
Abstract
Background:
Families of individuals with psychotic disorders are playing a major role in the care of their relatives, but report poorer physical competence, elevated symptoms of psychological distress and more psychopathological characteristics.
Aim:
To compare psychopathological characteristics demonstrated by caregivers of psychotic patients in Greece who participated in support groups organized by non-governmental mental health organizations (NGOMH) compared to caregivers who did not.
Methods:
Participants were caregivers of a psychotic patient assigned to either the intervention group (n = 165) or the non-intervention group (n = 345) according to specific criteria. Participants were assessed for psychopathological characteristics through clinical interviews and with the Symptom Checklist 90–Revised (SCL-90-R).
Results:
Participants who did not take part in the support groups had higher levels of psychopathological characteristics on the dimensions of interpersonal sensitivity (t = −2.065, p = .003), depression (t = 1.043, p = .007), anxiety (t = 1.001, p = .010), hostility (t = −4.345, p < .001), phobic anxiety (t = −2.845, p < .001) and paranoid ideation (t = −1.091, p < .001). Psychotic relatives of participating caregivers show higher compliance rates in taking their medications, and female caregivers tend to be more involved in the support groups.
Conclusion:
Participation in support groups and sharing of emotional expression, thoughts and ideas help the caregivers deal with their physical and psychological demands related to the caregiver load. As such, intervention strategies offered to caregivers in the support groups appear to positively contribute to the family with a psychotic patient and improve the quality of life of both patients and their main caregivers.
Introduction
Families of individuals with psychotic disorders are playing a major role in the care of their relatives. Most caregivers feel burdened when caring for relatives with major psychiatric disorders as these disorders are unpredictable and long-lasting. In order to keep the patients stable and maintain function, family members need to supervise medication compliance, urge patient self-care and protect them from possible harm (Schene, van Wijngaarden, & Koeter, 1998). This requires great time consumption and is psychologically demanding, and caregivers often carry out these tasks at great personal cost. They report poorer physical competence, elevated symptoms of psychological distress, feeling of stigmatization, limited time for leisure and socializing, and unreimbursed patient-related expenses (Foldemo, Gullberg, Ek, & Bogren, 2005; Ostman & Kjellin, 2002).
Further to the impact on the caregivers’ lives, an increased care burden has been associated with greater use of health services, psychotropic drugs (Perlick et al., 2007) and higher expressed emotion toward the patients, which may eventually lead to patient relapse (Raune, Kuipers, & Bebbington, 2004).
The level of care burden is the consequence of interplay between multiple factors, such as the caregiver’s socio-demographic characteristics, the patient’s condition, time spent on the care work and the presence or absence of protecting factors. According to prior studies, increased burden is associated with a greater severity of the patient’s psychiatric symptoms, poorer functional level and lack of social support (Magliano et al., 2002). Disputes have been noted in the risk factors related to caregiver’s gender, kinship with the patient and the time spent on the care work (Magliano et al., 2005). Caregivers often report feelings of loss and restrictions in their own social and leisure activities, which may be related to increased burden (Gutiérrez-Maldonado, Caqueo-Urízar, & Kavanagh, 2005; Perlick et al., 2007). As reported previously, caregivers have elevated symptoms of psychological distress, feeling of stigmatization, limited time for leisure and socializing, and unreimbursed patient-related expenses (Foldemo et al., 2005; Ostman & Kjellin, 2002), which may lead to psychopathology. In this respect, caregivers require social support networks to alleviate the distress and probability of developing psychopathology themselves.
The aim of this study was to investigate the psychopathological characteristics demonstrated by caregivers of psychotic patients in Greece who participated in caregiver social support groups organized by non-governmental mental health organizations (NGOMH) compared to caregivers who had not participated in such groups and had not received any support other than that provided by the psychiatrist who was therapeutically responsible for the patient.
We hypothesized that caregivers who participated in these support groups would demonstrate lower levels of psychopathological characteristics compared to caregivers who did not. Our hypothesis is based on the fact that caregivers who take part in the groups are trained to deal more adequately with the psychiatric symptoms and other health-related problems and further develop stronger and healthier relationships and a larger social support network.
