
Abstract
The concept of the social determinants of health has become increasingly accepted and mainstream in anglophone public health over the past three decades. Moreover, it has been widely adopted into diverse geographic, sociocultural, and linguistic contexts. By recognizing the role of social conditions in influencing health inequalities, the concept challenges narrow behavioral and reductive biological understandings of health. Despite this, scholars and activists have critiqued the concept of the social determinants of health for being incomplete and even misrepresenting the true nature of health inequities. Arguably, these critiques have been most thoroughly developed among those working in the Latin American social medicine and collective health traditions who formulated the “social determination of health” paradigm and the concept of interculturality decades prior to the advent of the social determinants of health. We draw on Jaime Breilh's main works, with a focus on the recently published book, Critical Epidemiology and the People's Health, to (1) provide a broad overview of the social determination of health paradigm and its approach to interculturality and (2) clarify how these ideas and the broader collective health movement challenge assumptions within the social determinants of health concept.
Keywords
Introduction
Social Determinants of Health
The social determinants of health refer to “the conditions in which people are born, grow, live, work, and age that shape health”. 1 Common examples of these health-relevant conditions include “socioeconomic status, education, neighborhood and physical environment, employment, and social support networks, as well as access to health care”. 1 Although the modern origins of the social determinants of health concept can be traced to the 1974 Lalonde Report and the 1986 Ottawa Charter, the term itself gained global prominence with the work of Wilkinson, Marmot, and others,2,3 especially with the widely cited 2008 report, Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health, which emerged from the World Health Organization's (WHO) Commission on Social Determinants of Health. The concept of the social determinants of health has subsequently received widespread attention from scholars in the anglophone world and globally. 4
The concept's advocates applaud its role in centering social conditions and inequality in discussions of health, disease, and their unequal distribution. These advocates see the social determinants of health concept as a corrective to narrow understandings of health that overemphasize the role of individual agency in health outcomes (i.e., unhealthy behaviors and lifestyles) and as a corrective to biomedical accounts of health that overemphasize acontextual biological pathology (i.e., “genetic drivers of disease”). By centering social conditions and inequality, the social determinants of health have become closely associated with struggles for health justice and equity.
However, scholars and activists working within the Latin American social medicine and collective health tradition contest this perspective and posit instead that the social determinants of health concept systematically—even if unintentionally—elides the social processes and forces generating unhealthy social conditions. In addition, they critique the social determinants concept for adopting a truncating logic that elides the complex, multidimensional, and interrelated processes that characterize social reality and focuses instead on discreet “factors” that can be isolated and placed within a Cartesian, linear, causal chain linking abstracted social conditions with health disparities. As a result, the concept forecloses more accurate understandings of the social dimensions of health and subsequent actions that could achieve health justice.
Latin American Social Medicine and Collective Health
Latin American social medicine/collective health refers to a movement and a body of theoretical and practical contributions of community members, activists, practitioners, and scholars fighting for the right to health and against social inequality and political repression throughout the region. Although the movement took definitive form in the 1970s, its historical antecedents can be traced to various currents, including Latin American thinkers such as Eugenio Espejo, Manuela Espejo, José Mejía Lequerica, Ricardo Paredes, Ramón Carrillo, and Salvador Allende, 5 as well as those associated with the nineteenth-century European social medicine tradition, such as Friedrich Engels, Louis-René Villermé, and Rudolf Virchow. 6 The movement seeks to understand more fully the relationship among social processes and organization—with a focus on political economy—and the unequal distribution of health and disease. But the movement is not simply theoretical or academic; many participants are actively engaged in social movements and political coalitions dedicated to health justice.
In part to distance their work from an overly biomedical framing that might be implied by the term “social medicine,” some Latin American scholars have adopted the term “collective health” to refer to this movement. 7 Collective health, a term originally coined in the context of Brazilian health reform movements, surpasses both individually focused health promotion and institutional public health actions. It is principally focused on collectively organized action to confront, understand, and modify social processes so that they protect and improve—rather than harm and degrade—human and natural life. 5 (p. 31) Although the terms “Latin American social medicine” and “collective health” have distinct origins and meanings, they are nonetheless often used interchangeably. While recognizing this complexity, we default to the term “collective health” throughout this article.
