
Abstract
Background:
Since December 2019, over 4,600 deaths and 84,000 confirmed cases were reported in China because of the coronavirus disease 2019 (COVID-19) pandemic. However, there is a dearth of studies on the psychological resilience in residents.
Aims:
This study aims to measure the psychological resilience of Chinese residents to reflect their psychological status as well as influencing factors during the pandemic.
Method:
We conducted a combination of stratified sampling and snowball sampling to select survey subjects. We employed the psychological resilience and influencing factor questionnaire based on the 10-item Connor and Davidson Resilience Scale (CD-RISC10) for survey. We collected data from 3,398 residents in China between 31 January and 29 February 2020. Multivariable linear stepwise regression analysis was used to determine factors associated with psychological resilience in residents.
Results:
The mean score of psychological resilience among Chinese residents was 27.11 ± 8.45 (SD = 7.98). There were some factors significantly associated with psychological status among the Chinese residents during the COVID-19 outbreak. Residents with lower financial status, living in rural areas, unmarried, lacking fixed employment or retirement guarantees, and lacking knowledge of policies were more likely to report a lower level of psychological resilience.
Conclusion:
Health service policy makers in many countries should adopt relevant measures to improve the psychological resilience of residents during the pandemic. This includes short-term aggressive treatment, strengthening health education, and improving the awareness of residents with respect to emergency health policies. In addition, the financial status, health levels, and risk management capabilities of residents should be increased over the long term.
Background
Since December 2019, around 57 millions coronavirus disease 2019 (COVID-19) cases have been confirmed around the world (Bulut & Kato, 2020; Kannan et al., 2020; Sifuentes-Rodríguez & Palacios-Reyes, 2020). Owing to the continuous increase in the number of suspected and confirmed patients, China has adopted a series of effective measures, such as lockdown, work stoppage and school closure, information dissemination, and other strategies to stem the spread of the virus (Wang & Wang, 2020). However, the actions of the government, particularly a scale of quarantine at the national level, have unknowingly increased panic and anxiety in the public and affected people’s psychological health. Currently, the pandemic-related studies focused on epidemiological surveys and infection protection measures while there is a lack of attention on psychological health problems in the general public (Li et al., 2020; Xiang et al., 2020).
Psychological resilience is defined by the American Psychological Association as ‘the process of adapting well in the face of adversity, trauma, tragedy, threats or significant sources of stress’ (Gong et al., 2020). Corresponding changes in psychological resilience in the public may occur with changes in lifestyle, educational level, and other social-demographic characteristics. Early studies on psychological resilience have proposed different resilience models. In 2003, Connor and Davidson developed the Connor and Davidson Resilience Scale (CD-RISC), which is widely used in many countries (Connor & Davidson, 2003). The psychological resilience scale includes 25 self-reported questions and covers five factors: personal competence; high standards and tenacity; trust in one’s instincts, tolerance of negative effect, and strengthening effects of stress; positive acceptance of change and secure relationships; control; and spiritual influences (Jung et al., 2012; Yu et al., 2011). Campbell-Sills and Stein conducted a further analysis of the CD-RISC psychological resilience scale and extracted 10 items to form the simplified Chinese version of the 10-item Connor and Davidson Resilience Scale (CD-RISC10), which is widely used (Ye et al., 2017).
Recently, some studies have explored the psychology of residents during COVID-19 (Li et al., 2020; Lima et al., 2020; Wang et al., 2020). These researches focuses on the psychological condition of residents, such as anxiety and depression, which has strong uniqueness, and was based on a scale and the results were more scientific (Sisto et al., 2019). However, no studies have investigated the psychological resilience among the Chinese adults. This study aims to explore the current status of psychological resilience among the Chinese adults during the COVID-19 pandemic and further examine the influencing factors in order to provide a reference for ameliorating psychological distress in the public during a pandemic, and formulate targeted intervention measures (Gong et al., 2020).