Materials and methods
Sample
The sample was composed of families of caregivers with a psychotic patient assigned to one of the two groups, according to participation (NGOMH; n = 165) or not (non-NGOMH; n = 345) in the support groups. The first group (participants who took part in the support groups) was recruited according to the following criteria: (a) minimum of 2-year participation period in the support groups for caregivers, (b) the patient of the caregiver family was diagnosed by an experienced psychiatrist as psychotic, (c) the caregiver was older than 18 years of age and maintained a functional relationship with the patient, (d) at least one caregiver took part in the social support group sessions, (e) the caregiver was cognitively competent to take part and benefit from the support group sessions and (f) all participants provided written informed consent to participate in the study, which was approved by the Ethics Committee of the University of Thessaly. The second group of caregivers was also recruited according to the above-mentioned criteria, but this group did not participate in the support group sessions and had no structured psychosocial support other than that provided by the psychiatrist who was therapeutically responsible for the patient.
We utilized a ‘snowball sampling design’ as this research was based on the recruitment of caregivers of known psychotic patients. All participants were recruited with the assistance of the staff employed at the NGOMH centers that collaborated for the treatment of patients. The study started on 1 January 2010 and was completed on 31 December 2013. The sample was composed of 510 participants (patient caregivers), which is approximately 1% of the actual population of family caregivers with a psychotic patient in Greece. This is the largest sample recruited in Greece for this particular type of study (see Table 1 for demographic characteristics of caregivers and Table 2 for demographic and clinical characteristics of patients).
Demographic characteristics of caregivers: mean (SD).
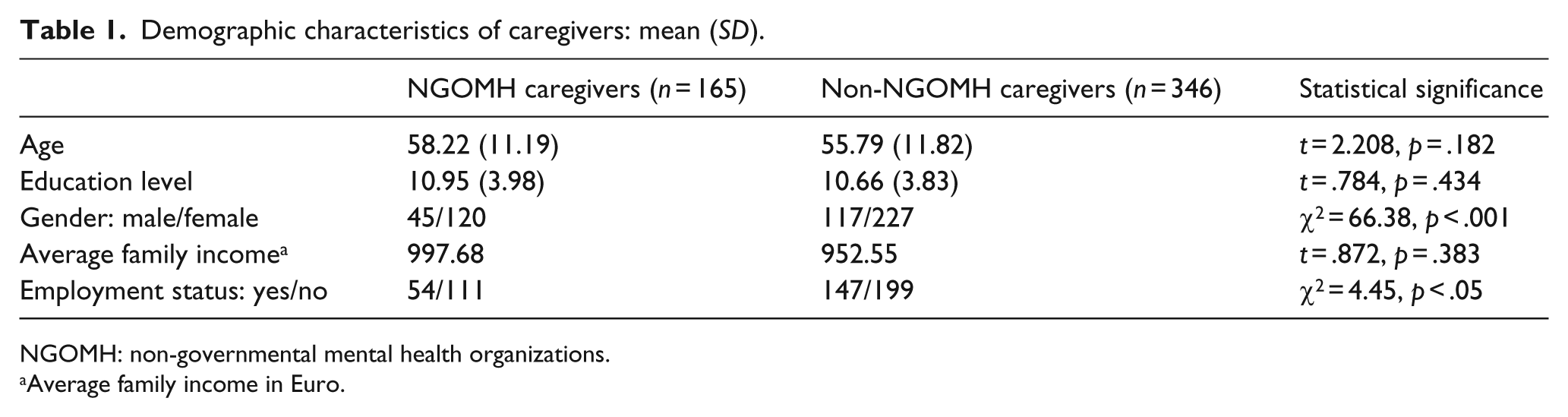
NGOMH: non-governmental mental health organizations.
Average family income in Euro.
Demographic and clinical characteristics of patients: mean (SD).
