
Abstract
Loneliness and depression are mental health problems prevailing in United States as well as the world. The primary goal of this study was to identify risk and protective factors associated with loneliness and depression at the individual, interpersonal and community levels among adults living on Mississippi Gulf Coast. Survey data on 310 adults from three coastal counties was analysed. Bivariate analyses and multiple logistic regression analyses were performed to determine correlates and predictors of loneliness and depression. Bivariate analyses showed that loneliness was correlated with marital status, insurance, income, perceived social support and community resilience. Depression was found to be correlated with marital status, insurance, education, income, perceived social support and community resilience. As expected, a significant correlation was found between loneliness and depression. Multiple logistic regression analyses revealed that race, marital status, income, perceived social support and community resilience predicted loneliness, while income and perceived social support served as predictors of depression. Results make it clear that in addition to addressing individual and interpersonal factors, community is important in reducing the incidence of loneliness.
Introduction
With rates doubling since the 1980s, loneliness has been declared an epidemic by the former U.S. Surgeon General Vivek Murthy (CBS This Morning, 2017). In support of this, a 2018 study found that 40% of Americans report experiencing unfulfilling social relationships, and 20% report feeling lonely or socially isolated (Berwick et al., 2018). Feelings of loneliness can negatively impact physical and mental health (Beutel et al., 2017; Luanaigh & Lawlor, 2008; Petitte et al., 2015). Furthermore, associations have been found between loneliness and elevated weight (Petitte et al., 2015), systolic blood pressure (Luanaigh & Lawlor, 2008; Petitte et al., 2015), HbA1C, and an increased risk of lung and heart disease (Petitte et al., 2015). Emotionally, lonely individuals are more likely to experience stress and symptoms of mental health issues like depression (Mushtaq et al., 2014; Richardson et al., 2017). These physical and mental health factors and the correlated feelings of loneliness can increase risk of mortality (Hawkley & Cacioppo, 2010; Holt-Lunstad et al., 2015).
Similarly, depression is also a common mental health condition. It is estimated that worldwide more than 250 million people suffer from the disorder (James et al., 2018). U.S. estimates place lifetime prevalence rates at approximately 20% of the population (Hasin et al., 2018). In 2017, close to 11% of Mississippi youth (ages 12–17) suffered at least one major depressive episode in a 12-month period (Mental Health America, 2020). This is concerning, as studies have found that mood issues in adolescents can predict depression in adults (Pine et al., 1999, 2002; Weissman et al., 1999). Among those with depression, 80% had some level of functional impairment, and 27% had serious difficulties in their daily life (Pratt & Brody, 2008). According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), depression leads an individual to experience a range of symptoms that include changes in eating and weight, sleep, movement and speech (as noticed by others), fatigue, difficulty concentrating and feelings of worthlessness or inappropriate guilt. Individuals may also think frequently about death or suicide. In addition, the sufferers will exhibit a decreased level of functioning, resulting in significant distress and impairment in social, occupational, or other functional domains (American Psychiatric Association, 2013). Although an increasing body of research has examined factors associated with loneliness and depression, most studies have focused on sociodemographic (e.g. age, gender, education, income, household type) and interpersonal factors (e.g. social network, social support) (Deckx et al., 2014; Ge et al., 2017; Lee & Goldstein, 2016; Yang, 2018). Limited attention has been paid to community factors in which individuals’ lives and interpersonal relations are embedded. In addition, the majority of studies investigating loneliness have focused on older populations, even though loneliness is prevalent across all age groups (Kearns et al., 2015; Lasgaard et al., 2016; Lee et al., 2019; Polack, 2018). The purpose of the current study is twofold: (1) to investigate determinants of loneliness and depression at the individual level (i.e. sociodemographic factors), the interpersonal level (i.e. perceived social support) and the community level (i.e. community resilience) factors among adults (age 18 or higher) living on the Mississippi Gulf Coast and (2) to examine the association between loneliness and depression.
Predictors of loneliness and depression
Loneliness can be defined as an emotional state that results from the distress felt by an individual when the need for social relationships is not realised (Hawkley & Cacioppo, 2010; Perlman & Peplau, 1981 as cited in Dahlberg & McKee, 2014; Pinquart & Sörensen, 2003, as cited in Luo et al., 2012). The lack of desired social relationships most often stems from isolation; as such, these two concepts are often measured together. However, the distinction must be made between perceived and physical isolation. Loneliness is associated with perceived social isolation. Meaning that individuals can live alone and not experience loneliness while one can be surrounded by others and experience loneliness (Hawkley & Cacioppo, 2010).