Methods
Study population
We conducted a cross-sectional survey in China from 31 January to 29 February 2020. A combination of stratified sampling and snowball sampling was used to select survey participants. We stratify the respondents mainly according to the eastern, central and western region of China. We selected residents from eastern (Beijing, Tianjin, Hebei, Liaoning, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong, Guangdong, and Hainan), central (Shanxi, Jilin, Heilongjiang, Anhui, Jiangxi, Henan, Hubei, and Hunan) and western (Chongqing, Sichuan, Guizhou, Yunnan, Tibet, Shaanxi, Gansu, Qinghai, Ningxia, Xinjiang, Inner Mongolia, and Guangxi) China to complete the psychological resilience survey. We adopted snowball sampling strategy to recruit participators; potential participators were electronically invited via WeChat. A total of 3,495 residents received the questionnaire, of which 38 participants did not respond and 59 questionnaires were not filled. The response rate was 97.22% and 3398 complete questionnaires were employed for results analysis.
This study protocol was approved by the institutional review board of Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China (IORG No: IORG0003571). All methods were performed in accordance with the relevant guidelines and regulations. Each participant in the study was informed and consented to the study.
Survey tools
The questionnaire consists of three parts: social-demographic information (such as gender, region, age, education level, and marital status), personal awareness and risk behaviors during the COVID-19 pandemic, and the psychological resilience scale.
The CD-RISC10 scale was used to measure the psychological resilience of residents. This scale consists of 10 items and the 5-point Likert scale was applied with 0 (never or not possible) to 4 (always or extremely possible). The total score of the psychological resilience scale is the sum of the scores of various items and ranges from 0 to 40 points (Cosco et al., 2016; Kwan et al., 2019). Higher the score, higher is the psychological resilience. The Cronbach α test was made use of to measure the internal consistency of the 10 items. The Cronbach α of the scale was 0.96, showing that the scale has robust consistency. The KMO was 0.96, thereby indicating that the scale has strong validity.
Data collection and quality control
The design of the questionnaire was based on literature review, small group discussion, and simulated interviews. In addition, we conducted a pilot study in Wuhan to improve the quality of the questions. Following that, we leveraged WeChat (China’s largest messaging platform with nearly 1 billion users, similar to WhatsApp in Western countries) to send the hyperlink of the online questionnaire that was designed using ‘Survey Star (wjx.cn)’ to participants. The researcher entered the data into the Internet database to ensure accuracy.
Data analysis
Descriptive analysis included the mean and standard deviation of continuous variables and the quantity and percentage of categorical data. The t-test and ANOVA were used to compare differential factors (understanding of COVID-19 symptoms and protective measures, and support for quarantine measures) for psychological resilience between different genders and regions according to demographic statistics (gender, age, marital status, and region) and socioeconomic status (education level and income) (Colosio et al., 2018; Guo & Zheng, 2019). No clustering was observed in the respondents (correlation = 0.03, p < .001). Therefore, the multivariable linear stepwise regression analysis model was used to estimate factors associated with psychological resilience in residents (inclusion and exclusion criteria were: p = .05 and p = .01). We used a variance inflation factor to assess multicollinearity. All analyses were carried out using STATA 12.0, and all differences were tested using two-tailed tests and a p-value of 0.05 was considered statistically significant.
Results
Table 1 reports the social-demographic characteristics of 3,398 respondents. The mean age was 27.64 years (SD = 7.73) and majority of respondents were female (66.51%). Among the respondents, 585 (17.22), 2716 (69.04%), and 637 (18.75%) were from eastern, central, and western China, respectively. Most of respondents (95.59%) were Han Chinese, unmarried (68.86%). Around 62% of respondents were students, soldiers, or freelancers. More than half the respondents (58.15%) lived in urban areas and further, more than half the respondents (53.74%) had a mean monthly family income at a low level. Most respondents (86.23%) had a good health status and (86.55%) medical insurance.
Statistical description of study samples.
