
Abstract
Background:
Health anxiety may be an increasing problem because of the focus on monitoring health and increasing use of the Internet for self-diagnosis (cyberchondria). There is very little information about changes in the prevalence of health anxiety.
Aim:
We compared the prevalence of health anxiety in four medical clinics in one hospital over a 4-year period using the Health Anxiety Inventory (HAI) as a diagnostic marker.
Method:
Patients attending cardiology, endocrine, gastroenterology and respiratory medicine clinics at King’s Mill Hospital, North Nottinghamshire, completed the HAI while waiting for their appointments. There were eight research assistants involved in collecting data, two in the 2006–2008 period and six in the 2008–2010 period. As a consequence, more data were collected on the second occasion.
Results:
There was an increase in the prevalence of health anxiety from 14.9% in 2006–2008 (54 positive of 362 assessed) to 19.9% (1,132 positive out of 5,704 assessed) in 2008–2010. This increase was primarily noted in gastroenterology clinics (increase of 10%) and not shown in endocrine ones.
Conclusion:
The prevalence of health anxiety is increasing in those who attend medical out-patient clinics. Reasons are given that this may be a possible result of cyberchondria, as the excessive use of the Internet to interpret troubling symptoms is growing. Further studies are needed in other populations, but there is reason to be concerned at this trend as it is likely to increase the number of medical consultations unnecessarily.
Introduction
The diagnosis of health anxiety is a relatively new concept. It is often regarded as a synonym for hypochondriasis, but it is not exactly the same. Although there continues to be some dispute over the subject, health anxiety can probably be regarded as anxious hypochondriasis and is best construed as an anxiety disorder (Scarella, Laferton, Ahern, Fallon, & Barsky, 2016; P. Tyrer, 2018), although there is overlap with obsessional disorders (Stein et al., 2016). It has a more restricted definition than hypochondriasis, as this describes the primary preoccupation with having a disease. It includes considerable depressive pathology, sometimes to the point of delusions, expressed most severely as Cotard’s syndrome (Berrios & Luque, 1999).
The best equivalent of health anxiety is the diagnosis of illness anxiety in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013), which includes the anxious preoccupation with either having or in danger of having a currently undiagnosed medical illness, in which the distress is created not by physical symptoms but by anxiety about their disease implications. In the forthcoming International Classification of Diseases–11th Revision (ICD-11), health anxiety is included under the general diagnosis of hypochondriasis, not very different from that in DSM-5 but including ‘catastrophic misinterpretation of bodily signs or symptoms’ as a feature, which is not always present in people with abnormal health anxiety.
The most likely estimate of its prevalence in the community comes from the Australian National survey in which figures of 6.3% for lifetime prevalence and 3.5% for current prevalence were found (Sunderland, Newby, & Andrews, 2013). This can be regarded as a baseline figure only, and there are suspicions that the condition is increasing in prevalence because of general guidance to people to monitor their own health with the help of apps (Parker et al., 2018) and the growing use of the Internet and social media to advise and diagnose symptoms (Starcevic & Aboujaoude, 2015), including cyberchondria, the repeated use of the Internet to diagnose symptoms unnecessarily, which is very closely linked to health anxiety (Fergus & Russell, 2016), and which has been shown to increase its severity and persistence (Doherty-Torstrick, Walton, & Fallon, 2016). But, despite these suspicions, currently there is no good evidence that the prevalence of health anxiety is increasing and in the current research of our group, we had an opportunity to evaluate this.
Method
Participants
The patients invited to take part in both of these studies were all attending cardiology, respiratory medicine, gastroenterology and endocrinology clinics at King’s Mill Hospital, North Nottinghamshire, UK. This is a general hospital that is fairly typical of general hospitals in the National Health Service (NHS). The patients in each study were assessed for health anxiety but seen for different purposes. The first study was a preliminary one to assess the relationship between health anxiety and other somatic symptoms by comparing scores on a standard scale for assessing health anxiety (Short Health Anxiety Inventory (SHAI); Salkovskis, Rimes, Warwick, & Clark, 2002) and a new one for assessing unexplained symptoms (Schedule for Evaluating Persistent Symptoms (SEPS); H. Tyrer et al., 2013). Patients attending cardiology, respiratory medicine, endocrine and gastrointestinal clinics were selected in the study. There were only a few part-time research assistants available in this study and they visited clinics on an ad hoc basis over a period of 24 months (August 2006 to July 2008). The timing of their visits was organised so that all relevant clinics were covered during the course of the study.
The second study was carried out as a large randomised controlled trial of the efficacy of an adapted form of cognitive behaviour therapy in the treatment of health anxiety, the CHAMP study (P. Tyrer, Cooper, Crawford, et al., 2011; P. Tyrer et al., 2014; P. Tyrer, Cooper, Tyrer, 2011), in which patients were recruited over 20 months between October 2008 and July 2010. In this study, there were many more research staff and they aimed to assess the majority of patients attending cardiology, respiratory medicine, neurological, endocrine and gastroenterology out-patient clinics at King’s Mill Hospital (and five other hospitals across England). For the purposes of the current study, only those attending King’s Mill Hospital were considered.
In both studies, patients attending were invited to complete the SHAI (Salkovskis et al., 2002) to identify those who probably had a significant degree of health anxiety (a score of 20 or more, now accepted as an accurate threshold; Hedman et al., 2015). Those who scored below this threshold were not seen again, and those who scored above the threshold were interviewed again to determine the feasibility of taking part in the full randomised controlled trial. In the second study, patients attending neurological clinics were also seen but they were excluded from the two study comparison. Ethical approval was given by the Derbyshire Research Ethics Committee (06/Q2401/130) for the first study (2006–2007) and by the North Nottingham Research Ethics Committee (08/H0403/56) for the second. The Z-test was used to compare the two proportions of health anxiety score between study 1 and study 2 by clinic type. The difference in the proportion of health anxiety scores together with their 95% confidence interval (CI) were calculated as well as the P-value. A 2-tailed P-value < 0.05 was considered statistically significant. Statistical analysis was performed using Stata 13.
