
Abstract
Background:
Up to 50% of patients with schizophrenia are non-adherent with antipsychotic medication.
Aims:
To establish the efficacy of adherence therapy (AT) compared to treatment as usual (TAU) in improving clinical outcomes in patients with schizophrenia following an acute exacerbation of illness.
Method:
A parallel-group, single-blind, randomised controlled trial. Fieldwork was conducted in Thailand. Patients received eight weekly sessions of AT in addition to TAU. The primary outcome was improvement in psychopathology (measured using the Positive and Negative Syndrome Scale (PANSS)) at 26-week follow-up. Secondary outcomes included patient attitudes towards medication, global functioning and side-effects.
Results:
In total, 70 inpatients with schizophrenia were recruited to the trial. At 26-week follow-up, PANSS total scores improved in the AT compared to the TAU group by a mean of −3.94 points (effect size = 0.24). The number needed to treat (NNT) was 5. There was no significant effect on patients’ attitudes towards treatment, functioning or medication side-effects. No treatment-related adverse effects were reported.
Conclusion:
AT improves psychopathology in Asian patients with schizophrenia following an acute exacerbation of illness.
Introduction
Maintenance treatment with antipsychotic medication is effective at preventing relapse in schizophrenia (Leucht et al., 2012) but requires that patients are compliant. In common with other long-term conditions, around 50% of patients with schizophrenia are non-adherent with medication (Lacro, Dunn, Dolder, Leckband, & Jeste, 2002). Non-adherence is associated with an increased risk of relapse, hospital admission and having persistent psychotic symptoms (Morken, Widen, & Grawe, 2008). Factors consistently associated with non-adherence include poor insight, negative treatment/illness beliefs, past non-adherence and a poorer therapeutic relationship (Lacro et al., 2002). Effective interventions to enhance adherence are required.
Adherence (nee compliance) therapy (AT) is a brief psychological intervention based on motivational interviewing and cognitive behavioural therapy (CBT) that aims to enhance adherence and improve clinical outcomes for patients with schizophrenia. To date, there have been 13 trials of AT involving 1197 patients, predominately conducted in Europe (Brown, Gray, Jones, & Whitfield, 2013; Gray et al., 2006; Gray, Wykes, Edmonds, Leese, & Gournay, 2004; Kemp, Hayward, Applewhaite, Everitt, & David, 1996; Kemp, Kirov, Everitt, Hayward, & David, 1998; O’Donnell et al., 2003; Schulz et al., 2013; Staring et al., 2010). Trials have also been conducted in America (Anderson et al., 2010; Byerly, Fisher, Carmody, & Rush, 2005) and Australia (Cavezza, Aurora, & Ogloff, 2013). The majority (9/13) have reported positive findings, although the largest trial (Gray et al., 2006) that involved 409 patients reported negative findings.
Rates of treatment non-adherence in Asian patients with schizophrenia are similar to those in Western populations. There have only been two published trials (Maneesakorn, Robson, Gournay, & Gray, 2007; Tsang & Wong, 2005) involving 110 patients who have tested AT in this population; the latter was an exploratory trial that informed this study. The aim in this trial was to test the effectiveness of AT in Thai patients following an acute exacerbation of schizophrenia.
Methods
A parallel-group, single-blind, randomised controlled trial (RCT) of adherence therapy compared to treatment as usual (TAU) in patients with schizophrenia following an inpatient hospital admission because of an acute exacerbation of schizophrenia. Patients were randomised on a one-to-one basis. Researchers who were blind to group allocation completed assessments. The fieldwork for this study was conducted in a large psychiatric hospital in Thailand. The trial adhered strictly to Consolidated Standards of Reporting Trials (CONSORT).
Objectives
The primary objective of this trial was to determine the effectiveness of AT compared to TAU in improving psychopathology at 26-week follow-up. Secondary objectives were to evaluate the effectiveness of AT at 26-week follow-up compared to TAU in improving patients’ attitudes towards medication, global functioning and side-effects of medication. A tertiary objective was to explore predictors of clinically significant improvement in psychopathology.
Participants
We included male and female patients over the age of 20 with a case note Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnosis of schizophrenia (American Psychiatric Association (APA), 2000) who were admitted for inpatient treatment because of acute exacerbation of their psychosis. The rationale for these criteria was that in some trials AT has been shown to be most effective just following an acute exacerbation of illness. Patients were excluded if
They had suicidal ideas or behaviours, because of the associated risks of conducting research in this group.
