
Abstract
Globally, the coronavirus disease 2019 (COVID-19) pandemic has resulted in several psychosocial manifestations across all socioeconomic strata. This study attempted to explore the details of a psychosocial support system implemented in Kerala, India, to address psychosocial issues during this pandemic. It employed a descriptive approach using qualitative and quantitative methods. The results can be summarized into 4 overarching themes: (1) process of implementation, (2) issues addressed, (3) experiences, and (4) success stories. This intervention targeted the whole population, with a specific focus on quarantined/isolated individuals and selected vulnerable groups. COVID pandemic has sowed several negative emotions, such as anxiety; and stigma and fearful thoughts, including suicidal ideations; trepidation regarding family members; and misinfodemics in general. Social and religious corollaries of the pandemic have intensified the psychological agony. The study provides an overview of the psychosocial intervention adopted by the state during the pandemic, which has helped both the beneficiaries and the providers. It has also helped to promote positive thinking and change the attitude toward the disease among the beneficiaries. It is highly commendable that timely intervention could obviate quite a few psychiatric emergencies, including suicides and aggressive behaviors. Considering its efficiency, flexibility, and sustainability, this model can be replicated in any setting.
The pandemic coronavirus disease 2019 (COVID-19) is a major public health concern distressing large spheres of lives globally. In India, the first case of COVID-19 was reported in Kerala in January 2020. As of October 31, 2020, the state had reported 433 105 confirmed cases with 78.6% recoveries.1–3 In Kerala, varieties of interventions were implemented through intersectoral coordination to flatten the pandemic curve. Measures such as lockdown, isolation of positive cases, quarantine of travelers and contacts, enforcement of the use of masks and social distancing, promotion of hand washing, and use of sanitizers were among them. Mental health experts anticipated that these measures, along with fear of disease, could adversely affect the psychological health of the society by developing stress, confusion, frustration, anxiety, substance abuse, suicidal ideation, and ambivalence.4,5 Psychosocial support for isolated, quarantined, and suspected cases; high-risk groups; caregivers; health care staff; family members; and the general population were found to be crucial. 6 Hence, a psychosocial support system was developed in the state. This article attempted to explain the implementation of a psychosocial support system in Kerala during the COVID-19 pandemic to provide constant, responsive, and sustainable support to the general public and explored the perceptions of stakeholders regarding the intervention.
Materials and Methods
We adopted a descriptive approach using qualitative and quantitative methods. Ethics clearance was obtained from the Institutional Ethics Committee at GH, Trivandrum, in April 2020. Ten in-depth interviews were conducted with state, district nodal officers, and beneficiaries to ascertain the details of intervention and how this intervention abetted both care providers and care receivers during this pandemic. The study participants were selected purposively from the districts where more cases were reported. Thus, the study was conducted in the Thiruvananthapuram, Ernakulam, and Palakkad districts.
The following stakeholders were interviewed:
One State Nodal Officer (SNO), Mental Health. To examine the details of intervention and to explore perceptions of the program Three District Nodal Officers (DNO). To understand the field-level implementation of the program and their experiences Six beneficiaries. To explore their perceptions of the program and their experiences
In-depth interview guidelines were developed and interviews were scheduled based on participants’ convenient dates and times. The participant's consent was taken before the interview. The main information collected from nodal officers included details of intervention in terms of planning and implementation, challenges faced, hesitancy from beneficiaries, success stories, and how the intervention affected their personal/professional lives. The main information collected from beneficiaries included their insights regarding this pandemic, their experiences/feelings with this intervention, and the coping strategies adopted through this intervention.
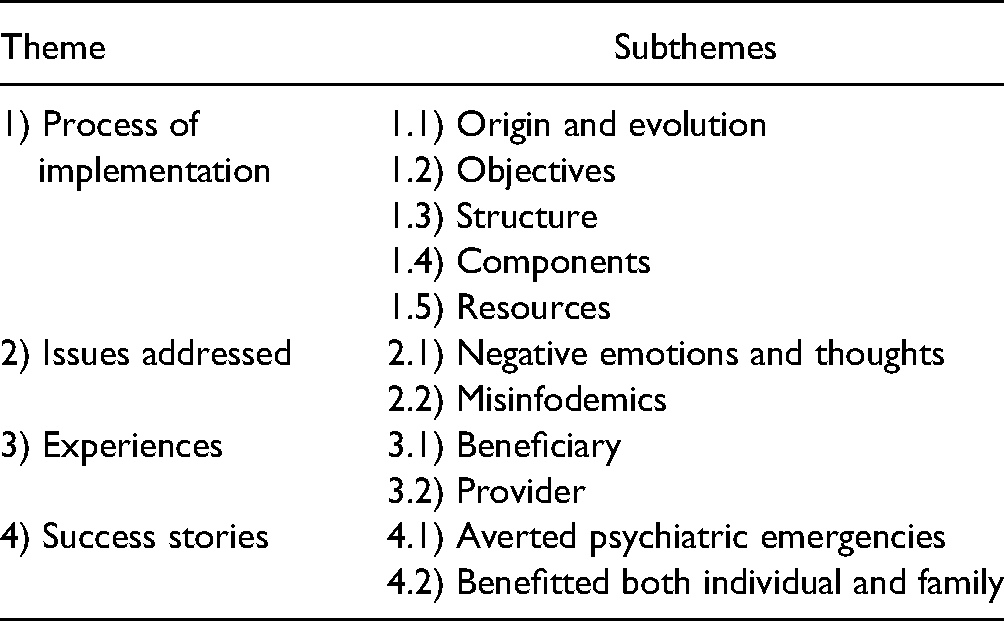
The information obtained through in-depth interviews was recorded, transcribed, and analyzed manually. Thematic analysis was done after coding. A set of main categories was established by grouping together all subcategories with similar meanings. These were reviewed repeatedly to identify emerging themes and subthemes (Table 1).
