
Abstract
Introduction
Depending on the age groups and definitions used, there are between 10 and 100 million street children and young people worldwide, most of them in low- and middle-income countries (Lieb et al., 2007).
High levels of urban violence have been considered a public health problem in Latin American societies (Briceño-Leon, 2005). In these environments, street children and youth are particularly vulnerable to violence and exploitation (Tyler and Beal, 2010). Although treatment centres and residential protective facilities for children and youth not wanting to return home are available, the process of therapeutic engagement is difficult as street children and youth have usually escaped abusive home environments and have difficulties engaging with the health professionals who try to help them.
Substance abuse and mental and physical health problems among street children and youth are substantial problems and the provision of medical and mental healthcare presents challenges to organizations working with this population (Souza and de Leon, 2007)
While treatment models focusing on mental health and substance abuse have been developed (Slesnick et al., 2007; Slesnick et al., 2008b; Slesnick and Prestopnik, 2005; Souza and de Leon, 2007; Waldron et al., 2001), descriptions of the implementation of these services and their outcomes for street children and youth in low-income countries remain rare.
This study describes the uptake and outcomes of a multidisciplinary case management approach for street children and youth attending a drop-in day care centre in Tegucigalpa, Honduras. The programme was implemented by Médecins Sans Frontières (MSF), an international, humanitarian, medical non-governmental organization (NGO). This paper describes the outcomes of psychological distress, substance abuse and the social situation of children and youth participating in centre activities and identifies how levels of psychological distress and substance abuse changed over time.
Methods
Setting
Honduras is a lower middle-income country located in Central America, with an estimated population of 7.5 million, half of whom are under the age of 19. Approximately 44% of Hondurans live on less than 2 dollars a day (Jacobi et al., 2002). Honduras is one of the most violent countries in Latin America and Tegucigalpa, a city with a population of approximately 1.25 million, has a homicide rate of 51 homicides per 100,000 inhabitants (Lieb et al., 2002). Although poorly documented, it is estimated that approximately 1,500 street children and youth under the age of 23 have been murdered in Honduras from 1998 to 2002 (Bott et al., 2005).
Sample
The study sample included children and youth who spent most of their day on the street, were under 25 years old at admission and were accepted to be registered in the centre. All visits to all centre services were recorded. A total of 800 individuals entered the centre between March 2005 and January 2009. This study describes the characteristics of the 400 individuals followed by the multidisciplinary care approach, which included at least two consultations with the mental health team where outcome measures were collected, who had agreed to participate.
Design
A longitudinal observational study based on routinely collected data was conducted.
The intervention
The centre served on average 30–40 children and youth each day, with opening hours from 10.00 am to 2.00 pm. Access to laundry, showers, recreation and a place to rest was offered. In general, children and youth approached the centre either through information provided by other centre attendees or through community outreach by centre staff. Street children and youth coming to the centre were registered and invited to deposit their belongings in a safe place inside the centre.
The different members of the team progressively performed individual assessments and prepared the case for a multidisciplinary discussion to be performed within one month of registration. During the discussion, an individualized therapeutic plan was designed and offered to the individual on his or her next attendance at the centre. Street children and youth were invited to comment on the treatment plan and make suggestions for improvement. A final therapeutic plan was designed and verbal consent on the treatment plan was obtained.
The therapeutic plan strategy had four main components (Figure I):
Mental health strategy. Trained clinical psychologists employed an adaptation of the community reinforcement approach (CRA) (Meyers and Miller, 2001). The CRA addresses the clinical needs of homeless individuals, including substance use, homelessness and mental health problems, using an operant perspective based on the assumption that environmental contingencies play a powerful role in behaviour change. CRA procedures overlap considerably with other cognitive–behavioural intervention models and have been successfully used with housed adolescents and homeless youth (Slesnick et al., 2007). Identification and referral of cases of severe mental illness to psychiatric facilities where psychopharmacological treatment was available was also part of the strategy.
Medical strategy. Health education sessions targeting the most common diseases among street children and youth were regularly performed. Primary care medical consultations and a basic package of reproductive healthcare was also available.
Social care strategy. Social workers developed a complete mapping of services available for street children and youth in Tegucigalpa. Each beneficiary was offered services depending on their motivation and interest.