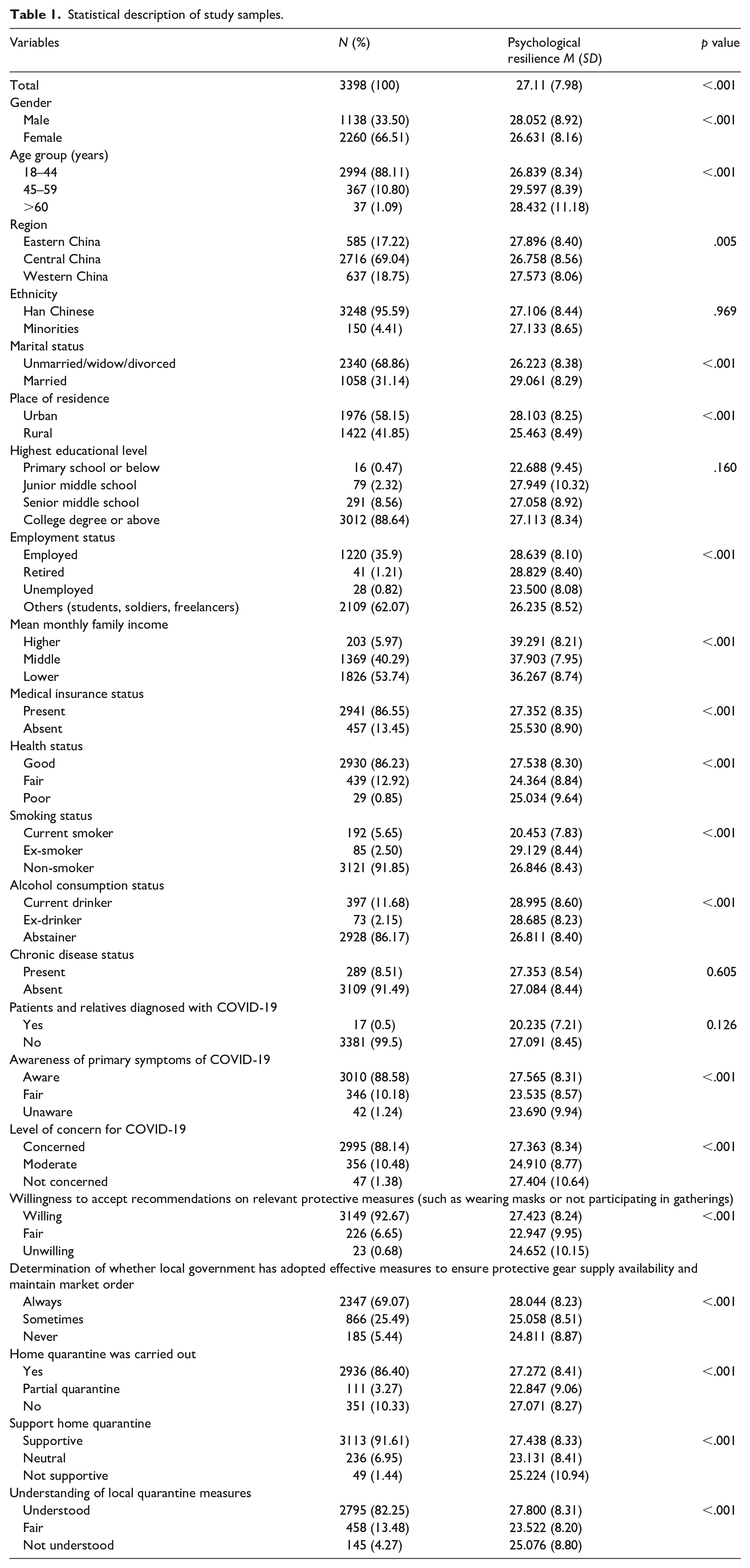
The mean psychological resilience score of respondents was 27.11 ± 8.45 (SD = 7.98), showing that Chinese residents had low psychological resilience. Table 1 shows the mean psychological resilience scores of different subpopulations. There were significant differences in psychological resilience between residents with different age groups, gender, education levels, regions, marital statuses, income levels, and health statuses. The differences in psychological resilience between residents of different regions, ethnicities, employment statuses, and medical insurance statuses were not significant.
Table 2 lists the multivariable linear stepwise regression analysis results of psychological resilience factors in respondents. Males, being married, lived in urban areas, resided where the local government had adopted effective measures to ensure protective gear supply and maintain market order, did not carry out home quarantine, supporting home quarantine, and understanding the control measures had high psychological resilience. In addition, respondents with fixed employment or were retired, in robust physical condition, being smoker or ex-smoker, aware of primary symptoms of COVID-19, and willing to accept relevant protective measures had higher psychological resilience.