Many working in collective health were initially hopeful at the prospect of the WHO Commission on Social Determinants of Health. Since the late 1970s, collective health scholars have contributed to developing a novel paradigm for understanding and explaining health in social terms, referred to as the “social determination of health” paradigm.5,8–11 Given the semantic and topical similarity, the concept of the social determinants of health seemed to be drawing on that work and placing it on a more global and visible stage. However, in time, collective health scholars realized that the concept of the social determinants of health—or “determinants theory”—diverged from their work in significant ways and even contained features that these scholars had long critiqued. 12 In light of this, many collective health scholars perceived a reenactment of colonial relations whereby academics from “core” North American and European countries extracted conceptual terminology and innovations from post-colonial countries in the global “periphery,” redefined those concepts in ways that contradicted some of their original meanings, and presented them as novel without reference to the scholars in Latin America who developed those concepts.
Social Determination of Health
Decades prior to the WHO Commission, Latin American scholars had developed various conceptual innovations for understanding the relationship among social organization, social processes, and disease distributions. Arguably, the most prominent of these innovations is the social determination of health paradigm, which was first proposed by Jaime Breilh in 1977 8 and further developed in the decades since by Breilh and various scholars of collective health. The paradigm draws broadly on diverse disciplinary and theoretical traditions, and it presents a challenge to the concept of the social determinants of health. While a comprehensive review of this paradigm is beyond the scope of one article, an overview is necessary to contrast it with the “determinants theory” of the social determinants of health.
Breilh borrows the definition of determination from Mario Bunge, 13 who characterized one dimension of the term as “a mode of becoming—how a process becomes such and acquires its characteristics”. 5 (p. 101) This definition recognizes that “epidemiological processes have empirically defined characteristics, which can be observed and recorded as variables”. 5 (p. 101) At the same time, epidemiological processes acquire their characteristics through social processes that transcend empirically observable causal conjunctions. Recognizing that health and disease are socially determined entails expanding the scope of epidemiological analysis so that it “is not limited to the phenomenon (i.e., single-plane ‘tip of the iceberg’) but must encompass the underlying determinant movements that generate the empirically observable elements”. 5 (p. 101) In this way, the social determination paradigm rejects the Humean empiricism5,14 that undergirds mainstream epidemiological thought in the works of Hill, 15 McMahon, 16 Rothman and Greenland, 17 and others and grounds it instead in dialectical formulations present in Marxian critiques of political economy,18,19 radical biology, 20 and critical realism. 21
A principal concept of the social determination paradigm is “subsumption”,5,8–11,22–25 which is taken from Marx's dual concepts of formal and real subsumption that describe the way that production is transformed under capitalist political economy. Within the social determination paradigm, the concept of subsumption displaces the reductive notion of causality as it is presented in the mainstream epidemiological paradigm. Subsumption involves the conditioning of a less complex process by a more complex one. According to Breilh, “Subsumption means incorporating by dominating and constraining to new conditions. The very development of the subsumed processes is restructured according to the limits and determinations imposed by the more complex order”. 22 (p. 81) Breilh sees this process of subsumption operating across three nested domains: general, particular, and individual.