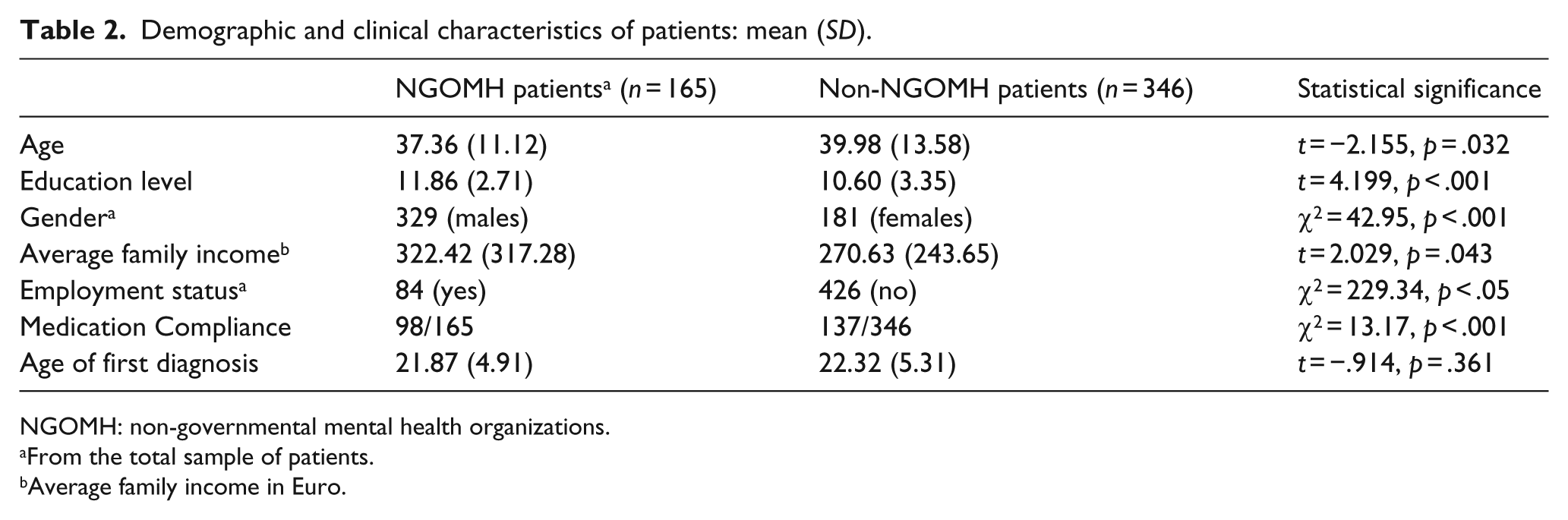
NGOMH: non-governmental mental health organizations.
From the total sample of patients.
Average family income in Euro.
Psychological measures
In order to investigate the psychopathological characteristics of caregivers, we utilized the Symptom Checklist 90–Revised (SCL-90-R) (Derogatis, 1983, 2000). The SCL-90-R is a 90-item self-report symptom inventory designed to reflect psychological symptom patterns of psychiatric and medical patients. Each item of the questionnaire is rated on a five-point scale of distress from 0 (none) to 4 (extreme). The SCL-90-R consists of the following nine primary symptom dimensions: somatization (SOM, which reflects distress arising from bodily perceptions), obsessive–compulsive (OC, which reflects obsessive–compulsive symptoms), interpersonal sensitivity (IS, which reflects feeling of personal inadequacy and inferiority in comparison with others), depression (DEP, which reflects depressive symptoms, as well as lack of motivation), anxiety (ANX, which reflects anxiety symptoms and tension), hostility (HOS, which reflects symptoms of negative affect, aggression and irritability), phobic anxiety (PHO, which reflects symptoms of persistent fears as response to specific conditions), paranoid ideation (PAR, which reflects symptoms of projective thinking, hostility, suspiciousness and fear of loss of autonomy) and psychoticism (PSY, which reflects a range of symptoms from mild interpersonal alienation to dramatic evidence of psychosis) (Derogatis, 1983, 2000).
