
Abstract
This article analyzes the relationship between various forms of intimate partner violence (IPV) and unmet need for family planning (FP) in South Asia. The data were obtained from the latest wave of the Demographic and Health Survey in Afghanistan, India, Maldives, Nepal, and Pakistan. Binary logistic regression analyses show mixed results, with a significant association between at least one type of IPV and unmet need for FP in all countries under study, except Maldives. There were also contrasting findings on the IPV–unmet need nexus, with a positive sign in some but negative sign in others. Women who experienced physical violence were associated with a higher odds of having an unmet need in Pakistan, but the opposite was true in Afghanistan and Nepal. The odds of having an unmet need were higher among Indian women who experienced IPV (sexual and emotional). In Afghanistan, women who experienced IPV (physical and emotional) have lower odds of having an unmet need. However, the interaction analysis of IPV (physical and sexual) and partners’ controlling behavior showed a positive association with unmet need. Policymakers need to develop policies and strategies to prevent IPV and reduce unmet need for FP, in line with the Sustainable Development Goals.
Keywords
Unmet need for family planning (FP) is defined as the proportion of women in the reproductive ages of 15–49 years, fecund and sexually active, who wish to stop or delay childbearing but are not using any contraceptive method. 1 The unmet need for FP remains one of the unfinished agendas of the Family Planning 2020 (FP2020) initiative, to reach an additional 120 million users of modern contraceptive methods by 2020 in the world's poorest countries. 2 Despite implementing the national FP program for more than half a century, some less developed countries, including those in South Asia, still have a low contraceptive prevalence rate (CPR) and a high unmet need for FP. In the 2010s, the CPR among South Asian countries ranged between 18.8 percent and 77.4 percent, and the levels were relatively lower than most developing countries in other Asian sub-regions. During the same period, the unmet need for FP among South Asian countries ranged between 5.7 percent and 31.4 percent, which was much higher than in other parts of Asia, where most of the countries have an unmet need of between 10 percent and 20 percent. 3 An estimated 218 million women aged 15–49 years have an unmet need for modern contraception in low- and middle-income countries. Of these, 148 million did not practice contraception, and 70 million used a traditional method in 2019. 4 Approximately 121 million unintended pregnancies occurred annually worldwide between 2015 and 2019, of which 61 percent ended in abortion. 5 These salient statistics indicate that more efforts and interventions are needed to achieve the Sustainable Development Goals (SDGs) target of “ensure healthy lives and promote well-being for all at all ages”, 6 particularly universal access to sexual and reproductive health care by 2030.
The CPR and unmet need for FP vary widely across the countries in South Asia. The level of contraceptive prevalence was as low as 18.8 percent in Maldives (2016–2017) and as high as 77.4 percent in Iran (2010–2011). In contrast, the level of unmet need for FP was the highest in the former (31.4%) and the lowest in the latter (5.7%). 3 With a share of nearly one-quarter of the world's population, 7 South Asia is home to about one-third of the world's extremely poor. 8 Low CPR and high unmet need for FP often result in high fertility and rapid population growth, 9 which lead to poverty in the less developed countries. 10 Rapid population growth in low-income countries, as in the case of South Asian countries, is detrimental to the country's development in the short and medium terms. 11 Moreover, high fertility strained the health care services and education provision and was found to have a negative impact on sustainable development in developing countries. 12
Past studies found that one of the reasons women did not use a contraceptive method was due to the opposition and the fear of violent reprisals from their partners.13,14 The theory of gender and power 15 elucidated the social structures that describe gendered relationships between men and women, including sexual division of labor, sexual division of power, and the structure of cathexis (social norms and affective attachments), all of which were fundamental in explaining gender roles in society. Specifically, gender differences in power resulted in physical and sexual violence against women, and women's sexual behavior was constrained by societal norms and expectations and distinguished by the emotional and sexual attachments that women have with men. 16 The traditional perception comprehended that a woman is possessed by the man and her role is to bear children. Women are also perceived as being morally and sexually weak and must thus be controlled by men. The social acceptance of violence against women as a justifiable means for a man to assert his position over the woman poses an impediment to the acceptance and use of contraception by women, even when they do not want to have more children. Studies showed that intimate partner violence (IPV)—behavior within an intimate relationship that causes physical, sexual, or psychological harm by partners—has brought about adverse sexual and reproductive health outcomes in women, such as the unmet need for contraception, unwanted pregnancies, induced abortion, low birth weight, non-use of contraception, and human immunodeficiency virus (HIV) infection.17–19
Women in developing countries generally suffered higher rates of IPV compared to women in developed countries. The World Health Organization reported that the prevalence of IPV ranged from 16.3 percent in East Asia to 65.6 percent in central Sub-Saharan Africa. 19 In Asia, the prevalence of IPV was the highest in South Asia, with a regional rate of 43 percent. 20 The latest wave of the Demographic and Health Survey (DHS) for Afghanistan, India, Maldives, Nepal, and Pakistan and the Bangladesh Violence Against Women Survey reported that the lifetime IPV among ever-partnered women among South Asian countries ranged between 16.3 percent and 54.2 percent, with the lowest in the Maldives, followed by Pakistan (24.5%), Nepal (25%), India (28.8%), Afghanistan (50.8%), and the highest in Bangladesh.21–26
The relationship between IPV and reproductive behavior is very complex and remains inconclusive. For instance, different forms of IPV may have a contrasting effect on contraceptive use. O’Hara, Tsai, Carlson and Haidar 27 discovered a negative association between severe physical IPV and contraceptive use and a positive association between severe sexual IPV and contraceptive use, but no association between emotional IPV and contraceptive use in Jordan. Several studies found that IPV was positively associated with unmet need,28–30 while others revealed a negative association 31 or no significant association. 32 These mixed findings show enormous uncertainty in the relationship between IPV and unmet need.