The outermost “general” domain is the most complex and therefore subsumes, or conditions, the less complex “particular” and “individual” domains. The general domain comprises the broad structural characteristics and power relations of a particular social formation and its mechanisms of reproduction, such as wealth production and capital accumulation, social relations, and society–nature metabolism (discussed further below). The subsequent middle “particular” domain comprises collective “modes of living,” which refers to group-differentiated patterns of life that exist along social hierarchies. This can include the shared consumptive practices, working conditions, incomes, and environmental conditions of particular social groups across social categories such as class, racial or ethnic group, and gender. Finally, the individual domain is the least complex and comprises individual “styles of living.” A style of living is distinct from the popular “lifestyle” concept in public health and medicine, referring to a host of interrelated attributes at the individual level, such as an individual's “capacity to organize actions in defense of health”, 5 (p. 125) their material resources, formal membership in organizations, subjectivity, identity, beliefs, values, and individual ecological settings. This process of subsumption across general, particular, and individual domains “concomitantly conditions the phenotypic, genotypic, and psychological processes of an individual” 5 (p. 110) and defines social reproduction, or the perpetuation of a social order, along with its epidemiological patterns, over time.
However, social reproduction is also shaped by humanity's relationship with nature, or—drawing on Marxian ecological theory—“society–nature metabolism”. 26 This refers to the various dynamics and processes of consumption, utilization, and transformation that characterize the human–nature relationship. For example, the accumulation of capital, a primary aspect of the general domain, is reliant on not only human labor, but also on the utilization of natural resources. And beyond utilizing these natural resources, this process also degrades environments and produces environmental hazards in the form of pollution. The impacts of degraded environments and environmental hazards are not evenly distributed across social groups and individuals. For Breilh, this relationship is central to the social determination paradigm because it shapes each of its domains, from the general to the particular and the individual 5 (see Figure 1).
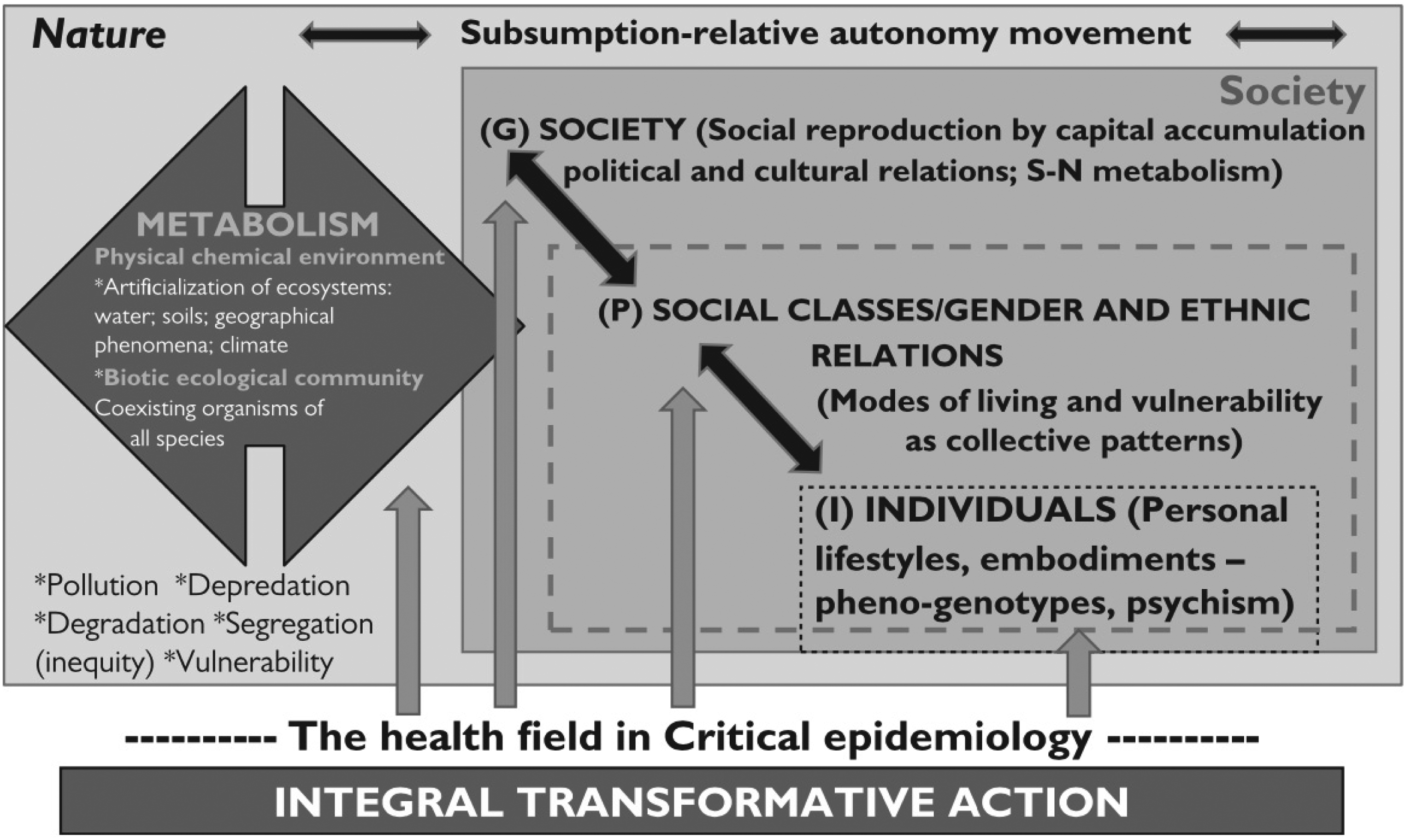
The social determination of health (complex-multidimensional movement). G, general; I, individual; P, particular. Originally published in. 5 (p. 96)
Breilh stresses that this process of determination is not deterministic. That is to say, this nested system of conditioning across the general, particular, and individual domains (i.e., subsumption) “is not a unidirectional mechanical relationship”. 5 (p. 110) Rather, subsumption exists in a dialectical relationship with the “relative autonomy” of sub-domains. While forms of political economy, the organization of production, and the accumulation of capital (general domain) will condition forms of social hierarchy across social groups based on class, racialized group, gender, and so forth (particular domain) that are embodied within individuals and manifest as observable health conditions (individual domain), there are ways in which change in the individual sub-domain can condition the more complex domains. For example, individuals and collectivities can organize and participate in coordinated political actions that may, in turn, modify the more complex “particular” and “general” domains, which in turn will result in new subsumptive patterns and epidemiological profiles.