Educational strategy. A team of educators coordinated all street outreach activities, recreational activities inside the centre and defaulter tracing for children and youth who did not attend the centre as planned according to their individual therapeutic plan.
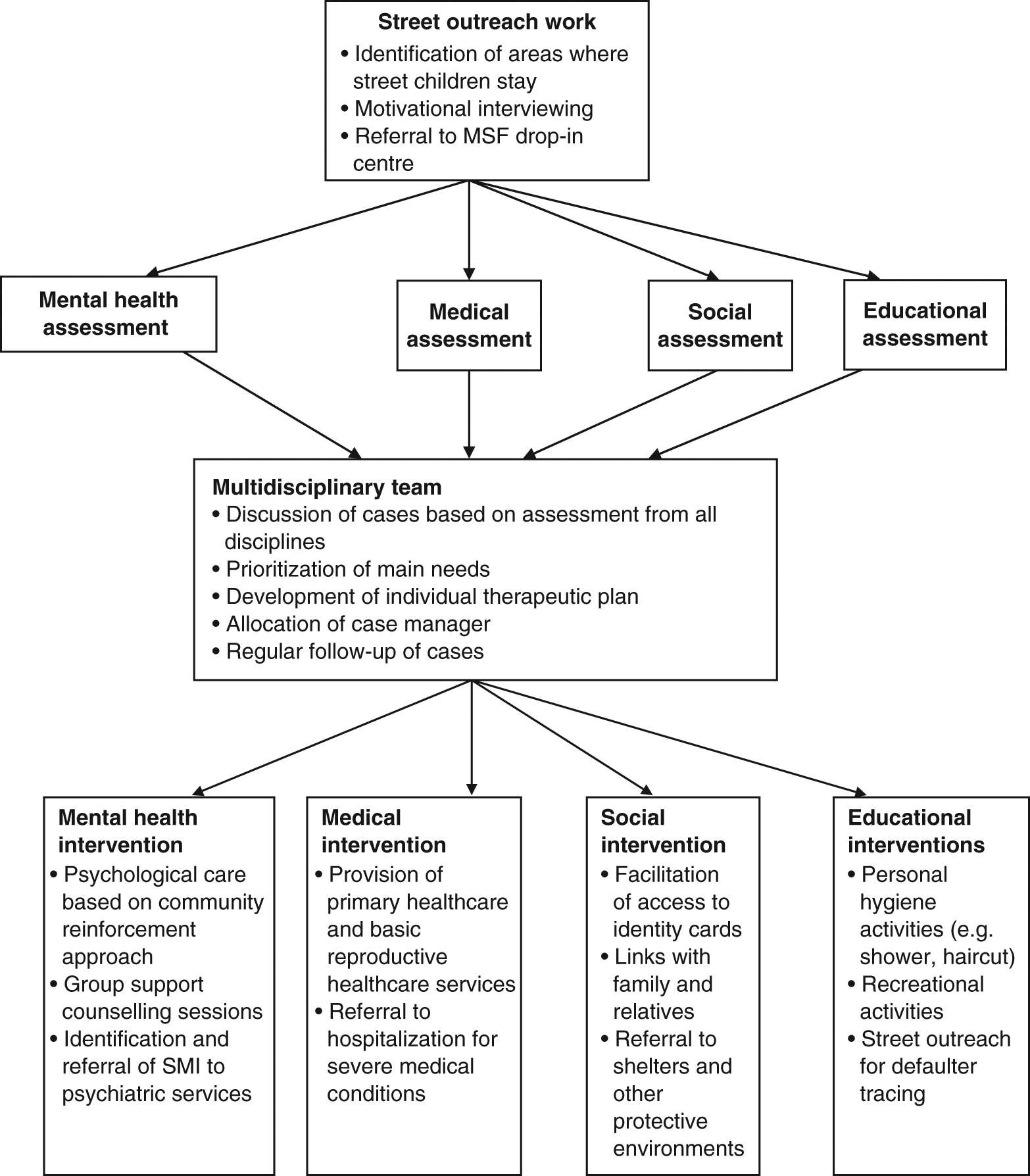
The structure of the street children and youth drop-in centre
One member of the team was appointed as a case manager and was responsible for coordinate access to services according to the treatment plan, including facilitating access and ensuring the delivery of those services inside and outside the centre.