The SCL-90 takes between 12 and 20 minutes to complete. With regard to its reliability, the internal consistency coefficient α values for the nine symptom dimensions ranged from 0.77 for psychoticism to a high of 0.90 for depression. Additionally, the few validity studies of the SCL-90-R demonstrate levels of concurrent, convergent, discriminant and construct validity comparable to other self-report inventories. The SCL-90-R has been used and standardized in the Greek population, and its reliability (Cronbach’s α) for the total items is 0.97 (Donias, Karastergiou, & Manos, 1991; Vitoratou, 2004). The cutoff for the SCL-90-R subscales is 0.99 (Donias et al., 1991).
Statistical analyses
Statistical analyses were performed with the SPSS package (Release 21.0). Group differences for demographic and clinical characteristics were investigated by means of independent sample t-tests (data met the assumptions required for parametric tests), and Pearson’s chi square (χ 2 ) tests were used to analyze categorical variables. Statistical significance was set at 5% significance level.
Results
Comparisons of demographic characteristics between caregivers who took part in the support groups and those who did not revealed non-significant differences in age (p = .182) and education levels (p = .434), but there were more female caregivers than male caregivers (p = .000). Furthermore, the mean family income of caregivers did not differ between the groups (p = .383), although less caregivers were employed (p < .05; see Table 1).
On the other hand, patients did not differ regarding their age of first diagnosis (p = .361) but differed on medication compliance, that is, patients who took part in the support groups showed better compliance (p = .000) and had higher average monthly incomes (p = .043). Also, patients who took part in the support groups had higher education levels (p = .000) but were slightly younger than the comparison group (p = .032), and there were significantly more male patients than females (p = .000; see Table 2).
Furthermore, in order to compare performance on the SCL-90-R between the caregivers who took part in the support groups and those who did not, we initially conducted a one-sample Kolmogorov–Smirnov test in order to examine test distribution. We found that our data were normally distributed and therefore used independent sample t-tests in order to compare performance between the groups. We found significant differences between the two groups on the dimensions of interpersonal sensitivity t = −2.065, p = .003; depression t = 1.043, p = .007; anxiety t = 1.001; p = .010; hostility t = −4.345, p = .000; phobic anxiety t = −2.845, p = .000 and paranoid ideation t = −1.091, p = .000. The remaining dimensions of the SCL-90 R did not differ between the two groups (see Table 3). These differences indicated that participating caregivers had less psychopathological characteristics as noted on the SCL-90-R.
Performance of caregivers who participated in NGOMH compared to caregivers who did not participate in NGOMH on the Symptom Checklist 90–Revised: M (SD).
