
Abstract
Background:
The clinical pathways for treating mental illness have received global attention. Several empirical studies have been undertaken on treatment pathways in Ghana. No study, however, has systematically reviewed the literature related to the pathways of mental health treatment in Ghana.
Aim:
This article aims to identify the pathways used to treat mental illnesses; examine the evidence about the possibility of collaboration between biomedical, faith and traditional healing pathways; and draw attention to the barriers hindering such collaboration.
Methods:
A search of the published literature was conducted using Medline, Embase, PsycINFO, CINAHL (EBSCO), Web of Science and Scopus databases. The search was limited to the articles that were published in English and released between 2000 and June 2018. The review synthesises both qualitative and quantitative data.
Results:
The findings showed that mental illnesses in Ghana are treated using a mixture of biomedical and faith-based and traditional healing services. Faith and traditional healing pathways are typically used as a preliminary source of cultural assessment before seeking biomedical treatment. There is an increasing desire for collaboration between biomedical, faith and traditional healing pathways. However, several individual factors (attitude or stigma, the perceived efficacy of treatment and differences in the treatment process) and health system factors (a lack of policy and regulation, a limited number of biomedical service providers, limited financial support and geographical isolation of services) jointly contribute to barriers precluding establishing such collaboration.
Conclusion:
This review recommends that policies, regulations, educational support and financial incentives should be developed to facilitate collaboration between biomedical, faith and traditional healing service provision.
Introduction
Treatment pathways generally outline the events and processes of treatment prior to the initiation of any medical intervention. Treatment pathways are influenced by a variety of factors (Scott, Walter, Webster, Sutton, & Emery, 2013). Several theoretical approaches have been developed to explain the sequential stages of treatment pathways (Bhugra & Flick, 2005; Scott et al., 2013) as well as the factors that can influence these pathways. Anderson and Newman’s theory of access to health services categorise these factors as predisposing, enabling and need (Andersen & Newman, 2005; Graham, Hasking, Brooker, Clarke, & Meadows, 2017; Kim & Lee, 2016). The ‘predisposing’ factors which encourage individuals to develop a propensity for the use of mental health services are grouped into demographics (age and gender), social structure (education, occupation, ethnicity, social networks and social interactions and culture) and attitudinal or belief systems (attitudes, values and individuals’ knowledge of the health care systems; Andersen & Newman, 2005; Graham et al., 2017; Kim & Lee, 2016). The ‘enabling’ factors refer to the strength of the existing health systems, including the availability, affordability, accessibility, acceptability, adequacy and awareness of mental health services (Andersen & Newman, 2005; Scott et al., 2013). The ‘need’ factors are concerned with the functional and health-related problems which prompt immediate use of mental health services. The need factors also explain the symptoms, functioning and quality of life of those people who make use of mental health services (Kim & Lee, 2016).
Pathways to treatment vary across societies and types of health condition. Mental illnesses may be treated with biomedical as well as faith and traditional healers. The choice of treatment often depends on which service is most accessible. Many health systems in high-income countries treat mental illness through biomedical approaches; in contrast, those in low-income countries often employ a mixture of biomedical, faith and traditional healing services (Adelufosi, Ogunwale, Adeponle, & Abayomi, 2013; Adeosun, Adegbohun, Adewumi, & Jeje, 2013; Burns & Tomita, 2015; Giasuddin, Chowdhury, Hashimoto, Fujisawa, & Waheed, 2012). The faith and traditional healing services in this context are often tied closely to the inherent beliefs and values emanating from traditional-cultural practices, rituals and belief systems.
In Africa, past evidence illustrates that people with mental illnesses mostly initiate their care with faith and traditional (or herbal) services, including religious practitioners and traditional healers (Adelufosi et al., 2013; Adeosun et al., 2013; Burns & Tomita, 2015; Kauye, Udedi, & Mafuta, 2015). When people with mental illnesses choose biomedical services, treatment is often initiated through general practitioners or mental health practitioners (Adelufosi et al., 2013; Burns & Tomita, 2015) who subsequently refer to psychiatric specialists (Bhugra & Flick, 2005; Fridgen et al., 2013; Scott et al., 2013).
In Ghana, several empirical studies have recently been undertaken on mental health services. These studies largely address the weaknesses in mental health systems (Deborah et al., 2019; Nartey et al., 2019), gaps in policy, experiences of caregivers and treatment pathways. However, very few studies have reviewed the literature on mental health-related issues in Ghana. The few review studies on mental health services in Ghana address the direction of neuroscience-related research. (Quansah & Karikari, 2016) and the estimation of epidemiological data on mental, neurological and substance (MNS) use disorders (Read & Doku, 2012). One other study (Osafo, 2016) that attempted to review the literature on treatment pathways provides a framework which establishes collaborative linkages between religious leaders and professional mental health workers.