While a number of studies have focused on which sociodemographic factors increase risk of loneliness and depression, their results are mixed. Especially, considerable variations exist across studies that examined the relationship between age and loneliness. Findings varied from positive relationships (i.e. increase of loneliness with age; Yang & Victor, 2011), inverse relationships (i.e. decrease of loneliness with age; Beutel et al., 2017), or curves (Lee et al., 2019). Similar results were found between age and depression: positive relationships (Stordal et al., 2001), inverse relationships (Kessler et al., 2010), or curves (Tampubolon & Maharani, 2017). These mixed results may result from variations in the age group of the study population, moderators (e.g. gender, income, education) and research methods. With regard to gender, Beutel et al. (2017) and Savikko et al. (2005) found loneliness to be more prevalent in women, while a recent meta-analysis indicated that similar levels of loneliness were detected between males and females across the life span (Maes et al., 2019). Lower education was found to be associated with greater loneliness (Savikko et al., 2005) and depression (Blackmon et al., 2017; Ten Kate et al., 2017) and poor income was found to be associated with increased loneliness (Savikko et al., 2005) and depression (Ten Kate et al., 2017). Not having a spouse/cohabiting partner or never being married was associated with greater loneliness (Von Soest et al., 2020) and depression (Walker & Druss, 2015).
At the level of interpersonal relationships, the current study focuses on perceived social support. Considerable research has been dedicated to the effects of social support on physical and mental health (Chen et al., 2019; Gariépy et al., 2016; Prati & Pietrantoni, 2010; Williams & Galliher, 2006). However, results varied based on how the studies conceptualised and operationally defined social support. Measurements varied from the objective (e.g. size of social network or received support) subjective (perceived support or satisfaction of support received); functional (e.g. tangible material aid, information and emotional support) or structural (e.g. size of network, frequency of contact) (Cohen & Wills, 1985; Fong et al., 2017; Prati & Pietrantoni, 2010; Vandervoort, 1999). In the current study, social support is conceptualised and operationally defined in subjective (i.e. perception) and functional terms. A number of studies have reported that perceived social support plays a protective role against loneliness (Tan et al., 2016; Yildirim & Kocabiyik, 2010) and depression (Grav et al, 2012; Hatfield et al., 2013; He et al., 2016; Kingston, 2013).
Whereas a wealth of studies have examined predictors of loneliness and depression at the personal and/or interpersonal levels, very limited attention has been paid to community level factors. Studies that emphasise the role of community in mental health and psychological well-being of community members have mainly focused on community support that is conceptualised variously as belongingness and connections to a community, participation in community, and availability and use of resources embedded in a community (Herrero & Gracia, 2007; Ng et al., 2014; Nwoke et al., 2016). The current study however sought to investigate the influence of community resilience on loneliness and depression. Although connection, caring and resources are key domains of community resilience, community resilience encompasses other dimensions of collective ability of a community that are essential in managing and responding to ongoing community issues and disasters. The concept of community resilience has been discussed in disaster-related studies as preparedness for, response to and recovery from a disaster often require collective efforts of multiple systems at the community level (Abramson et al., 2015; Lee et al., 2018; Pfefferbaum et al., 2013, 2015). Pfefferbaum et al. (2013) mentioned:
Community resilience is not simply a collection of personally resilient community members who respond individually to adverse events. Community resilience entails the ability of community members to take deliberate, purposeful, and collective action to alleviate the detrimental effects of adverse events. (p. 251)
Pfefferbaum et al. (2015) identified the following domains as key indicators of community resilience: ‘connection and caring, resources, transformative potential, disaster management, information/community’ (p. 190).
Despite the recognition that community resilience is important, not until recent years have instruments for measuring this construct been available (Pfefferbaum et al., 2015); therefore, there are very limited empirical studies available. Lee et al. (2018) found that higher levels of community resilience was associated with greater psychological resilience, which in turn related to lower levels of depressive symptoms among disaster survivors. There are studies that focus on community-level factors but they do not measure the concept of community resilience directly. For example, Wu et al. (2018) reported that greater neighbourhood-related stress (e.g. transportation, housing situation) was associated with greater depressive symptoms among breast cancer survivors. Fullerton et al. (2015) found that higher collective efficacy was associated with lower levels of depressive symptoms among survivors of a disaster. Lyons and Heywood (2016) reported that collective resilience was strongly linked to mental health among HIV-positive gay men.
