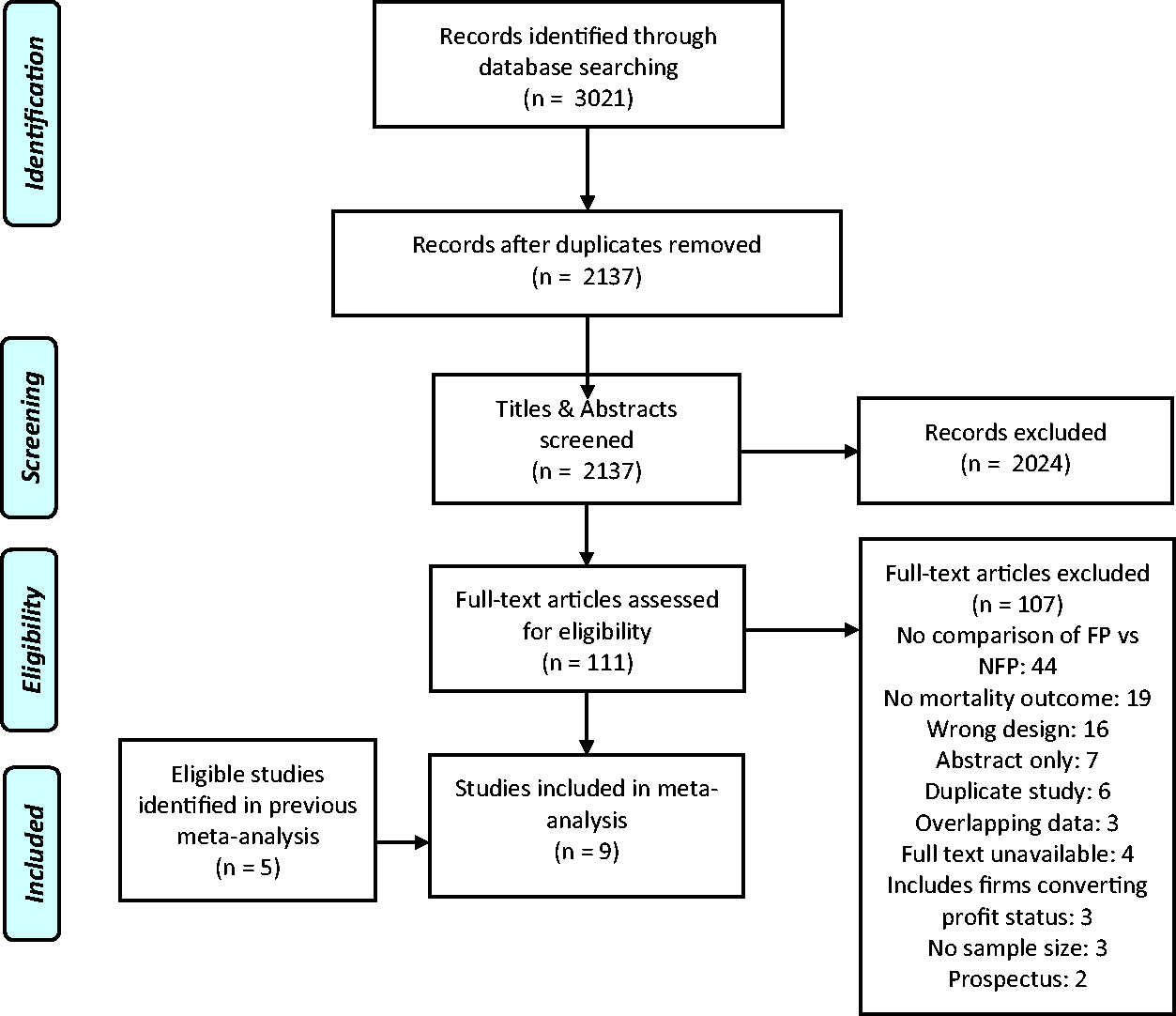
PRISMA flow diagram.
Title and abstract screening revealed 111 potentially eligible dialysis studies. Full text screening of these records revealed seven new relevant studies published since the only other systemic review, 4 four of which were included. Three new studies were excluded because of overlapping data, specifically analysis of the same database with overlapping years.10–12 (We received unpublished data from the author of one of the four included studies.) We also included data from five studies from the earlier systematic review, resulting in a total of nine hemodialysis studies.
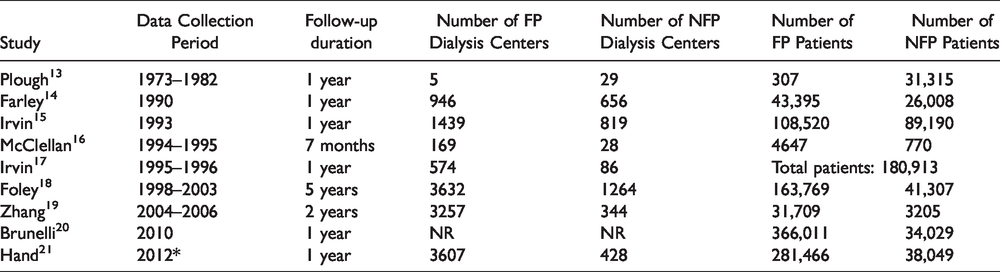
Table 1 presents study characteristics of publications included in the review. The nine studies included 1,163,144 patient-years. One study used mortality data for seven months, six studies had one year of data, and two studies included data for more than one year. All studies were conducted in the United States. Seven used data from the U.S. Renal Data System, while two used data from a subset of states.