Results
A total of 362 patients were screened in the first study and 5,704 in the second (Table 1). The difference can largely be explained by the research time available for assessment. This was 10 times more (30 hours vs 3 hours per week) in study 2 than in study 1. The number (%) of subjects with SHAI ≥ 20 and statistical analysis results for each of the clinics and in total are shown (Table 1).
Comparison of prevalence of pathological health anxiety (SHAI ≥ 20) over time between 2005–8 (Study 1) and 2008–2010 (Study 2) at King’s Mill Hospital, Notts in four medical clinics.
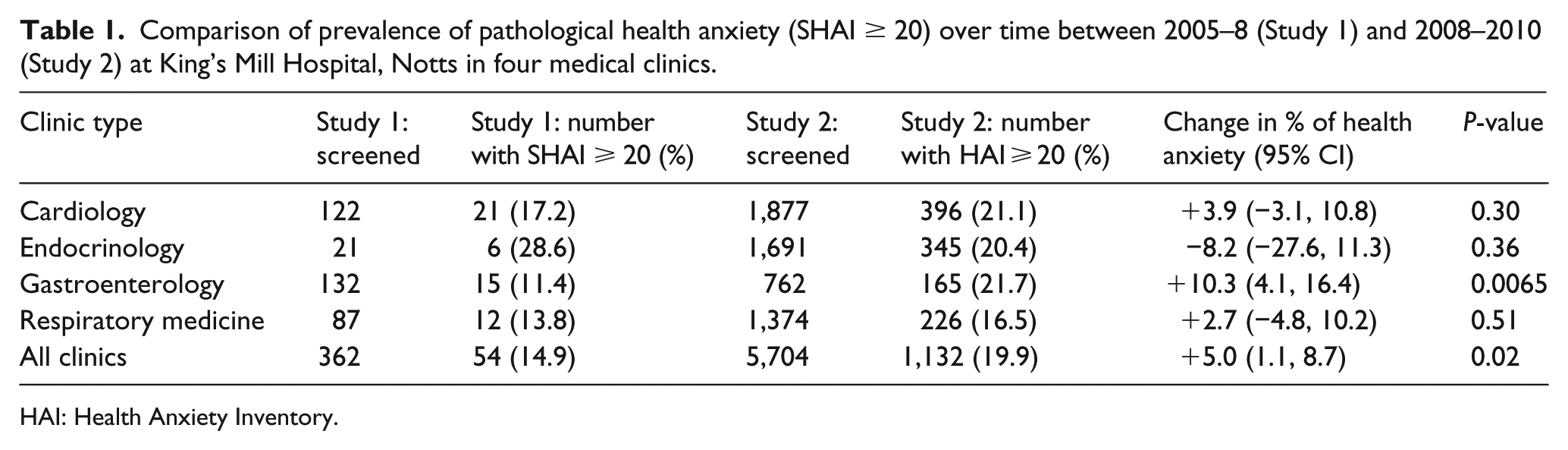
HAI: Health Anxiety Inventory.
Discussion
The result of this study is, we believe, first to show an increase in the prevalence of health anxiety over a relatively short period. Although there have been many suspicions that health anxiety is becoming more frequent, partly because of cyberchondria, this is the first study to show a definite increase, even though it was only over a 2-year period and the increase was not dramatic. The main limitation of the findings is that the two studies were not pre-planned to be linked, but the clinics were identical and the use of the SHAI questionnaire obviated any question of bias. The SEPS scale used in the first study was a project to evaluate its psychometric properties, and other instruments such as the Whitely Index might have been used if these studies had been linked in advance.
Although there was an overall increase in the prevalence of pathological health anxiety, a significant increase was only shown in gastroenterology clinics. This may be related to the much wider use of colonoscopy and endoscopy in recent years and greater attention given to conditions such as irritable bowel syndrome. The level of health anxiety in these patients has been noted to be high and reassurance counterproductive (Gasteiger et al., 2018). This type of patient is likely to be very frequent in gastroenterology clinics.
The other limitation that avoids general conclusions being drawn is that this study was carried out in medical out-patients, a population in which health anxiety is known to be highly prevalent (P. Tyrer, Cooper, Tyrer et al., 2011), and so the results may not generalise to other populations.
One of the major concerns in the health services of today is the increasing focus of personal responsibility in monitoring health, and this is a proper subject to be addressed by social psychiatry, even though most of the people with this disorder present to general hospitals, not mental health services. While the fundamental principles behind this are sound, the dangers of unnecessary worry and concern have been insufficiently recognised. The consequence is unnecessary consultation, over-investigation and preventable suffering (P. Tyrer, Eilenberg, Fink, Hedman, & Tyrer, 2016). Now that there are effective means of treating health anxiety that are cost-effective and long-lasting (Morriss et al., 2019; P. Tyrer et al., 2017). There is a need to redress the balance so that all practitioners become aware of the need to identify health anxiety before it becomes pervasive. The message of this article is that the need for such an initiative is becoming urgent.
Footnotes
Acknowledgements
The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. The authors thank Sandra O’Sullivan, Leila Ali, Faye Cooper, Stephanie Kings, Paula Seivewright, David Trevor and Gemma Walker for their help in collecting data in the two studies.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the Nicola Pigott Memorial Fund and the National Institute for Health Research (NIHR) Health Technology Assessment Programme (Grant Reference No. 07/01/26).