
Abstract
Background:
Currently, the number of natural disasters has increased sixfold when compared to the 1960s. The 2004 Indian Ocean Tsunami offered provided an opportunity for scientifically investigating the effectiveness of post-disaster programs across countries with diverse ethnic, religious and cultural backgrounds.
Aim:
This study aimed to assess the effectiveness of psychological interventions focused on the prevention or reduction in post-traumatic stress disorder (PTSD) symptoms and/or enhancement of psychological well-being implemented after the 2004 Tsunami.
Methods:
We systematically searched through MEDLINE, PsycINFO and The Published International Literature on Traumatic Stress (PILOTS) databases using the following keywords: ‘tsunami’ OR ‘Indian Ocean’, AND ‘intervention’.
Results:
Our systematic review included 10 studies which adopted 10 different psychological interventions. A total of 8 of the 10 studies reported positive results in reducing PTSD symptoms and most interventions showed high levels of cultural sensitivity. No significant harmful effects of the included interventions were identified although two studies used potentially harmful interventions.
Conclusion:
Evidence-based practice is a process of collaborative decision-making between the affected ones and interventionists. The practitioner assesses not only the availability of the level of evidence of the preferred interventions, but he or she also assesses his or her own expertise, the availability of resources, the surrounding context and the characteristics, values and preferences of relevant stakeholders.
Introduction
The Indian Ocean Tsunami happened on 26 December 2004 was estimated to have led to 274,000 casualties across 18 countries (Ramalanjaona, 2011), and the damages caused approximately amount to US$9.9 billion (Merlot & Cieri, 2012). In addition to the mass casualties and destruction of property, natural disasters can have a devastating impact on the psychological well-being of affected individuals (Carballo, Heal, & Hernandez, 2005; Math et al., 2008). Post-traumatic stress disorder (PTSD) is one of the most common psychiatric disorders observed among tsunami survivors. Review studies suggest that rates of PTSD after a disaster can range from 5% to 60% (Galea, Nandi, & Vlahov, 2005; Neria, Nandi, & Galea, 2008). Studies that specifically examined the impacts of the Indian Ocean Tsunami among Asians found that 14%–39% of children in Sri Lanka (Neuner, Schauer, Catani, Ruf, & Elbert, 2006), 11% of children in Thailand in affected villages (Thienkrua et al., 2006) and 12% of displaced adults in Thailand (Griensven et al., 2006) experienced PTSD symptoms after the Tsunami.
Although it has become a common reactionary strategy to provide psychosocial interventions to affected individuals (Palic & Elklit, 2011), the effectiveness of psychological interventions in reducing PTSD symptoms or promoting resilience among the affected Asian population is uncertain. Critics of these interventions caution that they may cause harm because (1) the use of Western-centric interventions were not adapted to the target populations’ religious traditions and cultural differences (Newport & Padma, 2007) and (2) the interventions were not implemented by qualified practitioners (Raphael & Meldrum, 1995). This study aimed to assess the efficacies or effectiveness of psychological interventions for the prevention or reduction in PTSD symptoms and/or enhancement of psychological well-being implemented after the Indian Ocean Tsunami.
The research questions of this study are as follows: (1) What were the efficacies of reported psychological interventions in reducing PTSD symptoms and/or enhancement of psychological well-being implemented after the Tsunami? (2) Were the psychosocial interventions carried out with rigorous or sound study designs? (3) Did the interventions cause harm to the study participants? And (4) Were the trials conducted in a culturally sensitive manner that accounted for the ethnic and cultural diversity in the target population of the studies?
Methods
Search strategy
Three major academic databases were systematically searched including MEDLINE, PsycINFO and The Published International Literature on Traumatic Stress (PILOTS) Database. The following keywords were used to identify peer-reviewed literature, namely, ‘tsunami’ OR ‘Indian Ocean’, AND ‘intervention’. The last search was conducted in July 2014. Full texts of all potentially relevant studies were assessed to see whether they met the inclusion criteria. To ensure a comprehensive search strategy, reference lists of included articles and Google Scholar were hand-searched for gray literature that might not have included in the searched academic databases.
Selection criteria
All post-tsunami psychosocial interventions that were provided to affected individuals were selected for review based on the following inclusion criteria: (1) evaluation utilized a pre- and-post-test methodology, (2) evaluations of the main outcomes including PTSD and psychological well-being using quantitative assessment tools, (3) study participants were non-Western populations and (4) published in English before June 2014.
