
Abstract
Background:
In general populations, consistent data highlight the relationships among violence, HIV risk behavior and depression; however, these patterns are not well understood among female sex workers (FSWs). We examined the relationship between FSWs’ experiences with sexual violence and consistent condom use as a key HIV risk behavior and explored mental health as a potential mediator.
Methods:
In total, 2,165 FSWs were recruited via respondent-driven sampling in Cameroon in 2016. The women answered questions about violence, condom use and mental health.
Results:
Inconsistent condom use with clients was reported by 23.5% of participants (508/2,165). Lifetime sexual violence was prevalent with 33.0% (713/2,163) of participants. Almost 50% (1,067/2,143) of respondents had some level of depression. Sexual violence was significantly associated with inconsistent condom use (adjusted risk ratio (aRR) 1.4, 95% confidence interval (CI) (1.2–1.6)). Of FSWs with no depression, 24.9% (267/1,071) reported sexual violence, versus 56.1% (32/57) of respondents with severe depression (p < .01). Severe depression significantly increased risk of condomless sex (aRR 1.8, 95% CI (1.3–2.6)); in mediation analysis, both sexual violence and severe depression remained significant predictors of condomless sex (aRR 1.4, 95% CI (1.2, 1.6) and aRR 1.7, 95% CI (1.2–2.4), respectively). Depression did not mediate the relationship between sexual violence and condom use.
Conclusion:
Sexual violence and depression are prevalent and independently associated with condom nonuse with clients among FSWs in Cameroon. Results highlight the need for interventions to address mental health as well as gender-based violence for FSWs.
Introduction
Gender-based violence (GBV), defined as ‘a harmful threat directed at any group or individual based on actual or perceived sex, gender identity and/or expression, sexual orientation, and or lack of adherence to varying socially constructed norms’, is pervasive globally (U.S. Agency for International Development (USAID), 2012). GBV includes physical and sexual violence, economic deprivation, threats, blackmail and psychological abuse (U.S. USAID & U.S. Department of State, 2016). Several decades of research on GBV have enabled an understanding of how GBV fuels health inequalities and perpetuates power dynamics that leave women marginalized (Shannon, Goldenberg, Deering, & Strathdee, 2014).
Disparate power dynamics leave certain groups of women at higher risk of GBV. Female sex workers (FSWs), in particular, report significantly higher rates of GBV than other women, for reasons including social norms, increased exposure to violent partners and lack of support services (Coetzee, Gray, & Jewkes, 2017). GBV is a symptom of gender inequities and is associated with heightened health risks and vulnerabilities among FSWs who report high rates of GBV by clients, partners and state actors (Deering et al., 2013; Lyons et al., 2017). In addition to being a human rights violation, experiences of GBV have been shown to increase risk and transmission of HIV (Lim et al., 2015). Despite declines in HIV rates in the countries most affected by the HIV pandemic, HIV remains concentrated among FSWs (Baral et al., 2012; Lancaster, Cernigliaro, Zulliger, & Fleming, 2016; MacAllister et al., 2015). A 2012 study determined that FSWs in low- and middle-income countries have a 13.5-times increased odds of HIV compared to all women of reproductive age (Baral et al., 2012). This increased HIV burden as both a cause and symptom of the inequalities inherent in the lives of FSWs and is perpetuated by individual, network and structural factors (Decker et al., 2015; Decker et al., 2013). Condom use has been shown to consistently impact rates of HIV prevalence and incidence among both FSW and non-FSW populations (Williams et al., 2014). While condom use may be a direct barrier to HIV transmission, the decision or ability to practice consistent condom use is understood as a decision made in context of larger structures, which often include economic necessity (Decker et al., 2015; Deering et al., 2013). Many sex workers enter the field due to financial vulnerability or lack of other economic opportunities, which can limit access to quality care (Lancaster et al., 2016). As sex workers, financial need limits agency in condom negotiation for FSWs, who may need to accept more money in exchange for condomless sex (Goldenberg, Duff, & Krusi, 2015). Coerced sex is often condomless, and sexual violence can create injuries and therefore increase biological susceptibility of sexually transmitted infections (STI) and HIV (Decker et al., 2013; Swain, Saggurti, Battala, Verma, & Jain, 2011). Client-perpetrated violence has been shown to significantly increase the odds of being offered and accepting condomless sex, showing a lasting impact beyond the incidence of violence (Deering et al., 2013). Finally, GBV can create mental health morbidities which can impact a woman’s ability to negotiate condom use, practice protective behaviors and access HIV health services (Devries et al., 2013; Hutton, Lyketsos, Zenilman, Thompson, & Erbelding, 2004; Jewkes, Dunkle, Nduna, & Shai, 2010).