Data collection
In the case files for the mental health consultations, a standardized questionnaire was integrated and completed at each visit. The questionnaire concerned sociodemographic characteristics, substance consumption levels, psychological symptoms of distress and sleeping arrangements in the week prior to the consultation. Verbal consent (in view of the very low literacy rates in this population) was obtained routinely at mental health consultations from each individual. Consent from parents or relatives was not asked as most children and youth did not want the centre to contact their families.
All data were collected by trained Spanish-speaking clinical psychologists. Permission to publish the findings was granted by the ethical review board of Médecins Sans Frontières.
Outcome measurements
The Teen Addiction Severity Index (T-ASI) is a semi-structured interview developed to evaluate the severity of adolescent chemical abuse, related problems and objective treatment outcome and follow-up (Kaminer, 2008). Studies have shown it to have good psychometric properties and satisfactory inter-rater reliability among adolescent substance abusers as well as the ability to describe changes over time according to its subscales (Brodey et al., 2008; Diaz et al., 2008; Sartes et al., 2009; Zanis et al., 1994). The T-ASI is the recommended instrument to periodically assess changes in response to treatment for adolescents in substance abuse treatment programmes (Kaminer, 2008). A Spanish version of the index was developed using standard translation and back-translation methods (Maneesriwongul and Dixon, 2004).
The following scores were extracted from the subscales, referring to the last 7 days before each consultation.
Psychological distress score: the number of symptoms was summed from a maximum of nine symptoms of psychological distress reported by the patient.
Substance use levels score: this describes the number of days without any substance use in the previous week.
Social situation: sleeping arrangements of children and youth were recorded and a graded scale was created with different sleeping arrangements reflecting different levels of security on the street. Five categories reflecting the progression to more protective environments were identified: (1) sleeping alone in the street; (2) sleeping on the street with other persons; (3) sleeping in a hotel room; (4) sleeping in a supportive institution; and (5) sleeping in an apartment or house with parents or family.
Other baseline and follow-up measures
At entry, baseline sociodemographic information was collected. During follow-up, information was collected about attendance to medical and social services consultations, group activities, and antenatal and family planning consultations. Medical and psychological consultations after violent events were also recorded, as was post-mortum information in the event of death.
Statistical analysis
The difference between the first and last patient visit for the three outcome measures was assessed using the Wilcoxon sign rank test.
Data on psychological symptoms score were analyzed using linear mixed effects (LME) regression models (Cudeck and Klebe, 2002). LME models the process of change in the studied population as well as at the individual level, while accounting for the correlation of observations within individuals and the imbalance in the number of observations per individual (Cudeck and Klebe, 2002; Laird and Ware, 1982; Raudenbush and Bryk, 2002). In the analysis, models were built sequentially, starting with a model assuming no trend either at the individual or population level, to a model containing both individual and population trends. The significance of adding extra terms to the model was assessed using the likelihood-ratio test. Subsequently, alternative models for trend were sought for the population and for individuals by including quadratic and cubic terms for time. Finally, analyses were performed to assess if the overall population trend across age group and gender were equivalent.
Substance use scores were reclassified into a dichotomous variable depending on drug use in the week prior to consultation. Since patients tended to fluctuate between stopping for one week and restarting drug use, for the survival analysis, a patient was classified as a failure if he had stopped substance use for more than 50% of the remaining follow up visits. Kaplan Meyer curves were built and the probability of remaining on substances at different time points calculated.
Results
Children and youth attending the centre
The baseline characteristics of children and youth who attended the centre between its opening in March 2005 and January 2009 were collated (Table I).