The details of the selection procedure are displayed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher, Liberati, Tetzlaff, & Altman, 2009; see Figure 1).
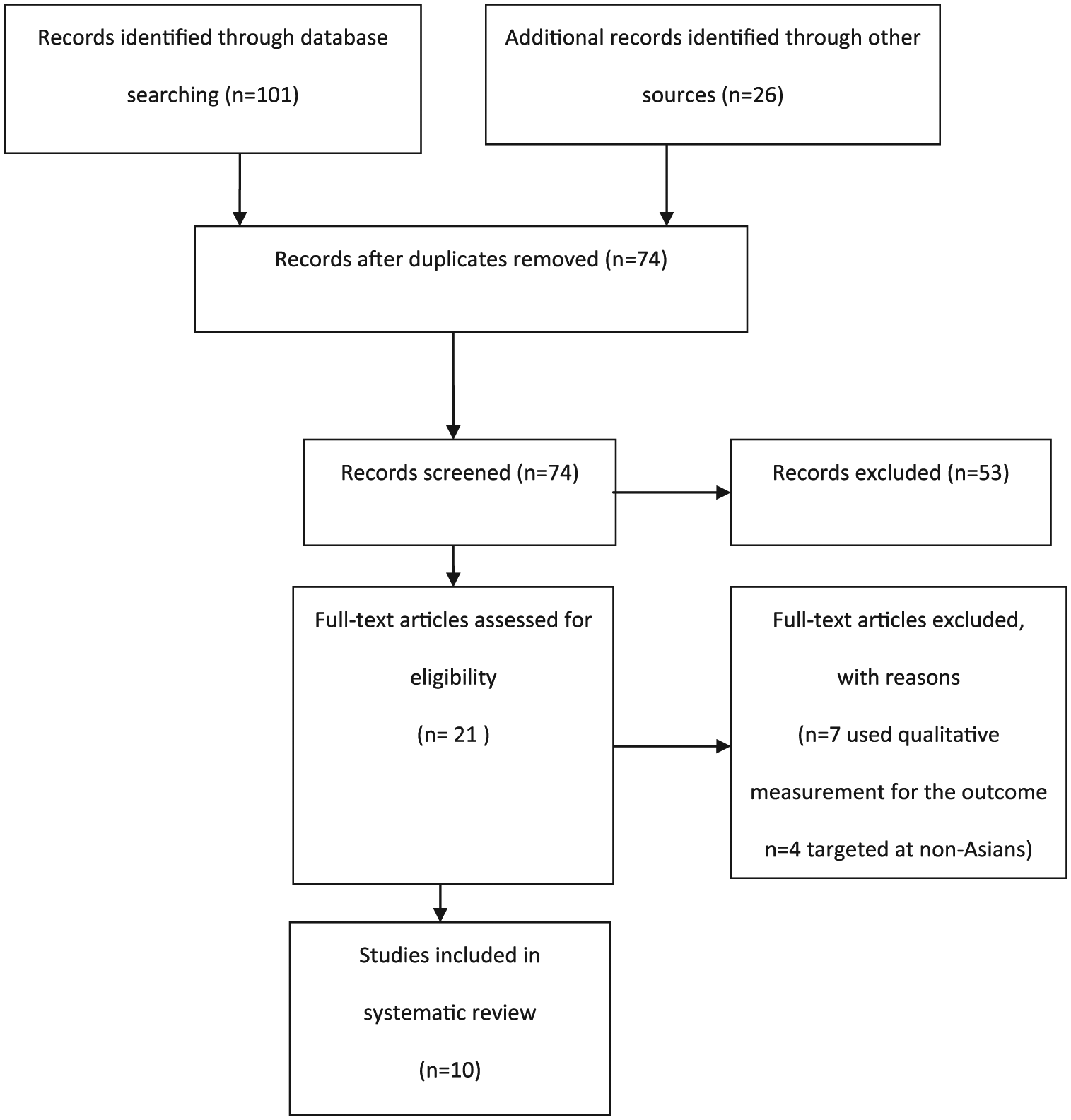
PRISMA flow diagram of identification and final selection of included studies in this review.
