
Abstract
Background and aims:
Support of personal recovery represents the aim for many modern mental health services. There is a lack of conceptual clarity around the application of the term however and this is particularly problematic with regard to the personality disorder diagnoses. This study sought to review the existing qualitative methods literature in relation to the experience of personal recovery in personality disorder.
Methods:
A systematic literature search was conducted. Identified studies were incorporated through meta-synthesis in order to develop higher order descriptive themes representative of the individual experience described within included studies.
Results:
Three studies were identified and incorporated into the meta-synthesis. Three novel higher order themes were developed: Safety and containment as a prerequisite to recovery, social networks and autonomy in the recovery process and identity construction as a process of change.
Conclusion:
Personal recovery in personality disorder is revealed as a complex process reflecting both personal and social experiences or desires. These findings have important implications for clinical practice – emphasising the need to work closely with individuals and to develop an understanding of both their social experience and networks. Further research, taking greater account of social context in the recovery process, is necessary.
Background
The support of personal recovery now represents a stated goal for many modern mental health services. The meaning of the term personal recovery is, however, complex and not always clearly defined (Pilgrim, 2008). With its origins in the deinstitutionalisation process of the United States, the idea of a recovery movement was adopted by mental health service users with an emphasis on personal empowerment, self expression and overcoming restrictions within social structures (Davidson, 2008; Deegan, 1996; Dillon, 2010). However, mental health services and professional bodies commonly cite descriptions of personal recovery as being more in keeping with a rehabilitative understanding, for example, living a satisfying life despite the limitations of illness (Anthony, 1993). The tension between these two positions has been described as understanding the distinction between descriptions of recovery from versus recovery in mental disorder (Davidson & Roe, 2007).
Despite these differences in position, most descriptions of personal recovery emphasise the idiographic nature of the process. Understanding the preferences of individuals seeking support in relation to mental distress is important as there is evidence that commonly used measures of clinical outcome do not match with the individual expectations of mental health service users (Andresen, Caputi, & Oades, 2010).
Research conducted considering the recovery experience of those with a mental disorder diagnosis has highlighted key themes of connectedness, hope, identity, meaning, empowerment and spirituality (Leamy, Bird, Le Boutillier, Williams, & Slade, 2011). This framework, developed by Leamy et al., emerged from the consideration of recovery narratives across a range of mental disorder diagnoses. However, they did not consider the specific experiences of those with personality disorder diagnoses where it can be argued that most of the pertinent themes they described may have been impacted upon in a chronic manner. This observation is important as longitudinal studies have demonstrated that while symptomatic remission occurs relatively commonly in those receiving a diagnosis of borderline personality disorder (BPD) longer term recovery, in terms of psychosocial functioning, is rarer (Zanarini, Frankenburg, Reich, & Fitzmaurice, 2012). Reviewing the development of new treatment interventions in the care of BPD, calls have been made for a greater focus on the clinical and research understanding of the concept of recovery in personality disorder to be developed (Nehls, 2000).
The concept of personal recovery in personality disorder is therefore not without problems and requires further research and clinical understanding. In order to address this concern, this study seeks to identify qualitative methods studies exploring the experience of personal recovery in personality disorder. While numerous quantitative methods studies exist exploring treatment outcomes in personality disorder, it can be argued that qualitative methods offer a valuable understanding of the personal recovery process from an idiographic perspective. In this manner, the concerns raised by Andresen, Caputi and Oades (2010) can be addressed. Such approaches also provide one means of addressing an identified research need to identify appropriate outcome measures as described in a recent publication by the UK-based National Institute for Health and Care Excellence (2009). For the purposes of this review, the term ‘personality disorder’ is used in place of any specific diagnostic term; it is argued that this is appropriate given concerns raised regarding existing classification systems and proposed changes to future classification (Frances & Nardo, 2013; Tyrer, Reed, & Crawford, 2015).
A literature search and meta-synthesis were therefore conducted with the aim of identifying existing qualitative research to allow the development of an adequate thematic map to outline findings in this area.
