
Abstract
Background:
This study assumes that just as public stigma differs depending on types of mental disorder, so too does self-stigma.
Aims:
This study aims to compare self-stigma among persons with schizophrenia, alcohol use disorder and gambling disorder, and thereby analyze the effects of self-stigma on their self-esteem.
Methods:
A total of 321 Korean adults involved in community mental services for schizophrenia (N = 116), alcohol use disorder (N = 102) and gambling disorder (N = 103) were surveyed (Mage = 40.74, standard deviation (SD) = 10.10, 83.8% male, 16.2% female). Participants were questioned on self-stigma and self-esteem. One-way analysis of variance (ANOVA) was used to compare the self-stigma by mental disorder type. Furthermore, in order to analyze the effects of self-stigma on self-esteem with subjects’ age and educational background controlled, hierarchical regression analysis was used.
Results:
The self-stigma of gambling disorder group was highest not only in overall self-stigma but also some of its subscales – alienation, stereotype endorsement and stigma resistance – followed by alcohol use disorder group and schizophrenia group. In all three groups, self-stigma had a negative effect on self-esteem, while stigma resistance of subscales was the most important predictor. In addition to stigma resistance, alienation was a predictor in the schizophrenia group, alienation and social withdrawal in the alcohol use disorder group and social withdrawal was a significant predictor in the gambling disorder group. Therefore, the predictors of self-esteem differed depending on the type of mental disorder.
Conclusion:
Based on these results, we suggest cognitive-behavioral intervention to raise subject awareness of the unjust social stigma and boost self-advocacy to resist the stigma.
Introduction
Social stigma toward persons with mental disorders limits various social opportunities and meaningful relationships for the afflicted, thereby decreasing their life satisfaction and hindering recovery. If someone recognizes a cue that a person has mental disorders, stereotypes are activated in that person’s thought process. When someone sanctions a negative stereotype, he or she is generating what is called prejudice. Prejudice is a result of cognitive and affective response to stereotype. Discrimination is a behavioral response to the emotion and beliefs generated by prejudice; for instance, social distancing is a common response (Overton & Medina, 2008). Persons with mental disorders become aware of stereotypes that exist about their group. As a result, they may withdraw from social relations and avoid social opportunities. Hence, in a society where social stigma prevails, self-stigma also exists (Vogel, Bitman, Hammer, & Wade, 2013).
Self-stigma is that persons with mental disorders internalize public stigma and apply the stigma to themselves. Accordingly, perception of public stigma contributes to the experience of self-stigma (Vogel, Wade, & Hackler, 2007). Several researchers have reported that individuals who experience self-stigma suffer from hopelessness (Lysaker, Roe, & Yanos, 2007), depression (Sirey et al., 2001), diminished self-esteem and self-efficacy (Seo & Kim, 2004; Vauth, Kleim, Wirtz, & Corrigan, 2007; Verhaeghe, Bracke, & Bruynooghe, 2008), and lowered treatment adherence (Livingston & Boyd, 2010; Tsang, Fung, & Chung, 2010).
Previous studies referred to self-stigma as perceived stigma or internalized stigma. Perceived stigma was used by Link (1987); persons with mental disorders are aware of a set of beliefs on how most people treat mental patients. If they undergo treatment, patients believe that they will be devalued and discriminated against. On the other hand, to experience self-stigma, the person must be aware of the stereotypes, agree with them and apply them to him/herself (Corrigan, Watson, & Barr, 2006). Hence, in the strict sense of the word, self-stigma is distinguished from perceived stigma based on awareness.
Previous studies on social stigma suggest that the emotional and behavioral response of the public may vary by mental disorder type. Most studies (Angermeyer, Holzinger, & Matschinger, 2009; Angermeyer & Matschinger, 2005; Corrigan, Lurie, Goldman, Slopen, Medasani, Phelan, 2005; Corrigan et al., 2000; Kim & Seo, 2011; Nordt, Rössler, & Lauber, 2006; Park & Seo, 2012) compared schizophrenia with depression, or compared it with substance abuse problems such as alcoholism and drug addiction. Most studies show that prejudice and discrimination are more severe against persons with alcohol and drug dependence than those with schizophrenia, while those against persons with depression are markedly low. The public perception of persons with alcohol and drug dependence is that they are more dangerous than the schizophrenia group and, therefore, should be more distanced from society. There have been a few studies that addressed problem gambling and behavioral addiction in comparison groups (Feldman & Crandall, 2007; Hing, Russell, Nuske, & Gainsbury, 2015; Horch & Hodgins, 2008). It was found that people’s fear of persons with gambling disorder was lower than that of those with schizophrenia or alcohol dependence but that their anger was higher than that toward people with schizophrenia; their level of anger toward persons with gambling disorder was similar to that toward those with alcohol dependence. However, the social distance was somewhat lower than that for alcoholism or schizophrenia. On the other hand, according to a Korean study (Park, 2018) that compares the social stigma between gambling disorder and alcohol dependence, the latter is seen to be more dangerous than the former, but the former is less recoverable.