Data extraction strategy, study evaluation and quality assessment
To assess the quality of the included trials, Downs and Black’s (1998) Quality Index was used. We acknowledge that many systematic reviews used the Consolidated Standards of Reporting Trials (CONSORT) to assess study quality. However, Downs and Black’s Quality Index was designed to assess a variety of study designs, whereas the CONSORT only evaluates randomized controlled trials. A numerical score was given to each included study (see Table 1). K.L. and P.W.C.W. assessed each study independently and their scores were compared and agreed upon. Studies were also evaluated on the number of follow-up assessments, the listing of previous applications of the study, their effect size and the statistical significance of their results.
Descriptions of included studies and the evaluation of their details.
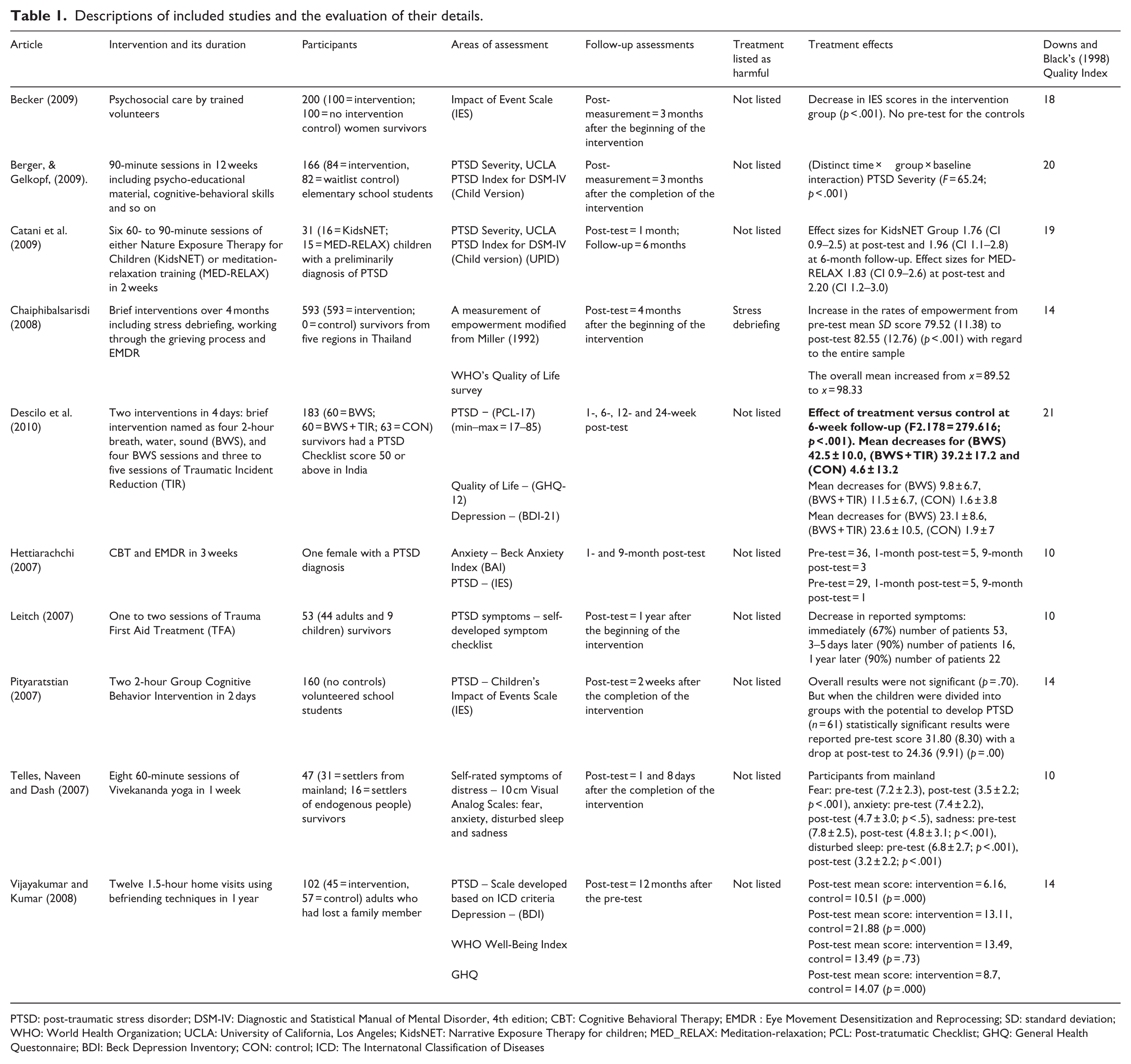
PTSD: post-traumatic stress disorder; DSM-IV: Diagnostic and Statistical Manual of Mental Disorder, 4th edition; CBT: Cognitive Behavioral Therapy; EMDR : Eye Movement Desensitization and Reprocessing; SD: standard deviation; WHO: World Health Organization; UCLA: University of California, Los Angeles; KidsNET: Narrative Exposure Therapy for children; MED_RELAX: Meditation-relaxation; PCL: Post-tratumatic Checklist; GHQ: General Health Questonnaire; BDI: Beck Depression Inventory; CON: control; ICD: The Internatonal Classification of Diseases
To address the concerns whether interventions were harmful (Tharyan, Clarke, & Green, 2005), first, the concept of harm, in this article, is understood based on Boisvert’s (2003) definition, which concludes a treatment can be considered harmful if a client experiences (1) symptom worsening, (2) appearance of new symptoms, (3) heightened concern regarding extant symptoms and (4) reluctance to seek future treatment. Authors of this study assessed the presence of harm of the reviewed studies according to the four components as suggested by Boisvert (2003). Second, we cross-checked the reviewed studies with the list of potentially harmful psychological interventions generated using a Delphi study methodology developed by Lilienfeld (2007).
To evaluate the ethical and cultural sensitivity of included studies, the content process, cultural considerations, ethics approval, employed volunteers or professionals and mentioned potential harmful effect to the participants were reviewed. These aspects of the studies were chosen based on critiques of interventions proposed by Wickramage (2006) and Galappatti (2005), who stated that intervention models clashed with traditional values of the community and were often poorly coordinated and resulted in confusion among survivors.