Critiques of the Social Determinants of Health Framework
“Tip of the Iceberg” Empiricism and Linear Cartesian Causality
From the perspective of the social determination paradigm, the concept of the social determinants of health is limited at the levels of its basic assumptions, focuses, and premises. Whereas the social determination paradigm seeks to understand a collective totality and how it produces various embodiments in the form of disease distribution, severity, and frequency according to inequitable social relations and subsumptive patterns, the “social determinants” concept seeks to establish a reductive causal chain of social risk factors (i.e., socioeconomic status, education level, characteristics of the neighborhood and physical environment, employment status and working conditions, and access to health care) divorced from the social processes that generate them. Analysis of these social processes is largely absent from the social determinants of health literature because such processes elude the mainstream epidemiological paradigm from which the social determinants of health concept emerges. According to Breilh, the limited, fragmented, and abstract image of social reality portrayed by mainstream epidemiology betrays a linear Cartesian logic that is incapable of capturing the holistic social totality that more accurately depicts the social dynamics responsible for the production of health, disease, and their distribution. As a result of mainstream epidemiology's limited ontological, epistemological, methodological, and political commitments, the processes responsible for social reproduction and the perpetuation of health inequities are necessarily ignored and left uninterrogated.
An example is useful to ground this critique and contrast the alternative approaches. Socioeconomic status, for instance, is considered a principal social determinant of health. 5 (p. 160) Within mainstream epidemiology, socioeconomic status is often operationalized as income. Income, then, becomes a central variable in different analyses seeking to understand associative and causal relationships between it and various health outcomes, findings that in turn attract significant professional and public attention. However, in the imposition of mainstream epidemiological logics and methods, there is a necessary separation of the income variable from a holistic understanding of society, its prevailing social hierarchies, collectives (such as class, gender, racialized groups, etc.), the power exerted by those collectives, and underlying social processes such as capital accumulation operating historically, geographically, and differentially across these different social hierarchies. As a result, a holistic and critical understanding of social determination and political economy is foreclosed through the reductive incorporation of complex social phenomena into mainstream epidemiology. And, in a sense, this fragmented view of social reality that mainstream epidemiology provides is the basis for the social determinants of health.