Methods
Sampling procedures
Data used in this analysis was collected in the fall of 2018 as a part of the Gulf Region Health Outreach Program and the University of Southern Mississippi’s School of Social Work efforts to determine the impact of human-made and natural disasters on coastal residents. Graduate and undergraduate students administered the study survey in three counties along the coast of Mississippi (Hancock, Harrison and Jackson Counties). Using public domain parcel maps, ArcGIS 10.2 software was used to randomly select households to be included in the survey. To ensure only occupied residential areas were included, parcels that contained non-residential buildings (businesses, schools, medical facilities, churches and industrial complexes) were eliminated. Additionally, any parcel with more than 2 acres or less than 0.1 acres were not included. Working in teams of two or more, surveyors were assigned a geographic area to survey. Each team was then given an aerial map laid out in a grid pattern with selected households highlighted. All student surveyors were required to attend training to ensure proper survey administration and competence using the survey maps.
Since the survey was initially designed to identify the impacts of Hurricane Katrina and the Deepwater Horizon Oil Spill, most of the sample resided between Interstate 10 and the Gulf of Mexico. The three counties surveyed had an estimated population of 397,261 in 2018 (United States Census Bureau, 2019). The survey included demographic questions and validated scales (e.g. Multidimensional Scale of Perceived Social Support, Communities Advancing Resilience Toolkit, UCLA Loneliness scale, Centre for Epidemiologic Studies-Depression scale) that measured perceived social support, community resilience, loneliness and depression. The project was reviewed and approved by the Institutional Review Board at the University affiliated with the researchers and student surveyors.
Measures
Perceived social support
Perceived social support was measured by the Multidimensional Scale of Perceived Social Support (MSPSS), a 12-item self-reported measure that assesses an individual’s perceptions of social support adequacy from different sources (i.e. family, friends, significant other) (Zimet et al., 1988). Responses were coded on a 7-point Likert scale, ranging from one (very strongly disagree) to seven (very strongly agree). A sum score was computed from the 12 items, yielding a possible total score between 12 and 84, with higher scores indicating higher levels of perceived social support. Evidence of reliability and validity for the MSPSS has been reported in many previous studies (Dahlem et al., 1991; Wittenborn et al., 2020; Zimet et al., 1988). In this study, the Cronbach’s alpha for the MSPSS was 0.94.
Community resilience
Community resilience was measured by using the Communities Advancing Resilience Toolkit (CART). This 24-item self-reported measure assesses perceived community resilience related to the dimensions of connection and caring, resources, transformative potential, disaster management and information and communication (Pfefferbaum et al., 2015). Examples of items: ‘People in my community help each other’; ‘My community has resources it needs to take care of community problems (resources include, for example, money, information, technology, tools, raw materials and services)’; ‘People in my community communicate with leaders who can help improve the community’ (Pfefferbaum et al., 2015, p. 189). Responses were coded on a 5-point Likert scale, ranging from one (strongly disagree) to five (strongly agree). A sum score was computed from the 24 items, yielding a possible total score between 24 and 120, with higher scores indicating higher levels of perceived community resilience. Evidence of reliability for the CART was reported (Pfefferbaum et al., 2015). In this study, the Cronbach’s alpha for the Community Resilience was 0.96.
Loneliness
The brief version of the three-item UCLA Loneliness scale was used to measure subjective feelings of loneliness and social isolation (Hughes et al., 2004). Participants rated each statement on a 3-point Likert scale ranging from 1 (hardly ever) to 3 (often). Items were then summed to form a total score ranging from 3 to 9, with higher scores indicating greater loneliness. The scale has evidence of adequate internal consistency and validity (Hughes et al., 2004). Cronbach’s alpha calculated in the current study was 0.82. Based on previous studies (Domènech-Abella et al., 2017; Steptoe et al., 2013), the cutoff score of ⩾6 was used to indicate loneliness in this study.