Characteristics of Studies Included in the Systematic Review.
GRADE Assessment.

Too few studies (fewer than 10) to address publication bias.
In random effects meta-analysis, FP dialysis centers had higher risk-adjusted odds ratios of 1.07 (95% CI 1.04–1.11) relative to NFP centers (Figure 2). Subgroup analyses were not conducted, as none of the pre-specified subgroups included at least three studies.
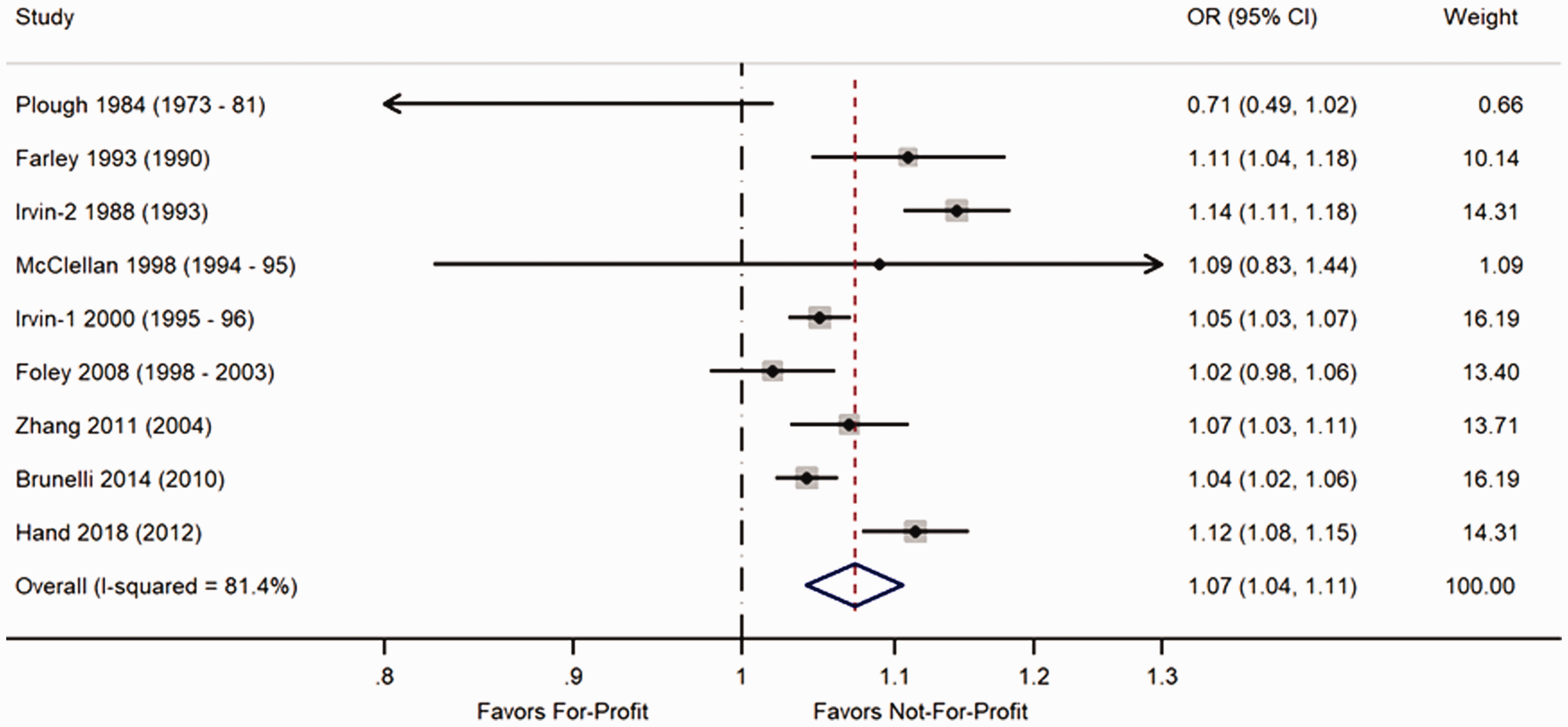
Mortality in for-profit vs. not-for-profit hemodialysis facilities.
Risk of Bias and Quality of Evidence
We judged eight of nine eligible studies to be at low risk of bias and one at moderate risk (Online Appendix 3). The domains of bias most often deemed unaddressed were related to assessment and management of prognostic variables (three studies). The study by Plough and colleagues 13 that was deemed at moderate risk of bias compared free-standing FP facilities to hospital-based NFP facilities that might serve sicker patients (and differ in co-interventions), hence biasing comparisons in favor of FP facilities. That study also failed to assess or address other important confounders, such as smoking status.