Results
Selection of studies
The search yielded 127 records from the databases. A total of 26 records were further identified by a hand search. After the removal of duplicates and the application of inclusion and exclusion criteria on abstracts, 21 full-text articles were examined for eligibility. Eleven studies were excluded because seven studies conducted on local population utilized qualitative measures of assessment; four studies targeted non-Asians that consisted of Norwegians, Swiss or Czech tourists. Therefore, a total of 10 studies were included for the review (see Table 1).
Descriptions of studies
The type of interventions, number of participants, measurements used and treatment effect of the included studies are summarized in Table 1. All the interventions were provided to both children and adults mostly about within 6 months after the tsunami. Four interventions were conducted in villages and homes in India, respectively (Becker, 2009; Descilo et al., 2010; Telles, Naveen, & Dash, 2007; Vijayakumar & Kumar, 2008), three in schools, refugee camp and a village clinic in Sri Lanka, respectively (Berger & Gelkopf, 2009; Catani et al., 2009; Hettiarachchi, 2007), and three in villages, refugee camp and schools in Thailand, respectively (Chaiphibalsarisdi, 2008; Leitch, 2007; Pityaratstian et al., 2007). Among the 10 studies, there was one quasi-randomized controlled trial (Berger & Gelkopf, 2009), three quasi-experimental design studies (Becker, 2009; Chaiphibalsarisdi, 2008; Vijayakumar & Kumar, 2008), five pre-/post-test design uncontrolled studies (Catani et al., 2009; Descilo et al., 2010; Leitch, 2007; Pityaratstian et al., 2007; Telles et al., 2007) and a single case study of a female survivor (Hettiarachchi, 2007).
The reviewed studies included 10 different intervention modalities: (1) psychosocial care (Becker, 2009); (2) mixed psycho-educational, cognitive-behavioral skills, art therapy and narrative therapy (Berger & Gelkopf, 2009); (3) narrative exposure therapy and meditation-relaxation training (Catani et al., 2009); (4) mixed stress debriefing, crisis intervention and eye movement desensitization and reprocessing (EMDR; Chaiphibalsarisdi, 2008); (5) brief intervention and traumatic incident (Descilo et al., 2010); (6) cognitive behavioral therapy (CBT) and EMDR (Hettiarachchi, 2007); (7) somatic experiencing/trauma first aid treatment (Leitch, 2007); (8) group CBT (Pityaratstian et al., 2007); (9) yoga (Telles et al., 2007); and (10) home visit befriending (Vijayakumar & Kumar, 2008) (see Table 1).