This article reviews the treatment pathways to mental health services in Ghana. The article specifically aims to identify the treatment pathways used to treat mental illnesses, gather evidence relevant to the potential collaboration between biomedical and faith-healing pathways and identify barriers confronting such collaboration. This evidence is relevant to policymakers, clinicians, faith and traditional service providers, academia and community members and serves to inform them about the best ways to foster collaboration. This review can also inform stakeholders of the additional gaps in the relevant literature and illuminate the direction and priority areas yet to be established for mental health research in Ghana.
Methods
Methodology
The literature review included qualitative, quantitative and mixed-methods studies for the exploration of treatment pathways to mental health services in Ghana (Grant & Booth, 2009). A five-stage approach was employed, which included problem identification, literature search, data evaluation, data synthesis and presentation results (Grant & Booth, 2009; Whittemore & Knafl, 2005).
Eligibility criteria
This review included all peer-reviewed published articles addressing treatment pathways to mental health services in Ghana. The quantitative papers used the cross-sectional design involving the administration of questionnaires, while the qualitative papers used phenomenological, exploratory, ethnographic and participatory action research methodology. The included papers targeted multiple participant groups, such as stakeholders from government ministries, health professionals, mental health service users, family members and caregivers and community members. The selected studies were published in English and from 2000 to June 2018.
Exclusion criteria
The review excluded studies that did not target pathways for treating mental illnesses; articles that had been published before 2000 and in languages other than English.
Search strategy
Six electronic databases were searched for the review: Embase, Medline, Web of Science, PsycINFO, CINAHL (EBSCO) and Scopus. Several steps were taken to search for the published literature. The first step involved an initial search in Medline and Scopus. The second step included the analysis of the search keywords in the titles and abstracts of the articles. The third step concerned the identification of keywords and index terms used in the articles across all the selected databases. The final step was a manual attempt at sifting through the reference lists of all the identified articles (Pearson et al., 2014).
Search terms and Boolean operators
The search terms and Boolean operators in this research were as follows: (‘Mental disorders’ OR ‘anxiety disorders’ OR ‘mental illness’ OR ‘mental health’ OR ‘bipolar and related disorders’ OR ‘elimination disorders’ OR ‘neuro-developmental’ OR ‘neurotic disorders’ OR ‘schizophrenia spectrum’ OR ‘psychotic disorders’ OR ‘substance-related disorders’ OR ‘trauma and stressor related disorders’ ‘psychiatric patient’) AND (stigma* OR discriminat* OR attitud* OR inclus* or equit*) AND (biomed* OR faith-bas* OR psychosoc* OR quality*) AND (service use* or uptake* or treatment*).
Critical appraisal
The authors developed a critical appraisal checklist using the Mixed Methods Appraisal Tool (MMAT; Quan et al., 2018) and the Joanna Briggs Institute (JBI; 2017) critical appraisal tool. The appraisal tool was divided into several sections: qualitative, quantitative randomised controlled trials, quantitative non-randomised (analytical cross-sectional), a quantitative descriptive, systematic review and mixed methods. Each of the sub-sections contained specific questions linked to methodological and reporting quality (see Supplemental Appendix 1). The appraisal helped us understand which articles to include or exclude in our study and obtain further information from the authors. Two reviewers independently appraised the methodological quality of all the papers prior to their inclusion in the final review. Overall, the methodological quality scores were assigned as follows: low quality (a score below 25%), medium quality (a score of 50%) and high quality (a score of 75% and above). These scores were computed by counting the number of ‘Yes’ responses for each sub-section of the methodological criteria and expressing them as a percentage (Quan et al., 2018).
Data management and extraction
The study used Endnote X8 to manage search results and screening. Two reviewers independently managed the data extraction process. A data extraction form was developed to extract information from all the included papers. The data extraction form was developed using the JBI (Pearson et al., 2014) and Cochrane (Moher, Liberati, Tetzlaff, Altman, & PRISMA Group, 2009) manuals. The authors also consulted experts in research methodology and the subject area. The data extraction form consisted of different sub-sections (study details, methodologies and treatment pathways); it also recorded additional information on mental health as well as recommendations and additional references.