Methods
The review was registered prospectively with the PROSPERO database – reference CRD42013006839. This report is structured in keeping with guidance for enhancing transparency in reporting the synthesis of qualitative research (Tong, Flemming, McInnes, Oliver, & Craig, 2012).
Systematic search strategy
An electronic search strategy was adopted in order to identify studies meeting the following inclusion criteria:
English language publication
Peer reviewed publication with online access to full text
Qualitative methods approach with transparent representation of service user experience
Exclusion criteria included the following:
Purely clinical definition of recovery (e.g. change in symptom rating scale)
No presentation of service user experience (e.g. no access to primary source material through quotation)
Literature relating solely to recovery in substance use disorder
The following databases were accessed: EMBASE, Medline, PsycINFO, Applied and Complementary Medicine Database (AMED), Social Policy and Practice, Applied Social Science Index and Abstracts (ASSIA), British Humanities Index, Social Services Abstract, Sociological Abstracts and Sage publications. Search terms were adapted to meet the requirements of individual search engines but such that the overall semantic meaning was not altered. The following terms were used for the search:
Personality disorder AND recovery
Search outputs were imported directly into electronic reference manager software, which allowed for the removal of duplicate material (Papers 3 for Apple OS X, www.papersapp.com).
Review of titles and abstracts allowed exclusion of identified papers of clear irrelevance to the search strategy; editorial and opinion commentary pieces were also identified at this stage. Full-text versions of remaining hits were obtained and reviewed according to the inclusion and exclusion criteria defined above.
Reference lists of identified reports and editorial commentaries were also searched to broaden the search strategy.
Critical appraisal of identified papers
Included papers were reviewed according to the standard criteria set out by the Critical Appraisal Skills Programme (CASP – www.casp-uk.net). The application of standardised assessments to qualitative methods studies is complex, however, and risks limiting the value of the findings (Barbour, 2001). As such, the purpose of critical appraisal in this review was not to exclude papers on methodological grounds but to incorporate this review into the analysis process through further clarification of the methodology, limitations, rigour and setting for each study. Critical appraisal was led by A.S. with close discussion being held regularly with the remaining authors.
Meta-synthesis
Meta-synthesis allows the combination of qualitative methods studies in a manner so as to develop overarching, third-order, themes that develop further understanding grounded in the material of the included studies. For this synthesis, an approach analogous to that of meta-ethnography was employed (Noblit & Hare, 1988) that has previously been described by other authors (Britten et al., 2002). Guidance relating to the writing of meta-synthesis reports, such as that described by Tong et al. (2012), does not focus on the specific synthesis methodology and this report is presented in light of findings from critical review of meta-ethnography publications (France et al., 2014).
The synthesis process was conducted over five stages with the first two authors, A.S. and C.S., conducting the first three stages and all authors being involved in the remaining analysis stages:
Reading: studies were initially read and then separated in order that results and discussion sections of reports could be incorporated into the analysis process.
Study relationship: reading of identified reports allowed the initial identification and comparison of related material and themes.
Study translation: a descriptive coding method was adopted in order to allow translation of the included studies. First- and second-order themes were developed according to the tradition of Schutz (1962). First-order themes represented original participant understanding, in the form of quotations, while second-order themes represented original author interpretation of findings. Descriptive codes were applied in order to capture understanding of these themes. Codes were used across all studies in order to complete the translation process. Summary tables of coding first- and second-order themes were developed.
Synthesis of translations: understanding of first- and second-order themes was combined through further reading and author discussion in order to develop third-order themes as described by Britten et al. (2002).
Expression of synthesis: writing as a form of expression and analysis was incorporated into the final two stages of the analysis process (A. Coffey & Atkinson, 1996). An iterative approach to writing and discussion, involving all authors, was adopted to the expression of findings in this report.