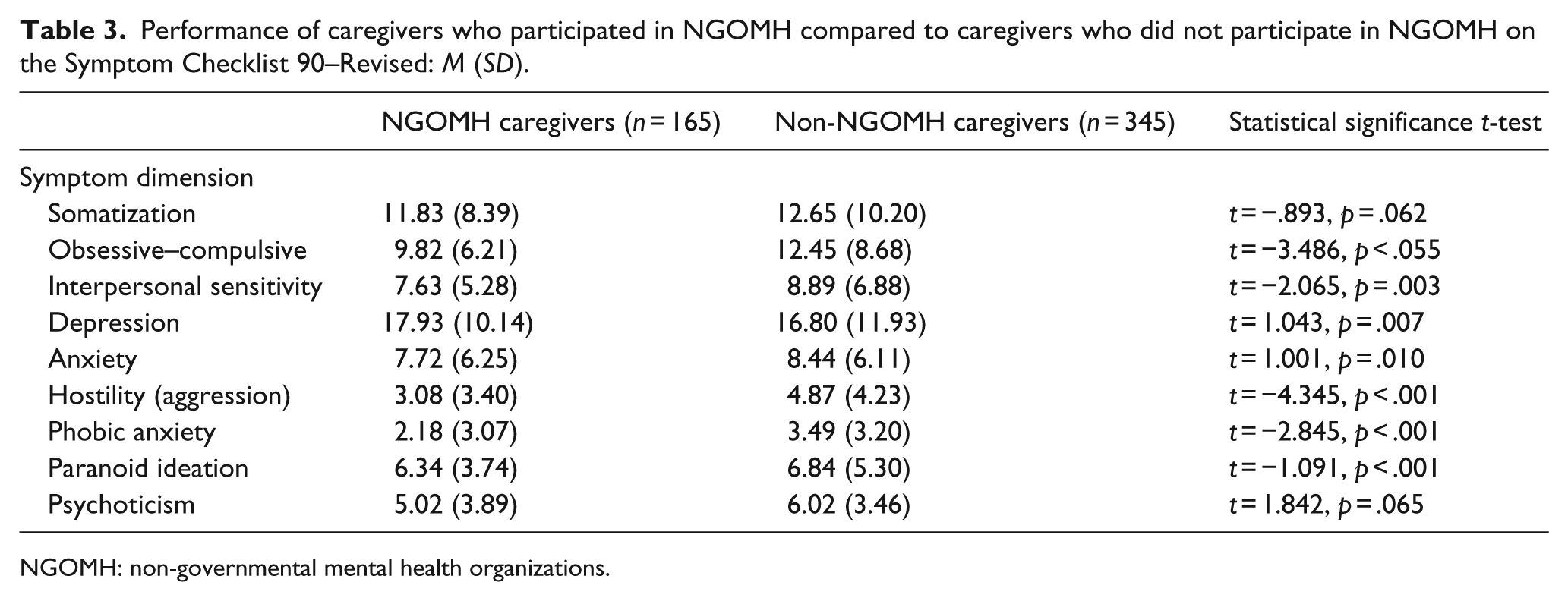
NGOMH: non-governmental mental health organizations.
In order to examine the potential contribution of demographics (age, gender, education level, average family income, employment status) of caregiver’s performance on the SCL-90-R, which might have contributed to the demonstrated differences noted between the comparing groups, we conducted a stepwise multiple linear regression analyses. Based on the results of the regression analyses, we found that none of the demographic characteristics contributed significantly to the noted differences between the comparing groups. In this respect, it appears that the positive effect (lower levels of psychopathological characteristics) of the intervention strategies offered to caregivers in the support groups is independent of the demographic characteristics of the caregivers.
Discussion
The competency of the caregiver to accomplish his or her goal with success is dependent on several factors. First is the ability of the patient to have a controllable clinical outcome and of the caregiver’s family status, which will allow him or her to provide sufficient caregiving. If the family is unable to provide care, this will lead to an increase in need of structures to accommodate these patients and of course public cost.
Self-care is based on the assumption that people with a common problem who collaborate in groups can actually provide better self-assistance through group interaction. Studies (Borkman, 1997; Kurtz, 1992; Lehman, 1995) have shown that taking part in support groups reduces feelings of isolation, increases practical knowledge and strengthens the courage of the participants to continue their battle. It also allows for developing new strategies to resolve their difficulties and formulate new social support networks.
Studies have shown that caregiver participation in support groups reduces emotional isolation, increases knowledge related to the disorder and reinforces participants’ courage to deal with the disorder (Borkman, 1997; Emerick, 1990; Kurtz, 1990). Furthermore, participation in support groups allows for the development of more efficient strategies for solving everyday problems related to the disorder and enhances new social support networks.
According to the findings of our study, it is clear that female caregivers of psychotic patients are more involved in the NGOMH support networks/groups offered in Greece compared to their male counterparts. This finding is supported by the fact that female caregivers in Greece have more free time as their main occupation/activities are those of a housewife (i.e. care of the home, preparation of food, etc.) and are more actively involved in the emotional/psychological support of the patient. In this respect, it is more viable for female caregivers to take part in psychoeducational and support groups regarding their psychotic relative. In addition, female caregivers appear more sensitive to the positive outcomes obtained by such support groups (Kurtz, 1990, 1992).