Data synthesis
We used the content analysis process to analyse and synthesise both qualitative and quantitative data (Brown & Lloyd, 2001; Pearson et al., 2014). The qualitative data were coded and presented alongside the quantitative data (Brown & Lloyd, 2001; Palinkas, 2014; Pearson et al., 2014). The coding process was repeated for all the extracted data. The coded ideas were then organised into themes, which in turn were used to organise the results.
Results
Characteristics of the included papers
The review included 26 papers that met the inclusion criteria. Of these, 16 contained qualitative data, 5 contained quantitative data and 5 were mixed methods. Of the 26 papers, 4 papers used the cross-sectional design (see Table 1). The review identified several themes that facilitated the discussion of findings. Of the 26 included papers, 21 met the criteria for high quality and 5 had a medium quality score (see Table 1).
Study characteristics.
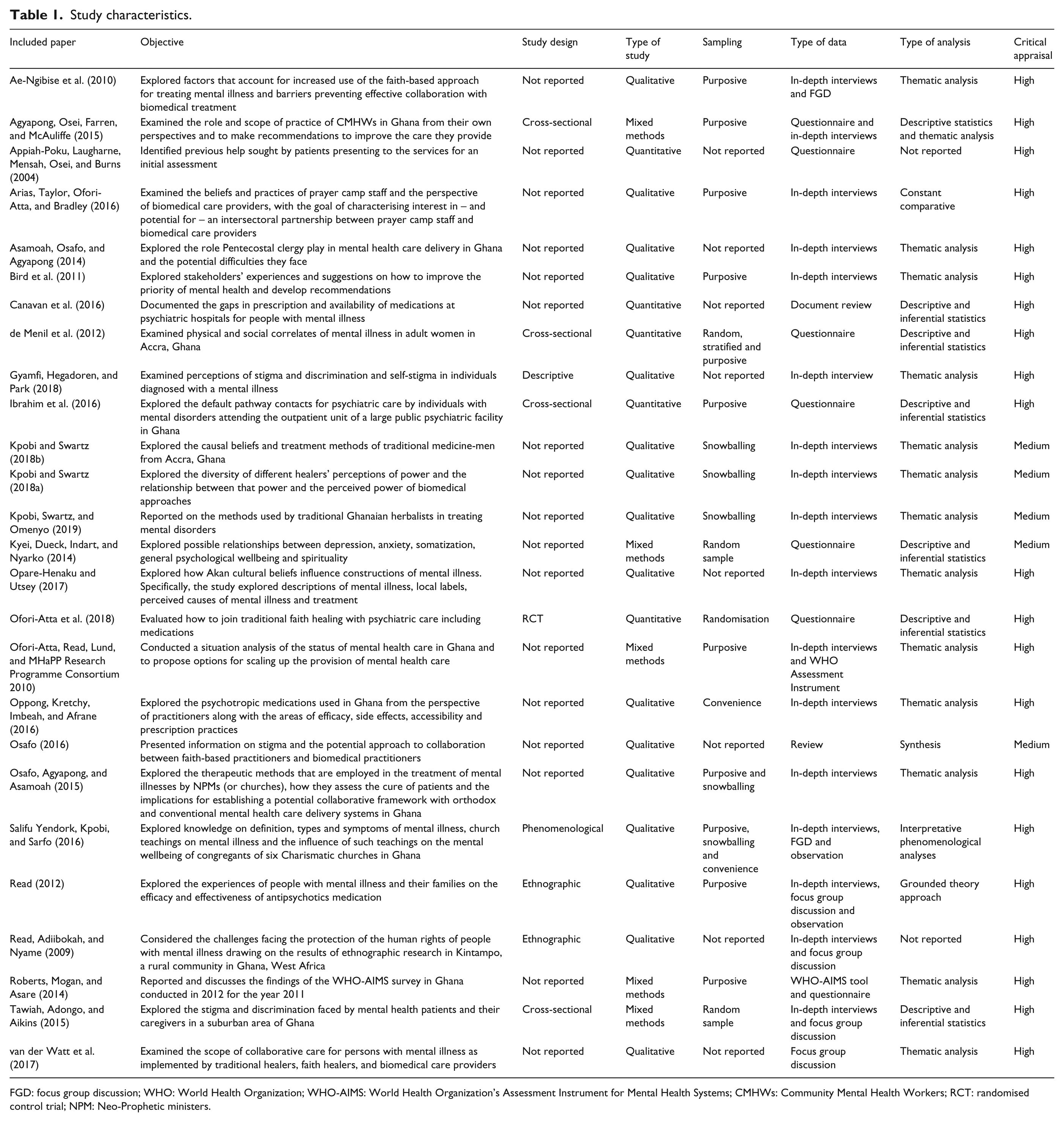
FGD: focus group discussion; WHO: World Health Organization; WHO-AIMS: World Health Organization’s Assessment Instrument for Mental Health Systems; CMHWs: Community Mental Health Workers; RCT: randomised control trial; NPM: Neo-Prophetic ministers.