Structurally, GBV risk is increased for FSWs through the marginalization caused by criminalization and punitive laws. Policies that criminalize the practice of sex work can encourage FSWs to practice in secrecy (Decker et al., 2015). This can impact the ability of FSWs to reach legal and medical services designed to support victims of violence and reach harm-reduction services (Shannon et al., 2015). Behavioral outcomes of GBV include associations with HIV risk behaviors including drug and alcohol use, high-risk sexual behavior and practicing condomless sex (Deering et al., 2014). A study among FSWs in Russia found violence to be significantly associated with HIV, with past-year experiences of client violence increasing the HIV risk over threefold (Decker et al., 2012). Partner violence compromises HIV care trajectories for FSWs, and a study from the Dominican Republic among FSWs living with HIV found that intimate partner violence was associated with decreased care seeking and retention for HIV (Mendoza et al., 2017). Specifically, depression has been shown to be associated with inconsistent condom use; having sex while using drugs or alcohol; reducing positive behavior change; limiting both cognitive and physical functioning; and potentially interfering with HIV prevention, treatment and health care (Hill, Maman, Kilonzo, & Kajula, 2017; Hutton et al., 2004). The pathways between GBV and depression, and depression and health behaviors may play a significant role among FSWs. This dynamic between depression and health behaviors, as it has been evaluated among FSWs, has shown some association between GBV, depression and condom use although merits more research (Patel, Ganju, Prabhakar, & Adhikary, 2016; Sherwood et al., 2015; Swain et al., 2011).
This relationship is particularly important within Cameroon, where HIV prevalence among FSWs is significantly elevated at 26%, compared to 4.5% among reproductive-aged adults (Decker et al., 2016). With high rates of GBV documented among FSWs in Cameroon, understanding how GBV affects overall health is central to addressing the country’s HIV epidemic (Decker et al., 2013). Mental illness and depression has been under-researched and evaluated for FSWs in Cameroon, potentially in light of the focus on HIV transmission and less on the context in which it occurs (Baral et al., 2012; Patel et al., 2016). While there is limited data, several previous studies have shown high rates of depression among adult Cameroonians (Kanmogne et al., 2017).
Within this body of work, depression and other mental health issues have received relatively limited attention. Greater clarity is needed as depression and mental health have long been associated with GBV and may potentially play a major role in impeding protective health behaviors. Mental health issues and depression must be understood in context of the root causes in which they exist and the comorbidities that impact condom use. The objective of this article is to evaluate the relationships between lifetime experiences of sexual violence, depression and inconsistent condom use with clients among FSWs in Cameroon.
Methods
Study population
In tandem with a large-scale, multi-dimensional programmatic intervention for HIV/AIDS among FSWs and men who have sex with men called Continuum of Prevention, Care and Treatment (CoPCT) of HIV/AIDS with Most-at-risk-Populations in Cameroon (CHAMP), an integrated behavioral and biological survey (IBBS) was conducted with FSWs at baseline. This cross-sectional study was conducted across five cities in Cameroon: Yaoundé, Douala, Bertoua, Kribi and Bamenda (Project Search: Research to Prevention, 2004, 2014).
Participants were recruited through respondent-driven sampling (RDS), which is a strategy for reaching stigmatized or hidden communities (Greiner et al., 2014; Heckathorn, 1997). Recruitment is done through coupons, which allow members of the population to recruit their communities into the study (Schonlau & Liebau, 2012). Women were successfully enrolled in the study if they had a coupon, reported practicing sex work within the past 3 months, were 18 years old or over, were capable of giving informed consent, lived in the study site/region, reported sex work as their principal source of income, had not participated in a similar study in the past 6 months and understood English or French.
Ethical approval was granted by Cameroon’s National Ethics Committee, CNERSH (Comite National d’Ethique sur la Recherce en Sante Humaine), study number 016/06/782/CE/CNERSH/SP. This analysis was submitted to the Johns Hopkins Bloomberg School of Public Health and was determined to be not research.
Procedures and methods
The survey was an interviewer-administered tablet-based structured questionnaire and was distributed in English, French and Pidgin. The questionnaires took around 60 minutes to administer and were conducted in private rooms within the study sites which were themselves strategically located to ensure confidentiality and comfort. Interviewers were trained in confidentiality procedures and on interview best practices. Respondents received a financial incentive upon completion of the study (2,000 XAF, ~$3 USD) and an additional incentive for each of their three referrals who completed the study (1,000 XAF per referral, ~$2 USD), though respondent’s answers or results did not impact if incentive was received. All women were administered an HIV test at site.
Measures
Condom use with clients was our main dependent variable, sexual violence experience was the main independent variable of interest and depression was the potential mediator of interest. Variables were chosen for analysis based on an evidence-based conceptual framework, which are considered to be associated with the main outcome of condom use for vaginal sex with clients among the literature.
