
Abstract
Background:
The lay public often conceptualise mental disorders in a different way to mental health professionals, and this can negatively impact on outcomes when in treatment.
Aims:
This study explored which disorders the lay public are familiar with, which theoretical models they understand, which they endorse and how they compared to a sample of psychiatrists.
Methods:
The Maudsley Attitude Questionnaire (MAQ), typically used to assess mental health professional’s concepts of mental disorders, was adapted for use by a lay community sample (N = 160). The results were compared with a sample of psychiatrists (N = 76).
Results:
The MAQ appeared to be accessible to the lay public, providing some interesting preliminary findings: in order, the lay sample reported having the best understanding of depression followed by generalised anxiety, schizophrenia and finally antisocial personality disorder. They best understood spiritualist, nihilist and social realist theoretical models of these disorders, but were most likely to endorse biological, behavioural and cognitive models. The lay public were significantly more likely to endorse some models for certain disorders suggesting a nuanced understanding of the cause and likely cure, of various disorders. Ratings often differed significantly from the sample of psychiatrists who were relatively steadfast in their endorsement of the biological model.
Conclusion:
The adapted MAQ appeared accessible to the lay sample. Results suggest that the lay public are generally aligned with evidence-driven concepts of common disorders, but may not always understand or agree with how mental health professionals conceptualise them. The possible causes of these differences, future avenues for research and the implications for more collaborative, patient–clinician conceptualisations are discussed.
Introduction
A significant body of research points to differences in how the lay public, and mental health professionals, conceptualise common mental disorders (Furnham & Chan, 2004; Giosan, Glovsky, & Haslam, 2001; López & Guarnaccia, 2000). This is concerning as disagreements between patient and clinician about the nature of the problem and how it is best treated are associated with decreased engagement, lower treatment adherence and ultimately poorer treatment outcomes (Fuertes, Boylan, & Fontanella, 2009; Horvath & Symonds, 1991). Such disparity was first publicly acknowledged as an issue in clinical practice in the United Kingdom with the advent of the Royal College of Psychiatry Stigma Campaign, which aimed to reduce this discrepancy by improving the public’s ‘mental health literacy’ (Cowan & Hart, 1998). Thornicroft (2000), in the National Service Framework for Mental Health, also called for clinicians to acknowledge and incorporate the autonomy of patients and their concepts of mental health into their clinical assessments and treatment plans. However, despite both professional and political acknowledgement of the importance of this shift, evidence has continued to demonstrate a lack of shared clinical decision making between patients and professionals (Dunn, 2004). An important first step in addressing this issue is investigating how the lay public intuitively conceptualise common disorders and how they differ with treating professionals.
In an attempt to gain a better understanding of how psychiatrists conceptualise mental disorders, Harland et al. (2009) developed the Maudsley Attitude Questionnaire (MAQ). The MAQ was designed to capture attitudes consistent with biological, cognitive, behavioural, psychodynamic, social realist, social constructionist, spiritual and nihilist models in a sample of psychiatrists. Predictably, Harland found that the biological model was favoured overall but that there were systematic variations in the strengths of endorsements per disorder, for example, the biological model was the most strongly endorsed model for schizophrenia and least strongly endorsed for antisocial personality disorder (APD) and so forth. Recently, Read et al. (2017) applied the same tool to a sample of clinical psychologists and examined how the two professions differ. Psychiatrists and psychologists were found to sit on opposite ends of a biological–psychosocial continuum, providing concrete evidence of where the two professions often clash in conceptualising mental disorder. In this study, an adapted version of the MAQ was administered to a sample of the lay public in order to investigate (1) if the MAQ can reliably capture the lay public’s concepts of mental disorder, (2) which disorders they consider themselves best informed about, (3) which, if any, explanatory models they endorse as a ‘best fit’ per disorder, and (4) where differences may rest with Harland’s original sample of psychiatrists.