Themes of the findings
The identified themes included treatment pathways, biomedical treatment, informal treatment from the faith and traditional healing, challenges confronting faith and traditional healing providers, a collaboration between biomedical and faith and traditional healing service providers and barriers to collaboration.
Treatment pathways
Several studies refer to biomedical treatment and faith and traditional healing services as pathways to treating mental health in Ghana.
Biomedical treatment
The evidence from the quantitative studies demonstrates that biomedical treatment is normally the preferred or default mental health service among the consumers and community members (Ibrahim et al., 2016; Kyei, Dueck, Indart, & Nyarko, 2014; Tawiah, Adongo, & Aikins, 2015). Estimates from two quantitative studies suggest that an average of 77.6%–79% of consumers sought biomedical care as their preferred treatment (Ibrahim et al., 2016; Tawiah et al., 2015). In a previous study, 52.3% (i.e. 56 out of 107 consumers) visited psychiatric hospitals, whereas 21.5% sought treatment from non-psychiatric general hospitals as their primary point of contact (Ibrahim et al., 2016). Similarly, 61.5% (i.e. 276 out of 448 community samples) preferred psychiatric care, psychotherapy, counselling and social intervention as their source for treating mental illness (Kyei et al., 2014). The evidence from the quantitative studies indicates that consumers and community members predominantly use biomedical treatment from psychiatric facilities and general hospitals to treat their mental illnesses. The consumers of services in these studies were asked directly to report where they accessed mental health services from the onset of the mental illness.
Informal treatment from the faith and traditional healing services
Evidence from the quantitative studies indicates that about 15%–35% of consumers and community members prefer faith-based and traditional healing services as their chosen method of treating their mental illnesses (de Menil et al., 2012; Ibrahim et al., 2016; Kyei et al., 2014; Tawiah et al., 2015). In a sample of 107 consumers of mental health services, 23.3% sought non-psychiatric treatment from religious and/or traditional healing centres as their first contact (Ibrahim et al., 2016). In contrast, evidence from the qualitative studies demonstrates that consumers use faith-based and traditional healing services as their default sources of treating their mental illnesses (Ae-Ngibise et al., 2010; Bird et al., 2011; Gyamfi, Hegadoren, & Park, 2018; Kpobi, Swartz, & Omenyo, 2019; Opare-Henaku & Utsey, 2017; Osafo, Agyapong, & Asamoah, 2015; Read, 2012).
Several studies illustrate the process involved in treating mental illnesses using a faith-based approach (Ae-Ngibise et al., 2010; Arias, Taylor, Ofori-Atta, & Bradley, 2016; Asamoah, Osafo, & Agyapong, 2014; Kpobi & Swartz, 2018a, 2018b; Kpobi et al., 2019; Osafo et al., 2015; Read, Adiibokah, & Nyame, 2009; Salifu Yendork, Kpobi, & Sarfo, 2016). The treatment process is categorised into two phases, which include spiritual cosmologies or hope induction (Ae-Ngibise et al., 2010; Kpobi & Swartz, 2018b; Osafo et al., 2015) and exorcism (prophetic deliverance; Asamoah et al., 2014; Kpobi & Swartz, 2018a; Kpobi et al., 2019; Osafo et al., 2015).
The initial phase (spiritual cosmologies), which corresponds to diagnosing and history taking in biomedical treatment, involves the use of spiritual means to identify the root cause of the condition and the appropriate treatment method from a supernatural authority (Asamoah et al., 2014; Kpobi & Swartz, 2018b; Osafo et al., 2015). Spiritual cosmologies begin with a consultation with a supernatural authority, which involves taking history or through the use of spiritual discernment (Ae-Ngibise et al., 2010; Osafo et al., 2015). For instance, faith-based healers (e.g. churches) use biblical texts for exhortation during the spiritual cosmologies phase (Osafo et al., 2015). Conversely, exorcism (prophetic deliverance), which appears as medication and prescription, employs various religious rituals and practices to understand the reason for the problem or illness and prescribe the appropriate solution (Asamoah et al., 2014; Osafo et al., 2015). Faith-based providers (e.g. churches) provide healing schools and deliverance sessions for consumers during this phase (Salifu Yendork et al., 2016). Furthermore, not only do faith-based and traditional healers rely on spiritual therapy but they also employ some components of psychotherapy, such as raising hope in consumers and their family members (Asamoah et al., 2014; Osafo et al., 2015).