Themes and Subthemes Evolved.
We also collected the details of calls from all district mental health centers. 7 The calls made by the team for each category were based on checklists prepared by mental health experts. They included the probes to understand psychosocial issues such as stigma, anxiety, stress, need for counseling, and other social needs faced during quarantine and lockdown. The secondary data was analyzed using Microsoft Excel.
Results
Four overarching themes were generated after the analysis namely (1) process of implementation, (2) issues addressed, (3) experiences and (4) success stories.
Process of Implementation
As part of the Rapid Response Team for prevention and control of the COVID-19 pandemic, a psychosocial committee was constituted at the state level to provide psychosocial support through the District Mental Health Programme (DMHP). DMHP is a program that decentralized mental health services to primary care by integrating mental health care with the general health care delivery system. It was launched in 1996 under the National Mental Health Project, which primarily aims to provide mental health care at the community level. Kerala is the first state in the country to have a decentralized mental health program in all districts. 8
The program “You are not alone, we are with you” (Ottakkalla, Oppamund), designed to assess and improve the psychological well-being of isolated and quarantined persons, their family members, selected vulnerable groups, health personnel, and other frontline workers through customized interventions, was commenced on February 4, 2020. This Psycho Social Support Team (PSST) reached out to the public to provide services by actively contacting them by telephone instead of providing services through a helpline number, a method adopted during the Nipah outbreaks and natural disasters in 2018 and 2019.
Initially, the interventions were more for psychological needs, but later, when the lockdown began, social needs also increased. All quarantined/isolated persons were contacted over the phone, to give reassurance and to share district helpline numbers to call back in case any additional needs arose. Medical and social requirements were reported to the appropriate medical officers and local self-governments (Figure 1). Tailor-made interventions were developed for each individual based on the need. Routine follow-ups were done on the fifth and 10th days after the initial contact.
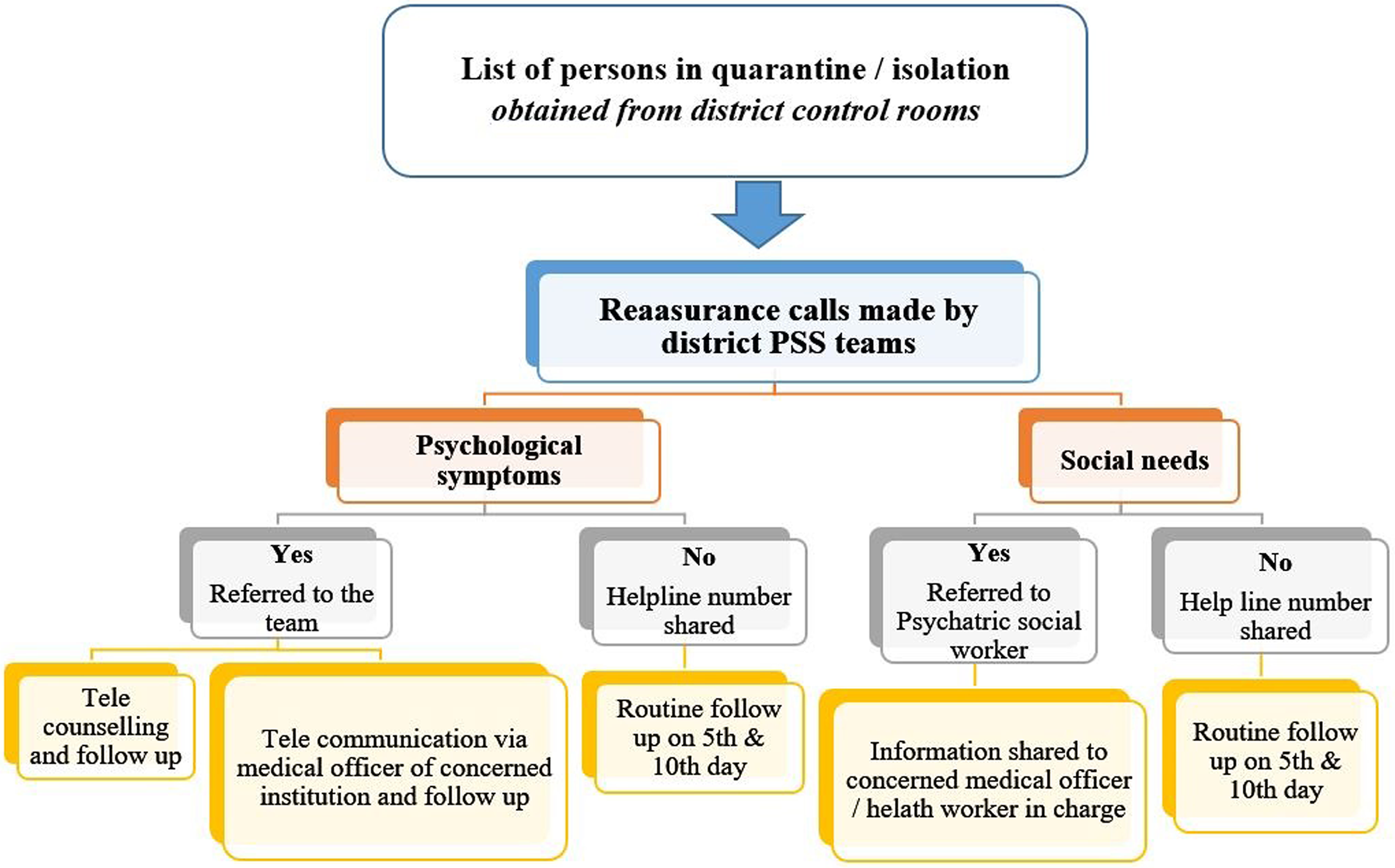
State psychosocial support system: algorithm.