Demographics
Demographics included study city, age of respondents, education levels, marital status, employment outside of sex work, experience living abroad in the past 10 years, having biological children, from an urban/rural community and living situation.
Risk determinants
The survey included questions about potential associated determinants including arrest history and drug/alcohol use. Alcohol use was defined as alcohol use in the past year, and drug use was defined as non-injectable illicit drug use, and illicit injectable drug use. Sex work–related characteristics included location of sex with clients (brothel, hotel/guest houses) and number of clients in the past month. The number of casual clients in the past month was dichotomized into over and under 20 clients to estimate the impact of high client loads. All measures were self-reported. Finally, HIV status was determined by blood samples through the lab within the IBBS. The tests were Alere Determine TM HIV – ½ and OraQuick HIV – ½.
Condom use
The main outcome, consistent condom use for vaginal sex with clients, was captured through questions on condom use with both regular and casual clients. Participants were first asked whether they had ever had regular clients or ever had casual clients. They were then asked about their lifetime experiences of condom use with each type of client. Inconsistent condom use was determined for this study as reporting anything other than ‘always’ using condoms with either type of client (MEASURE Evaluation, n.d.). For those who reported having regular and casual clients, consistent condom use was determined by reporting ‘always’ using a condom with both their regular and casual clients. If participants reported only having either casual or regular clients, consistent condom use was determined by ‘always’ using a condom for just the type of client they reported. No significant differences were found in condom use in vaginal sex with regular and casual clients for the covariates examined, so they were combined into one outcome indicator: condom use for vaginal sex with clients, dichotomized into outcomes of consistent or inconsistent use.
Violence
Sexual violence was defined as having someone ever force you to have sex when you did not want to (oral, anal, vaginal or with an object). Responses were ‘no’, ‘yes, in the last six months’, or ‘yes, but not in the last six months’. Responses were dichotomized into yes and no to determine proportions of ever experiencing violence, and GBV refers specifically to this type of sexual violence. For this article, we only looked at sexual violence.
Depression
Depression was assessed via the Patient Questionnaire 9 (PHQ9) (Cholera et al., 2014). Composite scores were developed and then categorized into levels of depression. Scores ranged from 0 to 26 and were classified to ensure maximum sensitivity into groups of no depression (0–4), mild depression (5–9), moderate depression (10–14), moderately severe depression (15–19) and severe depression (20–27) (Adewuya, Ola, & Afolabi, 2006; Pence et al., 2012).
Stigma
Stigma was categorized into three different scales to determine types of stigma experienced: anticipated, enacted (non-violent) and perceived. Anticipated stigma included afraid to go to health center, avoided going to health center and scared to be in public spaces. Enacted stigma included overheard health care workers gossip, faced verbal harassment or had been blackmailed. Perceived stigma was comprised of excluded from family, family made discriminatory remarks, rejected by friends, not treated well in a health center and police refused to protect, all due to status as a FSW (Stahlman et al., 2016).
Statistical analyses
Data from the five sites were combined into one total sample (N = 2,165). All analyses were conducted in Stata 14 (College Station, TX) (StataCorp LP, 2015). Table 1 reports demographic variables in crude numbers and proportions overall and by consistent condom use as the main outcome, with comparisons evaluated using chi-square p values. RDS-adjusted estimates were determined for demographic characteristic proportions as well. While crude numbers and proportions represent actual reported numbers in the study sample, RDS estimates attempt to determine the estimates of the covariates within the FSW population of Cameroon (Lyons et al., 2017). Crude estimates were used in the regressions in place of the RDS estimates, because there is no conclusion reached on how RDS should be handled within regressions (Schonlau & Liebau, 2012). Table 2 examined structural and sex work–related characteristics for the sample overall and in relation to condom use as the key outcome, again with chi-square analysis to evaluate comparisons.
Sociodemographic characteristics of female sex workers (N = 2,165).