There was case note evidence of drug or alcohol dependence, as substance abuse has been shown to negatively affect medication adherence. Addressing these behaviours is not part of AT.
Because of the potential to limit participants’ engagement with AT patients with organic brain disease, or moderate to severe learning disability, those who did not speak fluent Thai were also excluded.
Towards the end of their inpatient admission, patients were approached by a member of the treating clinical team to enquire if they would consider participating in the trial. If they expressed interest in the study a researcher completed a screening checklist to determine their eligibility and obtained written informed consent.
Ethical approval
Ethical approval was obtained from the Institute of Psychiatry, King’s College London, and the Thai Ministry of Public Health. Written informed consent was obtained from all patients participating in the trial.
Sample size
We calculated that 70 patients would be required for this trial. Based on our pilot trial (Maneesakorn et al., 2007), we estimated a 15-point difference in PANSS totals scores between the AT and TAU groups at the week 26 assessment. Our power calculation was based on the following assumptions: a standard deviation of 17, an alpha of .05, a 2-tailed test of significance, 90% power and that 30% of patients would withdraw.
Setting
Patients were recruited from 10 inpatient units in Sanprung Psychiatric Hospital in Chiang Mai, located in the North of Thailand. The hospital is responsible for 97,115 psychiatric patients (0.7% of the 15 million people living in 15 northern Thai provinces). The average length of inpatient stay is approximately 1 month.
Outcome measures
The primary outcome was improvement in psychopathology, measured using the Thai version of the Positive and Negative Syndrome Scale (PANSS-T). The PANSS-T has established psychometric properties in Thai patients with schizophrenia (Nilchaikovit, Uneanong, Kessawai, & Thomyangkoon, 2000). Secondary outcomes included patient attitudes towards medication measured using the Drug Attitude Inventory (DAI-30) (Hogan, Awad, & Eastwood, 1983); global functioning, determined using the Global Assessment of Functioning (GAF ) Scale (Hall, 1995); and side-effects of medication assessed using the Liverpool University Neuroleptic Side Effects Rating Scale (LUNSERS; Day, Wood, Dewey, & Bentall, 1995). The PANSS and GAF were already available in Thai. The DAI-30 and the LUNSERS required translation. Details of the translation process used are described elsewhere (Maneesakorn et al., 2007). All measures were administered at baseline and 26-week follow-up by research assistants who had been trained to administer the assessments in a standard way and were blind to treatment allocation. Researchers completed the measures in the outpatient clinic or in the patients’ own home dependent on patient preference. For the PANSS, we established a high degree of inter-rater reliability (r = 0.71, 95% confidence interval (CI) 0.48, 0.85) between researchers.
Randomisation
Randomisation was undertaken by an independent randomisation service. For allocation of the participants, a computer-generated list of random numbers was used. Patients were randomly assigned following simple randomisation procedures to AT or TAU. The nurse therapist (Suparpit von Bormann (S.v.B.)) delivering the intervention had the contact details of all patients involved in the study. S.v.B. was contacted by the randomisation service and was told which group patients had been allocated to. They then arranged assessment and, in the AT group, visits to deliver the intervention. Researchers were not able to access any information about group allocation and were instructed not to ask patients if they had received any additional therapy from a nurse.
Statistical methods
All analyses were conducted on an intention-to-treat basis. Outcomes were analysed using SPSS v14 (SPSS, Inc., 2005). Most outcome variables were not normally distributed at baseline, and log transformation was not considered to be appropriate when statistical advice was sought. The effect of the intervention was determined using analysis of covariance (ANCOVA) and regression analysis. Effect size was calculated using the t-test for the significance of the product–moment correlation coefficient that is suitable for unequal sample sizes. Binary logistic regression analysis was used to identify predictors of clinically significant improvement defined as a 25% or more reduction in PANSS total scores (Csernansky, Mahmoud, & Brenner, 2002).