Social stigma and self-stigma are two sides of the same coin. If social stigma varies depending on the types of mental disorder, self-stigma is also expected to do so. There are few studies that compare mental disorders in terms of self-stigma. Some researchers (Chang, Wu, Chen, & Lin, 2016; Karidi et al., 2014; Pal, Sharan, & Chadda, 2017; Ran et al., 2018) compare self-stigma among people with schizophrenia, bipolar disorder, depression and anxiety disorder. Based on these results, those with schizophrenia and bipolar disorder perceive self-stigma more than those with depression or anxiety disorder. In other words, the groups suffering from higher social stigma tend to suffer more from self-stigma. In addition, higher self-stigma leads to a lower quality of life. However, Drapalski et al. (2013) found that approximately 35% of people with schizophrenia, bipolar disorder and depression experience moderate or higher self-stigma, but that there are no differences based on the type of mental disorder. They suggest that regardless of the mental disorder type, self-stigma is correlated with low self-esteem and high psychopathology. Cerit, Filizer, Tural and Tufan (2012) analyzed the effects of self-stigma on the social functions of those suffering from bipolar disorder and found that self-stigma plays a core role in predicting social functions and is significantly correlated with social support, severity of symptoms and educational level. In those with schizophrenia, it was found that self-stigma diminishes social functions and increases social exclusion (Karidi et al., 2015).
Despite the fact that most of the previous studies comparing social stigma include alcohol dependence, drug addiction and gambling disorder, comparative studies on self-stigma do not include them. Most people with addiction problems have a more negative public response and higher social distance compared with schizophrenia or depression, and few studies focus on their self-stigma. Hing et al. (2015) surveyed how those with the problem of gambling perceive public response. Based on the results, they perceived that the public regards them as inferior, unintelligent or dishonest. Furthermore, they believed they have more social stigma than persons with schizophrenia or alcohol use disorder. Nevertheless, there are few studies that compare self-stigma among different mental disorders. Hence, this study is based on the premise that those suffering from higher social stigma also suffer more from self-stigma. Therefore, we compare self-stigma among persons with schizophrenia, alcohol use disorder and gambling disorder and analyze the effects of self-stigma on their self-esteem by mental disorder type.
Methods
Participants
This study used convenience sampling because it is practically limited to grasp the population with mental disorder due to the public tendency not to expose their mental disorders. We selected the participants among those who had been diagnosed with mental disorders and were used to the community mental health and welfare center, psychiatric rehabilitation facility, center on gambling problem, community addiction management center, GA (Gamblers Anonymous) or AA (Alcoholics Anonymous). They were required to give consent to take part in this study. All of them were between the ages of 20 and 60, and had passed the acute phase of addiction or withdrawal symptoms. We excluded the people with any damage to the ability to verify reality. In this study, we analyzed the data from 321 participants in total, who consisted of a schizophrenia group of 116, an alcohol use disorder group of 102 and a gambling disorder group of 103. Of them, 269 (83.8%) were male and 52 (16.2%) were female, with a mean age of 40.74 (±10.10). The high proportion of male participants in alcohol use disorder and gambling disorder groups is presumed to be related to the women’s cultural tendency of reluctance to expose their addiction problems. The period of education was 13.15 (±1.79) years. In terms of differences in the socio-demographic variables by mental disorder type (Table 1), the mean age of the alcohol use disorder group was the highest (46.89 ± 7.38 years), followed by the schizophrenia group (41.08 ± 9.11 years) and the gambling disorder group (34.57 ± 9.99 years; F = 46.708, p < .01). The period of education was longest in the gambling disorder group (13.54 ± 1.77 years), followed by the schizophrenia group (13.03 ± 1.58 years) and the alcohol use disorder group (12.88 ± 1.96 years; F = 3.946, p < .05). In terms of gender
Demographic characteristics of respondents.