Patient characteristics at the MSF Tegucigalpa street children and youth project. January 2009, Honduras
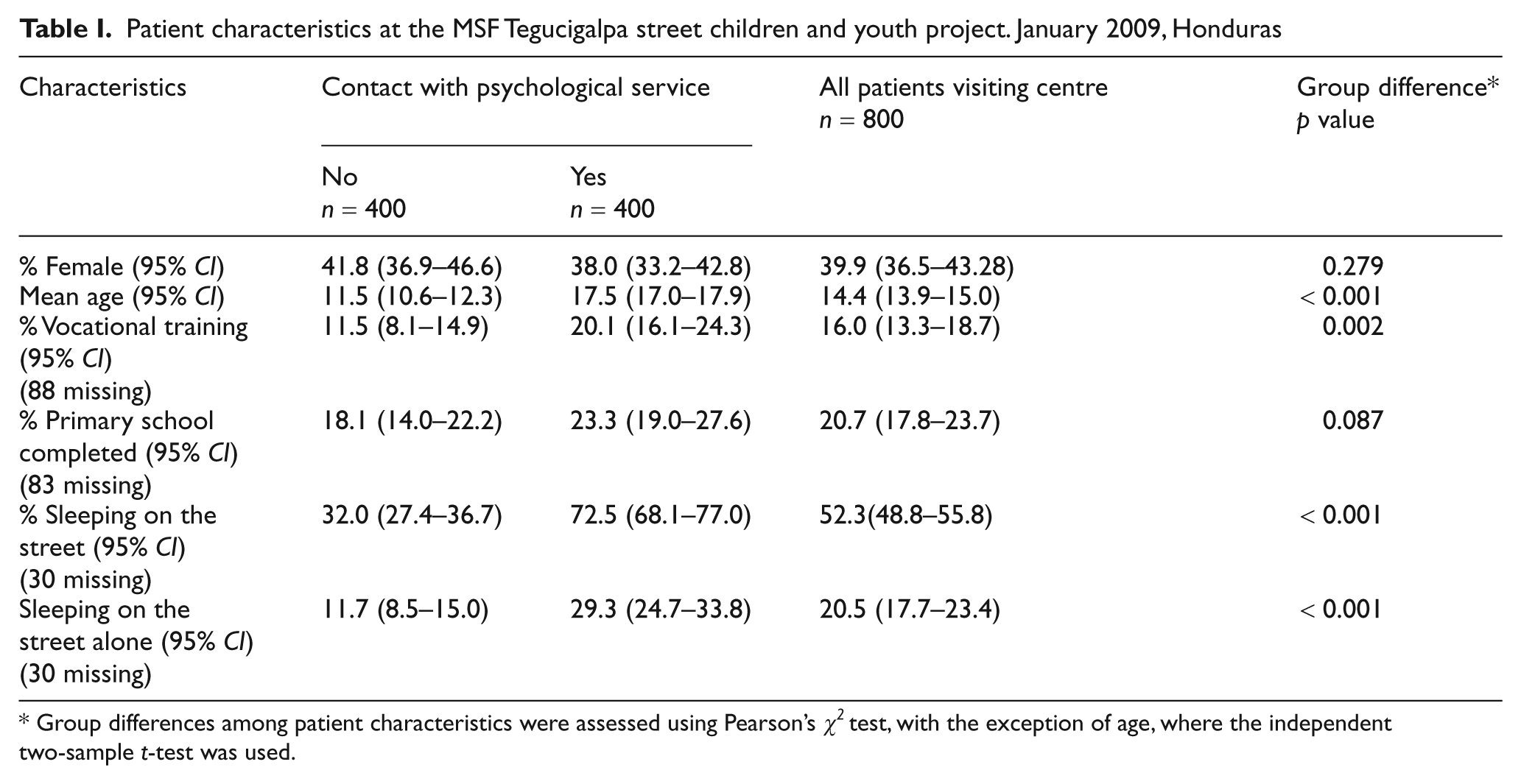
Group differences among patient characteristics were assessed using Pearson’s χ2 test, with the exception of age, where the independent two-sample t-test was used.
A total of 770 individuals provided information on sleeping situation. Of those sleeping on the street, most reported sleeping alone; 107 (13.9%) slept in small shelters rented on a daily basis; 39 (5.1%) spent their nights in institutions; and 221 (28.7%) spent the night in apartments or houses.
The median number of medical consultations attended was four (IQR 1-10) and the median number of social worker visits was two (IQR 1-8). Individuals attended a median of six group activities (IQR 2-29).
Out of 209 women, 84 (42%) attended antenatal visits and 97 (52%) came for family planning consultations with a median number of four visits (IQR 2-6).
Two hundred and thirty seven (237) (29.6%) individuals came to the centre to attend a medical or psychological consultation after being a victim of violence; this included 182 individuals (78%) who were sleeping on the street. The median number of visits per person after a violent event was two (IQR 1-3). A total of 32 (4%) individuals ever to have entered the centre are known to have died.