Interventions
Patients in the intervention group received eight sessions of AT as an add-on to TAU. A trained nurse therapist (S.v.B.) delivered all sessions. S.v.B received approximately 40 hours of AT training and regular clinical supervision from the third author (R.G.) and the second author (D.R.), who developed and manualised the intervention. AT is rooted in the observation that patients’ beliefs impact on medication compliance. A patient-centred manualised approach, AT is delivered as a course over a series of eight one-to-one sessions, each with a different focus. The fundamental clinical skills of adherence therapy include agenda setting, using the patient’s own language, collaborative working, linking sessions together and reflective listening. The four cornerstones of AT are keeping the patient engaged, minimising resistance to change, providing information required by the patient about medication and side-effects and using Socratic dialogue to generate discrepancies in patients’ beliefs about treatment. Within this framework there are specific AT exercises:
Assessment by exploring patients’ beliefs about treatment, practical problems with medication and side-effects and medicines reconciliation (reviewing all medication, prescribed or otherwise, patients are taking).
Structured medication problem solving to address practical issues with medication, for example, side-effects or remembering to take medication.
Using a medication timeline to help patients review past experiences of illness and treatment.
Exploring patients’ ambivalence about taking medication using a decisional matrix (the pros and cons of taking/not taking medication).
Testing patients beliefs about medication, for example, ‘I can stop medication once I start to feel well,’ ‘taking medication is unnatural,’ ‘medication is a slow acting poison’.
Helping patients to move forward in their lives, to consider ‘life goals’ and the role medication may play in achieving these.
TAU group: TAU included medication, vocational and recreational therapy and outreach community psychiatric support.
Results
Fieldwork was conducted from 1 November 2004 to 31 October 2005. Figure 1 shows the flow of patients through the trial. Of 155 patients screened to participate, 76 met the inclusion criteria. Six patients did not participate because they were living outside of the hospital catchment area or refused to take part. A total of 70 patients were randomly assigned into two groups. Two patients in the AT group were lost to follow-up at the 26-week assessment. One was discharged and could not be contacted; the other moved out of the area and did not leave a forwarding address. Missing data were handled using last observation carried forward (LOCF).
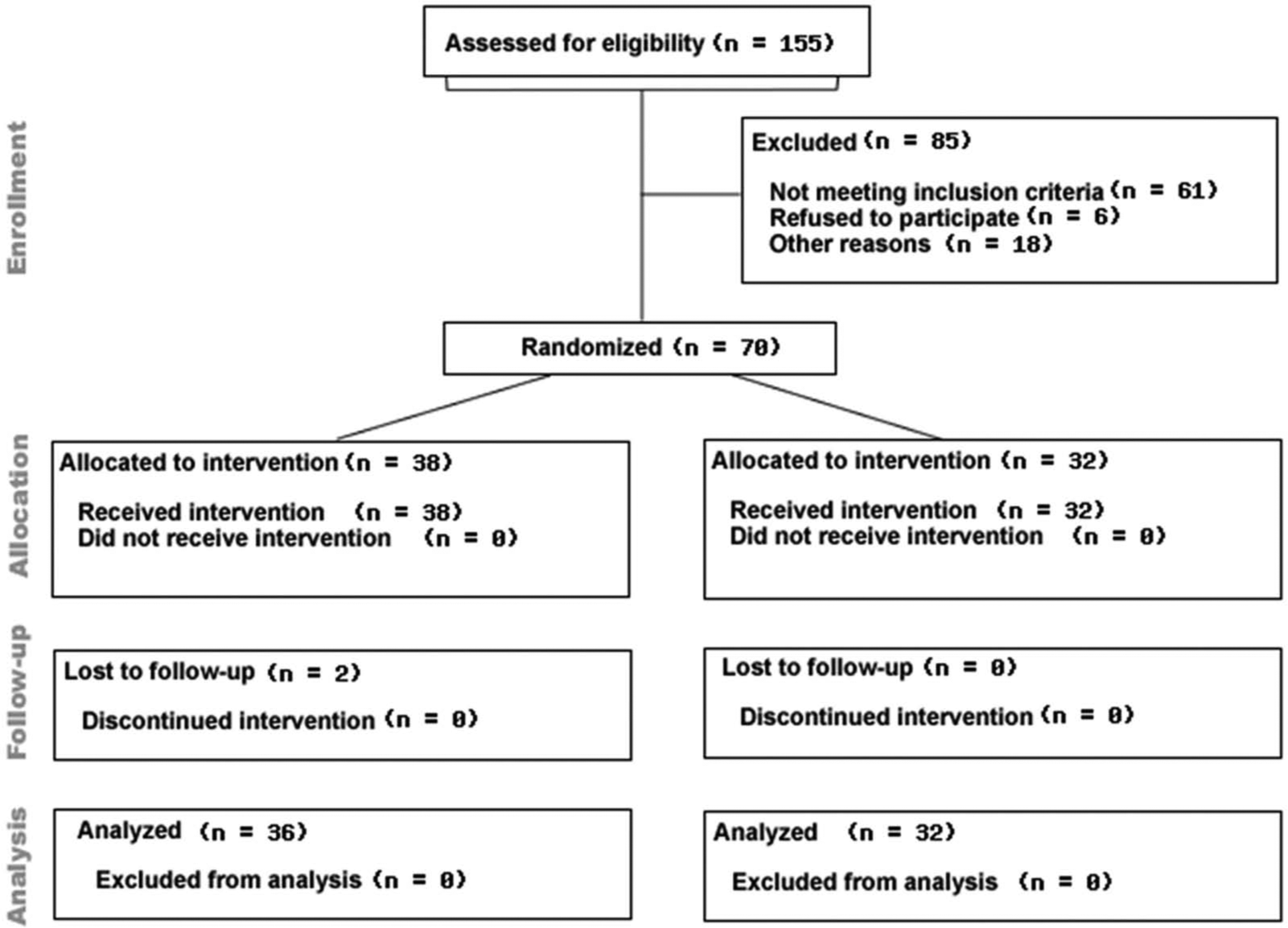
AT for schizophrenia.