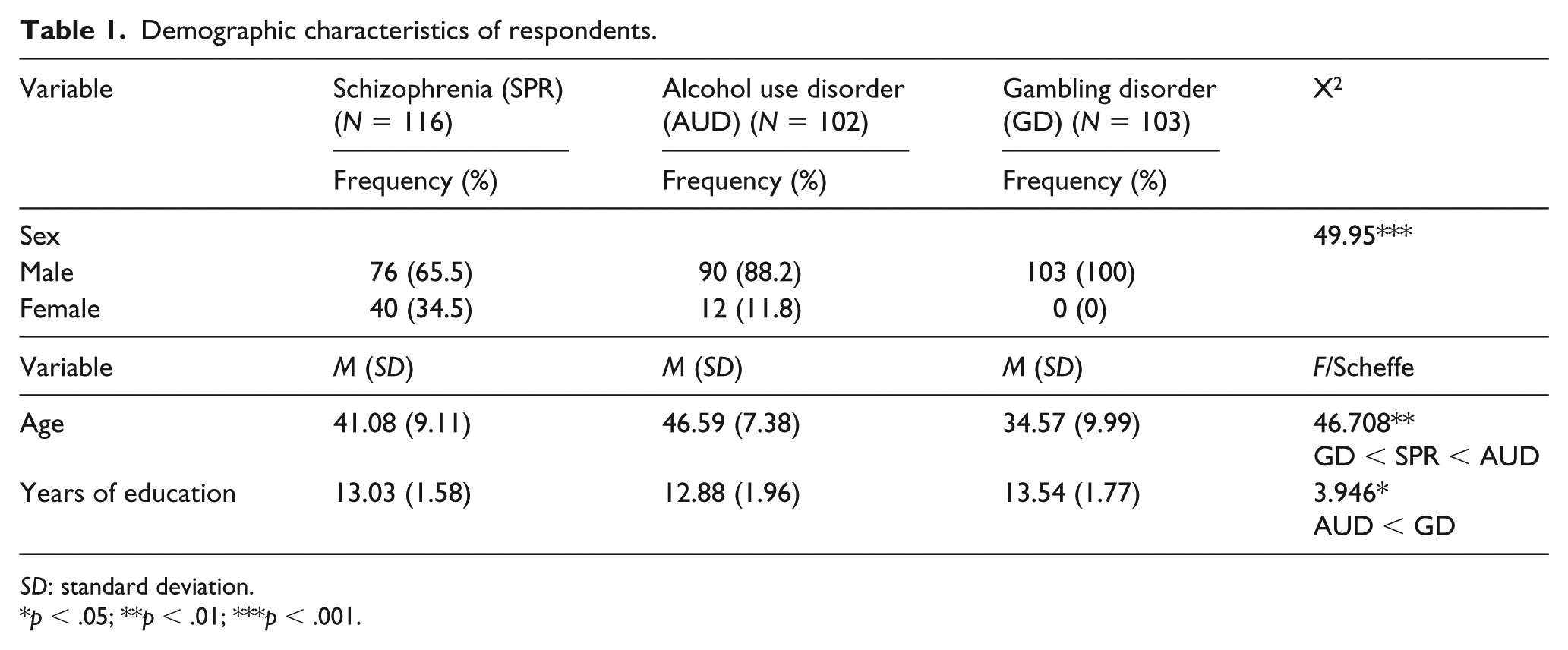
SD: standard deviation.
p < .05; **p < .01; ***p < .001.
The ethical research committee (Institutional Review Board No: GIRB-A18-Y-0028) approved the survey on 1 June 2018. After explaining the purpose of the study to participants, informed consent was obtained from them.