Multidisciplinary care
Of the 400 individuals attending multidisciplinary activities, 115 (28%) came to a single mental health consultation and 285 (71%) came to two or more sessions, making a total of 3,716 visits. The mean number of mental health consultations attended was 9.3 visits, with a median of three (IQR1-10). The mean time between the first and the last consultation was 18 months (95% CI: 16.4–19.6).
Description of mental health situation at first visit
At first visit, 219 (54.8%) individuals reported feeling depressed and hopeless, 312 (78%) reported anxiety and tension, and 184 (46%) reported to have little or no interest. Approximately one quarter, 110 (25.3%) reported having trouble controlling violent behaviour. Twenty four (24, 6%) reported having suicidal ideas and 5 (1%) reported having made a suicide attempt in the month prior to the first consultation. Of the 386 (96.5%) who provided information on substance use in the week prior to first visit, 275 (71.2%) had taken substances on every day of the week.
Changes in psychological, substance abuse and social situation scores
There was a reduction in symptoms in the psychological score between the first and last visit. Similarly, there was an increase in days without substance use and an improvement in sleeping arrangements (Table II).
Wilcoxon sign rank test for changes on psychological symptoms, substance use and social situation scores

The model of the psychological symptom scores showed that over time, the overall and individual trends were non-linear. There was no main effect of age or interaction of age over time, but there was a significant main effect of gender and a significant interaction of gender over time. The estimated reduction in scores per year was −0.45 (95% CI: 0.23–0.67) for males and −1.00 for female patients (95% CI: 0.76–1.24) (Table III).
Changes in average psychological symptoms score over time by gender, obtained from linear mixed effects model
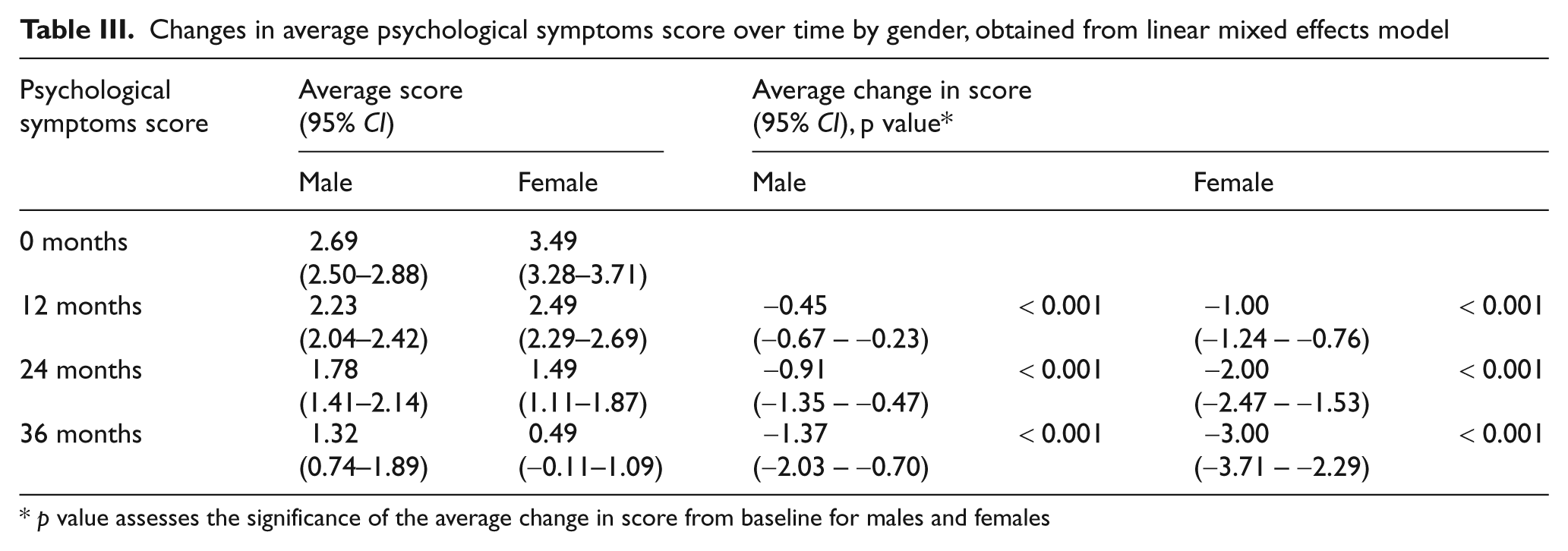
p value assesses the significance of the average change in score from baseline for males and females
Of the 236 patients who had baseline and follow-up visits, 114 (48%) reported using substances consistently throughout both periods, and 19 (8%) reported never to have used substances; 78 (33%) intermittently took substances during follow-up and 19 stopped substance use (8%). A further six (3%), who reported no substance taking at baseline, started taking substances during follow-up.