Stepwise regression analysis of associated factors for psychological resilience among respondents.
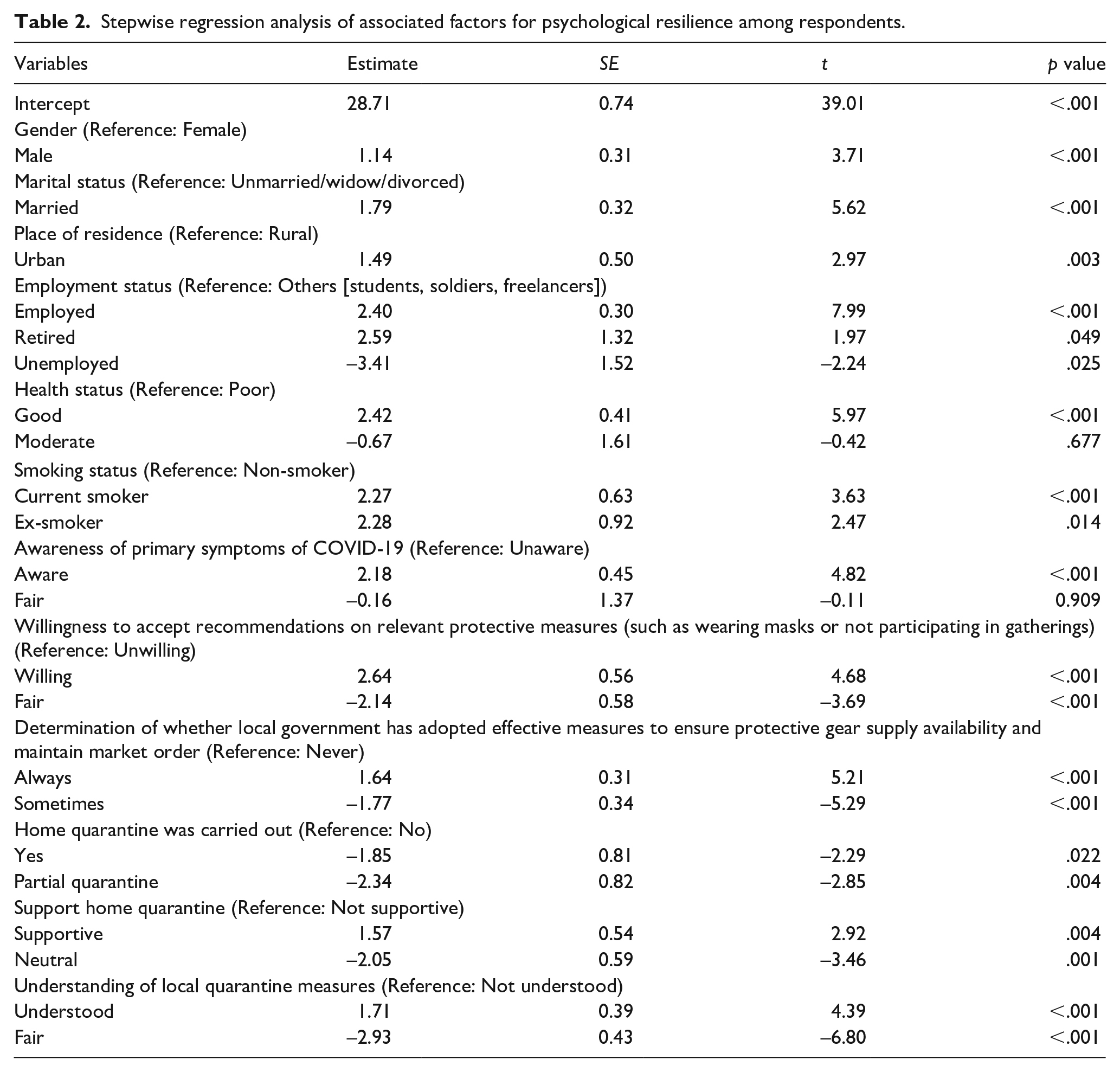
Table 3 reports the stratified multivariable linear regression results of predicted psychological resilience by gender and region. In groups with both genders, we found that marital status, region, individual health, clarity about primary symptoms of COVID-19, whether the local government has adopted effective measures to ensure protective gear supply availability and maintain market order, and understanding local quarantine measures are significantly related with psychological resilience. Male residents, who were married, in robust health, being current smoker, lived in places where the local government had adopted effective measures to ensure protective gear supply availability and maintain market order, and understand local quarantine measures have higher psychological resilience. Female residents, who were married, lived in urban areas, were clear about the primary symptoms of COVID-19, and understood local quarantine measures also had higher psychological resilience.