Results and discussion
Identified studies and critical appraisal
Figure 1 summarises the search process. The initial search identified a total of 5510 hits – with 818 duplicate papers then being removed by electronic reference management software. Review of title and abstract alone allowed for exclusion of a further 4668 papers; therefore, full-text versions of 24 papers were retrieved. Application of the full inclusion and exclusion criteria led to exclusion of a further 21 papers. Reference list review yielded no additional papers but showed cross-referencing between the included papers. Reasons for exclusion of papers following full-text review included the following: case study presentation only, not focussed on the experience of those with a personality disorder diagnosis and representation of personal recovery through quantitative scale definitions only.
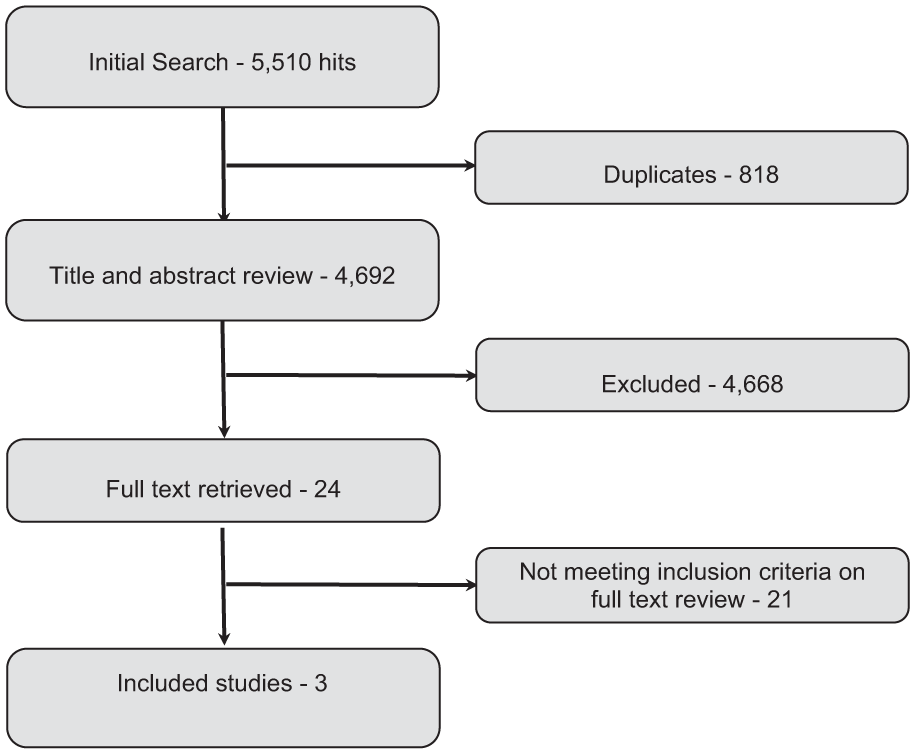