The quality of evidence is low because all included studies are observational in nature. The point estimate of all but one study favored NFP facilities. The one contrasting study by Plough et al. 13 is at high risk of bias and has the widest confidence intervals. Although the I2 index is 80 percent, all studies that individually show a benefit favor NFP: Inconsistency in the meta-analysis estimate arises from variation in the magnitude of NFP’s mortality advantage and very narrow confidence intervals. Not enough studies were eligible to evaluate publication bias.
Discussion
Pooled data from nine observational studies of hemodialysis centers suggest that mortality rates at FP facilities are approximately 7 percent higher than NFP facilities with comparable patients. 4 This figure may underestimate the FP disadvantage; the single study in our analysis that favored FP facilities was uniquely biased in favor of FPs by comparing free-standing FP dialysis facilities with hospital-based NFP facilities.
More than 100,000 patients in the United States with ESRD die each year. Applying our finding of the relative odds of mortality to the most recent available U.S. data, 1 we estimate that approximately 3,800 excess deaths could have been averted if U.S. FP hemodialysis centers had achieved the lower mortality rates of their NFP counterparts.
Our findings are consistent with those using complementary data sources and populations, outcomes, and analytic techniques. The only previous meta-analysis in 2002 by Devereaux and colleagues similarly found higher risk-adjusted mortality at FP dialysis facilities. More recent studies also find worse mortality rates under FP management: Regions where the two large FP providers are most dominant have higher mortality rates, 22 and improvement in outcomes was slower after facilities were acquired by one of the “Big Two” FP firms. 23 Several mechanisms that may explain why FP ownership worsens outcomes have been identified in recent years: at facilties acquired by the major FP firms, the mean erythropoietin dose increased by 129 percent (administering higher doses was more profitable, but associated with higher stroke and death rates), renal care quality metrics were worse, and the risk of hospitalization was 15 percent higher.24–26
Profit-seeking may also compromise patient outcomes by reducing referrals for transplantation rates; FP facilities have a 0.9 percent and 1.7 percent lower absolute incidence of living- and deceased-donor kidney transplantation compared to their nonprofit counterparts, respectively. 27
Although the public Medicare program covers about 80 percent of all patients with ESRD, FP dialysis operators now dominate the U.S. dialysis market,1,28 with the two largest firms, DaVita and Fresenius, providing services for 85 percent of all U.S. ESRD patients. 1 Our results raise concerns about the adequacy of government oversight of FP dialysis providers and the incentives that have led to FP providers’ market domination. As FP providers continue to gain market share, future research evaluating outcomes at FP facilities will be hampered by concerns about the reliability and generalizability of an ever-smaller NFP comparison group.
Strengths of this review include a prior registered protocol; explicit detailed eligibility criteria; a comprehensive, peer-reviewed search strategy; assessment of risk of bias of individual studies; quality assessment using the GRADE framework; avoiding use of overlapping data from prior studies4,29; and inclusion of unpublished data. Further, most eligible studies used data from the U.S. Renal Data System, ensuring analysis with a consistent set of covariates.
Our systematic review and meta-analysis have several limitations. Although all studies adjusted for multiple prognostic variables, observational studies cannot deal with residual confounding and thus the starting quality of evidence is low. Given that all included studies used data from the United States, generalization to non-American contexts is questionable without further evidence.
We find that mortality rates at FP hemodialysis facilities are substantially worse than at NFP facilities. As the U.S. health care system becomes increasingly dominated by private FP facilities (and in some cases by NFP facilities that operate much like FPs), the public and policy makers should assess the need for regulatory action and revising incentives in the dialysis industry.
Supplemental Material
sj-pdf-1-joh-10.1177_0020731420980682 - Supplemental material for Mortality at For-Profit Versus Not-For-Profit Hemodialysis Centers: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-joh-10.1177_0020731420980682 for Mortality at For-Profit Versus Not-For-Profit Hemodialysis Centers: A Systematic Review and Meta-analysis by Samuel Dickman, Reza Mirza, Maryam Kandi, Michael A. Incze, Lorin Dodbiba, Raad Yameen, Arnav Agarwal, Ying Zhang, Rakhshan Kamran, Rachel Couban, Gordon Guyatt and Steven Hanna in International Journal of Health Services
Footnotes
Acknowledgments
The authors thank Zahra Premji from the University of Calgary for peer review of the electronic search strategy. We also thank McMaster University’s Department of Medicine and Vice Provost’s Office for research funding. Patients or the public were not involved in the design, conduct, reporting, or dissemination plans of our research.
Author Contributions
Guyatt conceptualized the project. Dickman and Mirza supervised and wrote the first draft of the manuscript. Couban acquired the data. Kandi contributed statistical analyses, which were overseen by Hanna. Incze, Dodbiba, Yameen, Agarwal, Zhang, and Kamran analyzed data and contributed to editing and revising the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
Ethics approval was sought from the McMaster HiREB and deemed unnecessary given the low risk of harm in systematic reviews and meta-analyses.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Medicine and Vice Provost’s Office, McMaster University.
Registration
PROSPERO CRD42018085430.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.