To develop the example further, a mainstream epidemiological finding that, say, heart disease is more common among people with lower incomes calls for public health interventions to promote “heart-healthy” lifestyles, or information campaigns about these disease patterns among health care providers so they can more effectively treat these patients, or—in perhaps a more socially progressive scenario—an increase in resources to low-income people or even political demands to reduce economic inequality. However, many of these “reasonable” responses redirect attention (and sometimes responsibility and blame) to the actions of individuals, and all fail to grasp the fundamental process of social reproduction underlying this “tip of the iceberg,” empirically observable epidemiological fact. In this way, the social determinants of health, mainstream epidemiology, and—in Breilh's terms— “functionalist” public health foreclose forms of radical praxis 1 that might direct attention to, and ultimately challenge, these social processes.
The social determination of health paradigm insists that epidemiological tools of analysis cannot be allowed to divorce the empirically observable from their generative social processes. These must be analyzed as part of one holistic social, political, and economic totality that is sensitive to intersecting social forces. With regard to such forces, Breilh writes, “domination is not only class-based, but also forms a power structure, which is crossed and reproduced by relations of economic appropriation and expropriation, as well as by relations of ethnic and gender subordination”. 27 (p. 3) “[…] these three forms of inequality—class, ethnic, and gender inequality […] share the same germinal root, which is the accumulation and concentration of power, and […] the social reproduction of the three types of inequality is interrelated”. 27 (p. 3) This is important because, from the standpoint of Latin American social medicine and collective health, epidemiology needs to be part of an emancipatory political process.
Inequality, Equity, and Praxis
A related critique of the social determinants of health concept is that it is fundamentally concerned with documenting inequality, rather than understanding and acting on inequity. Breilh provides definitions of these two oft-discussed terms that diverge somewhat from their common usage within anglophone public health. According to Breilh, inequality refers to “the empirical embodiment of inequity” 5 (p. 158) and “the empirical ‘tip of the iceberg” expression of unfairness’. 5 (p. 158) As discussed, this is the traditional focus of the social determinants of health and mainstream epidemiology, which seeks to understand the relationship between social conditions (understood as empirical social risk factors) and disease distributions. On the other hand, inequity refers to “the mechanisms for [the] concentration of power by a social minority and the corresponding process of exclusion of the subordinate groups with regard to the access to goods and rights”. 5 (p. 158)
Whereas scholars motivated by the social determinants of health concept might examine unequal access to pharmaceuticals and the effect this has on health outcomes, those working within the social determination paradigm would seek to understand subsumptive patterns across general, particular, and individual domains and how these give rise to unequal pharmaceutical access. The latter approach entails analysis of the historical role of pharmaceutical companies in national and international political economy, their prioritization of profit and accumulation of capital over collective health, and their strategies for exercising power to realize those priorities—as well as how those processes within the general domain in turn subsume and shape the particular and individual domains. This analysis necessarily includes important “tip of the iceberg” empirical, epidemiological findings, such as differential access, but is not limited to those findings.
The difference between the inequality focus of the social determinants of health and the inequity focus of the social determination of health is not simply theoretical and epistemological; it is also practical and political. By isolating social risk factors and analyzing their effect on disease distribution, mainstream epidemiology calls for direct action on these social risk factors or, perhaps more commonly, indirect actions on individuals and their behavior that might mitigate the effects of risk factors. But this betrays Virchow's call for “radical measures” to address the social mechanisms that generate and distribute social risk factors, rather than “mere palliatives” 5 (p. 14) that seek to modify the risk factors themselves while leaving the broader structural conditions and social processes intact. The latter “palliative” approach results in a “functionalist” public health5,8,10,14 that is concerned with administering inequality instead of addressing inequity. In contrast, by focusing on inequity, “the mechanisms for [the] concentration of power”, 5 (p. 158) “process[es] of exclusion”, 5 (p. 158) and pathogenic social processes, the social determination paradigm informs political action aimed at reforming, transforming, and even abolishing these social dynamics.