While there is a sizable literature on the association between IPV and contraceptive use, very few have examined the linkage between IPV and unmet need, especially among South Asian countries. Past research on the unmet need for FP in South Asia focused on the individual country in the region and were conducted two decades ago.33–35 This article aims to analyze the relationship between all three forms of IPV (i.e., physical, sexual, and emotional violence) and the unmet need for FP in selected South Asian countries that have conducted the DHS. It is hoped that the findings from this study can provide some insights for policymakers in strengthening the FP program to reduce the high unmet need for FP among specific population groups and subsequently accelerate the progress to eliminate the unmet need for FP, to accomplish the unfinished agenda of the 1994 International Conference on Population and Development adopted at the 2019 Nairobi Summit.
Data and Methods
Data Source
The data for this study were obtained from the latest wave of DHS conducted in South Asian countries, and these include Afghanistan (2015), India (2015–2016), Maldives (2016–2017), Nepal (2016), and Pakistan (2017–2018). Since this study focused on the association between IPV and unmet need, only DHS that incorporated the domestic violence module was considered, and therefore Bangladesh was excluded from this study. This article covered all women of reproductive ages (15–49 years) who were married or in union and answered the domestic violence module. The sample size for each country was 20,793 in Afghanistan, 58,480 in India, 2,765 in Maldives, 3,447 in Nepal, and 3,192 in Pakistan. Using a cross-sectional study design, socio-demographic and economic characteristics and experience of violence by intimate partners were collected in the survey. Questionnaires and interviewing procedures for standard DHS have been reviewed and approved by the Inner City Fund Institutional Review Board. Permission to use the data was obtained from the DHS Program. The detailed explanation of the sampling frame and design can be found in the DHS published reports.
Study Variables
The dependent variable for this study—the unmet need for FP—was a binary variable coded as “yes” if women have an unmet need for limiting or spacing and “no” otherwise. The main independent variables include the three dichotomous variables measuring the experience of physical violence, sexual violence, and emotional violence in the past 12 months. Other socio-demographic and economic variables such as women's age, age at first marriage, place of residence, educational level, work status, number of living children, household wealth, exposure to FP via mass media, and controlling behavior by partners were also included in the study. Mass media exposure to FP measured women's exposure to FP messages on the radio, television, and in the newspaper or magazine in the past few months. Women who reported having been exposed to at least one of the media were deemed to have exposure to FP messages. Controlling behavior displayed by partners was measured through five questions. Women were asked if their partners: (a) were jealous if they talked to other men, (b) frequently accused them of being unfaithful, (c) did not permit them to meet female friends, (d) tried to limit their contact with family members, and (e) insisted on knowing where they were at all times. Women who reported experiencing any of the above were considered to be facing controlling behavior by partners.
Data Analysis
All analyses were performed using SPSS version 25. All data were weighted prior to performing the analyses to ensure each sample data was representative of the entire population. Descriptive analysis was performed to examine the distribution of all the variables. Bivariate analysis was carried out to examine the relationship between the dependent variable and each independent variable. The Chi-square test (or Fisher's exact test for 2*2 contingency table) was used to measure the significance of bivariate association between two categorical variables. Binary logistic regression was used to determine the net effect of IPV on the dependent variable, controlling for other independent variables. The magnitude and direction of the association between IPV and unmet need may vary by different types of violence. Thus, the effect of each type of IPV on the dependent variable was analyzed separately in three binary logistic regression models. Clark and colleagues 29 proposed that a partner's close control over the wife should be included as a correlate of IPV and a factor that may affect women's ability to meet their contraceptive needs. 29 Furthermore, a past study in India reported that women who experienced IPV and whose partners had controlling and domineering attitudes were less likely to use modern contraception. 36 Therefore, this study tested for the significance of the interaction term between each type of IPV and controlling behavior (IPV × control) in binary logistic regression models. A p-value of less than 0.05 was considered to be statistically significant.
Results
Table 1 shows the levels of CPR, unmet need for FP, and IPV in selected South Asian countries. India recorded the highest CPR of 55.1 percent and the lowest total unmet need of 12.7 percent, whereas Maldives had the lowest CPR of 20.2 percent and the highest total unmet need of 32.5 percent. The CPRs in Afghanistan, Nepal, and Pakistan were 22.8 percent, 52.6 percent, and 34.9 percent, with a corresponding total unmet need of 23.6 percent, 23.8 percent, and 17.1 percent, respectively. All three types of IPV were found to be the lowest in Maldives (physical: 4.9%; sexual: 0.5%; emotional: 6.5%) and the highest in Afghanistan (physical: 45.9%; sexual: 6.1%; emotional: 34.4%).