The 10 different interventions were delivered by trained community health workers (Becker, 2009), trained teachers (Berger & Gelkopf, 2009), not mentioned (Chaiphibalsarisdi, 2008), female counselors (Catani et al., 2009), specialists (Descilo et al., 2010), clinical psychologist (Hettiarachchi, 2007), trained volunteers with the presence of translators (Leitch, 2007), mental health professionals (Pityaratstian et al., 2007), yoga teacher (Telles et al., 2007) and experienced volunteers (Vijayakumar & Kumar, 2008) (see Table 2).
Ethical and cultural sensitivity of included studies.
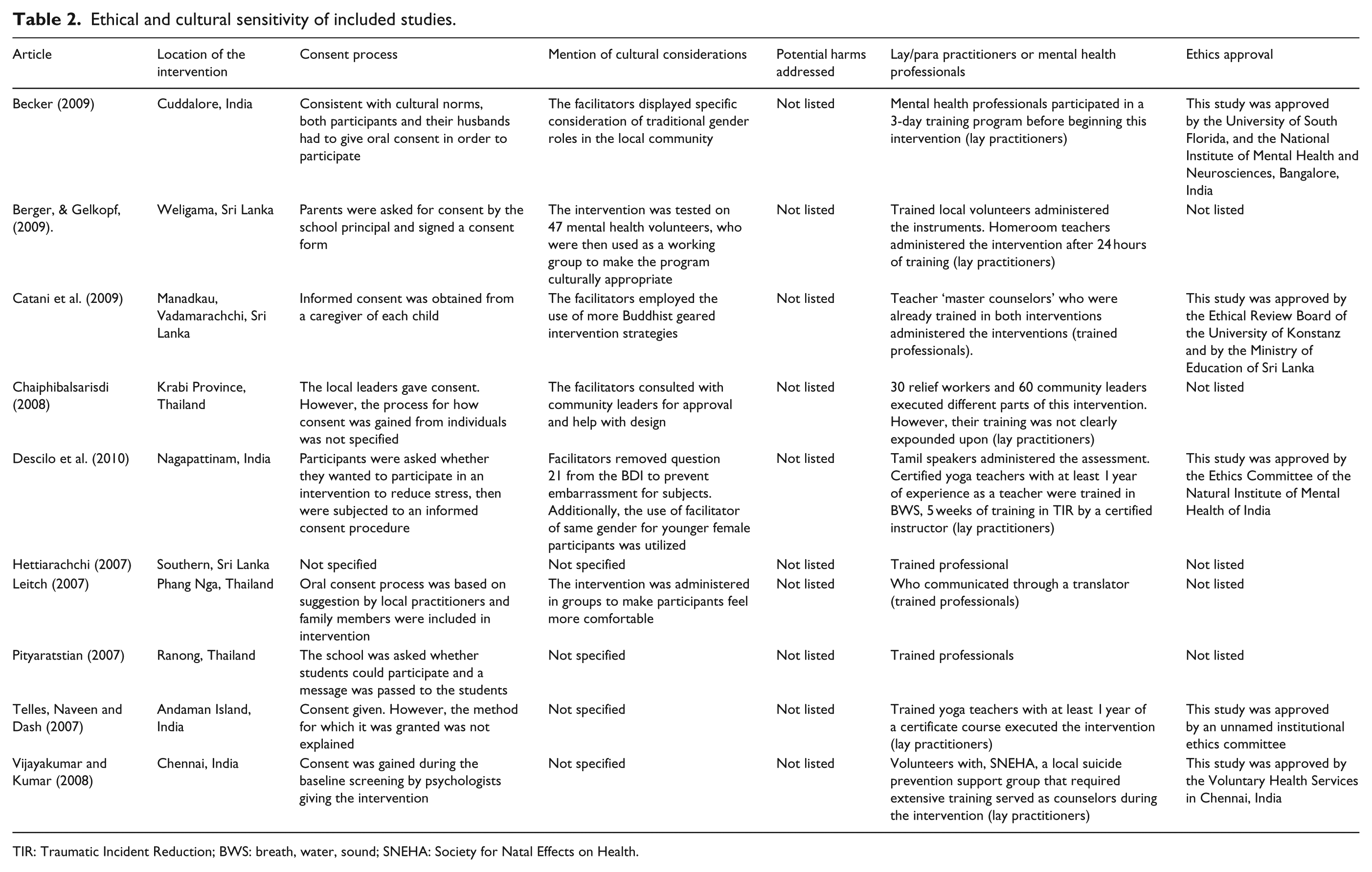
TIR: Traumatic Incident Reduction; BWS: breath, water, sound; SNEHA: Society for Natal Effects on Health.