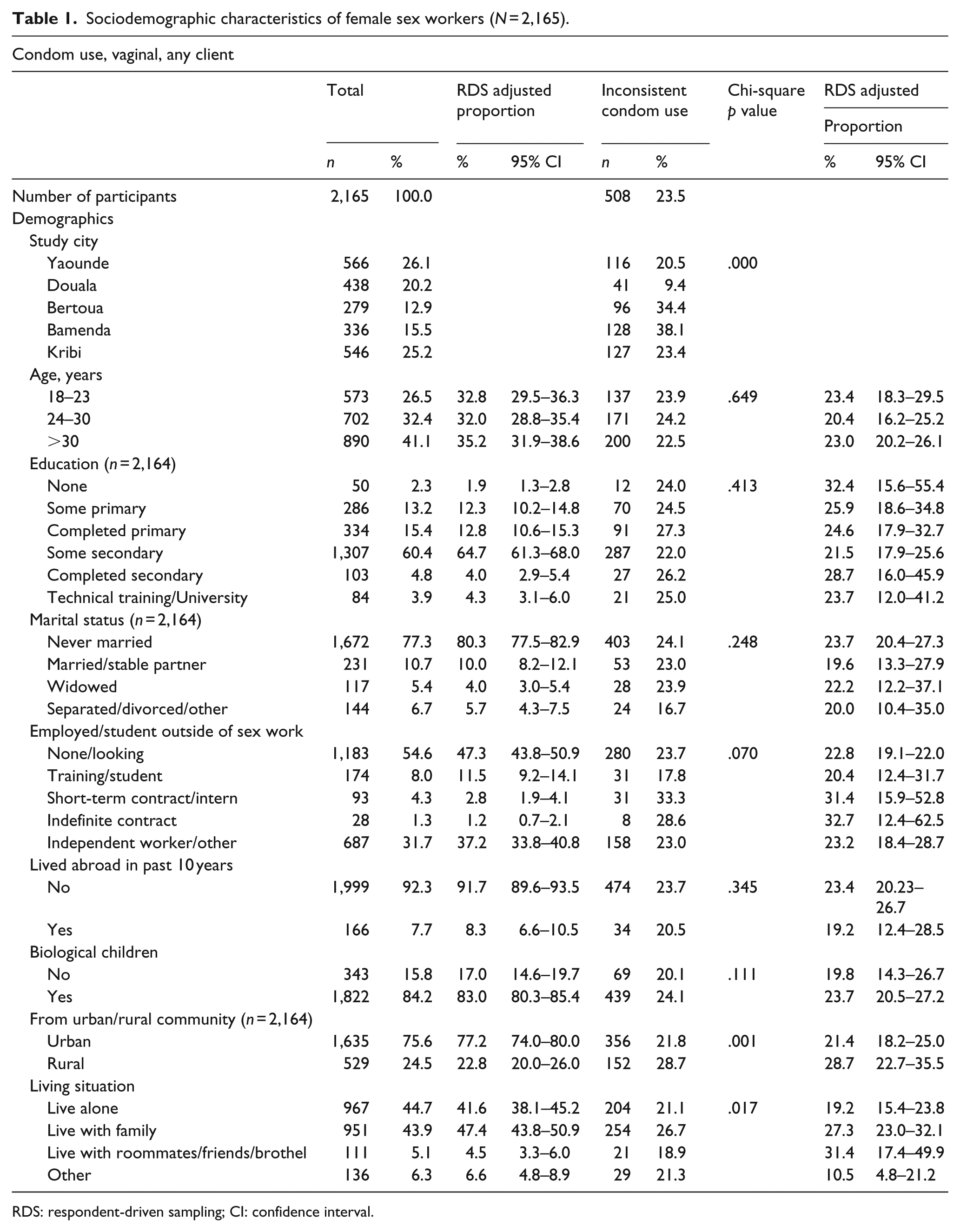
RDS: respondent-driven sampling; CI: confidence interval.
Violence, HIV and sexual history characteristics among FSWs.
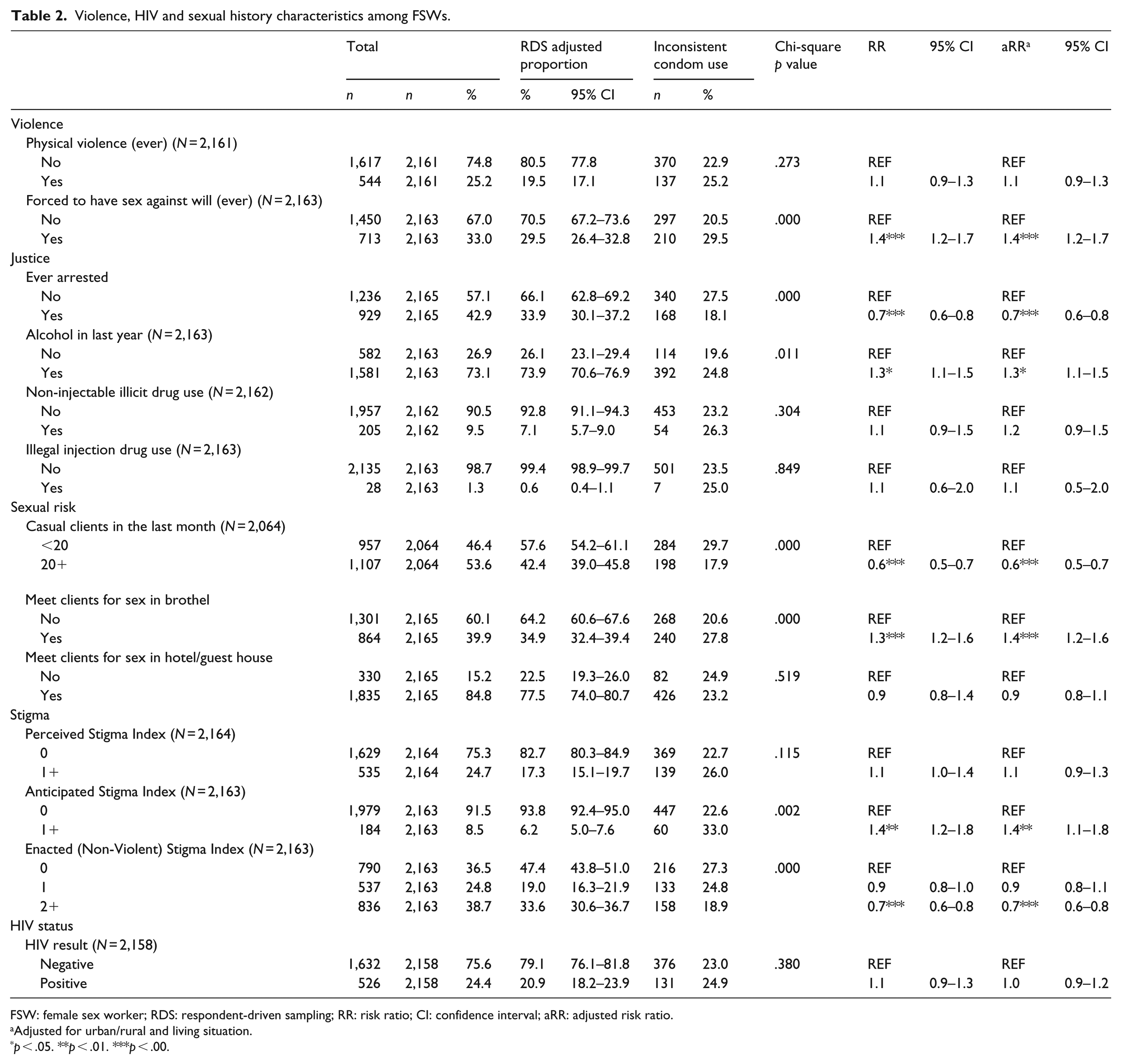
FSW: female sex worker; RDS: respondent-driven sampling; RR: risk ratio; CI: confidence interval; aRR: adjusted risk ratio.
Adjusted for urban/rural and living situation.
p < .05. **p < .01. ***p < .00.
Poisson regressions with robust error variance were used for all regressions (Zou, 2004). Bivariate models were used to determine risk ratios (RRs) and 95% confidence intervals (CIs) of all characteristics. Multivariate Poisson regressions were used to determine adjusted risk ratios (aRRs) of the sex work characteristics, justice-related variables, stigma experiences and HIV status covariates included in Table 2 and were adjusted for the demographic variables that were significantly associated with the outcome (chi-square p values < .05).
The final models used were to conduct a cross-sectional mediation analysis (Baron & Kenny, 1986). Mediation analysis was done by first describing the proportions of inconsistent condom use with clients for each level of depression and the associated chi-square p value. A bivariate model was used to assess the crude association of depression with inconsistent condom use. Second, we explored proportions of depression levels among those exposed and those unexposed to sexual violence and associated chi-square p value to examine the relationship between the potential mediator (depression) and the independent variable of interest (sexual violence). Three final models were used to assess association of inconsistent condom use with clients, sexual violence and depression using aRRs, and evaluated if depression was mediating the effect of GBV on inconsistent condom use with clients, as evidenced by significant changes in the aRR. Depression was chosen as a mediation factor by its significance in the adjusted model, as well as the possibility of its role in impacting condom use. Model 1 examined the impact of sexual violence on inconsistent condom use without controlling for depression, model 2 included depression but not sexual violence in the model, and model 3 included both depression and reported sexual violence. All final models included demographic and risk characteristics that were found to be significantly associated with inconsistent condom use in chi-square analyses at p < .05. All the covariates included in the final model were assessed for collinearity (Table 3).
Distribution of potential mental health mediators over outcome (unprotected sex) and independent variable (sexual violence).