The religious rituals and practices employed by faith and traditional healing service practitioners vary slightly depending on the service provider, such as Christian healers or traditional and herbal practitioners. For instance, the Christian healing approach uses fasting (abstinence from certain or all food and drink for a defined period of time), prayers, anointing oils or holy water to support the healing processes (Ae-Ngibise et al., 2010; Arias et al., 2016; Asamoah et al., 2014; Kpobi & Swartz, 2018a), while traditional healing practitioners rely on spiritual actions which can be performed by both consumers and their families, supplemented by herbal remedies (Kpobi & Swartz, 2018a; Kpobi et al., 2019). Some studies explain that, within the indigenous cultural context, herbal practitioners use traditional approaches to harness the properties of herbs and plants with the aim of healing consumers (Kpobi & Swartz, 2018a; Kpobi et al., 2019). In addition, some herbal practitioners supplement their treatment process with a spiritual component, which includes prayer and fasting or the recitation of incantations (Kpobi & Swartz, 2018a; Kpobi et al., 2019).
The elements that are common across all the faith-based and traditional healing services include a confession to wrongdoing, demand for respect and recognition as well as close adherence to instructions in order to achieve complete healing (Ae-Ngibise et al., 2010; Kpobi & Swartz, 2018a). There is also evidence of practices that appear controversial or contentious across most faith-based centres. These practices include the use of chains, caning, corporal punishment and the use of shackles in the process of treatment (Ae-Ngibise et al., 2010; Arias et al., 2016; Read et al., 2009). These practices which are often intended to prevent consumers from running outside prayer camps may constitute physical abuse and a breach of the human rights of people with mental illnesses.
Faith and traditional healing services use several outcome indicators to demonstrate healing from a mental illness. These indicators reflect the signs and symptoms of consumers, including restored orientation, self-care, community participation, complete exorcism and restored consciousness (Gyamfi et al., 2018; Kpobi & Swartz, 2018a; Osafo et al., 2015). Self-care and community participation are often assessed through consumers’ ability to perform daily living activities such as eating, dressing, exercising self-restraint and meaningful participation in social interactions (Osafo et al., 2015). These outcome indicators seem to correspond to what is used in biomedical treatment, which includes changes in the current and future mental health problems of consumers. For instance, biomedical treatment draws on the clinical outcomes (symptomatology, recovery, social disability and admission rates) and consumer perception (symptoms, functioning, quality of life and satisfaction) to measure the outcome of a treatment.
Several studies report that faith-based and traditional healing services tend to attach greater efficacy to their treatment processes than do the advocates of biomedical treatment methods (Kpobi & Swartz, 2018a). In particular, faith healers from Islamic perspectives are reported to perceive their healing strategies as more efficacious than biomedical treatment, mainly because of their use of certain words representing their deity (Kpobi & Swartz, 2018a).
Challenges facing faith and traditional healing service providers
The reviewed studies indicate that faith-based and traditional healing services face several difficulties in providing treatment to consumers. These challenges include the stigmatisation of people with mental illnesses and the services offered to them, abandonment of consumers by family caregivers, limited training in mental health services and inadequate resources (funds and materials; Arias et al., 2016; Asamoah et al., 2014). Several reviewed studies highlighted that the congregation at Christian healing centres and family members stigmatise consumers in their process of receiving treatment (Arias et al., 2016; Asamoah et al., 2014). Conversely, family members may abandon consumers at faith-based and traditional healing service centres, mostly due to stigmatisation and the burden of caregiving. In addition, faith-based and traditional healing practitioners have limited training in mental health services to suitably address the needs of consumers. These faith-based service providers (i.e. pastors) have largely been trained in theology and have limited knowledge of mental health-related issues (Asamoah et al., 2014).
Collaboration between biomedical and faith and traditional healing service providers
Evidence from the reviewed studies indicates that there is an increasing desire for collaboration between biomedical and faith and traditional healing services (Ae-Ngibise et al., 2017; Ae-Ngibise et al., 2010; Agyapong, Osei, Farren, & McAuliffe, 2015; Arias et al., 2016; Asamoah et al., 2014; Kpobi & Swartz, 2018a; Ofori-Atta, Read, Lund, & MHaPP Research Programme Consortium, 2010). Several studies note that biomedical and faith-based and traditional healing service providers currently collaborate informally (Ae-Ngibise et al., 2017; Ae-Ngibise et al., 2010; Agyapong et al., 2015; Arias et al., 2016; Asamoah et al., 2014; Kpobi & Swartz, 2018a; Ofori-Atta et al., 2010). This is mainly ascribed to the recognition that medical knowledge and biomedical treatment contribute to mental illness treatment. In addition, such services collaborate in order to increase their perceived legitimacy and pursue formal recognition (Arias et al., 2016; Kpobi & Swartz, 2018a). Herbalist practitioners who situate themselves between biomedical and indigenous knowledge also seek collaboration from biomedical professionals (Kpobi & Swartz, 2018a).