The SNO who heads the team is responsible for implementation and monitoring of the program in the state. Each district has a nodal officer who coordinates activities at the district level. A team including psychiatrists, psychiatric social workers, clinical psychologists, social workers, and counselors work at the field level. The details of calls made are reported on a daily basis through DMHP to SNO. Because there was a system in place for reporting and monitoring, no extra effort was required. Apart from the regular staff in DMHP, counselors from Integrated Child Development Service (ICDS), Integrated Counselling and Testing Centre (ICTC), National Health Mission (NHM), and voluntary counselors became part of the intervention.
In the wake of lockdown, services of the psychosocial team were extended to 7 groups with special needs. Specific guidelines and protocols were prepared for each group:
Mentally ill patients in treatment. During lockdown, mentally ill patients who were already on treatment from medical colleges, mental health centers, General/District/Taluk hospitals, and DMHP faced difficulty in accessing care and medication. There were apprehensions regarding the continuity of care, which may adversely affect their well-being. The PSST contacted them to inquire about their condition, provide psychosocial support, and check the availability of medicines, which was then reported to the nearest Primary Health Centre. Medicines were made available to all patients on treatment from Medial Colleges, Mental Health Centres and General/District/Taluk hospitals through their nearest centers. Children with special needs. During lockdown, children with special needs who were otherwise attending special schools were forced to remain indoors, which made them restless and difficult to manage. The parents were stressed because, there were no definite answers for their questions about what to do, where to go, and whom to contact. PSST decided to reassure the children and parents by reaching out to them by phone. With the help of the Social Justice Department, teachers in special schools were given online training to provide feasible therapies over the phone. Speech therapists, special educators in District Early Intervention Centers, and Mobile Intervention Units were also involved. Guest laborers. Guest laborers who were held up in various parts of the state due to lockdown were identified by the Labor Department and Local Self Government (LSGD). They were anxious about the well-being of their family members elsewhere and insecure about their jobs and the availability of essential items to tide them over the lockdown period. Counselors fluent in North Indian languages were identified and entrusted to provide them psychological support. Their social issues were also assessed and communicated to the concerned. Older persons living alone. A list of older persons living alone was collected with the help of the Social Justice Department and LSGD. Fear regarding the pandemic, loneliness, nonavailability of essential items, uncertainties regarding the continuity and follow-up of their chronic diseases, and concerns about their loved ones elsewhere were distressing older persons. Their medical, social, and psychological needs were identified and reported to the concerned. Persons with alcohol dependence. Due to the nonavailability of beverages during lockdown, the possibility of alcohol withdrawal and delirium tremens in many regular drinkers was anticipated. To address this issue, community-based deaddiction was initiated. Guidelines with reporting formats were communicated to primary care doctors who were trained online. To support them, a panel of psychiatrists was constituted in all districts. Most of the cases were managed in primary care settings, and cases of severe alcohol withdrawal were referred to higher institutions. Schoolchildren. Children faced many stressors due to their inability to go to school, to go out, to play, and to spend time with friends and in online education. PSST called schoolchildren over the telephone and supported them to overcome the stress, anxiety, depression, behavioral issues, suicidal behavior, and substance abuse in this crisis period. Health personnel. Health care workers, who are in the forefront of the battle against COVID-19, were stressed due to workload; changes in the mode, setting, and paraphernalia of work; and fear and apprehension regarding the pandemic, including themselves or their family members acquiring the infection. Training on stress management was provided, and leaflets on better communication skills were distributed, especially to those who were working in isolation wards. Reassurance calls were made to those working in both state and district control rooms. Online meetings with celebrities were arranged as stressbusters.
Issues Addressed
Negative Emotions and Thoughts
Almost all quarantined persons and their family members had anxiety, fear, stigma, and suicidal ideations. Quarantined persons reported that they felt like crying due to overriding thoughts of acquiring infection, isolation, and fear of losing relationships. Sleep was often disturbed with nightmares. Some felt guilty of being responsible for the possible exposure of the virus to their family, especially to older persons, children, and pregnant women. Such fears and worries developed a sense of uncertainty about the future.
I am so scared about my family … My father is a patient, if he gets infected … that too because of me … Will I lose my father? Oh God! (sigh) I can't even think about it, my whole body is numb.
I don't mind if I die due to Corona, but I am concerned about my wife who is pregnant and our baby in her womb … They should be safe.
Quarantined persons complained that the pandemic has adversely affected the economy of their families. Unskilled/daily wage laborers, small-scale business people, and expatriates lost their jobs and were facing a severe financial crunch due to loss of income, debts, and repayment of loans. Most of them were in a vulnerable position and had to start everything from scratch for their livelihood. Such thoughts could have contributed to emotional distress and depression. As reported by a DNO:
People have lost their jobs … suddenly they have no money to run their house, repay the loans, chitty etc. They have lost their hopes … leading to anxiety and depression. Few of them have attempted suicide, unable to bear the stress due to financial issues.