A number of important baseline differences in demographic characteristics were observed between the AT and TAU groups. Patients in the TAU group were older, less likely to have a carer and more likely to be working (Table 1).
Baseline demographic characteristics of participants.
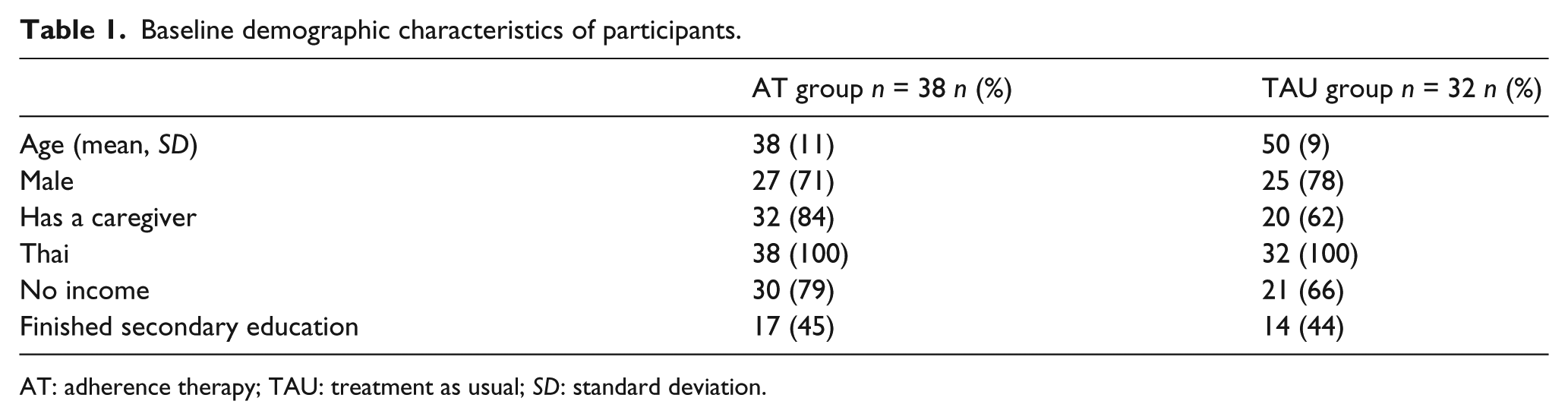
AT: adherence therapy; TAU: treatment as usual; SD: standard deviation.
The clinical characteristics of the two groups were broadly similar at trial entry. Average dosages of antipsychotics (in chlorpromazine equivalents) were, respectively, 332 and 329 mg/day for the AT and TAU groups. At baseline, 11 of 38 patients (29%) in the AT group and 9 of 32 (28%) in the TAU group were prescribed clozapine. At trial entry, the acute phase of the patients’ illness had passed and they had generally positive attitudes towards their medication. The TAU group had better global functioning and experienced more side-effects than the AT group (Table 2).
Baseline clinical characteristics of participants.