Measures
Self-stigma
To measure self-stigma of the participants, we used the Internalized Stigma of Mental Illness (ISMI) developed by Ritsher, Otilingam, and Grajales (2003) and translated into Korean by a professor in social welfare and two mental health professionals with doctorates. After translating the measure faithfully to the original scale, they revised the translated measure in accordance with Korean expressions, and reviewed the contents of the revised measure thrice. ISMI consists of five subscales: alienation, stereotype endorsement, discrimination experience, social withdrawal and stigma resistance. The alienation subscale (six items) seeks to measure the subjective experience of being less than a full member of society. The stereotype endorsement subscale (seven items) measures the degree to which the respondent agrees with the common stereotype about people with mental disorders. The discrimination experience subscale (five items) intends to capture the respondent’s perception of the way that they currently tend to be treated by others. The social withdrawal subscale (six items) measures avoidance of social situations because of mental disorders. The stigma resistance subscale (five items) portrays the experience of resisting or being unaffected by self-stigma. Stigma resistance items also serve as a validity check because they are reverse-coded (Ritsher et al., 2003). Each item is rated on a 5-point scale, from Completely not true (1) to Completely true (5). Higher scores represent greater self-stigma. Cronbach’s alpha was .74 for alienation, .75 for stereotype endorsement, .83 for discrimination experience, .86 for social withdrawal and .83 for stigma resistance. Cronbach’s alpha for overall self-stigma was .93.
Self-esteem
In order to measure self-esteem, we used the Self-Esteem Scale (10 items) developed by Rosenberg (1979). Respondents indicate how they agree or disagree with the statements, using a Likert scale from strongly disagree (1 point) to strongly agree (5 points). The negatively oriented items were reverse-coded so that higher scores indicate higher self-esteem. Cronbach’s alpha was .88.