Fear of the disease and concerns regarding social isolation precipitated stigma and discrimination toward the patients, travelers, and contacts. It has been noticed that people tend to hide their illness to avoid this. Even though the role of health care workers in the prevention and control of COVID-19 in Kerala is being recognized and appreciated widely, they are also facing stigma and discrimination from the public. The practice of putting a notice from the authorities in front of the houses where people are quarantined/isolated has induced shame and fear of being isolated by neighbors.
Issues such as financial insecurity and job uncertainty, along with fear of acquiring infection and social isolation, had triggered suicidal ideations in many. Alcohol withdrawal has also contributed to such ideations. As quoted by an expatriate:
I was in Dubai … lost my job during this crisis … all my fellow workers left to their places … I was alone in the labor camp and was a laughing stuff to all as there was nobody to take me home … except my aged parents … my wife had already left me … I will be devastated if I get infected. I have no other way … except suicide. Suddenly I got a revelation to call PSS Helpline number. The psychiatrist listened to me patiently … I was literally crying … it was a great relief and gave me ray of hope … He intervened and arranged for my return. Had I not made that call … I would not be here to talk to you.
Routine activities of all classes of people in all age groups were interrupted. Older persons were forced to stay at home and had to abstain from their routine leisure activities, such as morning/evening walks, visit to religious places, social visits, and gatherings. This in turn led to irritation, stress, anxiety, and agitation among them. This was more apparent among those who were living alone. As quoted by the SNO:
There was nobody to talk to older persons living alone … religious places were closed … no way to meet their peers … According to them, COVID is a curse to both humans and gods.
As educational institutions remained closed, children were homebound, escalating the burden of working parents. Mentally challenged children had a different set of problems. They became agitated by staying home as they were missing their friends, teachers, and their routine activities at their special schools.
Misinfodemics
Because COVID-19 is an emerging infectious disease, there were several misbeliefs and thoughts associated with it, which caused unnecessary fear among the public.
Initially, there were misperceptions regarding the symptoms, routes of infection, spread of the disease, and its treatment. There was so much hype about the disease, which resulted in undue fear among the people. One quarantined person's response:
I am hearing about such a disease for the first time in my life … terrified to see the rise in the number of cases. I am scared to eat, to touch door handles, utensils, and even to lie on my bed. These are soiled with virus … I will get infected if I touch them … can't imagine … if tested positive …
Bogus information through social media was a major problem from the start of the pandemic. Fake messages, images, and videos related to COVID-19 spread like wildfire, especially during the lockdown, and created panic among the public. They were ready to buy anything available in the market to combat COVID-19. Information, Education and Communication (IECs) materials regarding the reverse quarantine frightened older persons. As quoted by a DNO:
A 72-year-old man complained of frequent body pain, itching throat, and sweating of hands. He had a sense of feeling that he is going to die. He developed a kind of obsession and took frequent baths (six to eight times daily) and hand wash.
Experiences
Beneficiary
Prolonged stays at home and lack of regular social activities disrupted the emotional well-being of persons in quarantine, especially those who had an underlying cause. Timely interventions motivated them to adopt coping measures, including physical activities, relaxation exercises, positive thinking, and virtual socialization to regain the balance.
All were busily engaged in routine activities such as early morning cooking, physical activities, commuting to work, dropping off and picking up the kids from school, social/work responsibilities, weekends crammed with social activities, shopping, and grooming appointments before COVID-19. Everything came to a stop all of a sudden and it took a while for them to settle down, unlearn, and do with the bare minimum. They had plentiful time, but did not know what to do. PSST helped them to cope up with this new situation. They were motivated to learn new skills such as cooking, farming, stitching, and craft works and to develop new habits such as reading and indoor recreational activities, such as yoga. One beneficiary shared this vignette:
As recommended by the team, I have started exercises and using mindfulness-based stress reduction. I feel better now.
The PSST provided awareness and updates regarding the prevention and control of COVID-19 and equipped individuals and families to overcome the challenges/difficulties that cropped up in this crisis situation. This intervention could save many from the verge of suicide by enabling reassurance, positive thinking, and optimism.
The persons under quarantine had different requirements. Some of them opened up with a lot of expectation and considered the phone call as a last resort. The counselors could not only limit their service to psychological support, but were obliged to address their social needs as well. There was demand for essential items such as food, books, newspapers, clothes, medicines, and other groceries. The PSST tried to address these issues by reporting them to the concerned.
Provider Experiences
Several psychological, physical, and social requirements during the pandemic made people more vulnerable. In such a situation, a friendly phone call offering help was received with great appreciation. Consequently, efforts were made to develop a relationship between the counselor and the beneficiary. The expression of immense affection by the beneficiary granted a feeling of contentment and gratefulness to the providers. The positive experiences they shared improved the self-esteem and satisfaction of the providers. It created a feeling of entitlement, thus forcing them to be more responsible and committed in their work to fight this battle as a team.
This experience is unique and I am proud to be part of this. Appreciation and pleased words from the beneficiaries motivate us to work hard. They have given us a position in their hearts and even consider me as a brother.
Success Stories
Averted Psychiatric Emergencies
Effective and timely interventions have helped to avert psychiatric emergencies such as suicides and aggressive behavior. The PSST strongly believed that the interventions they provided over the phone have touched lives in a positive manner.