Transdisciplinarity and Interculturality
Finally, Breilh and others within collective health have noted that due to its emergence from mainstream science and epidemiology, the social determinants of health concept represents the perspective of a disciplinarily narrow scientific community, one with a cultural specificity that is distinct from the social movements and groups with which it interfaces. By failing to recognize its disciplinary limits and Eurocentric cultural norms, mainstream epidemiology risks reproducing the hierarchies it claims to address.
According to Breilh, The roots of functional, monomethodic, monocultural, and ‘Eurocentric’ thinking and practice can be found in the long process that began in colonial times. From our perspective, dominant Eurocentric knowledge does not fundamentally refer to the geographical or cultural origin in itself but, rather, to the dominant ontologies and epistemologies contained in the conservative science that accompanied the expansion of European rule, and the racist, patriarchal, and aristocratic philosophies of the ruling groups.
5
(p. 186)
To correct these shortcomings, collective health scholars have developed and built on the related but distinct concepts of multidisciplinarity, transdisciplinarity, and interculturality. On the one hand, Breilh defines multidisciplinarity as the “integration of the different scientific disciplines through interdisciplinary analysis, in a solidary-based scientific process, for the construction of a common project”. 10 (p. 286) On the other hand, transdisciplinarity goes even further and entails systematic integration of knowledge, articulation of conceptual frameworks, transgression of disciplinary boundaries, and prioritization of problem-solving. 28 It involves overcoming disciplinary compartmentalization and acts on the call to undiscipline disciplines. 29 Such “undisciplining” of the scientific endeavor is evident in the development of the social determination paradigm, which draws broadly from across scientific domains in order to construct a more accurate account of social processes, social hierarchies, and epidemiological distributions (Figure 1) and puts those analytic tools in the service of collective needs, political projects, and social emancipation.
However, even a transdisciplinary science that recognizes and seeks to work across disciplinary norms and cultures is not sufficient to establish a collective project for health equity because it fails to engage with forms of systematized knowledge that reside outside of the official institutions of science—for example, within popular or indigenous forms of knowledge that comprise unique and complex ontologies, epistemologies, moralities, and conceptions of justice, which ground knowledge about health and disease.30,31 The concept of interculturality has been developed to facilitate the articulation of discrepant and complex worldviews. Interculturality can be defined as “the integration of several cultures in the midst of a shared cultural vision, for the construction of a common project of democratization and equity, that is, where different cultures can reproduce and mutually sustain themselves under equal rights, responsibilities and opportunities”. 10 (p. 286)
Breilh's concept of interculturality5,10,27,32 goes well beyond—and even against—popular academic attempts to grapple with the idea of cultural difference through, for example, the concepts of multiculturalism, acculturation, integration, assimilation, or cultural competency. 2 Indeed, some of these concepts often reassert hegemonic forms of culture (e.g., Western, Eurocentric scientific culture) under the guise of cultural diversity and “multiculturalism.” Recognizing the ways that European cultural norms have been universalized in the realm of science to dominate, dispossess, and facilitate the extraction of resources, interculturality sets itself as a “counter-hegemonic” process that seeks to integrate “the strengths of all voices, and the progressive veins of all views”. 10 (p. 38) In this way, the objective of interculturality is fundamentally political, putting various sources of knowledge—Western and non-Western, academic and non-academic—at the service of a collective, emancipatory project. It entails the production of a new form of multiculturalism that enables productive critique and synthesis of different forms of knowledge. Thus, it puts the best critiques, scientific resources, and community resources at the service of an “articulated social bloc” of “affected communities and concerned and mobilized stakeholders”. 5 (p. 209)
Breilh goes so far as to state, “the major challenge and objective of twenty-first-century epidemiological knowledge is the construction of participative interdisciplinary–intercultural knowledge platforms”. 5 (p. 192) However, interculturality is not an uncomplicated project as the history of different systems of knowledge is characterized by hierarchy and violence—both structural and interpersonal—and animated by intertwined projects of colonialism, racism, patriarchy, and capitalism. Hegemonic science has been put into the service of these projects and used as a tool to eliminate other, potentially conflicting, systems of knowledge. These historical and contemporary asymmetries of power must be confronted through consultation and the prioritization of historically oppressed communities in the construction of an intercultural political project of emancipation in the realm of society and health.