Levels of CPR, Unmet Need for FP, and various Types of IPV.

Table 2 presents the bivariate analysis of the prevalence of unmet need for FP by type of violence and selected socio-demographic and economic variables. The percentage of married women who experienced IPV in the past 12 months having an unmet need for contraception ranged from 12.8 percent in India to 40.4 percent in Maldives. In each country, at least one form of IPV was significantly associated with unmet need for FP. Women who experienced any form of violence reported a higher prevalence of unmet need for FP compared to those who did not experience violence in the past 12 months. However, this is not the case in Afghanistan and Nepal, where Afghan women who experienced physical and emotional violence and Nepalese women who experienced physical violence had a lower unmet need for FP. For each type of violence experienced by the women, Maldives reported the highest prevalence of unmet need for FP across countries, while India had the lowest unmet need for FP. Married women who experienced controlling behavior from their partners tend to have a higher unmet need for FP than those without such experience in India, but the contrary was observed in Afghanistan.
Prevalence of Unmet Need for FP by Selected Variables.
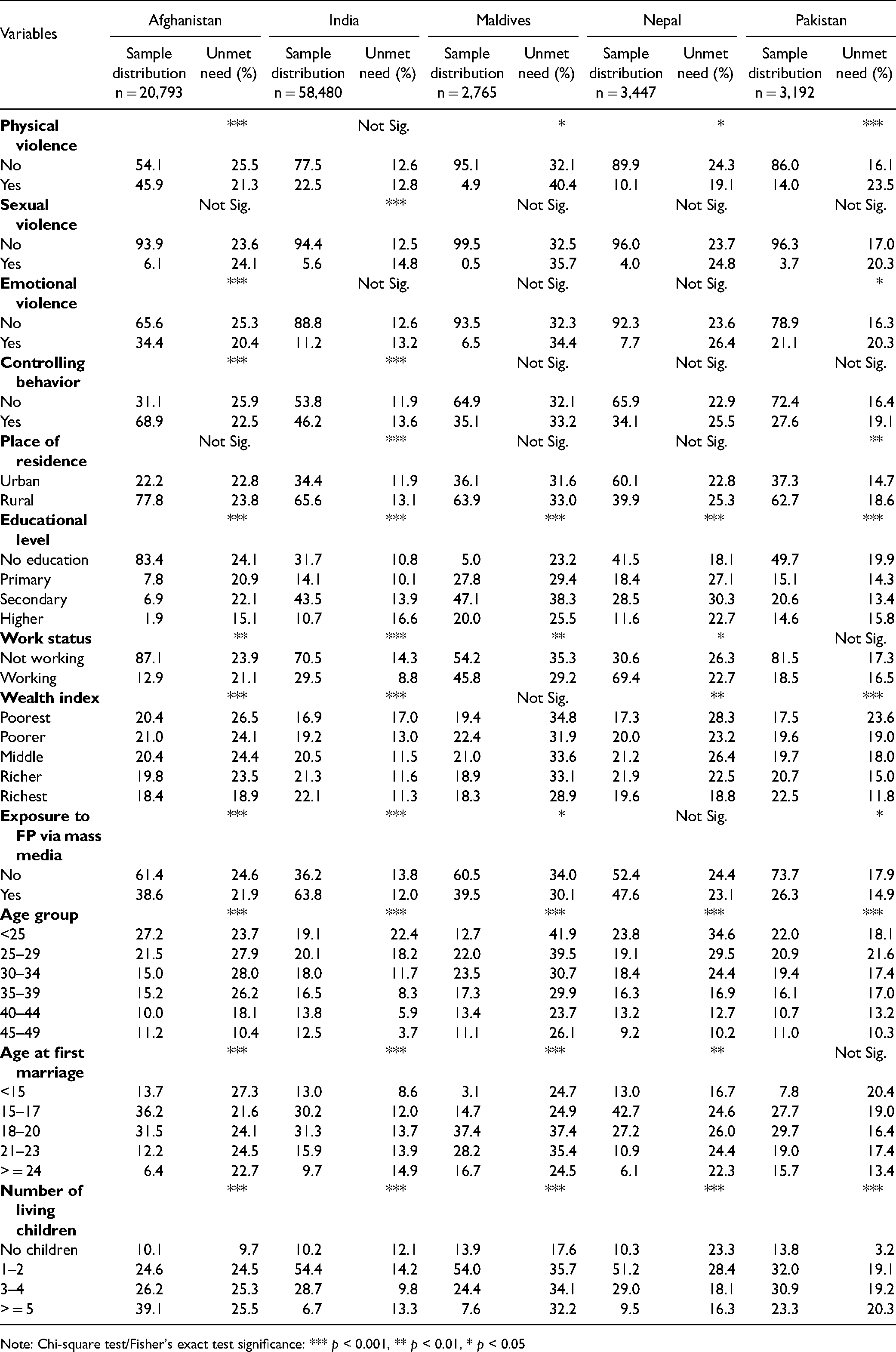
Note: Chi-square test/Fisher's exact test significance: *** p < 0.001, ** p < 0.01, * p < 0.05
Urban residence, current work status, and exposure to FP messages were significantly associated with a lower prevalence of unmet need for FP, with few exceptions (see Table 2). Unmet need decreased with women's educational level in Afghanistan and Pakistan, but the opposite was true in India, Maldives, and Nepal. Unmet need decreased significantly with household wealth, except in Maldives. Young married women generally experienced a higher level of unmet need compared to older women in all the countries. The prevalence of unmet need for FP increased with age at first marriage in India and Nepal, but the reverse was true in Afghanistan. The unmet need for FP among women with at least one child was significantly higher than those who were childless in Afghanistan, Maldives, and Pakistan, but it decreased with the number of living children in Nepal.