Depression
This study used The Centre for Epidemiologic Studies-Depression scale (CES-D; Radloff, 1977) to measure levels of depression in study participants. The 20-item scale has adequate internal consistency and validity (Conerly et al., 2002; Radloff, 1977) and is widely used as a self-report measure of depression in community-based epidemiological studies. The CES-D asks participants to rate how often they experience each symptom over the previous week using a 4-point scale ranging from 0 (rarely or none of the time) to 3 (most or all of the time). Four of the 20 items are reverse scored, with higher scores indicating greater depressive symptoms. Scores are summed across all items to create a total score that ranges from 0 to 60. Cronbach’s alpha calculated in the current study was 0.87. The total scores that are 16 or greater represent the likely presence of high depressive symptoms (Radloff, 1977).
Results
Sample characteristics
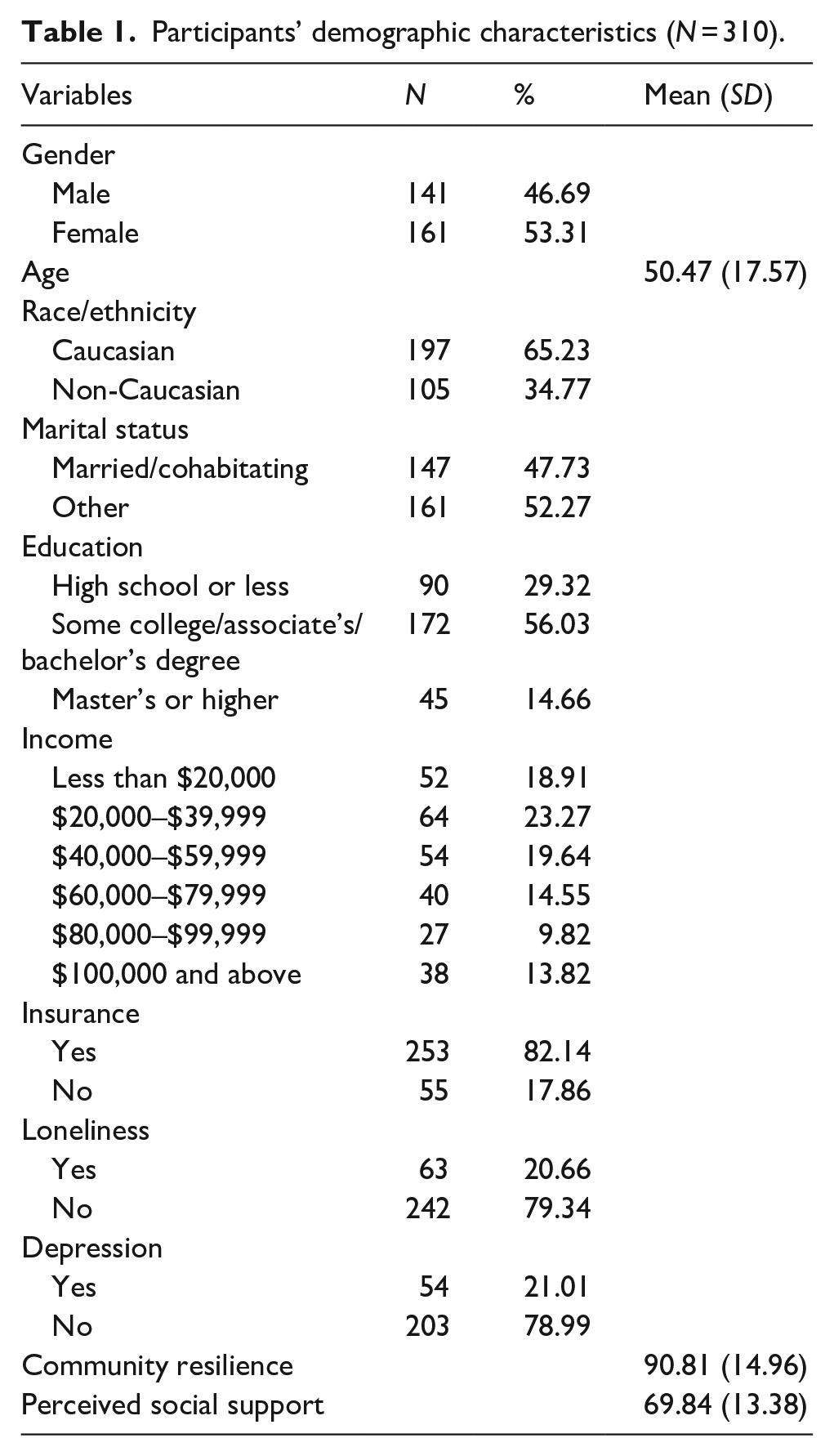
A total of 310 participated in the survey. 65.23% were Caucasian, and 53.31% of the participants were female. The average age of the participants was 50.47 years (SD = 17.57). Among the cohort, almost 30% of them had completed high school or less, 56.03% had some college/associate’s/bachelor’s degree while only 14.66% had master’s degree or higher. Around half of the participants were married or cohabitating with partners (47.73%). Regarding household income, 18.91% reported less than $20,000, 23.27% reported $20,000 to $39,999, 19.64% reported $40,000–59,999 and 38.18% reported $60,000 or higher. The majority of the participants had health insurance (82.14%). Among the participants, 20.66% and 21.01% were found to be living with loneliness and depression respectively. The average total score for community resilience was 90.81 (SD = 14.96) while the average total score for perceived social support was 69.84 (SD = 13.38). Table 1 presents descriptive statistics of sample characteristics.