The median time from first mental health visit to first reporting of no substance use in the last week was 11 months. The median number of months between consecutive visits where no substance taking was reported was 0.4.
Survival analysis was used to investigate time to first reporting no substance use in the last week. Taking the first visit with no substance use, the probability of remaining on substances at 12 months was 0.76 (95% CI: 0.69–0.81) and 0.51 (95% CI: 0.42–0.59) at 24 months. At 12 months, significantly fewer female patients remained using substances compared to male (logrank test: χ2 = 17.1, df = 1, p < 0.01).
Using the 50% or more of the follow-up visits rule to define “stopped substances of abuse”, 31 of the 87 patients (36%) stopped. The median time to stop was 6.6 months.
Under this rule, the probability of remaining on substances was 0.88 (95% CI: 0.82–0.92) at 12 months and 0.82 (95% CI: 0.75–0.87) at 24 months (Table IV). There was no difference in survival between males and females (logrank test: χ2 = 1.4, df = 1, p = 0.24. Kaplan-Meier curves were built to illustrate these results (Figure II).
Probability of continued substance use (95% CI). ‘Stop’ defined as more than 50% of follow-up visits without substance use*
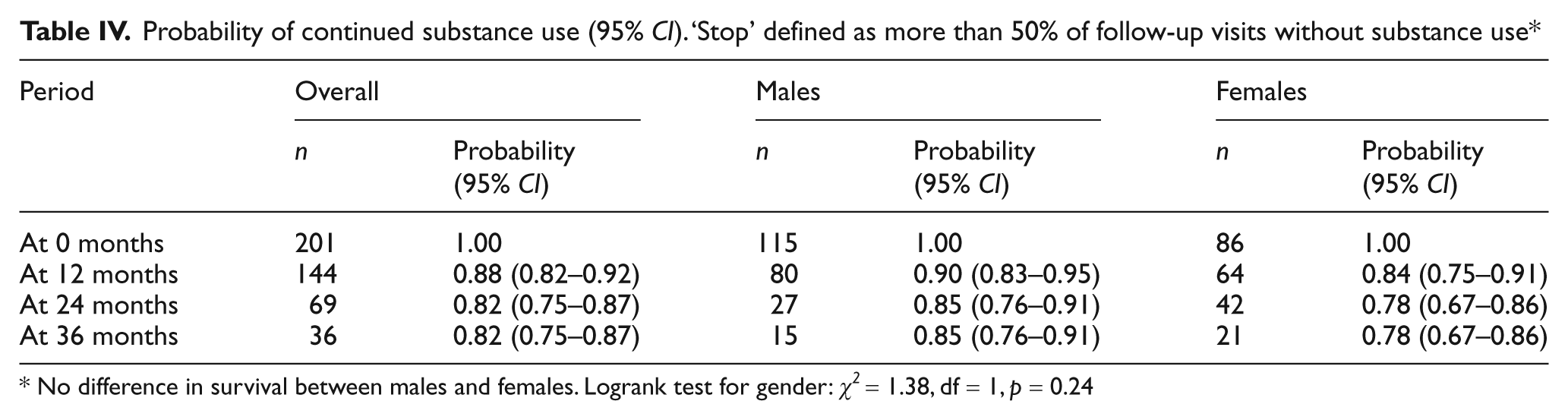
No difference in survival between males and females. Logrank test for gender: χ2 = 1.38, df = 1, p = 0.24
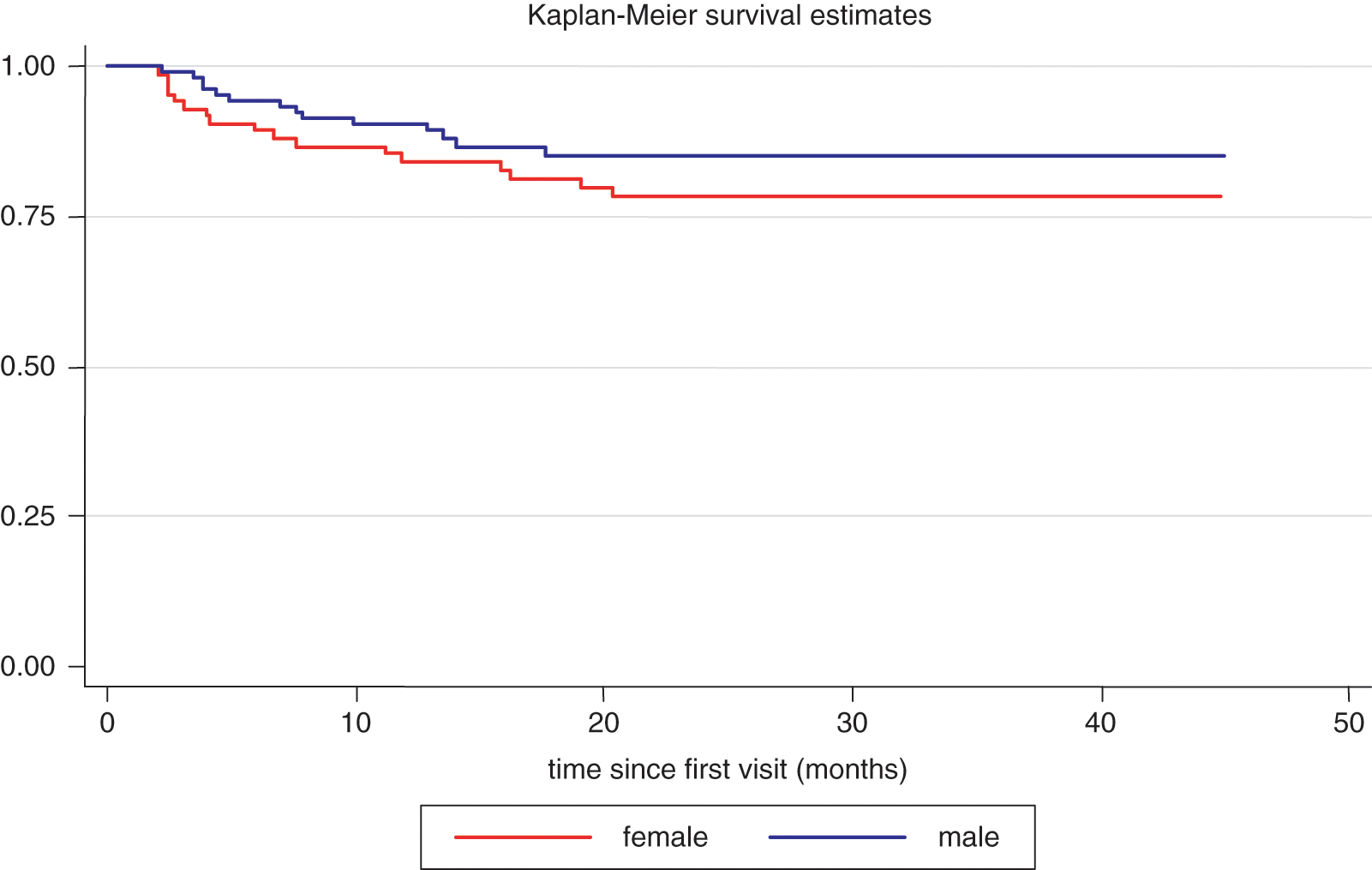
Survival curves for having more than 50% of remaining psychological consultations without substance use by gender
Discussion
This study aimed to describe the outcomes of psychological distress, substance abuse and the social situation of street children and youth participating in centre activities and identify how levels of psychological distress and substance abuse changed over time.
The results presented here demonstrate that service provision for street and youth populations is feasible in an urban and highly violent setting with services provided by different professionals targeting the complexity of the social, psychological and medical needs of such a vulnerable population. The programme was acceptable to street children and youth as indicated by their engagement in the programme and their regular attendance. The programme facilitated the decrease of psychological distress levels and the reduction of substance abuse in street children and youth.