Method
Research tool
The adapted MAQ consists of two sections. The first comprises 16 items related to demographic background, and the second includes 38 items designed to probe respondents’ perceived level of knowledge and the concepts they hold specific to common mental disorders; their aetiology, classification, research areas and treatment. Items probe for the endorsement of eight specific models: biological, cognitive, behavioural, psychodynamic, social realist, social constructionist, spiritualist and nihilist, in relation to four specific disorders: schizophrenia, major depressive disorder (MDD), generalised anxiety disorder (GAD) and APD (as defined by Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV)). In order to examine what models were endorsed for each disorder, a 5-point Likert-type scale was used for responses to statements, for example, ‘this disorder arises as a result of social circumstances or conditions’ (probing for the presence of a belief endorsing a social realist model). Responses range from 1 ‘strongly disagree’ to 5 ‘strongly agree’. The MAQ was originally designed for the use by trainee psychiatrists. To examine lay comprehension of psychiatric concepts as represented by the MAQ, a number of adaptations were made. First, four items were added that asked respondents to indicate the extent of their knowledge related to individual disorders ‘I have a good understanding of this disorder [Schizophrenia, MDD, GAD, APD]’. Second, an additional comprehension scale was added to each of the statements in section 2 for respondents to rate how well they understood the statement. The addition of this scale provided some insight as to the appropriateness of this questionnaire for lay samples and allowed for the examination of the level of understanding in relation to specific models commonly used to conceptualise disorders.
Procedure
Ethical approval was granted by the University of Hertfordshire Life and Medical Sciences Ethics Committee. Participants were volunteers responding to an advertising campaign both on social media and around a university campus. All participants were aged over 18 years. Any individuals who were studying a course or working in a profession related to mental health were excluded. The comparison group, Harland’s sample of psychiatrists, were sampled from the South London and the Maudsley National Health Service (NHS) Foundation Trust. Every junior- and senior-grade psychiatrist in training was approached by post and email. A total of 90 trainees were approached, and 76 returned completed questionnaires, giving a response rate of 84%. Data for this sample were obtained via contact with the authors.
Analysis
Mean model endorsement was calculated by the summation of the four features: aetiology, classification, research and treatment for each of the models per respondent. The summed scores provided an overall score for the model, which could then be calculated for the four disorders (i.e. a summed score was calculated for the cognitive model when applied to the disorder schizophrenia etc.). Repeated measures analysis of variance (ANOVA) was used to explore whether lay populations apply different models to different disorders. Multivariate analysis of variance (MANOVA) was used to compare data from the current sample with the findings of Harland et al., who applied the MAQ with a sample (N = 76) of psychiatrists.
Results
Characteristics of respondents
Respondents were 160 lay community members with a mean age of 36.5 (SD = 3.81). In total, 97 females (60.6%) and 63 males (39.4%) participated.
Lay understanding of specific disorders
Section 2, item 13 ‘I have a good understanding of this disorder [Schizophrenia, MDD, GAD, APD]’ was designed to probe perceived knowledge of specific disorders. Scores were aggregated across respondents, per disorder, with a score of one denoting a strong disagreement with the statement and a five denoting a strong agreement. Participants reported that they best understood MDD (M = 3.61, SD = 0.82), followed by GAD (M = 3.28, SD = 0.85), schizophrenia (M = 3.04, SD = 0.82) and finally APD (M = 2.58, SD = 0.82). A one-way repeated measures ANOVA found significant differences in knowledge across disorders, F(2.61, 414.81) = 55.31, p < .001, η2 = .26. A Greenhouse-Geisser correction was applied to account for the violation of sphericity (ε = .87; Field, 2005). Post hoc comparisons using the Bonferroni correction showed a significant difference (p < .001) between perceived knowledge of all models other than schizophrenia and GAD (p = .67).