One of the DNOs recalled a distress call received at 1:30
It was an expatriate from Dubai who was alone in the house and was all prepared to end his life. He took his phone to have a last look at his child's photo. Suddenly his eyes struck on a call he received last day from one of our counselors. He called in the number and even in that late-night hour, the counselor attended and talked for about one and half hours. He was totally shattered and was in severe despair. As it was an emergency, the call was diverted to me. I talked to him to avert his suicidal ideation. He was shifted to the hospital immediately and treatment was started at once.
Benefitted the Individual and Family
Even though the interventions were targeted for quarantined persons, the system actually benefitted persons belonging to all strata. The general public faced severe psychological issues during the lockdown because of fear and apprehension regarding loved ones who were stranded elsewhere.
One of the DNOs narrated an incident of a severe case of psychosis:
A young man working in the IT sector had to travel to Bangalore, leaving alone his wife with two small children in a flat. They had recently shifted to Trivandrum and had no friends or relatives nearby. He was held up in Bangalore as the declaration of lockdown came as a surprise. As the days passed, the wife became anxious and developed symptoms of psychosis. She did not feed the children nor care for them and refused to receive food from neighbors, suspecting the food being infected with virus. She went out in the rain, took a bath outside, beat up her children, and slowly transformed to a full-blown psychosis. Neighbors sought help in our helpline number. Her husband was contacted, briefed on the situation, and with his consent she was shifted to the hospital. Meanwhile, necessary arrangements were made for his return and for care of the children. To enable speedy recovery, hospital authorities permitted him to meet his wife during the quarantine period itself, abiding COVID protocol. Within five days, her symptom improved and she was sent home with her husband and children with weekly follow-up.
The study attempted to formulate a hypothetical model showing the interaction between identified themes and subthemes (Figure 2). It has been found that the state's novel psychosocial support system tackled the psychological and social issues associated with the pandemic promptly and effectively, thereby benefitting both individuals and families.
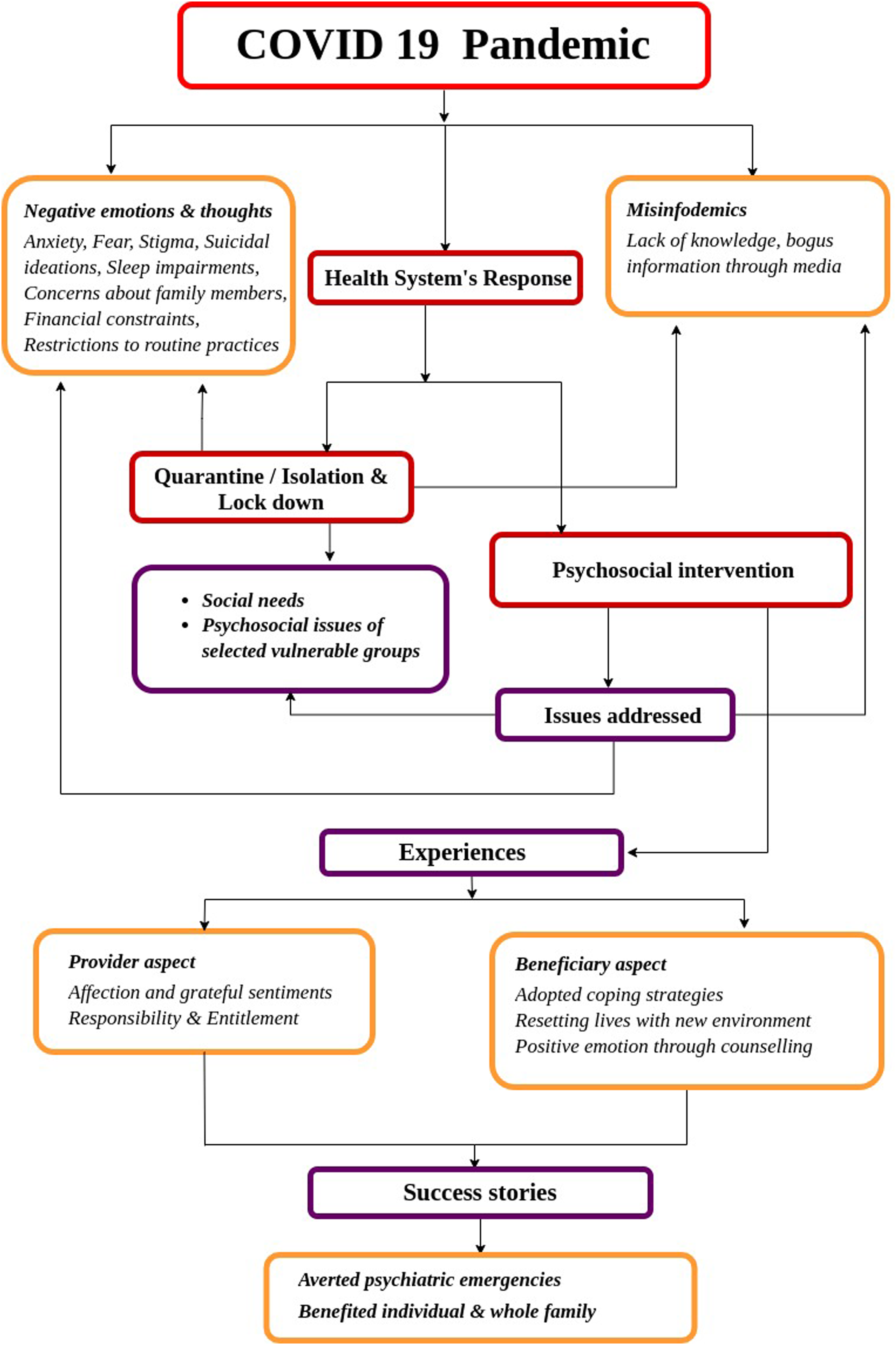
Hypothetical model showing the interaction between themes and subthemes.