The extant estimates suggest that about 1%–20% of mental health workers in hospitals and primary health care (PHC) settings have had contact with faith or traditional healer (Ofori-Atta et al., 2010). The reviewed literature suggests that 75% (e.g. 123 out of 164 Community Mental Health Workers (CMHWs) have previously collaborated with faith-based and traditional healing services, particularly on providing training in mental health activities as well as promoting social services to consumers (Agyapong et al., 2015). Similarly, several prayer camps have informal referral relationships with local hospitals and psychiatric units (Arias et al., 2016). Faith-based and traditional healing practitioners are reported to occasionally advise consumers who have obvious physical medical conditions to seek health services from health facilities for evaluation, prior to the initiation of faith and traditional healing (Arias et al., 2016). Faith-based practitioners permit these service users to take medication from health facilities concurrent with fasting and praying (Arias et al., 2016).
The reviewed evidence suggests several methods for facilitating potential collaboration between biomedical and faith-based and traditional healing treatment strategies (Ae-Ngibise et al., 2010; Doku et al., 2011; Osafo, 2016; van der Watt et al., 2017). These factors can be categorised into education, training (Ae-Ngibise et al., 2010; Osafo, 2016), financial support (van der Watt et al., 2017) and guidance through protocols and regulations (Ae-Ngibise et al., 2010; van der Watt et al., 2017). Further, there are calls for mental health professionals to incorporate spiritual assessment into their training programmes (Osafo, 2016) and regulate the activities of faith-based and traditional healing service practitioners with a view to preventing human rights abuse (Doku et al., 2011).
Collaboration between biomedical and faith-based and traditional healing service providers is perceived to offer the potential for improving treatment for consumers. For example, a randomised controlled trial that investigated the effectiveness of integrated traditional faith and mental health services has demonstrated the efficacy of the collaborative approach to treatment for consumers (Ofori-Atta et al., 2018). The intervention group in the randomised controlled trial paid an average of three (of four) visits to psychiatric facilities compared with the control group that paid 2.79 visits. The consumers in the intervention group were far more likely to receive treatment medication compared with the control group (i.e. 86.5% vs 15.7%; Ofori-Atta et al., 2018). Further, compared with the control group, the consumers in the intervention group had significantly limited symptom levels of thinking disturbance, hostility and suspiciousness as well as quality lifestyle (Ofori-Atta et al., 2018).
Barriers to collaboration
The reviewed studies highlight several barriers that can hinder collaboration between biomedical and faith-based and traditional healing services (Ae-Ngibise et al., 2010; Arias et al., 2016; Asamoah et al., 2014; Kpobi & Swartz, 2018a; Osafo, 2016; Roberts, Mogan, & Asare, 2014; van der Watt et al., 2017). These potential barriers are categorised according to individual practitioners and health system-related issues. The barriers associated with individual practitioners concern attitude and prejudice (Ae-Ngibise et al., 2010; Asamoah et al., 2014; Osafo, 2016; van der Watt et al., 2017), the perceived efficacy of treatment (Ae-Ngibise et al., 2010; van der Watt et al., 2017) and differences in the treatment process (Arias et al., 2016; Kpobi & Swartz, 2018a). The health system barriers included a lack of policy and regulation (Ae-Ngibise et al., 2010; Roberts et al., 2014), a limited number of biomedical service providers and financial support and geographical constraints (van der Watt et al., 2017).
Several of the reviewed studies suggest that both biomedical and faith-based practitioners have negative attitudes, especially distrust, which impede potential collaboration (Ae-Ngibise et al., 2010; Asamoah et al., 2014; Kpobi & Swartz, 2018a; Osafo, 2016; van der Watt et al., 2017). These attitudes and behaviours could be attributed to the different methods used for treating consumers by these practitioners. In some instances, the faith-based and traditional healing service practitioners oppose the practices of fasting and praying concurrent with taking psychotic medications. The faith-based and traditional healers argue that the psychotic medications may have negative side effects, preventing consumers from fasting and praying as part of taking faith-based healing (Arias et al., 2016). Alternatively, biomedical practitioners argue that the practices of faith-based and traditional healing services such as forced fasting, physical beatings, chaining and forced confinement are typical examples of potential human rights abuses (Ae-Ngibise et al., 2010).