Lay understanding of specific models
Each questionnaire item was accompanied by a comprehension scale; ‘I fully understand the statement’. Again, respondents chose from 1 (denoting a strong disagreement) to 5 (denoting a strong agreement). Comprehension scales were also summed across all questionnaire items, providing a measure of mean item comprehension for the questionnaire as a whole. Mean scores indicate respondents perceived their overall level of comprehension to be moderate to good (M = 3.72, SD = 0.69). Comprehension items were aggregated by model. When ordered from most to least understood, the spiritualist model was best understood (M = 4.11, SD = 0.58), followed by the nihilist model (M = 4.05, SD = 0.58), social realist model (M = 4.02, SD = 0.61), biological model (M = 3.31, SD = 2.93), psychodynamic model (M = 3.41, SD = 0.82) and finally the behavioural model (M = 3.49, SD = 0.75). A one-way repeated measures ANOVA revealed a significant effect of model on comprehension, F(5.12, 813.80) = 78.31, p < .001, η2 = .26. A Greenhouse-Geisser correction was applied to account for the violation of sphericity (ε = .73).
Lay model endorsement
In order to examine differences in model endorsement by respondents, a two-way repeated measures ANOVA was conducted. Greenhouse-Geisser corrections were applied to account for the violations of sphericity (ε = .80 for the main effects of model, ε = .85 for the main effects of disorder and ε = .52 for the interaction). The main effect of the model was significant (F(5.60, 891) = 199.43, p < .001), as was disorder (F(2.55, 404.65) = 38.97, p < .001) and the interaction between model and disorder (F(10.1, 1611.70) = 2.70, p < .001). Mean model endorsement per disorder for both the lay and Harland’s sample of psychiatrists can be found in Table 1.
Descriptive statistics for model endorsement per disorder for both Lay (N = 160) and psychiatrist (N = 76) samples.
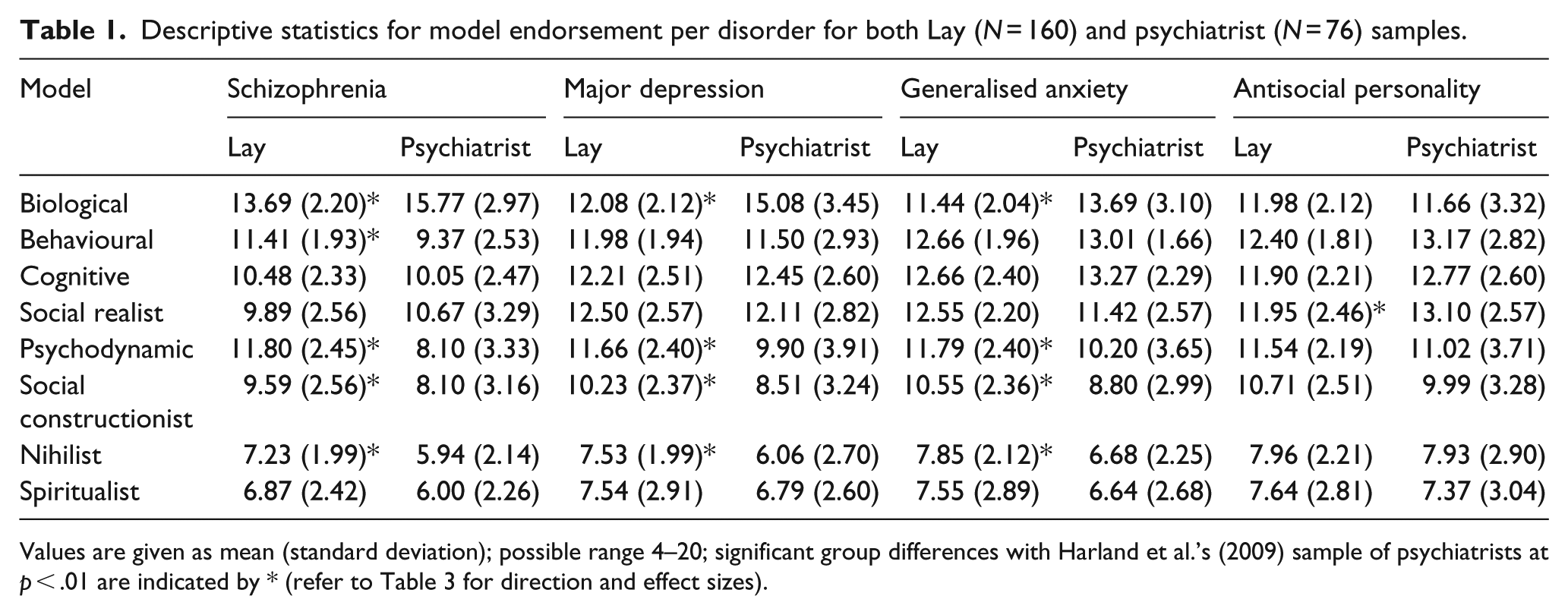
Values are given as mean (standard deviation); possible range 4–20; significant group differences with Harland et al.’s (2009) sample of psychiatrists at p < .01 are indicated by * (refer to Table 3 for direction and effect sizes).