Participants’ demographic characteristics (N = 310).
Bivariate analyses
The first set of bivariate analyses was performed to determine the relationship between loneliness and the independent variables. The results showed that there was a statistically significant relationship between loneliness and the independent variables – marital status (χ2 = 28.83, p < .001), insurance (χ2 = 15.88, p < .001), income (MH χ2 = 28.53, p < .001), community resilience (t = 4.91, p < .001) and perceived social support (t = 5.43, p < .001).
Another set of bivariate analyses were executed between depression and the independent variables of interest. Results revealed that depression was significantly related to the following variables – marital status (χ2 = 16.51, p < .001), insurance (χ2 = 4.41, p = .036), education (MH χ2 = 12.43, p < .001), income (MH χ2 = 25.62, p < .001), community resilience (t = 2.62, p = .009) and perceived social support (t = 4.37, p < .001).
Lastly, a bivariate analysis was performed to know if there is a significant relationship between loneliness and depression. At a significance level of .05, a statistically significant relationship was found between loneliness and depression (χ2 = 62.10, p < .001). The bivariate analyses results are shown in Table 2.
Bivariate analyses between loneliness, depression and independent variables.
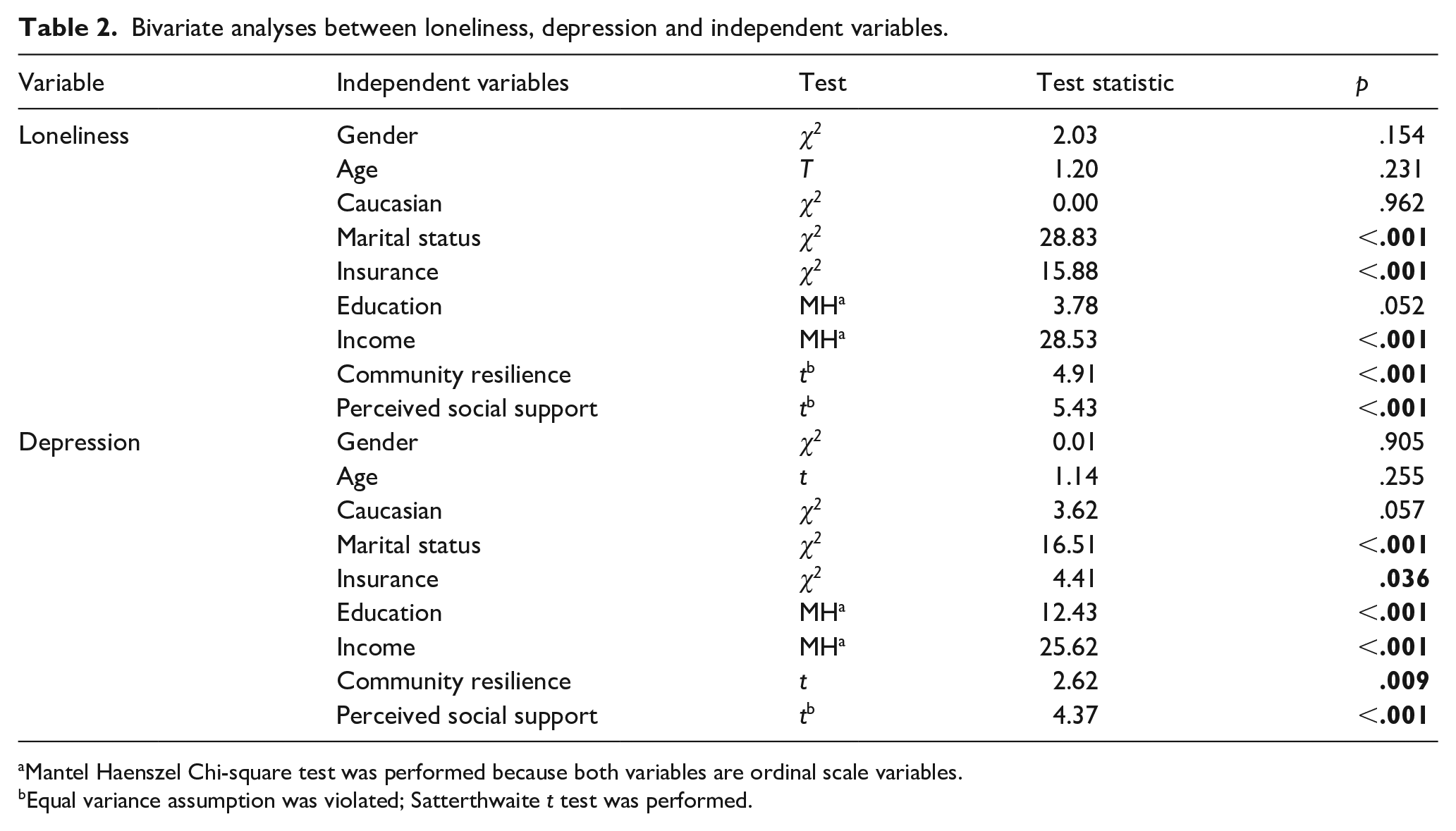
Mantel Haenszel Chi-square test was performed because both variables are ordinal scale variables.
Equal variance assumption was violated; Satterthwaite t test was performed.
Multivariate analyses
The first set of analysis included a multiple logistic regression analysis to predict the relationship between loneliness and the independent variables. The global model likelihood ratio test indicated that the overall model was statistically significant (χ2 = 84.27, df = 9, p < .001). The Hosmer and Lemeshow goodness-of-fit test results showed that this model has