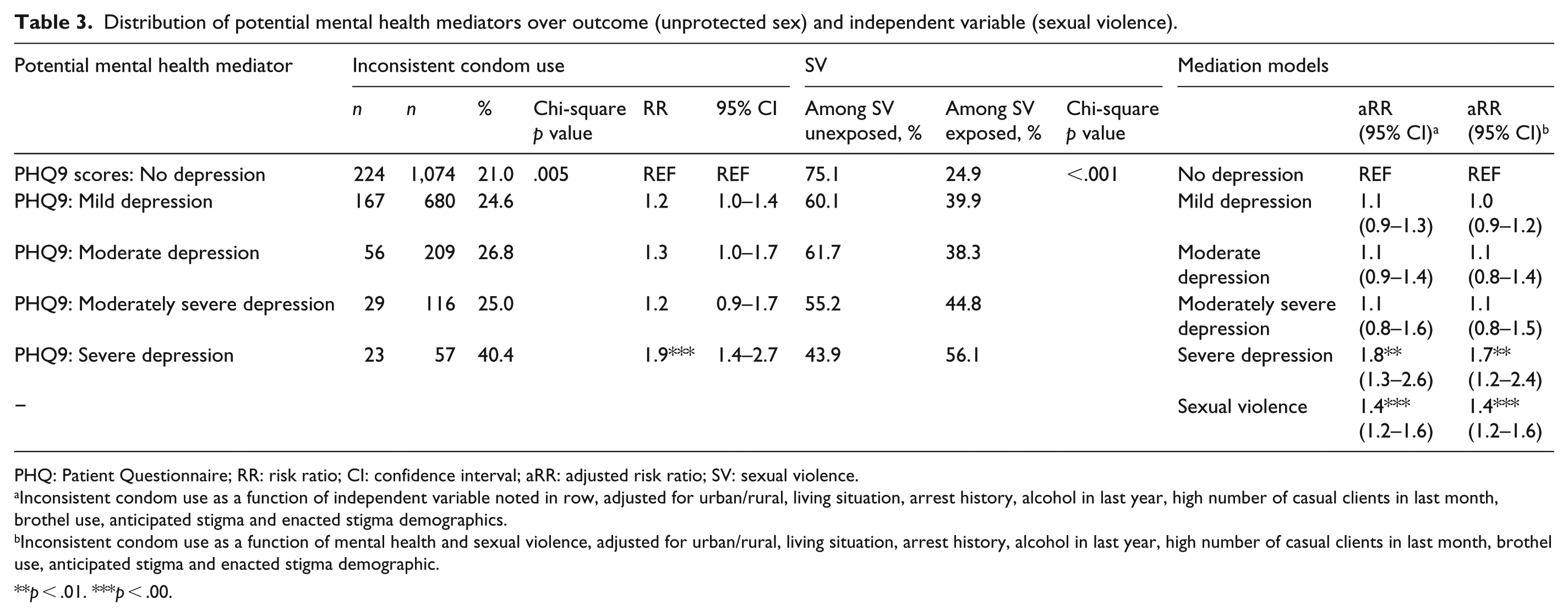
PHQ: Patient Questionnaire; RR: risk ratio; CI: confidence interval; aRR: adjusted risk ratio; SV: sexual violence.
Inconsistent condom use as a function of independent variable noted in row, adjusted for urban/rural, living situation, arrest history, alcohol in last year, high number of casual clients in last month, brothel use, anticipated stigma and enacted stigma demographics.
Inconsistent condom use as a function of mental health and sexual violence, adjusted for urban/rural, living situation, arrest history, alcohol in last year, high number of casual clients in last month, brothel use, anticipated stigma and enacted stigma demographic.
**p < .01. ***p < .00.
Results
Demographics
A total of 2,165 FSWs were included in the study sample. The proportion of individuals were dispersed relatively evenly among the cities, with the highest coming from Yaoundé (26.1%, 566/2,165) and the lowest percentage coming from Bertoua (12.9%, 279/2,165). The mean age of the participants was 30.1 (inter-quartile range: 23–36). The majority of participants had never been married (77.3%, 1,672/2,165). Over half of the population was unemployed or looking for work outside of sex work (54.6%, 1,183/2,165). Reported living situation was significantly associated with inconsistent condom use with clients (p < .05). The majority of the sample was split between living alone (44.7%, 967/2,165) and with family (44.0%, 951/2,165), with the rest living with roommates/friends/brothel (5.1%, 111/2,165) or other (6.3%, 136/2,165).
Risk characteristics: violence, justice, sexual risk, stigma and HIV outcomes
Overall, 23.5% (508/2,165) of respondents reported inconsistent condom use for vaginal sex with clients. Of the 33.0% (713/2,163) of FSWs who reported ever facing sexual violence, 29.5% (210/713) had practiced inconsistent condom use with clients (RR 1.4, 95% CI (1.2–1.7); aRR 1.3, (1.1–1.5)). Table 2 presented proportions, RDS adjustments and regressions unadjusted and adjusted for the significant demographic variables (urban/rural divide and living situation).