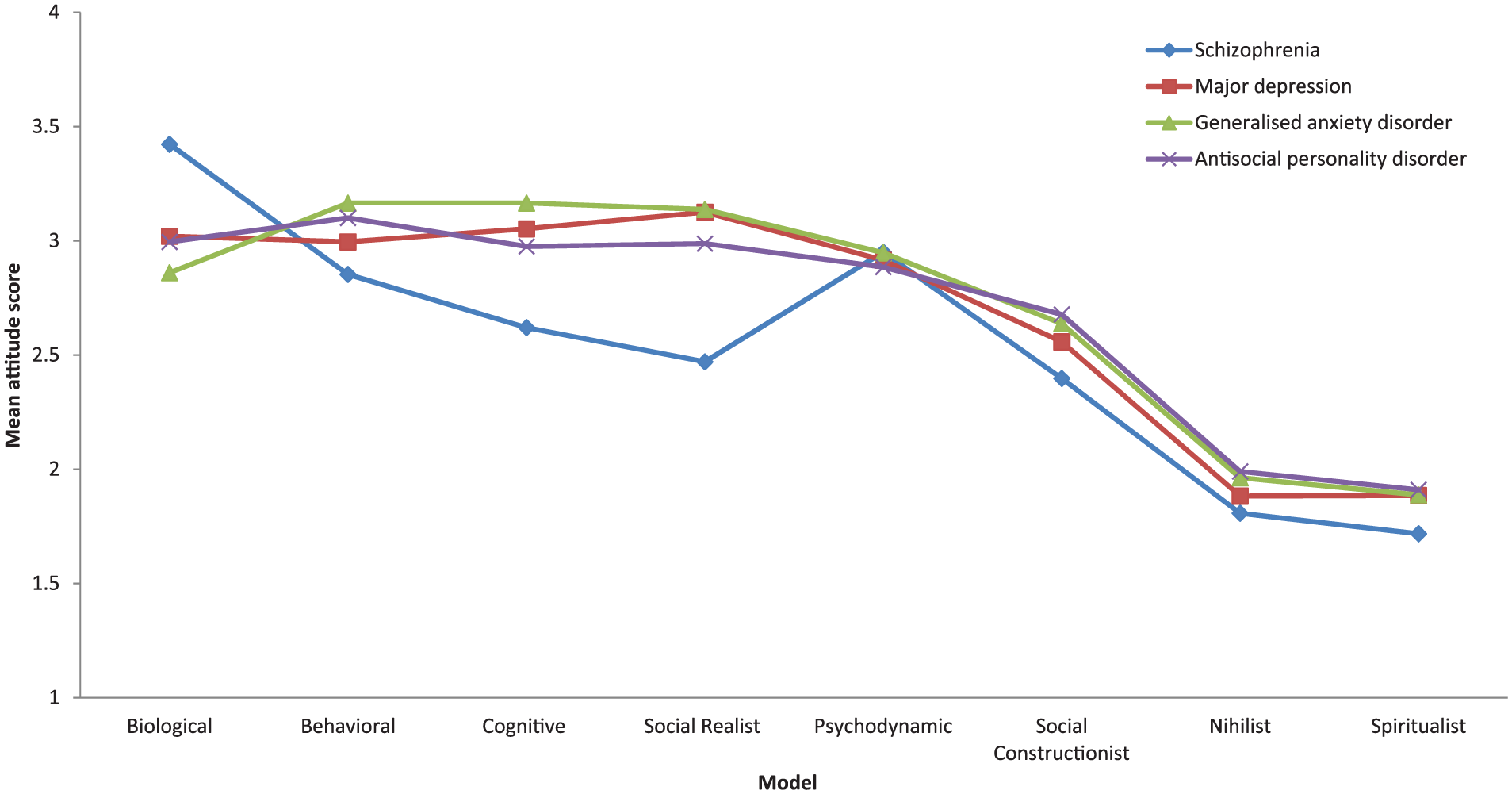
To examine the interaction effect of model and disorder, comparisons were drawn using eight separate one-way repeated measures ANOVAs. Post hoc pairwise comparisons were conducted (see Table 2). In terms of sequencing from the most to the least endorsed model (irrespective of disorder), the lay sample were most likely to endorse the biological model, followed by behavioural, cognitive, social realist, psychodynamic and social constructionist. Figure 1 provides a visual illustration of the data for the lay sample with model endorsement arranged in descending order. In relation to endorsing a specific model for a disorder, mean Likert-type scores ranged from 3.42 (biological model for schizophrenia), where the level of model endorsement was relatively high and therefore seen as a relatively ‘good fit’, to 1.91 (spiritualist model for APD), where the model is seen as a ‘poor fit’ for the disorder.
Effect sizes (d) for comparisons of the interaction effect of model by disorder for the lay sample.

GAD: generalised anxiety disorder; APD: antisocial personality disorder; ns: not significant; MD: major depression.
Values are given as d and p. Values that are both significant and have a medium to large effect size (d > 0.5) are given in bold.
p < .01; **p < .001.
Mean aggregate scores for the lay sample on a 1–5 scale (1 = strongly disagree, 3 = neutral and 5 = strongly agree).
Comparisons of lay sample with Harland’s sample of psychiatrists
To examine any differences in model endorsement between the lay and psychiatrist samples, a MANOVA was performed. Using Pillai’s trace, there was a significant effect of sample on model endorsement (V = .243, F(8, 227) = 9.12, p < .001, d = .243). However, Levene’s and Box’s tests indicated that assumption of equality of variance and homogeneity was not met. These violations were likely due to the comparatively small size of the psychiatrist sample (N = 76). In these circumstances, analyses can proceed, but with due caution (Tabachnick & Fidell, 2007). Univariate ANOVAs with a Bonferroni correction were applied. Comparisons were made per model and revealed significant differences in level of endorsement between psychiatrists and the lay sample across some, but not all, models. The biological model was endorsed by the psychiatrists at a significantly greater level (p < .001) than the lay sample for all disorders apart from APD with acceptable (d > .04) to moderate (d > .25) effect sizes (12), whereas the psychodynamic, social constructionist and nihilist models were all endorsed to a significantly greater level by the lay sample with all disorders apart from APD (p < .00, d > .04). Significance levels and effect sizes for the cross sample univariate ANOVAs can be found in Table 3.
Effect sizes (d) for differences between the lay and psychiatrist samples for the effect of model by disorder.