As part of this intervention, about 4 355 964 calls were made from February 4 to October 31, 2020. Out of this, more than 40% were active reassurance calls made to persons in quarantine/isolation, more than 25% for special target groups, and the rest were follow-up calls. Based on secondary data, we found that depression (75.2%) was a major problem among those who were under home quarantine, followed by stigma (69.5%) and anxiety (69.4%). Among patients who were under hospital isolation, sleep impairment was the main issue (43%). We found that many people who were under home quarantine faced difficulty in purchasing their regular medicines, food, and groceries, to take medical consultations (Figure 3) (State Mental Health Office, 2020).
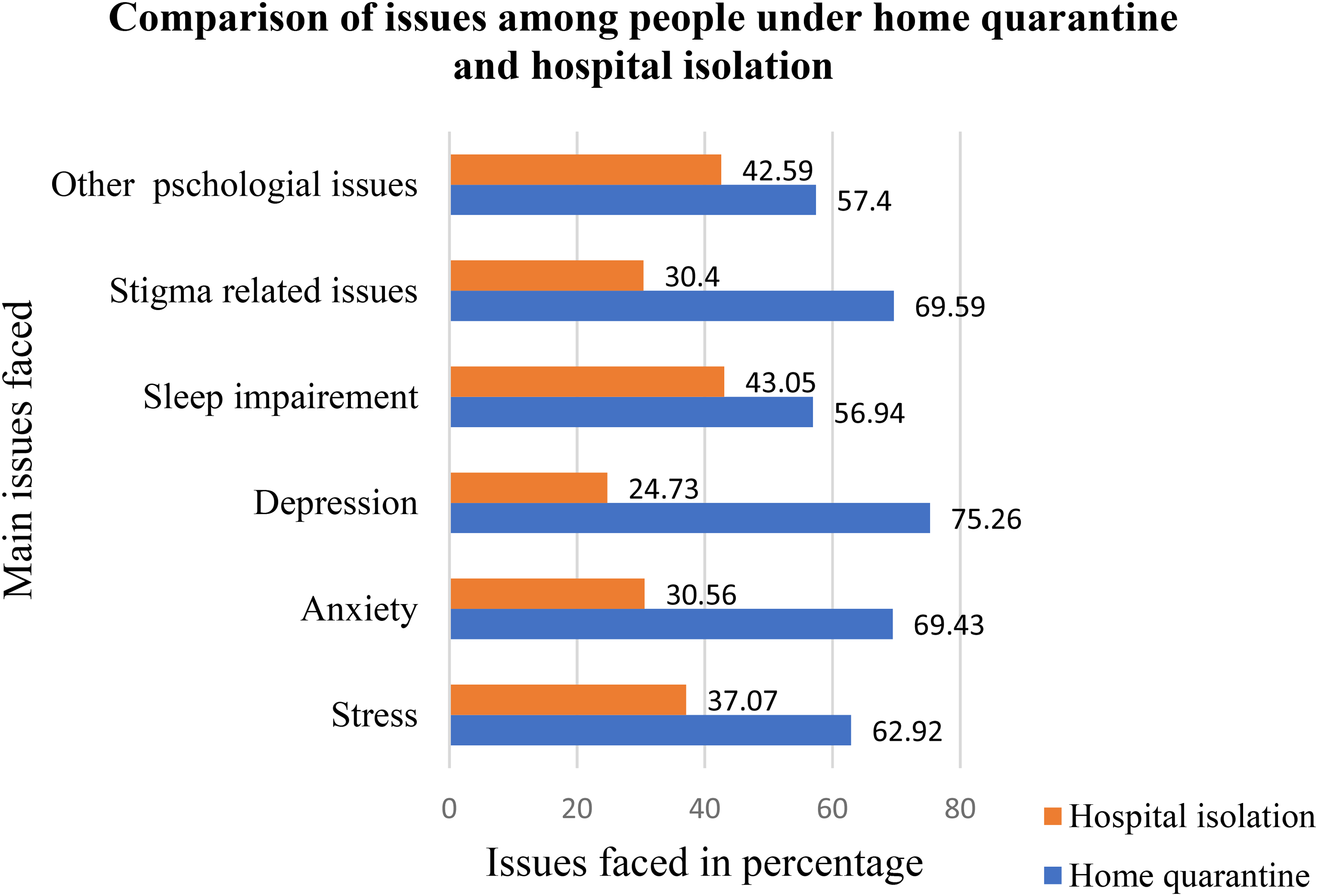
Issues among people under quarantine and patients under isolation.