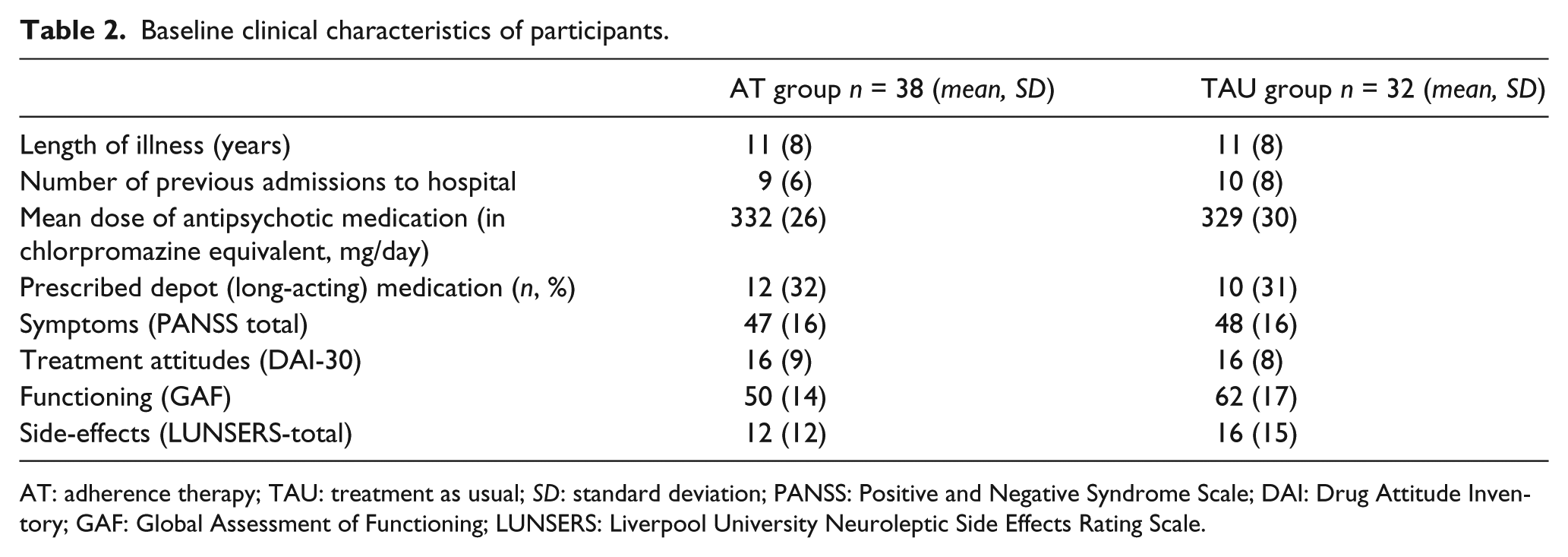
AT: adherence therapy; TAU: treatment as usual; SD: standard deviation; PANSS: Positive and Negative Syndrome Scale; DAI: Drug Attitude Inventory; GAF: Global Assessment of Functioning; LUNSERS: Liverpool University Neuroleptic Side Effects Rating Scale.
All patients received eight sessions of AT. The mean duration of each session was 41 minutes (standard deviation (SD) = 8) and ranged from 23 to 57 minutes. In total, patients received 5 hours and 25 minutes (SD = 1.16) of AT.
Outcomes
Compared to TAU, AT significantly improved patients’ psychopathology (Table 3) representing a small effect size (ES = 0.24). There were no significant differences in treatment attitudes, functioning or side-effects between AT and TAU. No treatment-related serious untoward incidents were reported.
Outcome measures at baseline and follow-up according to treatment group.