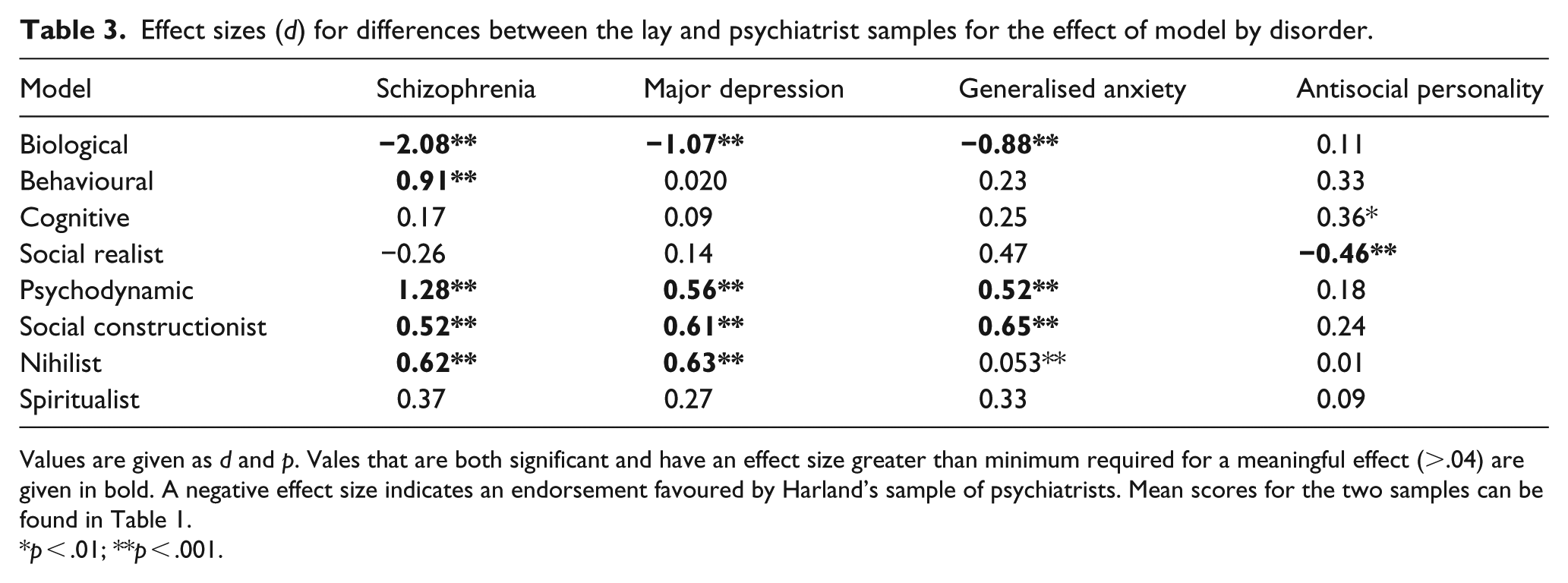
Values are given as d and p. Vales that are both significant and have an effect size greater than minimum required for a meaningful effect (>.04) are given in bold. A negative effect size indicates an endorsement favoured by Harland’s sample of psychiatrists. Mean scores for the two samples can be found in Table 1.
p < .01; **p < .001.
Discussion
This study used the Maudsley Attitudes Questionnaire to examine differences in how the lay public and psychiatrists conceptualise common mental disorders. The addition of the comprehension scale to the MAQ, its use with a lay sample and as a comparison tool with a sample of psychiatrists, has provided some useful findings. Generally, the MAQ appears to be accessible to the lay public, warranting further research to fully test its psychometric properties across different groups. At a practical level, the comprehension scale also provided some insight as to where the use of clinical language may unnecessarily impede a shared conceptualisation between patient and professional, factors explored later in this discussion.
First though, given the preliminary nature of this study, it is important to note methodological issues that give rise to future avenues of research for this tool. As noted by Read et al., the psychometric properties for this tool are not fully known, and construct validity was not tested for this adapted version – an important next step in the advancement of the MAQ. In this study, samples were not recruited equally; the psychiatrist sample was small, targeted (as opposed to self-selecting in the lay sample), drawn from a single site and taken at an earlier date than the lay sample, limiting the reliability and generalisability of the direct comparisons. Future studies using the MAQ as a comparison tool will benefit from simultaneous, identical and systematic recruitment methods. It is also important to note the limitations of a questionnaire in examining a multifactorial phenomena. As noted in prior studies (e.g. Blaxter, 1983), when considering concepts of illness, multiple variables are likely to interact in ways that may be difficult to detect using a questionnaire. Future studies may want to consider a mixed quantitative and qualitative method to provide greater richness to the findings. Nonetheless, the novel use of the MAQ for a lay sample has allowed for an exploration of the depth of the public’s understanding of a broad variety of models applied to common mental disorders. It has probed for the presence of eight separate models that had not previously been examined with the lay public, and the direct comparison with Harland’s sample of psychiatrists has provided a useful initial insight as to where differences between psychiatric and lay concepts of the same disorder may rest. Comparisons across other allied professions, particularly those found in multi-disciplinary mental health teams, where collaboration is so important, is an interesting avenue for future research.