Discussion
This review offers evidence of treatment pathways for mental health in Ghana. The reviewed studies indicate that mental illness in Ghana is treated using a mixture of biomedical, faith-based and traditional healing services. Initial studies suggest that the treatment modalities of mental health services may overlap and thus collaborating can potentially enhance treatment and healing.
Evidence from the quantitative studies suggests biomedical treatment as the preferred mental health service. In contrast, evidence from the qualitative studies suggests that consumers choose faith-based practitioners and traditional healers as their default or favourite source of treatment. In many cases, a mental illness in Ghana is treated using a mixture of biomedical and faith-based and traditional healing services. In particular, faith and traditional healing pathways are typically used as an initial source of cultural assessment before seeking biomedical treatment. The findings demonstrate that the treatment modalities intersect at a point where consumers have visited faith-based and traditional healing services and have subsequently accessed biomedical treatment. This finding confirms the pathways to treating mental illness in low-income countries, particularly in Africa (Adelufosi et al., 2013; Adeosun et al., 2013; Burns & Tomita, 2015; Giasuddin et al., 2012). Consumers who access biomedical treatment initially visit general practitioners before being referred to a psychiatric facility. Given the existence and potential utility of a mix of biomedical treatment and faith-based and traditional services, it would be appropriate to adopt a mixed-methods approach to examine the treatment pathways to mental health and further seek data convergence and complementarity. Qualitative data may provide a better understanding of consumers’ experiences of illness and reported symptoms, while the quantitative approach may assist in understanding pathway linkages. The findings from such a mixed-methods study could inform the future design of treatment pathways for consumers of mental health services.
This review illustrates a growing desire and interest in establishing formal collaboration between biomedical and faith-based and traditional healing services (Ae-Ngibise et al., 2017; Ae-Ngibise et al., 2010; Agyapong et al., 2015; Arias et al., 2016; Asamoah et al., 2014; Kpobi & Swartz, 2018a; Ofori-Atta et al., 2010). The call for recognising faith-based and traditional healing services is ascribed to the fact that such services are part of the historical cultural beliefs surrounding illness. Therefore, complementing such services with biomedical treatment can provide a holistic, culturally valid approach to consumers. Indeed, some biomedical and faith-based and traditional healing service providers have informally collaborated through informal referrals, training, advocacy and concurrent use of medication alongside faith-based treatment (fasting and praying). The desire to formally recognise and facilitate collaboration may potentially improve treatment processes and outcomes. Such collaboration can facilitate the early detection of conditions and adherence to medication and address recovery-oriented service delivery. In addition, the collaboration may also facilitate the development of a stronger biomedical knowledge base for faith and traditional service providers. In summary, collaboration can provide more holistic mental health services – congruent with common explanations of illness – and would, therefore, increase access to services, compliance with treatment models and medication use, leading to improved outcomes. Biomedical treatment providers working with traditional healers can also potentially improve their knowledge about the treatment, which is evidenced based and efficacious.
Our review identified several barriers that hinder potential collaboration between biomedical and faith-based and traditional healing service providers. These barriers are largely attributed to individual practitioners and health system factors. Individual impediments to collaboration include negative attitudes and prejudice against practitioners, perceived poor efficacy of practitioners’ treatment and differences in treatment processes (Ae-Ngibise et al., 2010; Asamoah et al., 2014; Osafo, 2016; van der Watt et al., 2017). These impediments are equally relevant to biomedical and faith-based and traditional practitioners. The evidence suggests that both biomedical and faith-based and traditional healing providers exhibit reciprocal negative attitudes and distrust and engage in undesirable accusations and counter-accusations against each other. The negative attitudes and accusations stem from an inherent cultural perspective that mistrusts biomedical practices and perceives such services as unappreciative of the historical artefacts surrounding traditional healing. These attitudes and associated behaviours impede potential collaboration. Similarly, health system barriers, such as lack of policy and regulation, limited availability of mental health professionals, limited financial support and geographical isolation, constitute additional obstacles to collaboration (Ae-Ngibise et al., 2010; Roberts et al., 2014; van der Watt et al., 2017). The findings advise governments to address these weaknesses in the current mental health system for the sake of effective collaboration.