Stratified stepwise regression of predictors of psychological resilience by gender and region.
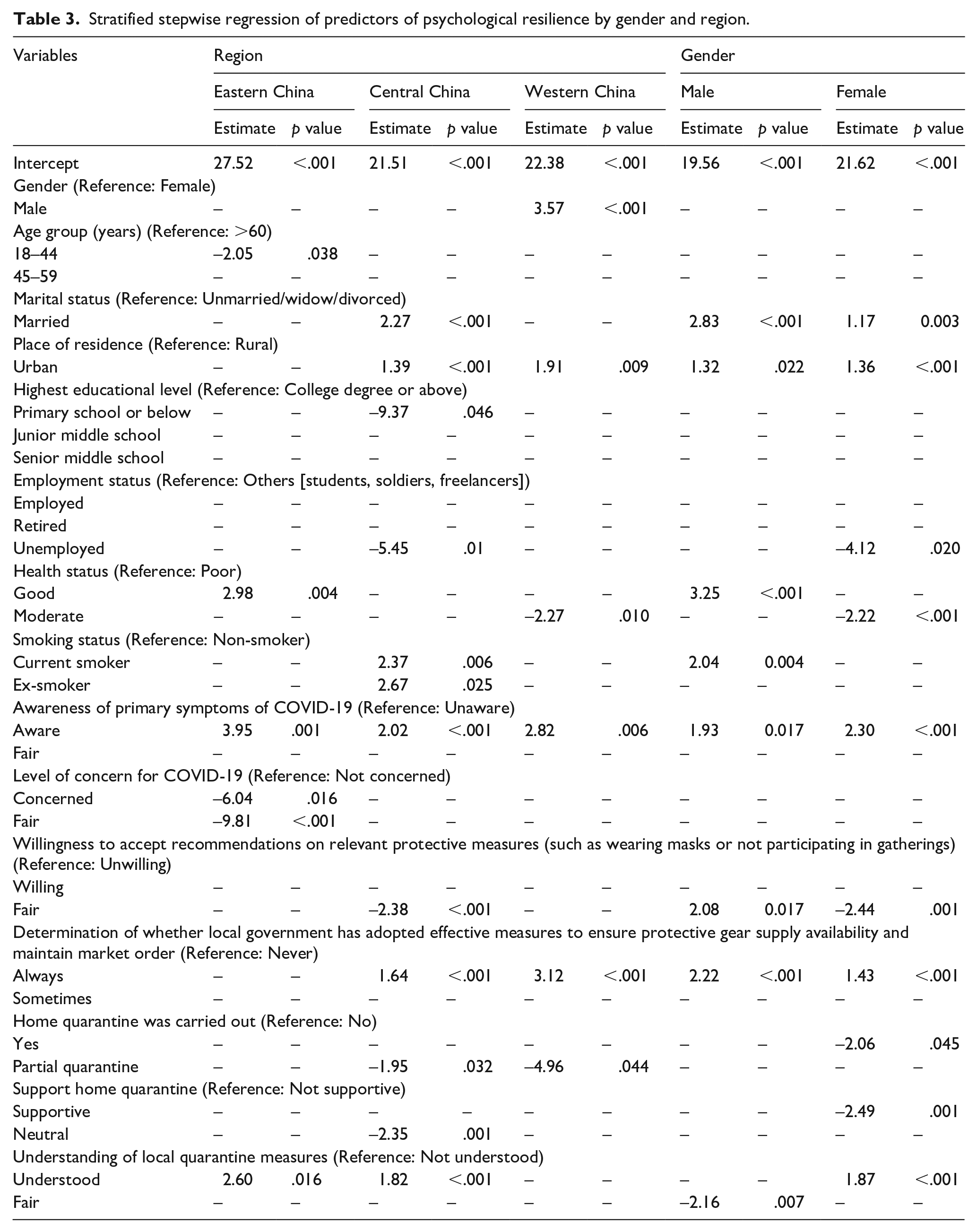
There were differences in the psychological resilience prediction results between different regions. In eastern China, residents with robust health status, who were clear about the primary symptoms of COVID-19, were less concerned about COVID-19, and understood local quarantine measures, had higher psychological resilience. In central China, residents who were married, live in urban areas, had higher educational levels, had fixed employment, being current smoker or ex-smoker, in robust health, were clear about the primary symptoms of COVID-19, living in places where the local government had adopted effective measures to ensure protective gear supply availability and maintain market order, and understand local quarantine measures have higher psychological resilience. In western China, residents who were male, live in urban areas, were clear about the primary symptoms of COVID-19, and lived in places where the local government adopted effective measures to ensure protective gear supply availability and maintain market order have higher psychological resilience.