The search process.
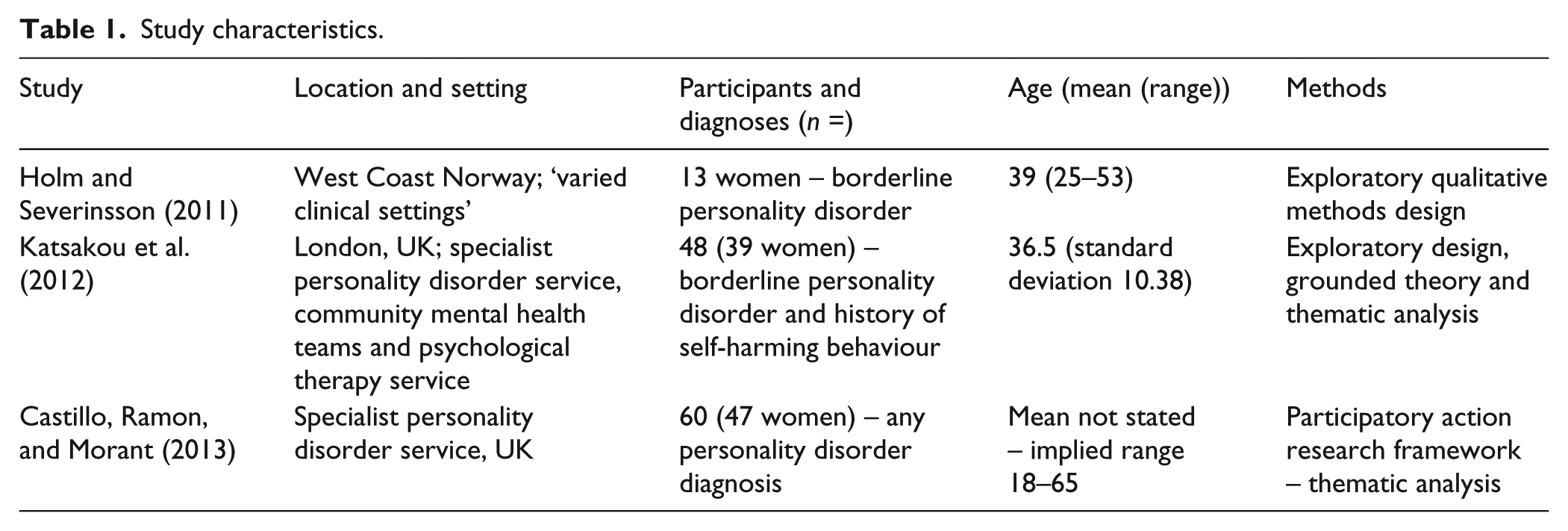
Three papers were therefore identified for inclusion in the meta-synthesis analysis (Castillo, Ramon, & Morant, 2013; Holm & Severinsson, 2011; Katsakou et al., 2012). Study characteristics are summarised in Table 1, and appraisal findings according to CASP criteria are shown in Table 2. The CASP statements, ‘Is a qualitative methodology appropriate’ and ‘How valuable is the Research’, are omitted from this appraisal.
Study characteristics.
Appraisal of included studies.
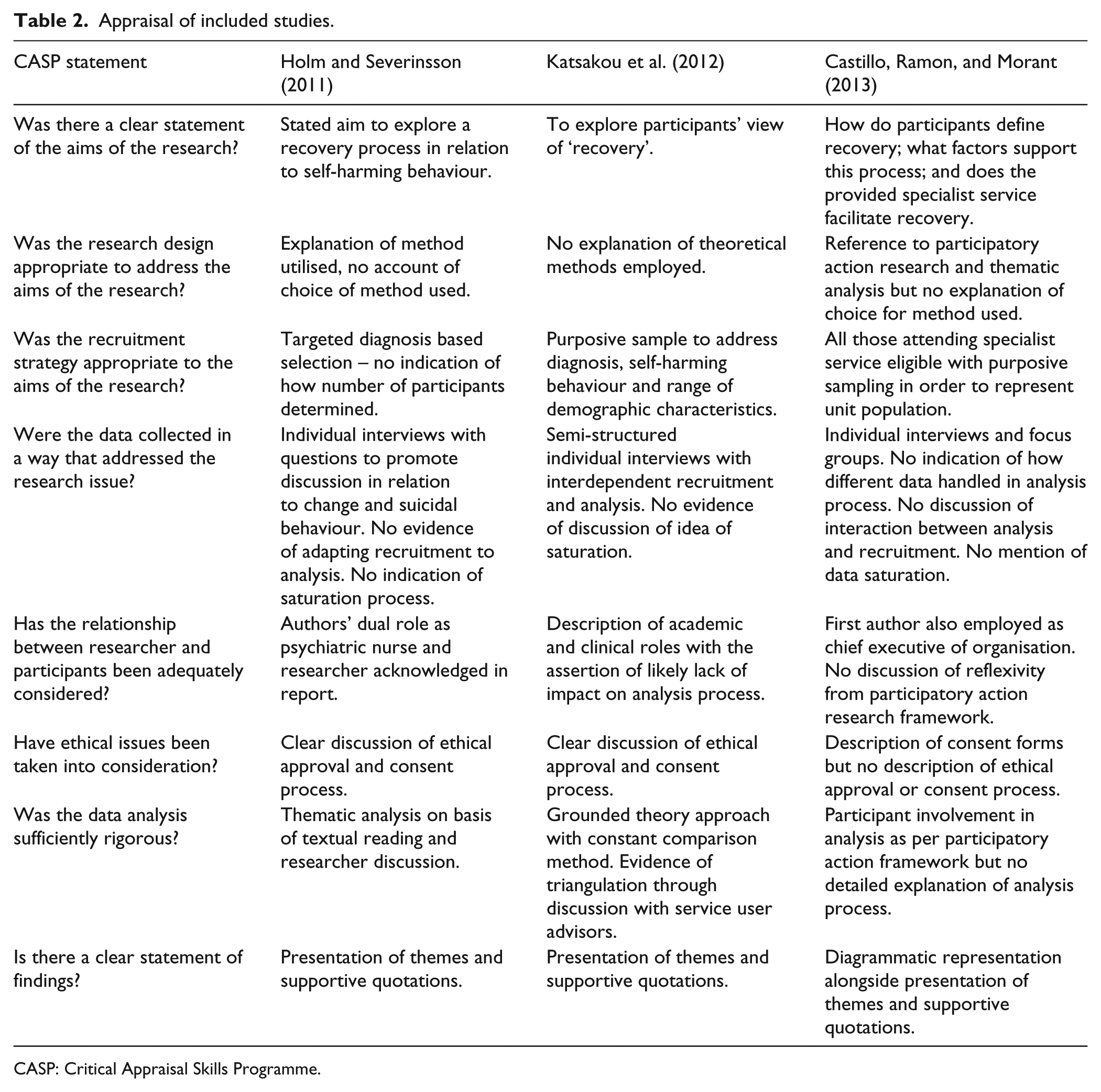
CASP: Critical Appraisal Skills Programme.
Overall, the findings from included studies were clearly represented. Theoretical considerations were given little description, however, in either the description of the research process or analysis. Clear incorporation of theory within qualitative research is essential to informing the reader’s interpretation of findings (Bradbury-Jones, Taylor, & Herber, 2014; Wu & Volker, 2009). Descriptions of possible reflexivity on the interview process and analysis were also limited – this may be particularly pertinent in the report by Castillo and colleagues where the role of service users in the analysis process was unclear (Macbeth, 2001). However, it should be acknowledged that further efforts in relation to reflexivity may have been undertaken but were omitted from published reports owing to reporting constraints.
Meta-synthesis
Synthesis findings are summarised in Table 3 and discussed in more detail below together with relevant existing literature in order to illustrate the context of findings. Illustrative first- and second-order themes are provided within Table 3 for each superordinate, third-order, heading.
Representation of meta-synthesis.