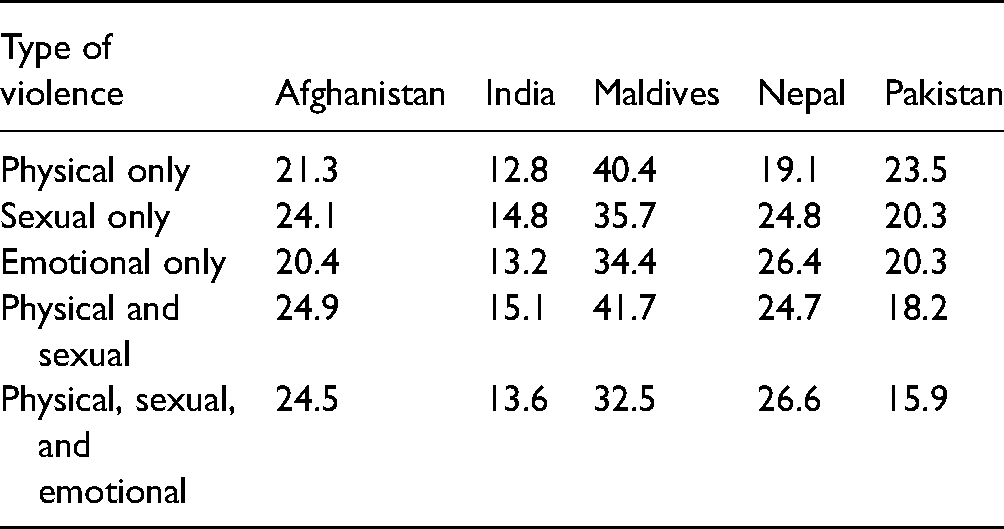
Table 3 shows the prevalence of unmet need for contraception by combination type of IPV. Women who experienced more than one type of violence reported a higher level of unmet need than those who experienced only one type of violence, as observed in Afghanistan, but the opposite was true in Pakistan. In India and Maldives, women who experienced both physical and sexual violence were more likely to have higher unmet need than those who reported only one type of violence. Nepalese women who experienced all three types of violence had a higher unmet need for FP compared to those who experienced any single type of violence.
Prevalence of Unmet Need for FP by Combination Type of IPV.