Quality of included studies – Downs and Black’s index scores
The methodological quality of the included studies varied possibly due to the difficulties in conducting studies with rigorous experimental research designs in transient settings such as refugee camps. Most studies reported information on aims/hypothesis, outcome measures and detailed descriptions of the evaluated interventions. Half of the studies did not have comparison groups, and the majority had short pre-/post-test interval. Only one study adopted a randomization methodology. None reported any adverse events.
The efficacies of the included trials
Reduction in PTSD symptoms
As reported in Table 1, eight studies found positive results in reducing PTSD symptoms at the post-evaluation periods. Berger and Gelkopf (2009) reported their school-based intervention produced statistically significant results and the percentage of students with potential PTSD dropped from 33% to 6%. Descilo et al. (2010) found statistically significant results between both of their treatment groups and the wait-list control on PTSD outcomes. Vijayakumar and Kumar’s (2008) befriending intervention helped lowering scores on the BDI and a PTSD assessment based on International Classification of Diseases (ICD) criteria when compared to a control group. Telles et al.’s (2007) yoga intervention reduced somatic and emotional symptoms at a statistically significant level compared with the control group. Becker (2009) found that a 3-month biweekly group intervention was able to statistically significantly reduce Indian women’s scores on the Impact of Event Scale compared with the control group. Leitch (2007) reported that 90% of participants reported improved symptoms 12 months after the intervention. Catani et al.’s (2009) meditation-relaxation training (MED-RELAX) and KidsNET intervention groups both displayed a decrease in PTSD symptoms after the intervention. There were no reported significant differences between the two groups’ results with regards to decreased displays of PTSD symptoms. Although the study lacked a control group, the intervention team believed their population displayed higher rates of recovery than could be accounted for by natural recovery alone due to the intervention. Children in their intervention groups at the 6-month post-test were found to meet the diagnostic criteria for PTSD at a rate of 19% and 29%, respectively.
Improvement in psychological well-being
Four studies found improvement in hope (Berger & Gelkopf, 2009), quality of life (Chaiphibalsarisdi, 2008), physical and psychological health (Descilo et al., 2010) and mental health (Vijayakumar & Kumar, 2008) at the post-measurement period.
Use of potentially proven harmful techniques
Two studies could be considered as harmful techniques using the four components as suggested by Boisvert (2003). Pityaratstian et al. (2007) reported after their intervention, children who initially did not meet the diagnostic criteria for PTSD measured by the Children’s Impact of Event Scale displayed a statistically significant increase in reported PTSD symptoms in the post-test measure. However, the intervention for children who met diagnostic criteria for PTSD during the baseline screening experienced a statistically significant decrease in PTSD rate. Another study evaluating the ability of psychosocial social interventions to raise feelings of empowerment conducted by Chaiphibalsarisdi (2008) produced both positive and negative post-intervention scores. The overall sample showed a statistically significant increase in empowerment. However, one group showed a decrease in empowerment scores.
One study adopted an intervention that has been suggested to have potential harmful effects (Lilienfeld, 2007). Chaiphibalsarisdi (2008) used stress debriefing techniques as part of the intervention in the study, whereas studies have found that individuals aided with stress debriefing showed higher rates of PTSD symptoms than the untreated control groups (McNally, Bryant, & Ehlers, 2003; Mayou, Ehlers, & Hobbs, 2000; Rose, Bisson, & Wessely, 2002).
Specifically, five studies did not report whether their studies had been piloted before the actual trials. Two studies adapted their interventions based on previous experiences working within the target population’s culture (Becker, 2009; Berger & Gelkopf, 2009). Three studies used interventions that had been previously tested outside of the target population’s culture (Catani et al., 2009; Hettiarachchi, 2007; Leitch, 2007).