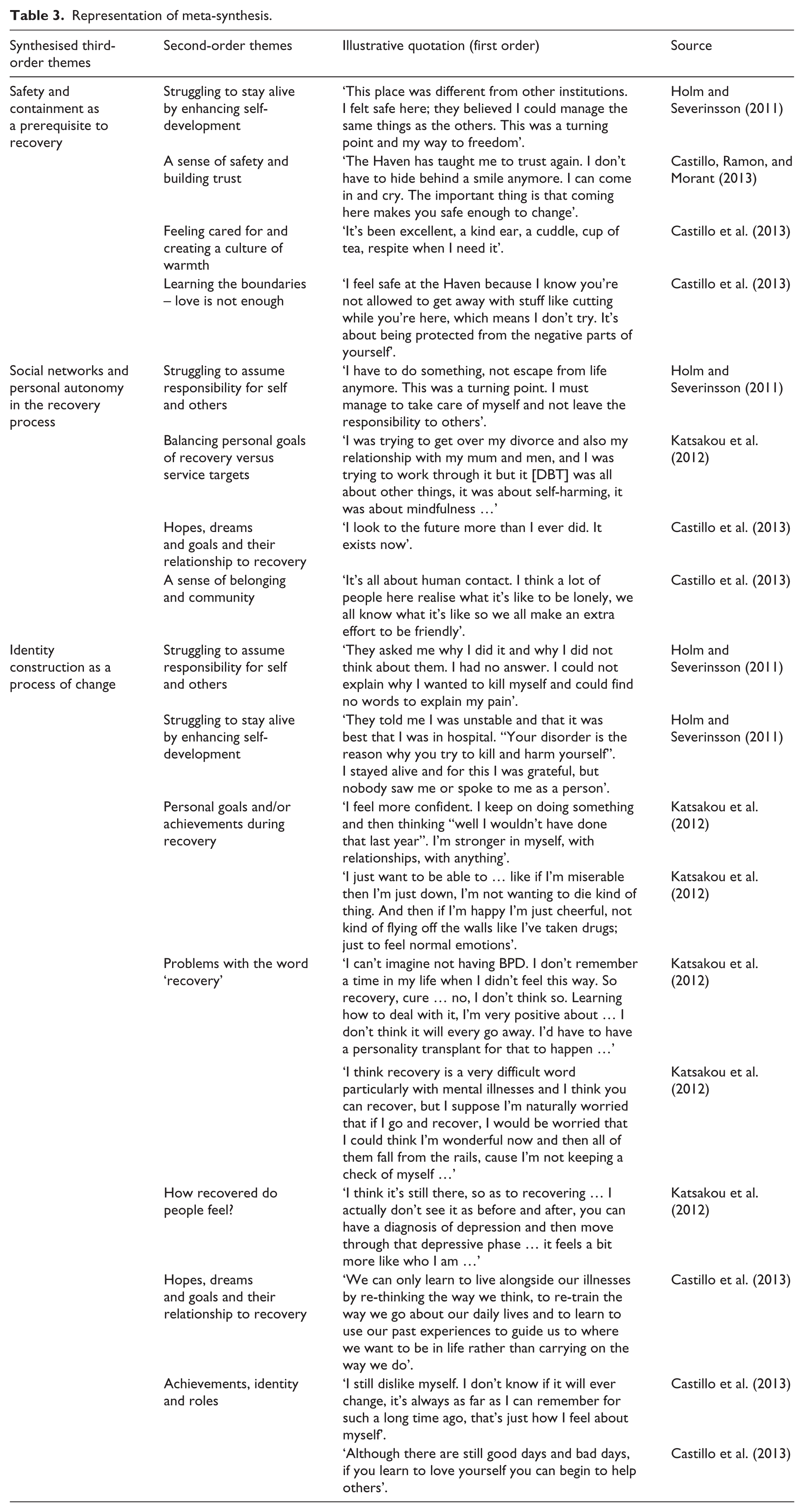
Safety and containment as a prerequisite to recovery
Participants described that in order for personal change to occur, it was necessary for them to feel safe, or contained, and that this allowed them to express their distress in a more manageable fashion. Such containment could be delivered through individual relationships (professional and peer), social networks or environments. This containment was described as being essential for the recovery process – with environments, or relationships with others, that were perceived as being toxic, or rejecting, leading to an impeding, or regression, in desired change.
This finding is in keeping with previous research literature that has emphasised the role of trusting therapeutic relationships as being essential in support of personal recovery (Adshead, 1998). Attachment theory (Bowlby, 2005) provides one means of understanding this phenomenon – by suggesting that during times of distress, individuals will seek out attachment sources, mirroring behaviour in early life. Fonagy and Luyten (2009) argue that BPD is characterised by a lowered threshold for activation of attachment behaviour, with accompanying loss of ‘mentalization’. As professionals also display varying attachment styles, the interaction between the professional and the individual seeking help is necessarily complex (Bucci, Seymour-Hyde, Harris, & Berry, 2015).