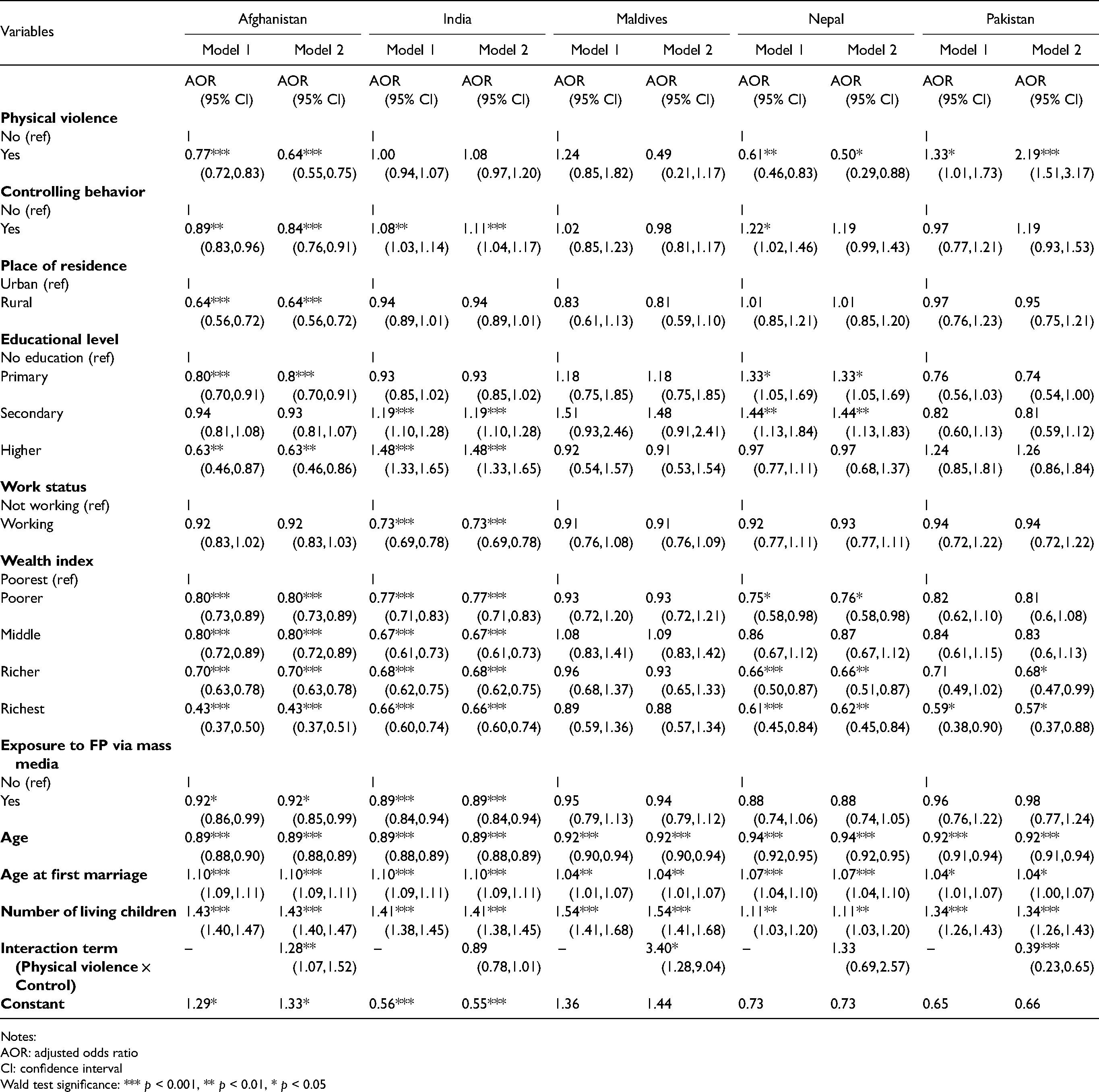
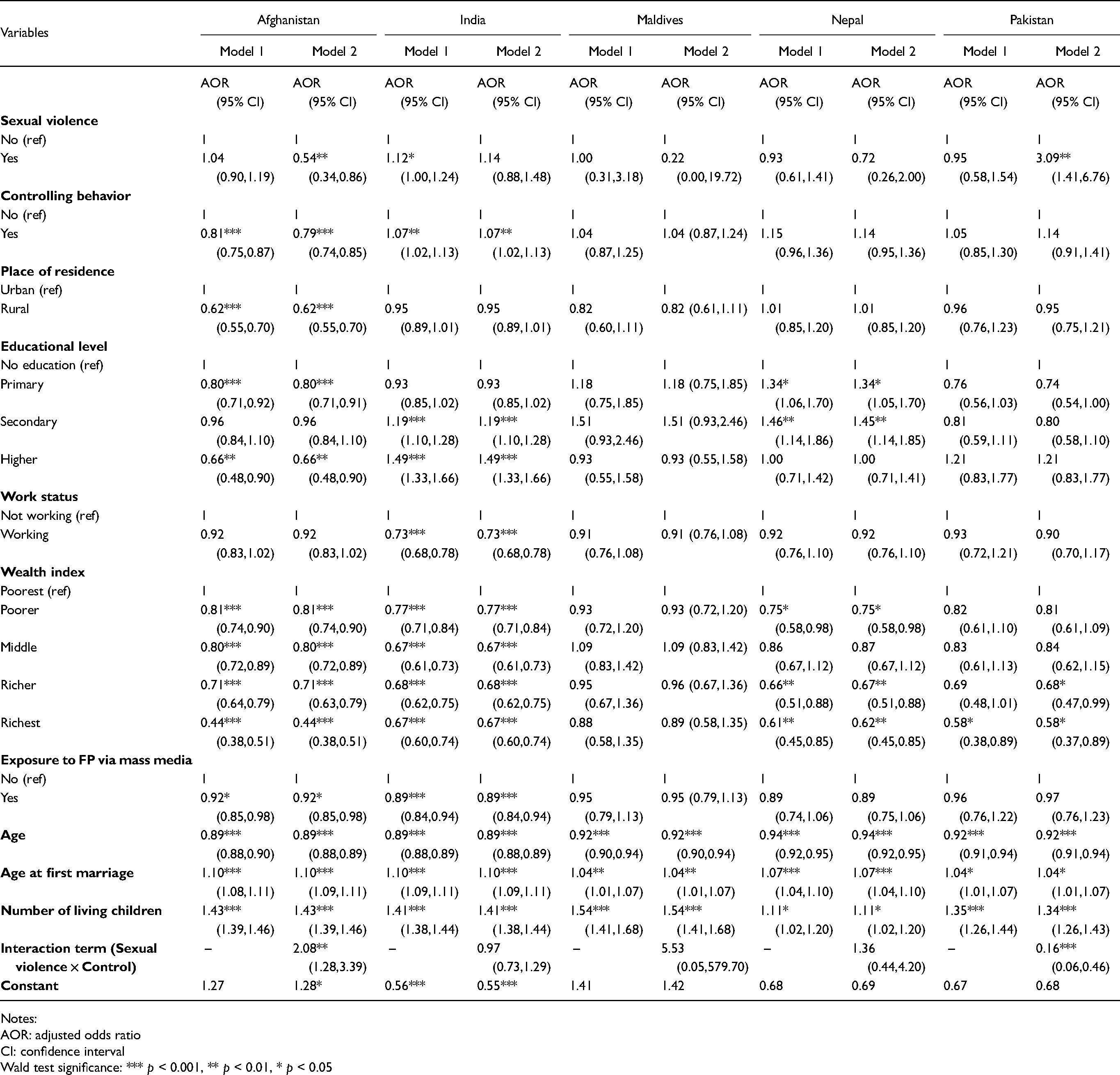
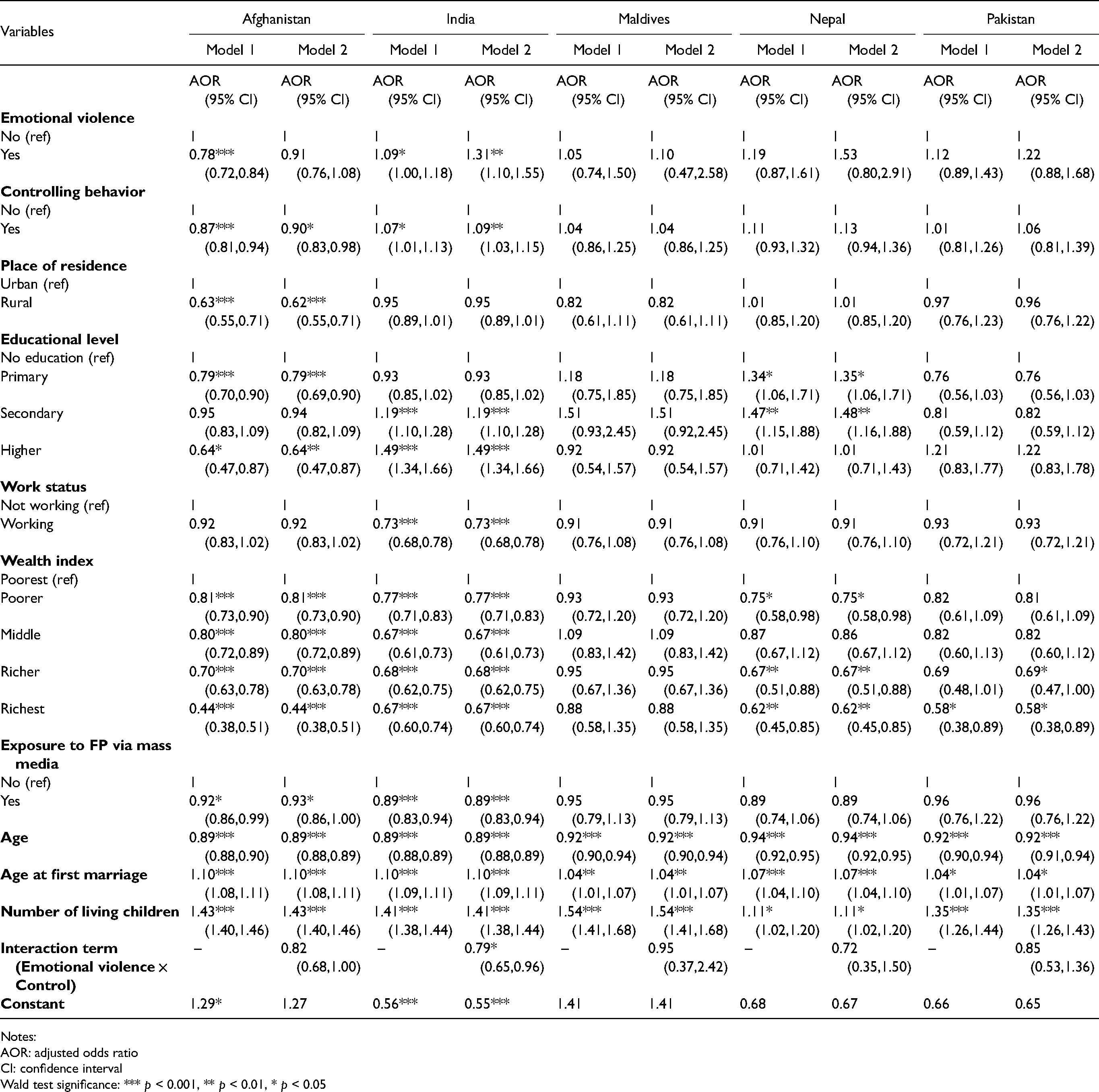
Tables 4, 5, and 6 present the binary logistic regression analyses of the unmet need for contraception among married women aged 15–49 years, using physical, sexual, and emotional violence as main independent variables separately, controlling for socio-demographic and economic variables in Model 1. The magnitude and direction of association between unmet need and socio-demographic and economic variables were similar in all three binary logistic regression models, but it is not the case for different types of IPV. Women who experienced physical violence have lower odds of having an unmet need for FP in Afghanistan (AOR = 0.77) and Nepal (AOR = 0.61), but were found to have higher odds of having an unmet need in Pakistan (AOR = 1.33). Higher odds of having an unmet need were found among women who experienced sexual violence and emotional violence in India, with an AOR of 1.12 and 1.09, respectively. However, Afghan women who experienced emotional violence have lower odds of having an unmet need for FP (AOR = 0.78). All three binary logistic regression models show that women who reported controlling behavior by partners were associated with lower odds of having an unmet need in Afghanistan, but higher odds of having an unmet need in India.