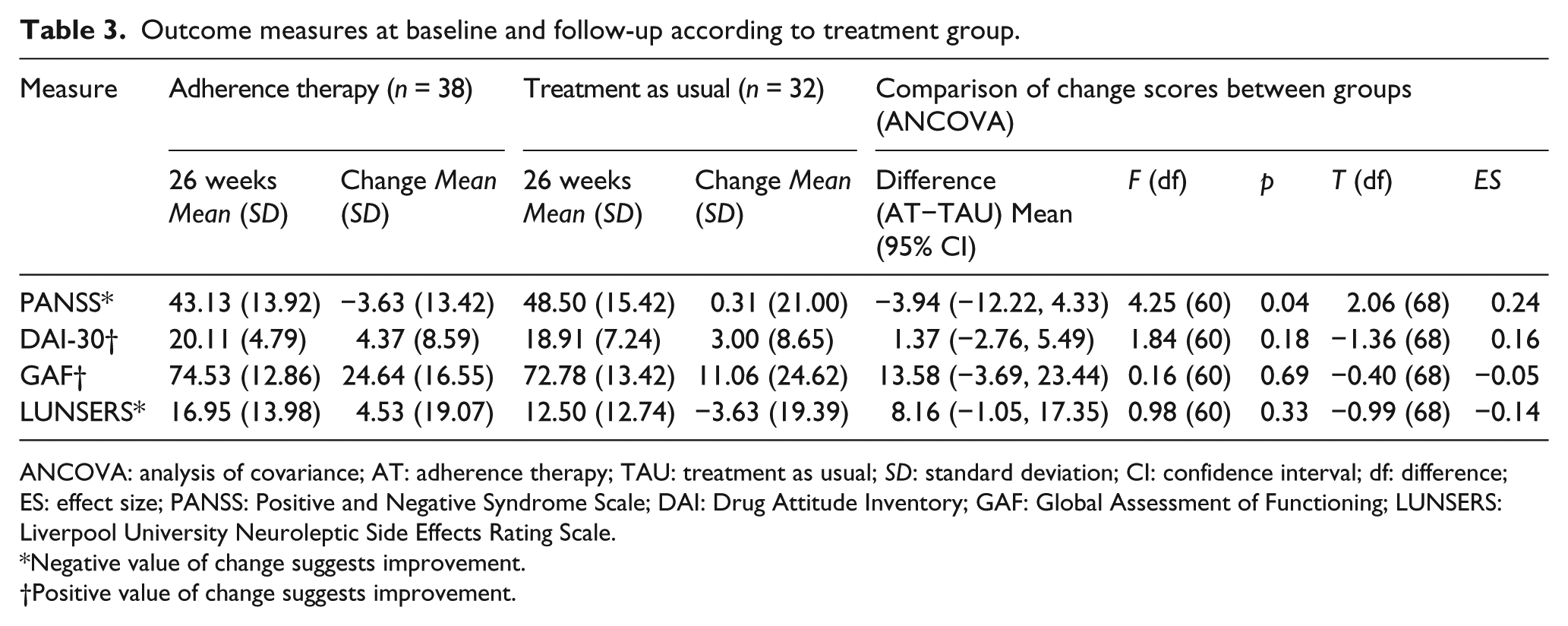
ANCOVA: analysis of covariance; AT: adherence therapy; TAU: treatment as usual; SD: standard deviation; CI: confidence interval; df: difference; ES: effect size; PANSS: Positive and Negative Syndrome Scale; DAI: Drug Attitude Inventory; GAF: Global Assessment of Functioning; LUNSERS: Liverpool University Neuroleptic Side Effects Rating Scale.
Negative value of change suggests improvement.
Positive value of change suggests improvement.
PANSS baseline scores were the only significant predictor of clinical improvement at follow-up (Exp (B) = 1.10, 95% CI = [1.04, 1.15], p < .01) accounting for 83% of the variance.
Number needed to treat (NNT) is defined as the number of patients who must be treated to prevent one additional adverse event. For the purposes of this trial, this was defined as any patient that experienced a relapse of their psychosis (a minimum 25% increase in PANSS total scores). In the AT and TAU groups, 17 (45%) and 21 patients (66%), respectively, met these criteria. We calculated that five patients (95% CI 4.53, 4.99) needed to be treated with AT to prevent one relapse.
Discussion
The objective of this trial was to establish the effectiveness of AT compared to TAU in improving psychopathology in Thai patients with schizophrenia at 26-week follow-up. The results of this trial suggest that AT is effective at treating schizophrenia symptoms in Asian patients with schizophrenia with a NNT of 5.
AT was delivered, following an acute exacerbation of their psychosis, to adult, Thai, men and women, with a range of income, different educational background and with varying levels of caregiver support. The results suggest that a range of patients, from those with a relatively short duration of illness and only a single previous admission to those that have been unwell for many years and have had several previous admissions, can benefit from AT following an acute episode of illness.
As in the initial Kemp et al. (1996, 1998) and Schulz et al. (2013) studies, participants in this trial were recruited following an acute episode of psychosis. Other trials (Gray et al., 2006) have recruited patients who have been clinically stable and community dwelling. This is a potentially important difference between the studies. It may be that the most opportune moment to tackle adherence is following an acute episode of illness of admission to hospital. Authors of Crisis Theory (Caplan, 1964) argue that it is just after a crisis event that people are most amenable to changing behaviour. Schulz et al. (2013) suggest that it is immediately following an acute episode of illness that AT should be applied. The findings of this trial are consistent with this hypothesis.