The idea of safety and containment, however, raises additional concern around the experience of leaving, or moving between, environments. This was described by participants in the identified studies with discharge or transfer being a point of care requiring particular care and attention. Transitions between clinical and community environments are recognised as being problematic with potential impact on the individual’s sense of personal identity – illustrating a potential overlap between this third-order theme and the idea of identity as a change process (M. Coffey, 2012).
Social networks and personal autonomy in the recovery process
Recovery was represented as a developing exercise of personal autonomy – with descriptions of ‘turning points’ wherein individuals recognised that change was necessary and took steps to secure this. In this manner, people were able to develop hope for future change. However, there was also a recognition that any change necessarily occurred within social spaces and would be influenced by others, for example, family members, significant relationships and professionals. There was also tension here, however, with participants in the study by Katsakou et al. describing difficulty with differences between their priorities and those of the mental health services – for example, with individuals wishing to address difficulties within personal relationships, while feeling that professionals instead focussed on domains related purely to risk, such as self-harming behaviour.
Social network support is known to play a key role within any change process. Perry and Pescosolido (2015) demonstrate that the strategic activation of social networks is a key component in help-seeking behaviour in response to distress; furthermore, they describe how activation of stronger ties, or ties with others who display a pro-healthcare orientation, results in more profound and lasting changes over time (Perry & Pescosolido, 2015). Cohen and Wills (1985) suggest that social networks may have both direct and indirect effects on the experience of distress – allowing improved response to disorder but also providing a buffering effect against social stress. Social network support for individuals with experience of mental distress tends to be less than that for individuals with physical illness, however – with individuals receiving a diagnosis of schizoaffective disorder reporting less satisfaction with and lower perceived support from social networks than individuals with a diagnosis of diabetes (Nettelbladt, Svensson, Serin, & Öjehagen, 1995). This disruption of social network support may also expand to the family members of individuals with mental disorder diagnoses (Magliano, Fiorillo, Malangone, De Rosa, & Maj, 2006). Stigma in relation to experiences of mental distress are also likely significant here and may result in marginalisation of individuals from family and professional support (Bonnington & Rose, 2014).
Identity construction as a process of change
Identity construction appeared to be central to the experience of personal recovery in each of the identified studies. Participants described a process of ‘identity work’ – that is, the manner in which experience is incorporated into the sense of self alongside other competing identities (Adams, Pill, & Jones, 1997). For some, this involved the complex task of working to understand previous acts, or behaviours, and to make sense of these experiences. This could involve the adoption of an ‘illness identity’ to account for their experience – however, others described the stigmatising effect of this pathologisation of their behaviours, an experience that may be particularly pertinent in relation to help seeking for those with a personality disorder diagnosis (Bonnington & Rose, 2014). Recovery then became about moving beyond this state and developing hope for a future identity – a stronger, more confident, self or one who was simply able to experience ‘normal’ emotion. This process was complicated, however, with participants expressing difficulty with the idea that one could ‘recover from’ personality disorder – instead suggesting that this would become a permanent facet of their identity and that a guard should be maintained against destructive, or self-injurious behaviour.
The manner in which individuals manage experiences of distress and the resultant narratives they construct are known to have lasting influence for the individual’s sense of self, or identity (Crossley, 2000). Such narrative identities can also be seen as being performative in nature informed by both the audience and individual, emphasising again the role of social networks in the recovery process and providing a link between the second and third overarching themes described in this report (Riessman, 2003). Thoits (1985) hypothesises that individuals may ‘self-label’ in response to distressing experiences and behaviours and that this leads to help-seeking behaviours. However, such labelling of individuals, either by the self or others, may also act as a barrier to change and engagement with services, possibly raising concerns about the firm manner in which some individuals incorporated the identity of ‘disorder’ into their sense of self (Scott, 1973a, 1973b). Adler and colleagues (2008, 2012), working with individuals who had received psychotherapy, identified that the manner in which an individual incorporates his or her understanding of therapy and distress into a personal narrative can have implications for on-going psychological health (Adler, 2012; Adler, Skalina & McAdams 2008).