Arrest was found to be associated with inconsistent condom use. Just under half of the respondents reported being ever arrested (42.9%, 929/2,165), 18.1% of which reported inconsistent condom use with clients. Experience of arrest remained significantly associated with inconsistent condom use even when adjusted for significant demographic variables (RR 0.7, 95% CI (0.6–0.8); aRR 0.7, 95% CI (0.6–0.8)). Of the 2,163 respondents who responded regarding their alcohol use, the majority reported drinking alcohol in the past year (73.1%, 582/2,163). A higher percentage of those who had used alcohol in the past year reported inconsistent condom use with clients (24.8%, 392/1,582) than non-users (19.6%, 114/582), and alcohol use in the past year remained significantly associated with condom use in the adjusted model (RR 1.3, 95% CI (1.1–1.5); aRR 1.3, 95% CI (1.1–1.5)).
In total, 53.6% (1,107/2,064) of respondents reported having over 20 paying casual clients in the past month, which was significantly associated with inconsistent condom use. Inconsistent condom use was prevalent among 29.7% (284/957) of FSWs who had fewer than 20 casual clients in the past month and was significant in both the unadjusted and adjusted models (RR 0.6, 95% CI (0.5–0.7); aRR 0.6, 95% CI (0.5–0.7)). When considering location of meeting with clients, 39.9% (864/2,165) of FSWs reported meeting their clients in brothels. Among FSWs who used brothels, inconsistent condom use was significantly higher than those who used other locations: 27.8% (240/864) to 20.6% (268/1,301), respectively (RR 1.3, 95% CI (1.2–1.6); aRR 1.4, 95% CI (1.2–1.6)).
Anticipated stigma was significantly associated with inconsistent condom use (RR 1.4, 95% CI (1.2–1.8); aRR 1.4, 95% CI (1.1–1.8)), as was the higher level of enacted stigma (RR 0.7, 95% CI (0.6–0.8); aRR 0.7, 95% CI (0.6–0.8)).
Mediation model
Any level of depression was present among 49.8% (n = 1,067) of respondents and was significantly associated with inconsistent condom use (p < .01). Among those with any depression, those with severe depression showed almost twice the risk of inconsistent condom use compared to those without depression (RR 1.9, 95% CI (1.4–2.7)). With increasing depression level, the proportion of those who had experienced sexual violence increased; among respondents with no depression, 24.9% (267/1,071) reported exposure to sexual violence versus 56.1% (32/57) of respondents with severe depression who reported experiencing sexual violence (p < .01).
In the final multivariate mediation models, the RR of inconsistent condom use among FSWs who reported sexual violence did not change when depression was not included in model 1 (aRR 1.4, 95% CI (1.2–1.6)) compared to when it was included in model 3 (aRR 1.4, 95% CI (1.2–1.6)). Severe depression was significantly associated with inconsistent condom use in model 2, which accounted for significant demographic and risk characteristics (aRR 1.8, 95% CI (1.3–2.6)). In model 3, sexual violence and depression were both significantly associated with inconsistent condom use, which suggests independent impact rather than mediation (sexual violence: aRR 1.4, 95% CI (1.2–1.6); severe depression: aRR 1.7, 95% CI (1.2–2.4)).
Discussion
Women face power imbalances during condom negotiation, and structural determinants reinforce these gendered power disparities. This dynamic is profound for FSWs, who negotiate condom use repeatedly in the context of high rates of violence and depression (Decker et al., 2012). As seen in this study, GBV and depression significantly impacted condom use with clients in Cameroon, both independently and in conjunction. Condom use by FSWs is not a behavior that occurs in isolation but in the context of high rates of comorbidities and underlying inequalities. In these results, sexual violence and depression were independent, significant cross-sectional predictors of inconsistent condom use with clients. While sexual violence was associated with depression, depression did not appear to mediate the relationship between sexual violence and condom use. Results illustrate the need to understand the larger contextual factors which may be fueling GBV and depression among FSWs, as both impact inconsistent condom use. Through decreased use of consistent condom use, GBV and depression may ultimately increase vulnerability for HIV transmission and create an environment of risk for FSWs.
FSWs are members of a socially and economically marginalized group with limited access to comprehensive care. FSWs included here reported low levels of education and high rates of unemployment. In part due to such underlying inequalities, the work environment for FSWs offers particular risk of violence, which may fuel depression; the intersection of isolated work locations, punitive policing practices and abusive clients suggests interventions that address structural issues would enable a more effective HIV prevention approach (Lyons et al., 2017). The social, economic, work and political contexts such as poverty and gender inequality may play a larger role in determining condom use among FSWs, and research is needed to further understand depression and violence in this context (Decker et al., 2015; Deering et al., 2014; Papworth et al., 2014). Addressing violence and depression for FSWs requires addressing the power dynamics and larger structures which create and fuel health disparities for women who sell sex (Sagtani et al., 2013).