Binary Logistic Regression of Unmet Need for FP (Physical Violence as the Main Independent Variable).
Notes:
AOR: adjusted odds ratio
CI: confidence interval
Wald test significance: *** p < 0.001, ** p < 0.01, * p < 0.05
Binary Logistic Regression of Unmet Need for FP (Sexual Violence as the Main Independent Variable).
Notes:
AOR: adjusted odds ratio
CI: confidence interval
Wald test significance: *** p < 0.001, ** p < 0.01, * p < 0.05
Binary Logistic Regression of Unmet Need for FP (Emotional Violence as the Main Independent Variable).
Notes:
AOR: adjusted odds ratio
CI: confidence interval
Wald test significance: *** p < 0.001, ** p < 0.01, * p < 0.05
Rural residence was associated with lower odds of having an unmet need for FP in Afghanistan. Better-educated women reported lower odds of having an unmet need compared to those with no formal education in Afghanistan, but the reverse was true in India and Nepal. Lower odds of having an unmet need for contraception was observed among working women in India. The odds of having an unmet need for contraception decreased with family wealth across countries, except in Maldives. Women who were exposed to FP information through mass media have lower odds of having an unmet need for contraception in Afghanistan and India.
In all five countries, the odds of having an unmet need for contraception decreased with age but increased with age at marriage and the number of living children. Nevertheless, the magnitude of age at marriage effect on unmet need for contraception differed slightly across countries, in which the effect was larger in Afghanistan and India, but smaller in Maldives and Pakistan. The number of living children had the largest positive effect on unmet need for contraception in Maldives, and the smallest effect was observed in Nepal.
Turning now to the interaction analysis, Model 2 shows the correlates of unmet need for FP with an interaction term between each type of IPV and partners’ controlling behavior (see Tables 4–6). After adjusting for socio-demographic and economic variables, women who experienced IPV (physical and sexual) and partners’ controlling behavior have higher odds of having an unmet need for FP than those who did not experience IPV and controlling behavior by their partners in Afghanistan, but the opposite was true in Pakistan. Maldivian women who reported physical violence and controlling behavior by partners were associated with higher odds of having an unmet need. On the contrary, Indian women who experienced emotional violence and controlling behavior by partners have lower odds of having an unmet need compared to their counterparts.
Discussion
The unmet need for FP has a severe impact on women's lives. Unintended pregnancy was significantly higher among women with unmet need for contraception, 37 and this worldwide public health concern imposes a great burden on economic development. 38 Hence, it is of paramount importance to reduce and subsequently eliminate the unmet need for FP for the benefit of both women and society.
The key findings from this study concerned the differing effects of physical, sexual, and emotional violence experienced in the past 12 months on the unmet need for FP among married women across South Asian countries. In the multivariate analysis, women who reported experiencing physical violence were more likely to have unmet need in Pakistan, but the opposite was true in Afghanistan and Nepal. On the other hand, women who reported experiencing sexual violence have a higher level of unmet need in India. The level of unmet need among women experiencing emotional violence was higher in India, but lower in Afghanistan, after controlling for other socio-demographic and economic variables. This study also reveals that controlling behavior by partners was negatively associated with unmet need in Afghanistan, but positively associated with unmet need in India. IPV and controlling behavior may disempower women and affect women's autonomy over FP decisions, 39 which explains the higher level of unmet need for FP among those who experienced IPV in India and Pakistan.
Contrary to the findings of the main effects, the interaction analysis of IPV and partners’ controlling behavior shows a positive association with unmet need in Afghanistan and Maldives. Under the patriarchal culture (as in South Asia), men perceived themselves as justified in using violence to maintain control over women. 40 Paul and Mondal 36 suggested that women who experience IPV and domineering attitudes by partners may encounter greater difficulties in using a contraceptive method to achieve their fertility goals. 36 This analysis implies a higher unmet need for FP under the influence of IPV and partners’ controlling behavior.