a good fit for prediction (χ2 = 3.24, df = 8, p = .918). Caucasian, marital status, income, community resilience and perceived social support were statistically significant at α = 0.05. If a participant is Caucasian, he or she will have about 4.7 times more likely to be lonely (OR = 4.70, 95% CI: 1.68–13.13, p = .003). Marital status has a negative relationship with loneliness. If a person is married/cohabitating, they are around 84% less likely to be lonely compared to unmarried or single persons (OR = 0.16, 95% CI: 0.05–0.48, p = .001). Income has a negative relationship with loneliness. If a participant belongs to a higher earning category, the odds of being lonely decreases by around 35% (OR = 0.65, 95% CI: 0.44–0.96, p = .032). Community resilience and social support also have a negative relationship with loneliness. As community resilience scores and perceived social support scores increase, the odds of being lonely decreased 4% (OR = 0.96, 95% CI: 0.93–1.00, p = .027) and by 5% (OR = 0.95, 95% CI: 0.92–0.98, p = .005), respectively.
The next set of analysis included a multiple logistic regression analysis to predict the relationship between depression and the independent variables. The global model likelihood ratio test indicated that the overall model was statistically significant (χ2 = 48.62, df = 9, p < .001). The Hosmer and Lemeshow goodness-of-fit test results showed that this model has a good fit for prediction (χ2 = 7.11, df = 8, p = .525). Only income level and perceived social support are statistically significant at α = 0.05. Both independent variables had negative relationships with depression. As income level increases, the odds of being depressed decreases by 40% (OR = 0.60, 95% CI: 0.41–0.88, p = .008). As perceived social support score increases, the odds of being lonely decreased by around 5% (OR = 0.95, 95% CI: 0.91–0.98, p = .003). Table 3 presents the results of the multiple logistic regression analyses.