The lay public in this sample viewed themselves as best informed about MDD, followed by GAD and then schizophrenia – those disorders that have received greatest public health investment (McCrone, Dhanasiri, Patel, Knapp, & Lawton-Smith, 2008) . They reported having a poor understanding of APD, and this was reflected in the breadth of models they endorsed for the disorder, appearing to show greatest variability where knowledge was perceived to be at its weakest.
On the whole, the lay sample appeared somewhat aligned with the models of mental disorder currently endorsed by the NHS via the National Institute of Health and Care Excellence (NICE), favouring biological, behavioural and cognitive models. Their conceptualisations were obviously less defined than the comparative sample of psychiatrists; however, as in prior studies (Furnham & Anthony, 2010; Furnham & Kuyken, 1991; Jorm et al., 1997; Lauber, Nordt, Falcato, & Rössler, 2001), the two samples were found to hold some consistent views with regard to the aetiology and treatment of specific disorders.
Lay respondents showed the greatest understanding but the least support for the less scientifically orientated models such as the spiritualist and nihilist models. Conversely, they showed the least understanding but greatest support for the more technical, evidence-based interventions such as the biological, behavioural and cognitive models. The seemingly counter-intuitive drive to endorse the models about which the least is known warrants further attention. Perhaps, the participants were merely conforming to the ‘good participant role’ in endorsing models that are assumed to be aligned with the researchers views, or their response could be attributed to a ‘complexity bias’ (Klayman, 1995), a logical fallacy that prioritises complex solutions, even ones we cannot fully understand. A third plausible explanation is that the lay sample were already invested in the more evidence-driven models of intervention as a whole, but simply struggled to understand some of the complicated clinical language used in this study, and so frequently in clinical practice. An examination of the relationship between the complexity of language used to conceptualise mental disorders and service users’ willingness to engage in a treatment is also an interesting avenue for future research.
Overall, both samples prioritised the biological model as reflected in the high level of endorsement for the statement, ‘the disorder results from brain dysfunction’ (biological model, concerning aetiology). The model as represented in the MAQ conceptualises mental disorder as organic – a neurological abnormality that should be researched and treated accordingly. The predominance of a biological model has been found in some (Angermeyer, Breier, Dietrich, Kenzine, & Matschinger, 2005), but not all (Link, Phelan, Bresnahan, Stueve, & Pescosolido, 1999), prior research concerning lay populations. Its predominance is curious. Over the past 20 years, there have been significant efforts within the scientific community to link our biology-specific alleles to specific mental disorder without great progress (Keller, 2008). Indeed, there is increasing recognition of the phenotypic and genotypic variation within specific disorder (Adriaens, 2007). The allure of biological psychiatry, the belief that mental disorders are distinct categorical entities, with fixed internal properties has been greatly discussed and critiqued (e.g. Cooper, 2005); yet, it perseveres in some mental health professions and the lay public. Its predominance among psychiatrists is perhaps unsurprising, given their primary training is biologically based. In Harland’s sample of trainee psychiatrists, their endorsement of the biological model appears particularly strong, a propensity that has been found to be inversely proportional to overall number of years in clinical practice (Ahn et al. 2006), suggesting an increasing appreciation for the multifactorial nature of many mental health difficulties. It is less obvious why the lay public prioritise biological concepts to understand mental health issues. From an evolutionary perspective, it has been argued that we are predisposed to categorise mental disorder to identify poor adaptation in others and threats to the survival of our genes (Carruthers, 2006). Equally, cognitive scientists have asserted that simple, essentialist categorisations like this help us make order from disorder, expedite inferences and reduce the cognitive load in decision making and are thus intrinsically appealing to the layman (Barrett, 2001). At a broader sociological level, it has been argued that increased access to psychiatric treatment (Angermeyer & Matschinger, 2005) or an over representation of biological research with regard to mental illness in the UK media (Lewison, Roe, Wentworth, & Szmukler, 2012) are key factors in the lay public prioritising biologically based conceptualisations of mental disorder. As with the aetiology of mental disorder, the reasons for our preference for a biological model are likely multifaceted.