In this way, interculturality is not an event or a competency, but rather a process that involves a “double translation” or cross-fertilization, wherein reciprocal enrichment occurs in a framework of solidarity and in the context of a project of struggle for equity and the elimination of class, gender, racial, and ethnic hierarchies. Drawing on work by Mignolo,
37
Breilh defines double translations as the process by which two logical apparatuses, two worldviews prepare to ‘contaminate’ each other to enrich the vision and overcome limitations. Interculturality is an emancipatory process supported by solidarity work from various cultures, without the absorption of one with respect to the other. Going through this double translation allows for the strengthening of the critical horizon of knowledge and nurtures a practice of health in equity; equity through the struggle for the abolition of a class society, the struggle to overcome gender asymmetry, and the struggle for emancipatory multiculturalism.
10
(p. 64)
This challenge to the “uniculturality” of mainstream epidemiology and the social determinants of health, grounded in collaborative work with indigenous communities and organizations, has led Breilh and others in collective health to emphasize the importance of systematized knowledges beyond the formal scientific domain. One such form of knowledge resides within South American indigenous thought centered on Sumak Kawsay, 38 roughly translated as “living well,” which similarly challenges oppressive social hierarchies, extractive human–nature systems, and endless capital accumulation (Table 1). Instead, Sumak Kawsay puts forward a rich philosophy and worldview emphasizing solidarity, reciprocity, complementarity, and relationality.
Complementarities of Critical Academic and Indigenous Thinking a .
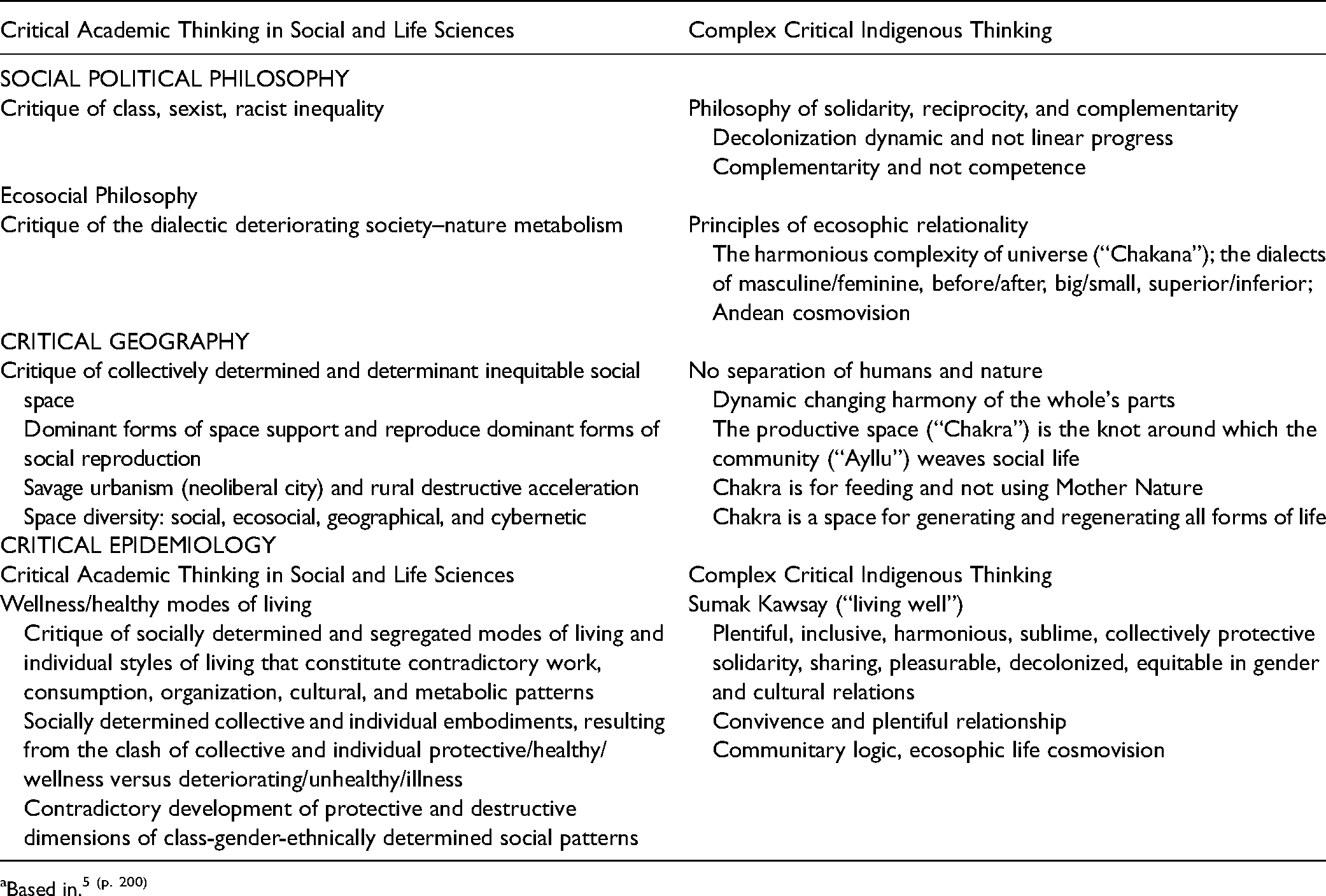
Based in. 5 (p. 200)
Again, for this complementarity not to end in subordination, it is important that praxis is formed by an equitable definition of problems and solutions among the social participants involved. It implies a non-elitist complementing of strengths and the mutual compensation of weaknesses in order to build concrete, territorialized actions in a social territory.