Apart from the effects of IPV and controlling behavior, this study also highlights the importance of socio-economic variables in explaining the differentials in the unmet need for FP, especially the effects of women's education, employment, family wealth, and exposure to FP via mass media. The level of unmet need for FP was much lower among better-educated women in Afghanistan. Education not only provides a platform for women to exchange the latest information on FP matters, 41 but also empowers them to be the main decision-maker in childbirth-related matters, 42 which results in higher contraceptive use and lower unmet need for FP among better-educated women. The negative association between unmet need for FP and women's education was well-established in past literatures.35,41–44 However, this study reveals that better-educated women in India and Nepal have a higher unmet need for FP. The positive association between women's education and unmet need may be partly explained by ethnic and caste diversity, especially in the highly diverse Indian population. Nevertheless, different ethnic classifications were used in the DHS conducted across South Asian countries. For instance, “caste” was asked in India DHS while “ethnicity” was used in Nepal DHS. Hence, the ethnic/caste variable is excluded from this study for standardization purposes. Further research is needed to understand the complex relationship between women's education and unmet need in these countries, using the mixed-method approach.
Working women were less likely to have an unmet need for FP in India. This result corroborates with findings from Singh and colleagues. 45 Working women are generally more financially independent and have more control over contraceptive decisions. In some cases, pregnant working women may encounter workplace discrimination, 46 and therefore they tend to use contraception to control pregnancy, and subsequently, the lower unmet need for FP.
Evidence from this study suggests that family wealth was negatively associated with unmet need in all countries under study except Maldives. Unlike women from impoverished families, women from better-off families have fewer financial constraints in obtaining FP information and services. 47 These women are usually more educated and knowledgeable about FP methods, contributing to the lower unmet need for FP. This study also reveals that exposure to FP via mass media led to a lower unmet need in Afghanistan and India. FP advertisement through mass media contributed to raising women's knowledge of FP and creating awareness of the importance of FP to maternal and child health. 48 Frequent exposure to mass media will gradually change the cultural mindsets toward accepting FP, especially in rural areas. 49 Women can obtain the latest information on FP through mass media and thus are less likely to have an unmet need for contraception.
This study raises important implications. Good health, well-being, and gender equality are the vital SDGs to be achieved by 2030. Preventing IPV could reduce the unmet need for contraception, especially in Pakistan and India. Hence, ending IPV in South Asia—the region with the highest regional rate of IPV in Asia—demands immediate attention to “kill two birds with one stone.” Empowerment and participatory approaches such as microfinance programs with gender-equality training and the Stepping Stones training program (a training package on gender, HIV, communication, and relationship skills) were found to be effective in reducing gender inequality and preventing IPV in South Africa. 50 The Stepping Stones training program was adapted for use in India, but this program warrants recognition and support from the government authorities. Other South Asian countries may adapt this program for use in each country, and cross-country collaboration should be facilitated in accelerating the realization of “zero unmet need for contraception by 2030,” as set by the United Nations Population Fund.
It is worth noting that every six in 10 Afghan women have no exposure to mass media on FP. The government should fortify the FP program and organize campaigns regularly via mass and social media to raise public awareness concerning the importance of contraception in planned parenthood. In the past few decades, mass media campaigns were proven successful in promoting FP and changing contraceptive behavior in Bangladesh 51 and Nepal. 52 Hence, improving women's exposure to FP information via mass media can go a long way in lowering the unmet need for contraception. Furthermore, these advertisements could also incorporate information promoting positive gender roles, in the hopes of preventing gender-based violence.
It is essential to design and customize specific FP strategies and programs to target the poor, unemployed, and lesser-educated in reducing the high unmet need for FP among these marginalized groups. A comparison of the strength of FP programs in 63 developing countries, including Bangladesh and Pakistan, by Bongaarts 53 disclosed that a strong FP program with information, education, and communication components could increase contraceptive use and reduce unmet need. A recent study on fertility differentials in Bangladesh and Pakistan also reaffirmed the important role of FP program in explaining CPR differences between these two countries. 54 Hence, a strong program with support from the government, including large-scale, community-based contraceptive distribution and low-cost contraceptive services to disadvantaged groups, can eliminate socio-economic barriers to contraceptive uptake. A community-based approach could be an effective strategy in implementing community-based health educational intervention designed to reduce gender-based violence and unmet need for FP. A health educational intervention in Sri Lanka showed significant results in improving knowledge and attitudes on FP and reducing the unmet need for modern contraceptive methods. 55 Sri Lanka's case could serve as a model for other South Asian countries in designing health policies.
Limitations
The unmet need for FP is influenced by both demand and supply factors. The DHS data excluded information on the supply factors, such as the quality of the FP services. Hence, this study analyzed only the demand factors. The unmet need for FP in this analysis was the sum of unmet need for limiting and unmet need for spacing, and these were not analyzed separately due to the cross-country nature of this study.
Conclusion
South Asian countries have grappled with rapid population growth through various means for more than half a century. Despite that, FP programs in South Asian countries often encounter challenges in raising contraceptive use and reducing the unmet need for contraception. These programs achieved remarkable results in most South Asian countries until the 1990s, but progress has remained stagnant since then. This study found a significant association between IPV and the unmet need for contraception. There is a need for policymakers to develop policies and strategies to prevent gender-based violence and improve women's socioeconomic status, which in turn will empower women and reduce the unmet need for contraception.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.