Being male was identified as a predictor and interacting factor with time on improving psychological outcomes, whereas substance abuse was seen to decline more in females. Identifying predictors of positive outcomes in street children and youth populations is vital in order to design programmes to better address their needs. Future research should explore the reasons for such heterogeneous outcomes.
An important finding of this study is the fact that the individuals followed in the programme progressed to more protective environments. The results suggest that structured interventions can help street children and youth to leave dangerous street environments.
Few studies have described the outcomes of street children and youth attending day care centre programmes (Slesnick et al., 2007; Slesnick et al., 2008b; Slesnick and Prestopnik, 2005). Services providing psychological care, case management and the provision of basic necessities have shown to lead to improvements in mental health, substance abuse and social stability (Slesnick et al., 2008b). Similar to the present study, these services are based on outreach work. As a first step, street children and youth are invited to attend the drop-in centre. Once there, a case management approach is proposed where children and youth are assessed and a dedicated clinical manager coordinates access to mental healthcare and general medical services on behalf of the child, including facilitating access and ensuring service delivery.
The results of this study adds to existing evidence from developed countries on the impact of drop-in centres’ service delivery models for street children and youth with substance abuse problems in three respects. First, outreach work and the case management approach is a feasible and acceptable model of service provision for street children and youth populations, even in challenging urban and violent settings such as Tegucigalpa. Second, it provides a framework of the structure and content of services that could be provided for similar populations in different settings. Finally, the results highlight the benefits of multidisciplinary care programmes engaging with street children and youth populations and having them as active participants of the therapeutic process. The multidisciplinary intervention targets a reduction of psychological distress and substance abuse and therefore facilitates the process of motivation and guidance for street children and youth to progress to safer environments.
The drop-in centre is a key actor in facilitating the access for street children and youth to services provided inside the treatment centre and especially to existing health facilities and social services that often refuse this population. By facilitating access to existing services, the treatment centre initiates the process of inclusion of street children and youth into general population services. This could further help to reduce discrimination and violence against such marginalized groups.
Limitations
The most important limitation of this study is that it reports on monitoring and evaluation of an ongoing intervention rather than a controlled clinical trial evaluation. It is not possible to comment on the effectiveness of individual aspects of the intervention. Furthermore, the findings are for street children and youth that were able to access the services provided by centre. These children might be different to the street children and youth who could not access the services due to more complex or severe mental health and social needs, therefore these results may not necessarily be generalizable to the general population of street children and youth.
A second limitation concerns beneficiaries lost to follow-up. Although lost to follow-up is usual and expected for services providing care for such populations (Slesnick et al., 2008a), these children and youth could have deteriorated further. Although outreach work aimed to find defaulters, not all children and youth were traced due to the extreme complications of this process. More studies are necessary in order to understand the determinants of lost to follow-up and the development of strategies to increase adherence to therapeutic strategies. Similarly, not all children and youth responded to all questions and assessments, which led to missing values. As all participation was voluntary, no special attempt was made to elicit information from beneficiaries. Participation and continued attendance at the centre was the priority in order to ensure that a protective environment was preserved.
A third key limitation concerns the analysis presented here. For the survival analyses, beneficiaries were considered as having ‘stopped substance use’ if they reported no such use at more than 50% of their visits. Using a stricter criterion would change the magnitude of the effect reported here, but would not change the qualitative conclusions concerning harm reduction. This issue highlights the need to consider multiple indicators when evaluating programmes and working towards better defining indicators for future programme planning and evaluation.
Conclusion
Street children and youth populations are particularly vulnerable to violence and exploitation in developing countries facing epidemics of urban violence. This study revealed a mortality rate of 4% over the follow-up period, which is far beyond what is expected in this age group. This mortality rate reveals the urgency to respond to the immediate medical, social and psychological needs of street children and youth populations.
There are key policy implications of this programme for the planning of services for street children and youth populations in low-income countries. Drop-in centres based on outreach work and the case management approach could be a promising strategy to address the complex health and social needs of street children and youth. Providing acceptable and effective services to street children and youth populations in low-income countries should be considered a priority to ensure that the most marginalized groups receive appropriate care.