At a disorder-specific level, some of the differences between the two samples become more evident. As in prior research concerning our understanding of schizophrenia, the biological model was favoured by both samples. However, the behavioural and psychodynamic models also featured in the lay understanding of the disorder, suggesting the lay public also hold an individual’s social circumstance and their early development as factors that may predispose an individual to developing schizophrenia.
For GAD, the lay sample endorsed cognitive and behavioural models to a significantly greater level than for any other disorder, suggesting they view erroneous thinking and unhelpful, learnt behaviour as specific features of GAD, perhaps driven by the recent proliferation of cognitive-behavioural treatments for anxiety disorders (Williams & Marinez, 2008). While the psychiatrists were also likely to endorse cognitive and behavioural models, as with both schizophrenia and MDD, the biological remained their favoured model, perhaps reflecting the primacy of pharmacotherapy in the psychiatric treatments for these conditions. In contrast to the psychiatrists’ prioritisation of the biological model for MDD, the lay public prioritised the social realist model, suggesting they also hold the reality of an individual’s circumstance as significant in maintaining the disorder. Current epidemiological research appears to accommodate both models, with some favouring biological factors (Sullivan et al., 2000) and others environmental (Peyrot et al., 2013), but with both likely lacking explanatory power when considered in isolation.
In reference to the disorder APD, the behavioural model was most endorsed by the lay sample, followed by the biological and social realist models. That they were not endorsed to a significantly greater level than in regard to any other disorder suggests that the lay public hold less defined concepts of APD. Arguably, the public’s lack of knowledge regarding APD is reflected in the punitive attitudes commonly found towards antisocial behaviour, whereby aetiology is far less frequently held in consideration when compared to the treatment of mental illness (Nee & Witt, 2013). Patterns of model endorsement from the psychiatrists were very similar to the lay sample, marking a clear departure from their hitherto primary endorsement of the biological model. This departure may reflect the historical demarcation of ‘mad’ and ‘bad’ behaviour by health professionals, the former commonly viewed as a biological illness typically treated with medication in the health system and the latter a personality trait typically treated punitively within the judicial system (Vossler et al., 2017). Incarceration as a means of treatment has consistently failed to significantly impact on remission and recidivism rates (Lipsey & Cullen, 2007), highlighting inadequacies in how professionals and the public alike currently conceptualise APD and its treatment. This finding highlights the need for public and professional education regarding the causes of APD and a re-evaluation of how it is best treated; a good starting place will be to consider the factors that influence how APD is currently conceptualised and why.
Despite the identified weaknesses, it is clear that the lay public hold some clearly defined views on common mental disorders and that they differentiate how they are best understood and treated. It is also clear that that some clinicians and service users will hold conflicting explanations for the same psychological phenomena. This remains an important area of research as when conceptualisations are not shared between professional and service user, clinical outcomes are likely to be negatively affected. Given the complexity of mental health conditions and the many facets to our understanding of it, it is unlikely that this issue will be resolved in the near future. With so little certainty about the cause of mental disorder, clinicians may benefit from considering both the accuracy and the utility of the conceptualisations they develop together with their clients. This MAQ provides a useful tool with which to further investigate these phenomena.