Despite the existing barriers, our review suggests that collaboration can be strengthened through the provision of several support mechanisms for both faith-based and traditional healing and biomedical service providers. These support mechanisms include education, training, financial support and guiding protocols and regulations (Ae-Ngibise et al., 2010; Doku et al., 2011; Osafo, 2016; van der Watt et al., 2017). Specifically, education support can be provided to faith-based and traditional healing service providers through participatory training workshops, manuals and toolkits. In particular, the participatory workshops can occasionally bring together biomedical services providers, family caregivers, consumers and faith-based healing service providers. This can equip faith-based and traditional healing service providers with knowledge about biomedical services and the need to foster collaboration. Furthermore, the pre-service and in-service curriculum and modules used to train mental health professionals should incorporate the activities of faith-based and traditional healing services, spirituality and religious-cultural beliefs (Doku et al., 2011; Osafo, 2016). This may equip mental health professionals with the understanding of alternative approaches to mental illness based on tradition and culture (regardless of illness outcomes), which is necessary for effective collaboration with faith-based and traditional healing service providers.
Limitations
This review has several limitations, which are largely pertinent to the search words, language, scope and the period from which the articles were selected. The review was limited to studies that had been conducted in Ghana, published in English and released between 2000 and June 2018. The scope of the study inevitably omitted the relevant articles published before 2000 as well as those in other languages. However, the combination of clearly articulated search methods, consultation with research librarians, a review process that included multiple experts and a critical appraisal tool that allowed measuring the methodological quality helped address these limitations.
Conclusion
Our review identified 26 papers that had studied the pathways to treating mental illnesses in Ghana. The review demonstrated that mental illnesses in Ghana are treated using biomedical and faith-based and traditional healing services. Consumers may access faith-based and traditional healing services as an initial source of mental health service before accessing biomedical treatment. Our findings suggest that the consumers who seek biomedical treatment initially visit their general practitioners before a referral to a psychiatric facility. Traditional healers are not part of a formal referral pathway and are largely sought out by indigenous and faith-oriented consumers because of religious and/or cultural beliefs and rituals surrounding mental illnesses.
The review indicates that biomedical and faith-based and traditional healing service providers continue to express interest in collaborating in the treatment process. However, several individual and health system factors jointly hamper establishing such collaboration. The individual factors reflect negative attitudes and behaviours which are amplified by systemic barriers, including lack of policy and regulations, limited availability of mental health professionals, limited financial support and geographical distance.
Implications for policy and future research
Given the empirical evidence of treatment pathways used for mental health services in Ghana, this is however far from comprehensive. The existing evidence about treatment pathways largely addresses faith-based and traditional healing service providers and mostly uses qualitative approaches with relatively little evidence arising from quantitative approaches. Based on the findings from this review, we can make several recommendations for policy and clinical practices:
Policy, regulations and financial incentives should be developed to facilitate collaboration between biomedical, nursing and faith-based and traditional healing services;
Advocacy for and awareness about the existing pathways to treating mental health services should be funded and prioritised in policy initiatives;
Current mental health services should be focused on recovery-oriented practices that incorporate traditional and faith-healing services;
Adequate training and educational support should be provided to both biomedical, faith-based and traditional healing service providers to foster effective collaboration. Specifically, education support for faith-based and traditional healing service providers can be delivered through participatory training workshops, provision of guiding protocols or manuals and toolkits. In addition, the pre-service and in-service curriculum for training mental health professionals should incorporate modules on faith-based healing, spirituality and religious-cultural beliefs.
In addition, based on the current findings, the following suggestions are offered for future research:
Researchers and clinicians interested in mental health issues should attempt to explore the juxtaposition of biomedical and faith-based treatment of mental health services in Ghana;
Research on mental health services should use interventional design to examine the effectiveness of recovery-oriented practices that incorporate faith-based and traditional healing services;
Research on treatment pathways for mental health services should use a mixed-methods approach, which is capable of gaining the perspectives of community members, consumers and mental health professionals.
Supplemental Material
Quality_assessment_tool – Supplemental material for Pathways to mental health treatment in Ghana: Challenging biomedical methods from herbal- and faith-healing perspectives
Supplemental material, Quality_assessment_tool for Pathways to mental health treatment in Ghana: Challenging biomedical methods from herbal- and faith-healing perspectives by Eric Badu, Rebecca Mitchell and Anthony Paul O’Brien in International Journal of Social Psychiatry
Footnotes
Acknowledgements
The authors wish to thank the University of Newcastle Graduate Research Australia for the Doctoral Scholarship offered to the lead author (E.B.). The authors are also grateful to Debbie Booth, the librarian, for supporting the literature search.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.