Multivariate logistic regression model.
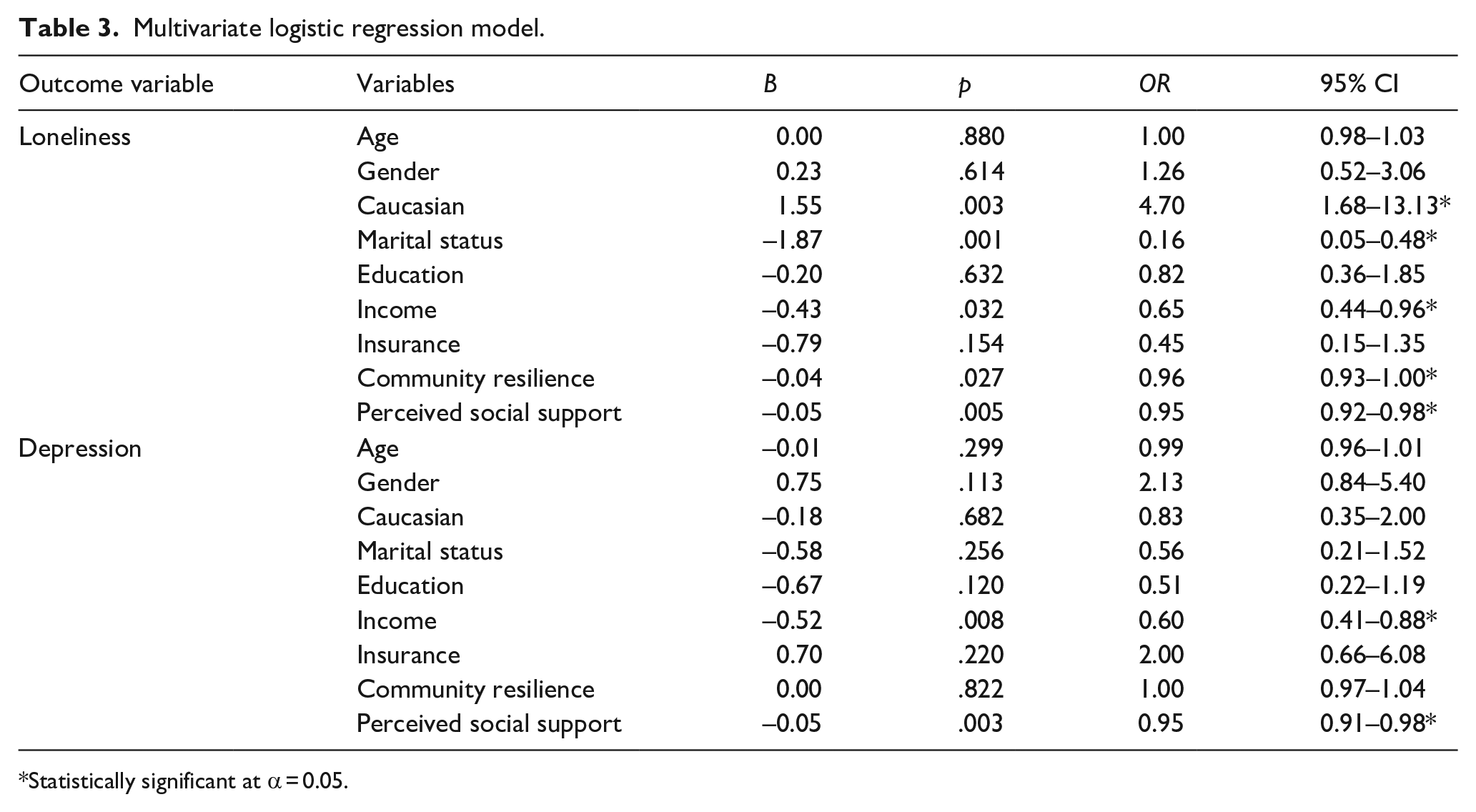
Statistically significant at α = 0.05.
Discussion
The primary goal of this study was to determine which correlations and predictors existed between loneliness and depression at the individual, interpersonal and community levels among adults living on the Mississippi Gulf Coast. Secondly, the authors sought to determine the association between loneliness and depression in the sample. As with previous studies, our results indicated a correlation between loneliness and depression (Mushtaq et al., 2014; Richardson et al., 2017).