Discussion
This analysis based on cross-sectional data from a large population showed that the mean psychological resilience score of Chinese residents during the COVID-19 pandemic was 27.11, indicating that they had low psychological resilience levels. Psychological resilience in these residents was affected by many factors, such as gender, age, marital status, residence, education level, employment status, health status, smoking status, clarity about primary symptoms of COVID-19, level of concern for the pandemic, willingness to accept recommendations on relevant protective measures, whether a local government has adopted effective measures to ensure protective gear supply availability and maintain market order, whether home quarantine was employed, support for home quarantine, and understanding of local quarantine measures. In addition, there were differences in the correlation between psychological resilience in residents and selected prediction factors by gender and region.
Married residents have higher psychological resilience than unmarried/widow/divorced, that is, had better psychological resilience levels. This may be because families can provide some support during emergencies. Therefore, married residents had more confidence in overcoming the pandemic. This phenomenon also appeared in residence, income status, and employment status. Residents who lived in urban areas, had better financial status, and fixed employment or retirement guarantees were calmer in the face of the pandemic and therefore can maintain a robust psychological status.
By integrating the psychological resilience of residents in different regions, we established that psychological resilience in residents from eastern China was higher than those in central and western China. A possible explanation was that economic development in eastern China was rapid and the quality of life of residents was generally better than those in central and western China. Owing to the effects of economic levels, residents from different regions exhibited different psychological health statuses during the pandemic. This suggested that countries and the government should focus on improving the economy and level of urbanization of residents to ensure that they have strong material foundations and risk-management capabilities and are able to maintain high psychological quality during emergencies.
Another study found that residents with higher educational levels have higher psychological resilience during a pandemic. At the same time, residents who were clear about COVID-19 symptoms have higher psychological resilience than those who are unclear. Further, residents who understand local quarantine measures had greater psychological resilience than those who did not. From these conclusions, we speculated that the cause of this was that residents with higher educational levels and who understand quarantine measures were more rational and can objectively foresee potential crises and changes. Therefore, they had better psychological status and maintain high psychological resilience (Zhong et al., 2020). This suggested that governments should actively conduct health education and policy popularization to improve policy understanding in residents in order to bolster psychological status.
Resident health was also an important factor that affected psychological resilience. Residents with robust health have a better psychological status than those in poor health. At the same time, residents who themselves as well as with relatives that were not confirmed COVID-19 cases had far higher psychological resilience than those who themselves and with relatives that were confirmed COVID-19 cases. We speculate that as COVID-19 was highly infectious, subjects in poor health or those with close contact with confirmed patients will have greater psychological stress. Therefore, the government should actively test suspected patients, treat confirmed patients, and carry out sufficient quarantine to ensure the health of residents.
Another finding was that when the local government adopted effective measures to ensure protective gear supply availability and maintain market order, residents usually had more psychological resilience. This shows that government policies can provide some psychological support for residents – residents will have the confidence to face the pandemic if the government employs effective measures to treat confirmed cases and control the spread of the disease (Reynolds et al., 2020). This suggests that governments should respond to the concerns of the public when a pandemic arises and employ relevant measures to ensure their livelihood along with the physical and psychological health of residents.