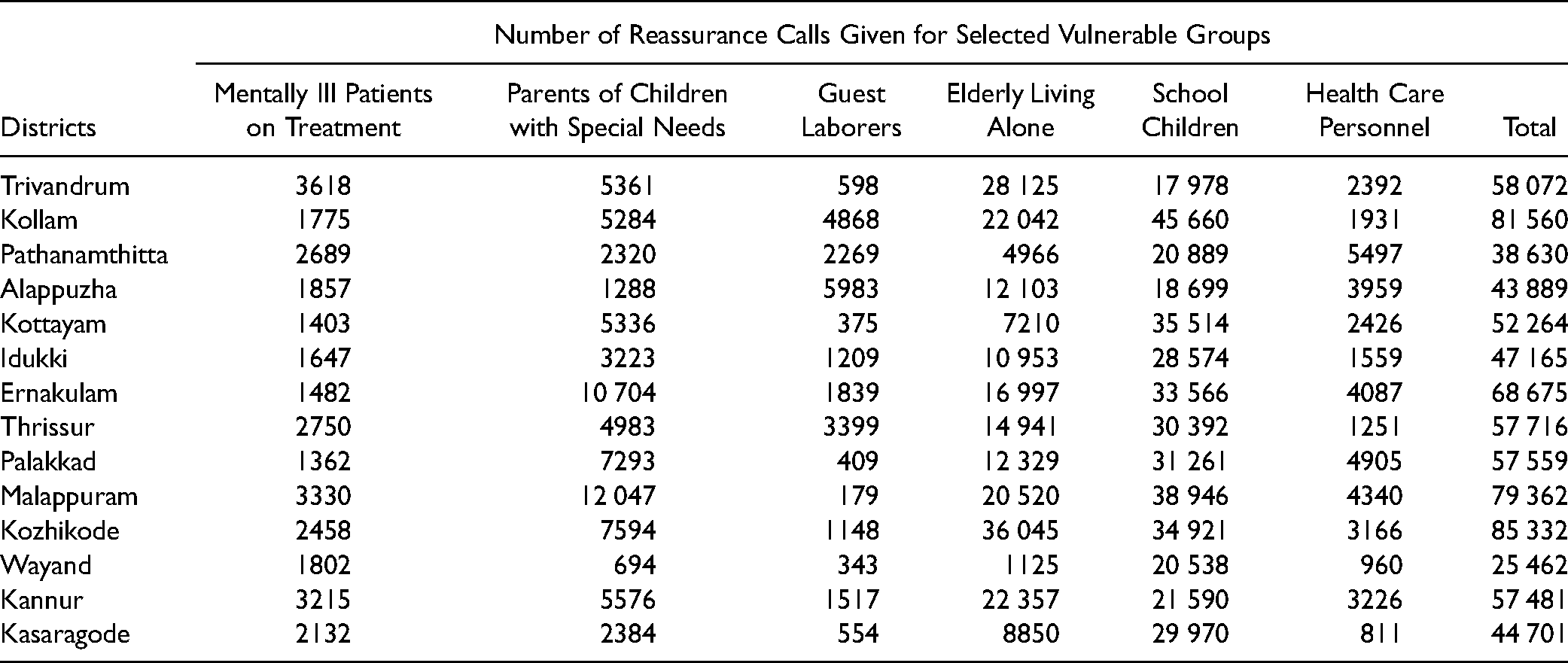
It has been found that the number of calls was higher in 2 districts, namely Ernakulam (325 544) and Thiruvananthapuram (310 372), where a higher number of cases was reported (1112 and 790, respectively). During lockdown, the team extended its support to some 6 special target groups. The number of calls given by the PSST for such groups is depicted in Table 2. Overall, a large number of calls were made in the Kozhikode district, followed by Kollam and Malappuram. Among the selected vulnerable groups, the PSST of all districts gave immense support to schoolchildren and to elderly people living alone.
Reassurance Calls Made for Target Groups During Lockdown.
Discussion
This study tried to describe the innovative and novel intervention adopted by the state during the COVID-19 pandemic to address the psychosocial needs of the public. It also explored the experiences of both provider and beneficiary with the intervention. As mentioned in some earlier studies, it is vital to understand the psychosocial issues connected with COVID-19 to find evidence-based methods to address them.9–11 Some of the issues that emerged are common to all countries and all settings. However, we have some specific issues that have to be dealt with. Broadly, the findings can be summarized into 4 major themes.
The intervention was given for 9 selected categories based on the notion of “xenophobia” reported during previous epidemics and pandemics. 12 The pandemic has not only imposed strong and extensive psychosocial consequences on the general population, but also on the medical population, which abridged the capacity, responsiveness, and pliability of the health care system irrespective of private and public.13,14 Previous outbreaks have shown that the psychological impact of quarantine can vary, from immediate effects, such as irritability, fear of contracting and spreading infection to family members, anger, confusion, frustration, loneliness, denial, anxiety, insomnia, and despair, to extreme consequences, including suicide.15–17
Similarly, this study could identify many psychosocial issues such as anxiety, fear of isolation, stigma, and nonrealistic panic on lockdown-related scarcity of essential and emergency services.18–20 “Coronaphobia,” a mass fear of COVID-19, might generate negative psychological responses, including maladaptive behaviors and emotional distress.9,11 Concerns about family members, especially older people and children, were common among isolated/quarantined persons, consistent with another study. 21 Suicidal ideations associated with high perceived stress related to COVID-19 were found as a major issue, comparable with other studies.22,23 The study identified that psychosocial intervention was helpful in providing emotional relief to those quarantined/isolated. The World Health Organization (WHO) has also issued specific considerations to reduce psychosocial problems, especially the stigma associated with COVID-19.