Statistical analysis
In order to review the basic assumptions of regression analysis before analyzing, we examined outliers, normality and multi-collinearity. In order to analyze the differences in variables by mental disorder type, we used chi-squared test, one-way analysis of variance (ANOVA) and Scheffe post hoc comparison analysis. To verify the reliability of the scale, Cronbach’s alpha internal consistency reliability was used. In order to analyze the effects of self-stigma on self-esteem, hierarchical regression analysis was performed. We analyzed all the data in this survey using SPSS 21.0.
Results
Comparing self-stigma among persons with different mental disorders
When comparing subscales of self-stigma depending on the types of mental disorder (Table 2), it was found that alienation and stereotype endorsement of the gambling disorder group were higher, followed by the alcohol use disorder group and the schizophrenia group. The differences in social withdrawal and discrimination experienced by mental disorder type were not statistically significant. Stigma resistance was lower in the gambling disorder group than in schizophrenia and alcohol use disorder groups. Accordingly, the gambling disorder group was more affected by self-stigma than schizophrenia and alcohol use disorder groups, and least resistant to it. The overall self-stigma score was higher in the gambling disorder group than in the schizophrenia or alcohol use disorder groups.
Means and standard deviation (SD) for self-stigma by mental disorder type.
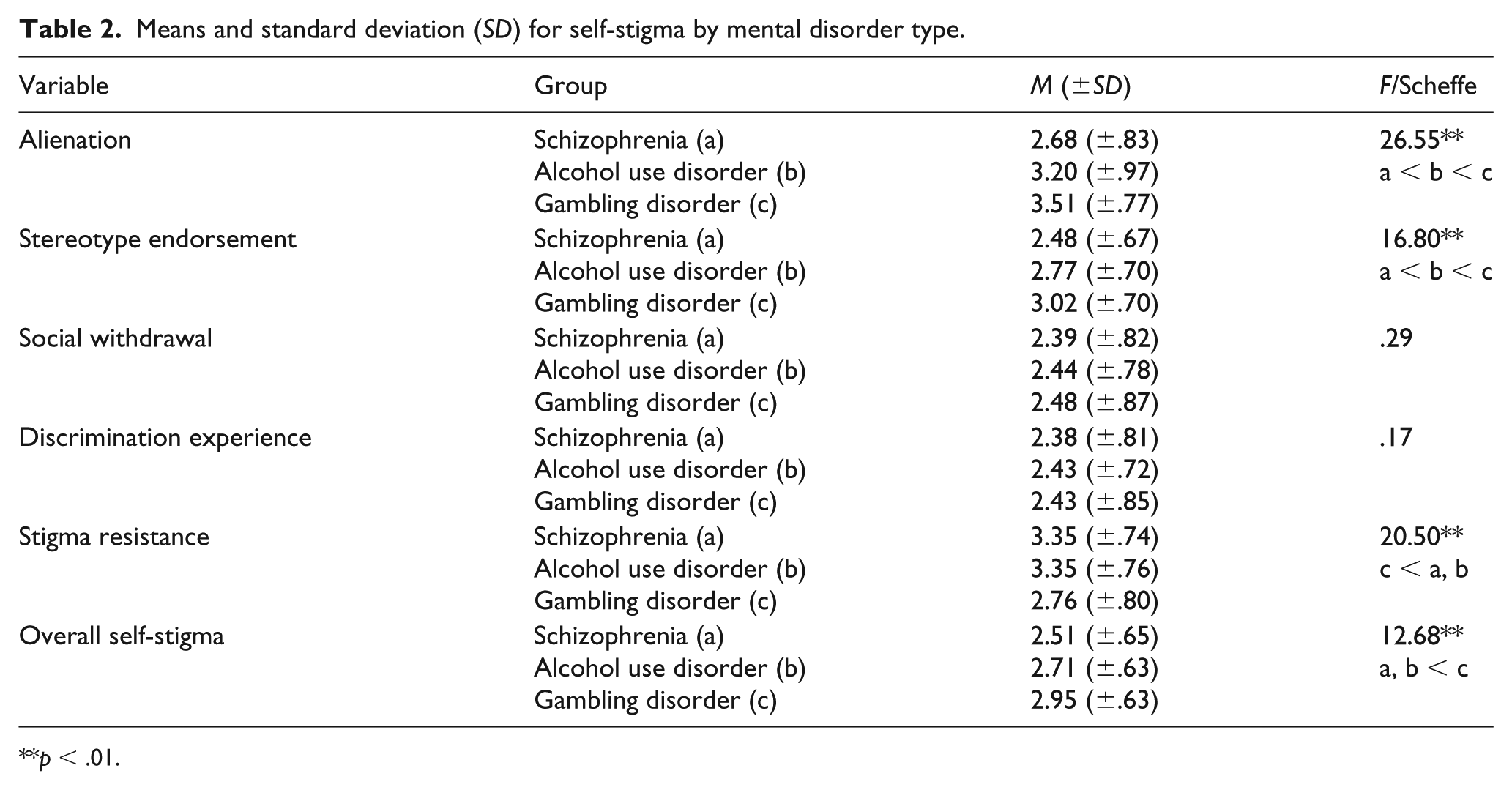
p < .01.
Impact of self-stigma on self-esteem of persons with different mental disorders
With age and years of education controlled, the effects of self-stigma on self-esteem were analyzed using hierarchical regression analysis (Table 3). In all the three groups, subscales of self-stigma had significant relationships to self-esteem.
Effect of self-stigma on self-esteem of persons with different mental disorders.
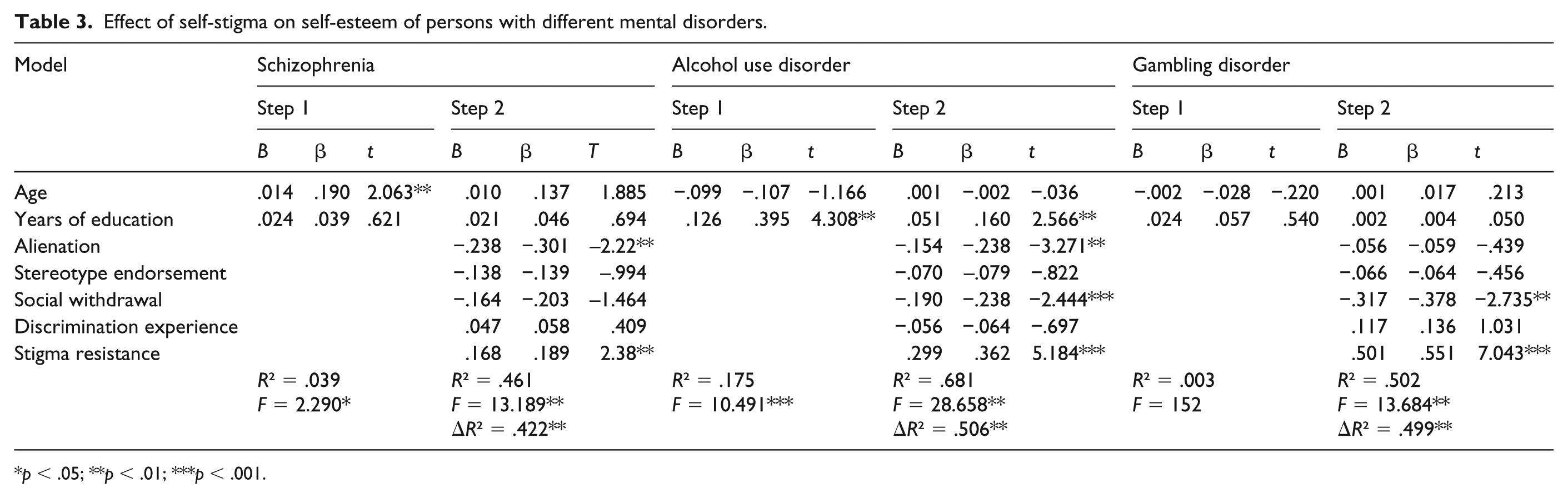
p < .05; **p < .01; ***p < .001.