5
(p. 189)
Conclusion
Despite the fact that, today, the social determinants of health concept and the mainstream epidemiological tradition from which it emerges enjoy an increasingly hegemonic status within much of health professional education and research, Latin American collective health scholars have long developed alternative, complex, insightful conceptualizations of the relationship between “the social” (i.e., social organization, social processes, and social structures) and disease distribution. However, these perspectives have been largely excluded from academic, practitioner, and activist communities outside the region. In this article, we complicate perspectives on the social determinants of health among anglophone health professional audiences by drawing on the work of collective health scholars, with a focus on the work of Jaime Breilh. We explore specific critiques of the social determinants of health based on the social determination of health paradigm, including the concept of interculturality. More work is needed to disseminate Latin American social medicine and collective health perspectives,39,40 which are necessary for realizing health justice and global health equity. The work of Jaime Breilh and other collective health scholars calls for an “emancipatory social project, one that implies the construction of alternative power, and that must be articulated not only around academic or institutional efforts, […] but also around the vital processes of popular organizations and movements”. 10 (p. 32) By engaging directly and non-hierarchically with the profound vision of health equity articulated by the collective health movement, those fighting for health justice around the world can access invaluable tools to achieve their goals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fondo Nacional de Desarrollo Científico y Tecnológico, ANID, Chile, through the Fondecyt Regular Project 1210602, William T. Grant Scholar Award 2017-2022 and Clif Family Foundation, 2021-2022.