“Misinfodemics” or misinformation during a pandemic is crucial as it is usually widespread through social media/mass media and may have psychological impacts in the form of mass confusion, panic, anxiety, phobia, depression, obsession, irritability, delusions, and other paranoid ideas. 24 Similar issues were noticed, especially among older people, that resulted in obsessive compulsive symptoms. Unchecked mind-boggling rumors, flashy news propaganda, and sensationalism cause “coronavirus infodemic,” a term coined by the WHO that denotes fright and panic due to the COVID-19 pandemic. 25 Social media platforms were used for spreading misinformation by laypersons in an impetuous and erratic manner to gain popularity and income. Strict measures were taken as part of the intervention to create awareness regarding misinfodemics among the public. Cases of misinfodemics, if noticed, were reported to the media cell, one of the 18 committees of the Rapid Response Team at the state level, for further action.
Many persons could benefit from and adopt positive thinking and develop other psychological defense mechanisms to overcome the crisis. Reports suggest that counseling services addressed psychological and behavioral health sequelae of pandemic COVID-19 and effectively equipped vulnerable people to handle the catastrophe.26–28 Psychosocial intervention through tele-counseling services also helped people, especially expatriates, to develop more rational and positive attitudes. It helped most of the beneficiaries adopt coping strategies, including relaxation techniques, meditation, and mindfulness, and extracurricular activities, indoor recreational activities, reading, gardening, and cooking.
Few studies related to COVID-19 identified quarantined/isolated persons, children, and older persons as vulnerable populations, whereas our study found expatriates as vulnerable apart from other categories. The interventions helped them to adapt to the current, stressful environment and to get rid of their suicidal ideations. A higher number of psychosocial support calls was made by districts with higher numbers of active cases.
It was found that the main reason for the success of this intervention was intersectoral coordination. The roles played by the line departments, including labor commission, social justice, women & child development, police, local self-government, and education departments, were laudable. Proper coordination at grassroot levels helped a great deal to connect the target groups and to address their social needs effectively. Appropriate and timely action and communication with other members in the rapid response team were also found to have played a pivotal role.
Even though this intervention was received with great enthusiasm, there were a few challenges during the implementation. Contact numbers of some persons under quarantine/isolation provided by the districts were either wrong or belonged to the hotel/resort/travel agency. As a result, the team found it difficult to reach out to all of them. Some events that could have been prevented could not be prevented due to a delay in getting the list of target people.
As per our knowledge, this is the first study from Kerala, India, on psychosocial interventions during the COVID-19 pandemic. This intervention is flexible, sustainable, and equitable as it is piggybacked on an existing system of DMHP. Because the program is not resource intensive, this model can be replicated effectively anywhere in the world. Nonavailability of the sociodemographic characteristics of participants limited further analysis.
Conclusion
This study provided a comprehensive description of the psychosocial intervention adopted by the state during the COVID-19 pandemic. To an extent, it has contributed immensely to alleviating the psychosocial issues that prevailed during quarantine and lockdown. Prevention of some psychosocial emergencies can be flaunted as a major achievement of this intervention. The program can be projected as a robust and cost-effective model for other states to adopt (Supplemental data).
Supplemental Material
sj-docx-1-joh-10.1177_00207314211019240 - Supplemental material for Psychosocial Intervention Model of Kerala, India During Pandemic COVID-19: “Ottakkalla Oppamundu (You’re not alone, we’re with you)”
Supplemental material, sj-docx-1-joh-10.1177_00207314211019240 for Psychosocial Intervention Model of Kerala, India During Pandemic COVID-19: “Ottakkalla Oppamundu (You’re not alone, we’re with you)” by Rekha M. Ravindran, Anjali Krishnan R., Kiran P.S., Bindhu Mohan and Shinu K.S. in International Journal of Health Services
Supplemental Material
sj-docx-2-joh-10.1177_00207314211019240 - Supplemental material for Psychosocial Intervention Model of Kerala, India During Pandemic COVID-19: “Ottakkalla Oppamundu (You’re not alone, we’re with you)”
Supplemental material, sj-docx-2-joh-10.1177_00207314211019240 for Psychosocial Intervention Model of Kerala, India During Pandemic COVID-19: “Ottakkalla Oppamundu (You’re not alone, we’re with you)” by Rekha M. Ravindran, Anjali Krishnan R., Kiran P.S., Bindhu Mohan and Shinu K.S. in International Journal of Health Services
Supplemental Material
sj-xlsx-3-joh-10.1177_00207314211019240 - Supplemental material for Psychosocial Intervention Model of Kerala, India During Pandemic COVID-19: “Ottakkalla Oppamundu (You’re not alone, we’re with you)”
Supplemental material, sj-xlsx-3-joh-10.1177_00207314211019240 for Psychosocial Intervention Model of Kerala, India During Pandemic COVID-19: “Ottakkalla Oppamundu (You’re not alone, we’re with you)” by Rekha M. Ravindran, Anjali Krishnan R., Kiran P.S., Bindhu Mohan and Shinu K.S. in International Journal of Health Services
Supplemental Material
sj-docx-4-joh-10.1177_00207314211019240 - Supplemental material for Psychosocial Intervention Model of Kerala, India During Pandemic COVID-19: “Ottakkalla Oppamundu (You’re not alone, we’re with you)”
Supplemental material, sj-docx-4-joh-10.1177_00207314211019240 for Psychosocial Intervention Model of Kerala, India During Pandemic COVID-19: “Ottakkalla Oppamundu (You’re not alone, we’re with you)” by Rekha M. Ravindran, Anjali Krishnan R., Kiran P.S., Bindhu Mohan and Shinu K.S. in International Journal of Health Services
Footnotes
Acknowledgments
The authors are pleased to acknowledge the contributions of the whole DMHP team and District Nodal Officers of Mental Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.