In the schizophrenia group, age and years of education explained for a 3.9% variance in self-esteem. Age of participants had a significant effect on self-esteem (β = .190, p < .01). At the second step, when the subscales of self-stigma were entered, the explained variance increased to 46.1%. In particular, alienation (β = −.301, p < .01) and stigma resistance (β = .189, p < .01) were significant predictor variables. In the schizophrenia group, the lower the alienation and the higher the stigma resistance, the higher was their self-esteem.
In the alcohol use disorder group, age and years of education explained for a 17.5% variance in self-esteem. Years of education had a significant effect (β = .395, p < .01); the longer the period of education, the higher the self-esteem. At the second step, when the subscales of self-stigma were entered, the explained variance increased to 68.1%. Also, alienation (β = −.238, p < .01), social withdrawal (β = −.238, p < .001) and stigma resistance (β = .362, p < .001) were significant predictors. In the alcohol use disorder group, the lower the alienation, the less the social withdrawal, and the higher the stigma resistance, the higher their self-esteem.
On the other hand, in the gambling disorder group, age and years of education did not significantly predict self-esteem. At the second step, when the subscales of self-stigma were entered, the explained variance for self-esteem was 50.2%, which is statistically significant. Of these, social withdrawal (β = −.317, p < .05) and stigma resistance (β = −.551, p < .001) were the most significant predictors. Therefore, in the gambling disorder group, the less the social withdrawal and the higher the stigma resistance, the higher their self-esteem. In sum, the subscales of self-stigma had negative impacts on self-esteem in all the three groups. Among these subscales, stigma resistance is the most important predictor of self-esteem, regardless of the group. However, stereotype endorsement and discrimination experience were not predictors in any group.
Discussion
As long as public stigma toward mental disorders exists, persons with mental disorders who internalize stigma experience diminished self-esteem. Based on the premise that as social stigma varies by mental disorder type, self-stigma should also differ, this study compares self-stigma among persons with schizophrenia, alcohol use disorder and gambling disorder, and then analyzes the impact of self-stigma subscales on self-esteem. As a result, some important facts were discovered.
First, when comparing the subscales of self-stigma and overall self-stigma by mental disorder type, the gambling disorder group scored the highest in terms of not only overall self-stigma but also some of its subscales – alienation, stereotype endorsement and stigma resistance – followed by the alcohol use disorder and schizophrenia groups. In previous studies comparing social stigma by mental disorder type (Angermeyer, Matschinger, & Corrigan, 2004; Fernando, Deane, & McLeod, 2010; Jorm & Griffiths, 2008; Kim & Seo, 2011; Park & Seo, 2012), alcoholics scored higher than schizophrenics in terms of danger and social distance. Hence, it can be assumed that the alcohol use disorder group score higher than the schizophrenia group in terms of not only social stigma but also self-stigma. For the gambling disorder group, people’s fear and social distance are lower than for the schizophrenia or alcohol use disorder groups (Feldman & Crandall, 2007; Horch & Hodgins, 2008), but their self-stigma is the highest. These results confirm previous findings (Hing et al., 2015) that those with the problem of gambling believe that public stigma toward them is greater than toward persons with schizophrenia or alcohol use disorder. Since self-stigma not only impairs quality of life but is also closely related with lowered treatment compliance (Hajda et al., 2015; Malla, Norman, & Voruganti, 1999; Sirey et al., 2001; Tsang et al., 2010), constant professional endeavor is necessary to reduce their self-stigma. Most studies on social stigma and self-stigma tend to focus on persons with schizophrenia for whom integration into the community is emphasized during the process of their recovery. However, since the social stigma and self-stigma of persons with substance and behavior addiction problems are higher than for schizophrenia, it is necessary to discuss strategies to help them overcome this social stigma and self-stigma.