Since 1996, there have been 13 trials of AT (Anderson et al., 2010; Brown et al., 2013; Byerly et al., 2005; Cavezza et al., 2013; Gray et al., 2004, 2006; Kemp et al., 1996, 1998; Maneesakorn et al., 2007; O’Donnell et al., 2003; Schulz et al., 2013; Staring et al., 2010; Tsang & Wong, 2005). This trial replicates and extends the work of Kemp et al. (1996, 1998) and others (Brown et al., 2013; Cavezza et al., 2013; Gray et al., 2004; Maneesakorn et al., 2007; Schulz et al., 2013; Staring et al., 2010; Tsang & Wong, 2005) who reported AT is effective at treating schizophrenia and suggests the intervention can be applied into a culturally different Thai population of patients. However, the effect size in this trial was smaller than in our own exploratory (Maneesakorn et al., 2007) trial, where we reported a large effect size (ES = 0.56).
We chose to use symptoms, measured using the PANSS and not adherence as our primary outcome for this trial. There is no valid and reliable measure of medication adherence; pill counts, clinician rating and belief/attitude scales have been used but authors report only a weak correlation between them (Gray et al., 2006). Enhancing adherence without showing that clinical outcomes have improved is meaningless to patients and perhaps unethical. In this trial, we observed only modest improvements in patients’ symptoms. In part, this may be explained by the lower level of psychopathology patients were experiencing at baseline compared to those in our pilot study (a possible ceiling effect). The more modest effect we observed in this compared to previous trials may also be explained by differences in duration of follow-up; in the first trial, patients were followed up after 9 weeks (after completion of the intervention), and in this trial follow-up was at 26 weeks. This observation may suggest that the effects of AT in an Asian population degrade over time.
Limitations
The use of TAU as the control condition is a limitation of our study because it does not control for the non-specific effects of a mental health worker spending regular time with a patient. While the provision of a control intervention might have strengthened the design of our trial, we felt that it was ethically dubious engaging patients in a time-consuming treatment that had been specifically designed to be inert.
That patients at the start of the study were generally adherent, potentially restricting the effect of AT, is a further limitation of our trial. Sufficiently strict inclusion criteria ensuring that only non-adherent patients were included should have been applied.
In this study, there was a single therapist who, it might be argued, had a high level of motivation to demonstrate the effectiveness of AT. The study could have been strengthened if there were more therapists delivering the intervention. Therapist fidelity to AT was not monitored; consequently we cannot determine how faithfully the intervention was delivered. Other AT trials (Gray et al., 2006) have monitored fidelity and our study would have been enhanced if we had used these procedures.
Future research
The results of AT trials are mixed. The findings from this and other recent trials suggest that AT is perhaps most effective following a psychiatric crisis. A case can perhaps now be made for a full trial of AT in this population. It is important to note that any such trial should pay close attention to challenges of recruiting non-adherent patients with schizophrenia to their trial. The importance of effective sampling and recruitment strategies in such a study cannot be underestimated. There is a real risk that if these issues are not addressed a potentially effective schizophrenia treatment may be rejected because it has not been tested on the right patients.
Conclusion
The results of this adequately powered RCT suggest that AT is an effective intervention in an Asian population of patients following an acute episode of schizophrenia.
Footnotes
Acknowledgements
We thank all the participants including clinicians, nurses and patients for their support in the trial (ISRCTN: 74277581; the Current Controlled Trials Limited).
Contributors
R.G., D.R. and S.v.B. designed the study. S.v.B. delivered the therapy, analysed data and coordinated the study. S.v.B. wrote the initial draft. All authors finalised the manuscript and approved the final document. R.G. is the guarantor for the study.
Conflict of interest
S.v.B. and D.R. have no conflicts of interest. R.G. has received honoraria and provided consultancy to AstraZeneca, Bristol-Myers Squibb, Jannsen Cilag, Eli Lilly and Co. and Otsuka Pharmaceutical Europe Ltd.
Full protocol
A copy of the trial protocol can be obtained from the corresponding author on request.
Funding
The Royal Thai Government provided a PhD scholarship for S.v.B.