This study found that there were some gender differences in psychological resilience. Males had a greater level of psychological resilience than females. Employment status, home quarantine strategies, supporting home quarantine played important roles in predicting psychological resilience in females, while smoking status was significantly associated with higher psychological resilience in males.
Stratification analysis determine that psychological resilience in residents from eastern China was higher than those from central and western China and there was no major difference in psychological resilience between residents from central and western China. In addition to economic factors, the origin and major pandemic region was in central China (Hubei province) with the pandemic in surrounding provinces being complex, possibly the basis for the lowest psychological resilience in residents of central China.
China has a major rural population and is the world’s largest developing country (Tan et al., 2018). Even though China has greatly developed the healthcare industry and response capabilities towards public health emergencies after the 2003 SARS pandemic (Zheng, 2020), stronger measures are still required against the national COVID-19 pandemic and a heavy price has been paid to stop its spread. At present, COVID-19 has spread to more than 200 countries across the world and is defined as a pandemic by the WHO. In the face of a severe pandemic, how various countries, including many developing countries, handle it has become an extremely important international matter. When various governments adopt diverse pandemic control measures, they should actively pay attention to the psychological resilience of residents to maintain psychological health and social stability. At the same time, from a long-term perspective, various countries should enhance their economies, level of urbanization, and risk-management capabilities. Moreover, they should actively treat confirmed patients, isolate susceptible populations, strengthen health education, and improve residents’ understanding of health response policies to handle possible pandemics in the future.
Advantages and limitations
This study has several advantages. Firstly, this is the first national study on psychological resilience in residents and relevant factors. Secondly, compared with other studies, this study has a larger sample size of target populations in eastern, central, and western China. Further, in this study, professional research methods were used and a large sample size was employed for investigation to obtain reliable results. Thirdly, with the popularization of smart-phones and rapid development of communications tools, an Internet-based survey method was employed. This study was conducted in an advanced interaction platform and a higher response rate was obtained by chatting with the survey subjects.
However, this study has various limitations. In the questionnaire, some potential predictors of psychological resilience among Chinese resident were not investigated, such as culture. In addition, this is a cross-sectional study, which limits the temporal and causal relationships. Therefore, longitudinal studies should be conducted in the future to evaluate the relationship between various influencing factors and psychological resilience in residents.
Impact on future studies and practice
In the face of a severe pandemic, governments should pay attention to the psychological health of residents. Our study results suggest that it is necessary to employ measures to resolve and improve factors that are confirmed to be related to psychological resilience. Therefore, national healthcare policy makers should adopt relevant measures to improve the psychological resilience of residents during a pandemic. This includes short-term aggressive treatment, strengthening health education, and improving the awareness of residents regarding emergency health policies. In addition, financial status, health levels, and risk-management capabilities of residents should be improved over the long term. Moreover, additional studies measuring the average level and influencing factors of residents’ psychological resilience in China are warranted, which aims to provide some references for relevant research fields in China and internationally.
Conclusion
In conclusion, a low psychological resilience in Chinese residents during the COVID-19 pandemic reflects a poor psychological health. This is particularly for residents with poor financial status, living in rural areas, who are unmarried, have low educational levels, lack fixed employment or retirement guarantees, and lack knowledge on policies regarding lower psychological resilience. Our study results serve as a valuable reference for the psychological status of residents during public health emergencies in China and other countries while enriching international research on this topic. During pandemic management, the government should consider these factors and maintain the physical and mental health of residents.
Footnotes
Authors’ contributions
XS, YL, and YG conceived and designed the study. JF, KT, and YG participated in the acquisition of data. XS and YL analyzed the data. ZL and KT gave advice on methodology. XS drafted the manuscript. YL, JF, ZL, KT, and YG revised the manuscript. All authors read and approved the final manuscript. YG is the guarantor of this work and had full access to all the data in the study and takes responsibility for its integrity and the accuracy of the data analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Science Foundation of China (71804049), the Fundamental Research Funds for the Central Universities (2020kfyXJJS059), and Guizhou Province Science and Technology Support Project ([2020]4Y165)