Conclusion
This article aimed to review the existing qualitative literature relating to personal recovery in personality disorder and develop a thematic map representing the material identified. Three overarching and interdependent themes were synthesised. These themes show some overlap with existing recovery frameworks (Leamy et al., 2011) but also display unique properties indicative of the distinct experiences and difficulties faced by those receiving a personality disorder diagnosis. The focus of each of the identified themes represents domains of function likely to be particularly disrupted, or complicated, in this population. These findings may also echo previous research (Andresen et al., 2010) in demonstrating the inadequacy of many outcome measures used in clinical practice and research in relation to personality disorder diagnoses – focus on symptomatic rating does not appear to be sufficient in representing the recovery process. This is also in keeping with the findings of longitudinal studies, described above (Zanarini et al., 2012), which demonstrate that while ‘symptom remission’ is not uncommon in individuals with a diagnosis of BPD, lasting psychosocial recovery is rare. One possible alternative approach, acknowledging these tensions, is the adoption of tailored measures that seek to adequately capture personal meaning with regard to quality of life and to allow interventions to be adapted to meet personally significant aims (Wallcraft, 2011).
Limitations
The greatest limitation of this report is the small number of identified substrate studies for inclusion in the meta-synthesis. Further research is indicated to assess these themes in more detail and in different social settings. The included studies were of good methodological quality; however, little attention was apparently given to reflexive issues during the data collection and analysis process. Theoretical influences on the analysis process similarly receive little description. Given the relationship of findings in this report to ideas of personal identity and the complexities of working with individuals with experience of personal mental distress, these domains should receive greater consideration in future work.
Each of the identified studies was conducted within a general community setting. However personality disorder diagnoses are represented with differing prevalences in different social settings; for example, prevalence rates in forensic populations are recognised as being particularly high (Fazel & Danesh, 2002). The social setting may therefore require further consideration in future studies.
Much of the existing published academic literature in the study of personality disorder relates specifically to the experience of those receiving a diagnosis of BPD, and two of the three studies in this review similarly focussed on this diagnosis. This imbalance in the research base also needs to be addressed in future studies (Bateman, Gunderson, & Mulder, 2015).
Issues of reflexivity in the current analysis were addressed through involvement of a multidisciplinary research team throughout the analysis process. Regular research meetings were held with discussion of emergent themes, and the incorporation of an iterative writing process allowed further exploration of themes. The analysis was grounded within a contextual constructionist epistemology – that the experience of phenomena is determined by interactions between the research participant, researcher and other audiences (Madill, Jordan, & Shirley, 2000). Triangulation of findings was considered through research meetings and sensitisation to the existing theoretical literature with developing theoretical understanding through further literature reading in the light of synthesis findings.
Implications and future work
The findings have implications for both clinical practice and research. From a clinical perspective, there is evidence that interventions offered by mental health services do not fully address the needs of individuals with a personality disorder diagnosis. By focussing on the domains identified in these recovery narratives, services will better be able to meet the needs of these people. Support of interpersonal relationships with both professionals and non-professionals appears crucial to providing the sense of safety necessary before identity work may occur. The interplay between professional and client attachment style may also have to be taken into consideration. The demands of such relationships on professionals are well recognised and services may be required to adopt close supervision facilities, if these are not currently available, in order that clinical staff may better continue to fulfil their roles (Adshead, 1998). A review of outcome measures to allow identification of those most closely aligned with domains of significance to personal recovery is also necessary.
Further qualitative research studies, paying particular attention to issues of reflexivity, are necessary to address the small number of studies directly addressing the experiences of individuals in receipt of a personality disorder diagnosis. Given the implication of social networks and spaces in the recovery process, these studies should also seek to review the experiences of individuals within a variety of social settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Andrew Shepherd receives funding from the NIHR in the form of a doctoral research fellowship award. The views represented here are those of the authors and not necessarily representative of the NIHR, NHS or the Department of Health, UK.