Depression was significantly associated with inconsistent condom use throughout all models, indicating the impact of mental health on protective behaviors among FSWs. A 2015 study in Cameroon among HIV-positive patients with depressive symptoms showed decreased PHQ9 scores and increased overall health following 4 months of antidepressant treatment (Gaynes et al., 2015). The study also found that self-efficacy scores increased in the same time period. However, self-efficacy – impacted by GBV and depression – may not be enough to create consistent condom use among FSWs (Jones et al., 2016; Shannon et al., 2009). For FSWs, further research is needed to understand how and why depression and GBV decrease condom use, and how established mental health interventions can be adapted to address the context of their lives. GBV has been studied as a power relationship and representative of gender inequality, often fueled by the types of poverty and inequality which may be the same as those which cause a woman to enter sex work (Papworth et al., 2014; Shannon et al., 2014; Tsai, 2013). Research is beginning to discuss depression in this light as well, and the rates of depression seen in this study make clear the need to understand depression and mental illness as a symptom of larger health disparities. This study represents the impact on FSWs of multiple burdens of GBV, gender inequality and depression, each exaggerated by poverty and lack of economic access seen among these respondents (Beattie et al., 2010; Goldenberg et al., 2015).
The elevated levels of sexual violence suggest that interventions focusing on supporting FSWs should address structural drivers of violence. With health equity paradigms encouraging health systems to think about ‘demand-side’ interventions, documenting the prevalence of depression, violence and their impact on condom use for marginalized populations has potential to make real change (Ostlin et al., 2011). This study attempts to center the inter-connected demands of the FSWs’ complexities to inform interventions that are driven by the users of the health systems (Ostlin et al., 2011).
Limitations
There are several limitations with this study. This was cross-sectional, limiting the ability of the study to determine temporal ordering, causation or directionality of events. Furthermore, there is potential of RDS to create bias in the sample by not reaching FSWs who have limited social networks and may as a result be at even increased risk for marginalization not represented within this study (Lyons et al., 2017). Moreover, the primary sexual violence indicator, forced sex, may have missed sexual experiences that were pressured or coerced (Patel et al., 2016). The sensitive and stigmatized nature of both sexual violence and mental health may have caused some respondents to self-censure, which would result in missed cases, despite the research team training to ensure accurate and comfortable reporting. There is potential for unmeasured or missed confounding, or factors which may have impacted the final indicator but were not included in the analysis.
Conclusion
Inconsistent condom use with clients remains highly prevalent among FSWs in Cameroon. Violence and depression faced by the FSW population impact condom use, yet remain under-researched among FSW populations. Understanding the factors that drive inconsistent condom use with clients is pivotal to reducing HIV incidence among FSWs, improving their overall health and ensuring their ability to seek care. While there is value in increased study of research integrating social inequities, power asymmetrics and social determinants of health, these data already provide guidance on the importance for programs to address underlying inequities driving sexual practices and health outcomes (Ostlin et al., 2011). Mental illness and depression remain poorly researched among FSWs in light of the intersecting epidemics of GBV and HIV. While this study focused on indicators specifically around depression, the overall research indicates a huge need to further understand mental health as a factor in behaviors. Mental health potentially impacts every level of HIV care and must be better considered as a factor impacting the health of FSWs. Taken together, these data suggest that research and programming which focuses on violence and harm reduction for FSWs, and addresses disparities beyond the individual level, have the potential to address health disparities for this highly marginalized population.
Footnotes
Acknowledgements
The authors are grateful to all who supported this work. This study was conducted through Continuum of Prevention, Care and Treatment of HIV/AIDS with Most-at-risk Populations in Cameroon (CHAMP). The program is implemented by CARE International in Cameroon in collaboration with Johns Hopkins University (JHU), Global Viral (GV) and eight local community-based organizations (MotoAction, Alternatives Cameroun, CMWA, Horizons Femmes, Humanity First, ASAD, CAMNAFAW and SWAA Littoral) and in coordination with the National AIDS Control Committee and the Ministry of Public Health.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was made possible by the generous support of the American people through the U.S. Agency for International Development (USAID) and the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR). The contents are the responsibility of Johns Hopkins University and do not necessarily reflect the views of USAID, PEPFAR or the U.S. Government. CHAMP, a 5-year cooperative agreement (AID-624-A-14-00003), is a large-scale HIV prevention, care and treatment program for key populations in Cameroon. CHAMP is led by CARE Cameroon in partnership with Johns Hopkins School of Public Health, Global Viral and MotoAction. S.B.’s effort was funded in part from the Johns Hopkins University Center for AIDS Research, an NIH-funded program (P30AI094189), which is supported by the following NIH Co-Funding and Participating Institutes and Centers: NIAID, NCI, NICHD, NHLBI, NIDA, NIMH, NIA, FIC, NIGMS, NIDDK and OAR. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or AHRQ.