Second, as a result of analyzing the effects of self-stigma on self-esteem, it was found that self-stigma has negative effects on self-esteem for all mental disorder types. These results confirm those of previous studies (Livingston & Boyd, 2010; Picco et al., 2016; Seo & Kim, 2004) in that self-stigma has a deleterious effect on the lives of people with mental disorder. Self-stigma is an important factor that affects not only self-esteem but also self-efficacy (Corrigan, Larson, Rüsch, 2009; Vauth et al., 2007; Wright, Gronfein, & Owens, 2000) and quality of life (Kao et al., 2016; Seo & Kim, 2004) across all types of mental disorders.
Third, it has been discovered that stigma resistance among the subscales of self-stigma is an important predictor of self-esteem in all the three groups, which means that the higher the stigma resistance, the higher the self-esteem. Since stigma resistance is positively related to self-efficacy, quality of life and recovery (Firmin, Luther, Lysaker, Minor, & Salyers, 2016; Lau et al., 2017), it is essential that persons with mental disorder can resist the social stigma and boost their self-advocacy. Corrigan and Watson (2002) suggested ‘a situational model of personal response to stigma’, and argue that if people with mental disorders perceive that the negative public response is unjust, their self-esteem will remain intact. Therefore, resistance to the stigma may protect their self-esteem and encourage them to feel more empowered (Rüsch, Lieb, Bohus, & Corrigan, 2006).
Fourth, the predictors of self-esteem differ by mental disorder type. In the schizophrenia group, alienation is as much an important predictor of self-esteem as stigma resistance. In the alcohol use disorder group, stigma resistance, alienation and social withdrawal are significant predictors. Also, in the gambling disorder group, both stigma resistance and social withdrawal are important predictors of self-esteem. Accordingly, in the schizophrenia group, their subjective perception that they have yet to be integrated into the community sufficiently negatively affects their self-esteem, but in those with addiction problems (alcohol and gambling disorder), keeping their problem secret and avoiding social relationships affects their self-esteem. Moreover, these responses may worsen the psychopathology, increase the risk of relapse (Link, Cullen, Struening, Shrout, & Dohrenwend, 1989) and cause a high level of anxiety (Vauth et al., 2007).
Based on our findings above, we suggest the following. First, it is necessary to develop a different strategy to mitigate the negative effects of self-stigma for each mental disorder type. In persons with schizophrenia, it is necessary to provide opportunities to participate in community life. Since the mental health policy of Korea still supports forceful and segregation treatment, it is necessary to provide a free environment in which various social activities can be involved. In those with addiction problems, it is essential to encourage them not to avoid social relationships and help them to actively face the stigma toward them. Therefore, they require an intervention to be made aware of their problem, and not to withdraw but pursue diverse opportunities. Second, researchers should suggest ways to overcome the self-stigma, focusing on stigma resistance. Since stigma resistance is a significant predictor of self-esteem in all types of mental disorders, cognitive-behavioral intervention is required to help them to become aware of the unjust social stigma, and how to resist it. In addition, self-advocacy is needed for those with mental disorders to publicize the injustice of social stigma and express their righteous anger (Corrigan, Giffort, Rashid, Leary, & Okeke, 1999). Third, most anti-stigma strategies focus on the public stigma. However, as long as the social stigma prevails, self-stigma remains. Therefore, mental health professionals are obliged to develop strategies to help them overcome the self-stigma.
Social stigma and self-stigma are two sides of the same coin. Nevertheless, most of the studies on self-stigma focus on schizophrenia and depression rather than addiction problems. This study compares the self-stigma of persons with alcohol use disorder and gambling disorder with the schizophrenia group. However, there are several limitations. First, since this study is based on subjects’ self-reports, it did not include clinical evaluations such as social functions and psychiatric symptoms that are presumed to be important predictors of self-esteem. Second, despite there being differences in social stigma by gender (Schnittker, 2000), this study could not cover gender differences of self-stigma because most of the participants with addiction problems were male. Third, this study could not determine the mediating or controlling variables for the relationship between self-stigma and self-esteem.