Furthermore, our data indicate that patients, whose caregivers participate in support groups, show much higher compliance rates in taking their medications and therefore a much lower relapse rate. This finding is independent of the socio-demographic characteristics of the caregiver families.
Several studies in the last decade support our outcome regarding the lower relapse rate in caregivers who have participated in psychoeducational support groups for psychotic patients (Falloon, 1986; Falloon, Boyd, & McGill, 1982; Falloon et al., 1998; Lehman, Carpenter, & Goldman, 1995; Schooler, Keith, Severe, & Matthews, 1995). An important factor, however, that contributes to this outcome is the fact that patients also participate in similar support groups following the activities of their caregivers.
These patient support groups include a range of activities, including occupational and recreational (e.g. drawing, constructional activities, music, photography), psychotherapy, psychological support, and so on. In this respect, the lower relapse rate of patients whose caregivers take part in support groups is related, to a great extent, to an improved social support network, better strategies to deal with the disorder (i.e. increased practical knowledge), healthier and more controllable environment at home, fewer feelings of isolation and improved self-esteem to deal with the disorder.
Regarding the development of psychopathological characteristics related to caregiving, it appears from our analyses that caregivers who took part in the support groups showed better levels of physical and psychological adaptation and less significant psychopathological characteristics compared to their counterparts who did not participate in such groups. More specifically, we found clinically significant differences in levels of interpersonal sensitivity, depression, anxiety, hostility (aggression), phobic anxiety and paranoid ideation on the SCL-90-R between the two groups, favoring those who participated. This finding is supported by other studies (Cohen & Willow, 1985; Lehman, 1995), which have shown that participation in support groups and sharing of emotional expression, thoughts and ideas help the caregivers deal with their physical and psychological demands related to the caregiver load.
More specifically, interpersonal sensitivity, that is, feelings of low self-esteem and personal insufficiency, is dealt with to a large extent and is overcome in caregivers who participate in these groups due to the process of positive interaction that allows for a higher acceptance rate of their situation. Caregivers in this sense are not interested in ‘what others have to say’, but rather devote their efforts in sensitizing the society as regards the prejudice related to psychiatric disorders. Their aim is to deal with the obstacles that will allow the reintegration of the psychotic patient into society. Unlike participating caregivers, their counterparts deal with the ‘stigma’ of the psychosis in a more passive way, leading to tension, increased levels of stress and less effective strategies to cope with the everyday needs of the patient.
Furthermore, as stated by Clay (2003), caregivers who take part in such groups reinforce their control mechanisms and achieve their set goals much easier. The process of reinforcement provides the caregiver with a range of choices, the strength to make decisions, access to necessary information, funding and the sense that they can make the difference. In this respect, psychosis gradually becomes less a medical and more a social problem requiring social and political interventions (Clay, 2003; Flyckt, Lothman, & Jorgensen, 2011). This process assists NGOMH caregivers to better deal with their physical and psychological problems, such as depression, anxiety and aggression.
Caregivers who did not participate in support groups tend to experience the psychosis of their patients in isolation, develop less effective coping strategies and have significant difficulties in formulating social support networks. This in turn leads to increased family and caregiver burden, poor functional outcomes and higher rates of relapse.
As such, intervention strategies offered to caregivers in the NGOMH support groups in Greece appear to positively contribute to the family with a psychotic patient and improve the quality of life of both patients and their main caregivers. Several studies (Caqueo-Urízar et al., 2011; Saunders, 2003; Schooler et al., 1995; Upmanyu, Minhas, & Goloshejerdi, 2000) have found similar positive effects of support groups on caregiver coping with the psychotic patient and confirm our outcomes.
Our findings have implications for possible political interventions related to mental health issues, especially in Greece, where for the last 5 years a financial crisis exists, which has significantly reduced the funding available for mental health purposes. In this respect, the development of NGOMH-related support groups in large cities in Greece or at least in cities where psychiatric clinics function may contribute to improvements in the caregivers’ quality of life and the development of active programs will function as low-cost supplementary mental health facilities.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.