Individual factors
Both bivariate correlations and multiple logistic regression analyses revealed significant relationships between loneliness and marital status and loneliness and income. These relationships were in the expected direction where greater income and being married/cohabitating was related to a decrease in loneliness. Having health insurance has negative direction with loneliness and depression as expected. The insured group showed less loneliness (16.5%) than uninsured group (40.7%). In addition, the insured group has lower depression rate (18.2%) than the uninsured group has (31.9%). At the multivariate analyses, however, insurance was not a significant predictor of loneliness or depression. Depression was also correlated with marital status, income and education. In addition, as expected, regression analysis revealed that individuals with lower income were more likely to experience depression.
While further research is necessary to understand the relationship between race and loneliness, our findings suggest that Caucasians are more likely to experience loneliness. This is in contrast to a recent survey that found no racial differences in rates of loneliness among adults (Cigna, 2018b). A 2015 study of older adults did find that African Americans are more likely to experience feelings of social isolation (Miyawaki, 2015). While social isolation is considered an objective measure of contact and loneliness is most often defined as a subjective feeling, the constructs often co-occur. However, even when combining these constructs, there are limited studies that explicitly investigate racial differences.
Interpersonal factors
The study explored the relationship between perceived social support and the outcome variables. Social support was found to be strongly correlated (p < .001) with both loneliness and depression. Regression analysis revealed that higher levels of social support decreased the odds of developing both loneliness and depression. These findings are consistent with prior research indicating that improvements in social support reduce loneliness (Eskimez et al., 2019; Kwag et al., 2011). The same is true for depression. Investigations into the connection between social support and depression have found deficits in social supports increase the risk for depression in adults (Gariépy et al., 2016; Kim & Shin, 2004) and adolescents (Dingfelder et al., 2010; Gariépy et al., 2016; Stice et al., 2004).
Community factors
With the limited research available on the impact of community on loneliness and depression, the authors sought to determine if community resilience, as measured by the CART, was related to loneliness or depression. Of particular interest was the finding that although we found statistical relationships between community resilience and loneliness as well as depression, community resilience served as a predictor for only loneliness not depression. One explanation for the connection between community resilience and loneliness may be found in a 2001 study investigating the impacts of how an individual’s sense of community affects well-being (Prezza, 2001). The study found that having a sense of community reduced feelings of loneliness. While a sense of community is a different concept than community resilience, a strong sense of community may influence the individual’s emotional state. In this case, a resilient community would have a more positive impact on the individual. However, further study investigating how the concepts of community resilience and community connection is warranted to determine if the two are truly connected.
Implications for practice and policy
Although understanding the relationship between community resilience, loneliness and depression warrants further investigation, there are practical implications that follow from the present study. Mainly, interventions designed to reduce loneliness or depression should not be limited to addressing individual factors. While the precise reasons for the interactions are not currently understood, Bronfenbrenner’s Ecological Systems Theory would argue that the individual cannot escape the influence of their environment (Coady & Lehmann, 2016). Therefore, interventions to reduce loneliness and depression should include components that are designed to promote positive interactions between individuals and resilient communities. Furthermore, individual service providers should assess the communities they serve to determine their level of resilience, even if the community has not experienced a known disruption (i.e. disasters or trauma). Community-level interventions should be implemented in communities who demonstrate lower levels of resilience. In addition, lawmakers and funding agencies should support evidence-based practices to promote community resilience as a way to improve the overall health of the community.
Limitations
This study presents an argument for the role of individual, interpersonal and community factors in loneliness and depression. However, caution should be exercised when interpreting the results. The use of cross-sectional data prevents the inference of causality. Also, the sample was comprised of individuals residing on the Mississippi Gulf Coast. At the time of data collection, the area had experienced both Hurricane Katrina in 2005 and the Deepwater Horizon Oil spill in 2010. Efforts to support the communities and their residents as a result of these events were not measured, limiting the findings.
Conclusion
This study examined factors associated with loneliness and depression among Mississippi Gulf Coast residents. Findings related to individual and interpersonal correlates were similar to those in other studies. Differing from other currently available studies, this investigation added the concept of community resilience. Community resilience has been understudied in literature not relating to disasters. Results make it clear that the community is important in reducing the incidence of loneliness. As such, future research should investigate the role of community resilience in the psychological outcomes of individuals.