Cultural sensitivity of the included studies
It was found that the 10 included trials had high levels of cultural sensitivity. However, the authors had a number of concerns about the reviewed studies. Five studies did not mention whether their interventions were ethically approved from an institutional review board. Three studies did not state the consent process. Hettiarachchi (2007) did not list if the subject, who was a client at the clinic, consented to be part of the research as well as the intervention process. Pityaratstian et al. (2007) reported talking to school officials but not guardians of the children. Chaiphibalsarisdi (2008) reported researchers consulted a local resource team but not how they gained consent from individual participants. Four studies worked to incorporate cultural norms into the consent process; this consisted of gathering the consent of family members, even if the target participant was not a child. Becker (2009) only accepted participants whose husbands consented in their intervention.
Discussion
‘Do no harm’ is an essential criterion of any evidence-based practices across all helping professions. This review was inspired by recent scientific queries that questioned the ethics and efficacy of interventions implemented after the Indian Ocean Tsunami in 2004. First, this article found that 9 out of the 10 included studies reported positive effect on the reduction in PTSD symptoms among the participants after the intervention, the quality of the studies varied and the majority adopted a less rigorous research methodology, that is, lack of control comparisons. Therefore, improvements in participants’ scores due to natural recovery cannot be fully discounted. Second, no particular interventions reported adverse events happened during the study. But according to the definition of harm adopted in this study, three interventions could be considered as potentially harmful. Third, contrary to some critics that interventions implemented in the Tsunami were conducted in a culturally incompetent manner, it was found that the included studies showed high level of cultural competency. In particular, lay practitioners in all the studies had outside training in the field in which they were administering care prior to the Tsunami. With regard to adapting to cultural practices, three studies used meditation and yoga-based practices (Catani et al., 2009; Leitch, 2007; Telles et al., 2007) to enhance the cultural competency of their interventions which is consistent with recommendations from British Psychological Society’s psychological first aid recommendations.
Limitations
One major limitation of this review is the narrow range of publications being identified in the literature. The inclusion criteria that only studies published in English would be selected further limited the number of qualified publications. During the search process, at least three studies published in the local languages were identified but excluded from this review. Conclusions in this study are also restricted by the lack of consistency in the assessment instruments. Hence, the generalization of the findings of the study is undermined by the small number of participants included in the review, the large variations of interventions and scales of the reviewed interventions.
Conclusion
When people affected by tsunami are asked what their major concerns are after a disaster and they reported that were ‘job loss, loss of property and status, and difficulty in performing religious rituals’ (Fernando, 2005). Accessing psychological services did not seem to be one of their major immediate concerns. Needs identified and desired by survivors should be prioritized. When basic needs are attended to first, if resources are available, there is time for the development and the implementation of high quality and culturally competent psychosocial interventions on a grass roots level.
Evidence-based practice is a process of collaborative decision-making between those who may be affected by the behavioral health decision, for example, individuals, families, organizations and communities. The practitioner assesses not only the availability of the level of evidence of the preferred interventions, he or she also assesses his or her own expertise, the availability of resources, the surrounding context and the characteristics, values and preferences of relevant stakeholders, especially the ones who are in need. Hence, it appears to be too simplistic to state that post-disaster relief efforts should only support interventions supported by strong scientific evidence with regard to their efficacy. This review is cognizant of the complexity of that statement as well as the realistic difference between theory and real-life practice in post-disaster situations.
While recognizing the complex obstacles faced by volunteers and mental health practitioners in these scenarios, we propose that there is at least one way to cultivate better and more ethical interventions through the act of asking for service and study participation consent. For instance, Citraningtyas, Macdonald, and Herrman (2010) gave an example of cultural clashes between aid workers and parents of children receiving aid interventions. In Aceh, Indonesia, aid workers felt that play-based activities should be a priority for child survivors of the tsunami. Parents, however, wished for their children to take solace in religion through studying the Quran each afternoon, resulting in conflict. This conflict could have been avoided through ensuring that parents were given the opportunity to give their full and informed consent and an opportunity to help design interventions aimed at targeting their children. Silove and Zwi (2005) state that the greatest intervention that can be given to survivors is to allow them to be ‘[the] architects of their own psychological recovery’ (p. 269). Therefore, it is our duty as scientific practitioners as well as practicing scientists to fully empower individuals to take charge of their mental health and decide whether they would like to participate in interventions once they have been given all the information, including what potential harm could come from their participation and non-participation.
Footnotes
Acknowledgements
The authors would like to thank Aviv Itkin, Zoe Lukens, Sarah Briedenbach and Joshua Wolper for their help in editing this document.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.