
Abstract
Introduction:
Studies have demonstrated that mental health problems among university students may be increasing in both prevalence and severity. This study aimed to identify ways to reduce stigma and improve students’ utilization of mental health services.
Methods:
We performed a content analysis on video proposals to address stigma and mental health at universities, submitted by 15 teams from nine Asian-Pacific countries as part of a case competition. We examined five domains: (1) tone; (2) cultural context; (3) mental health issue of focus; (4) prevention versus secondary prevention; and (5) main intervention strategies.
Results:
Five main intervention strategies emerged: (1) educational campaigns; (2) peer interaction and support; (3) counseling; (4) screening; and (5) self-management. The results suggest that mental health literacy is low among students. Educational campaigns and events to increase awareness and reduce stigma were the most commonly incorporated strategy, through film screenings, mental health days, and social media. Building empathy through personal stories from celebrities and other students was also highly recommended. Second, counseling was incorporated in 80% of proposals, with a preference for peers and staff support, and web-based therapy over professional counselors, except in severe cases. Programs to increase social contact were the third most common strategy, suggesting students may feel isolated and disconnected. Creating common spaces for students to interact and pairing of students with and without mental health issues were widely suggested. The use of technology was recommended for self-management of mental health and for mandatory mental health screening, which was generally only recommended for incoming students.
Conclusions:
Our analysis provides insight into student-generated intervention approaches to prevent and address stigma associated with mental health issues among students. A greater university commitment is needed to provide a range of resources, including education and counseling, to leverage technology, and to foster stronger support networks among students.
Introduction
Mental health problems represent a significant health problem among university students. Studies from China, Hong Kong, Indonesia, Japan, Taiwan, and the US have all found that mental health problems among university students appear to be increasing in both prevalence and severity (Fan et al., 2012; Ohnishi et al., 2016; Peltzer et al., 2017; Sobowale et al., 2014; Tresno et al., 2012; Uchida & Uchida, 2017; Yousuf et al., 2013). Further, studies have shown that social isolation and mental health problems have worsened as a result of the recent COVID-19 pandemic (Chen et al., 2020; Orbin et al., 2020; Rains et al., 2021). Even in non-pandemic times, university can be a stressful time for students due to challenges such as separating from parents, forming personal relationships, living independently, managing coursework and other activities, and planning for a career. New and transfer students, and international students may be at greater risk of poor mental health due to major life changes as a result of entering the university (Chan et al., 2014; Liu et al., 2019). However, most of the existing studies on this topic have focused on medical students or come from Australia and the US.
Stigma and mental health services
Psychotherapy and medications have been shown to be effective in treating mental health problems. However, even when mental health services are available, their utilization among university students is very low (Eisenberg et al., 2012; Gulliver et al., 2010; Harrod et al., 2014; Kisch et al., 2005; Pirkis et al., 2003; Roh et al., 2009; Sobowale et al., 2014). Commonly cited barriers to utilization of these treatment include lack of mental health literacy, preference for self-management of problems, and negative attitudes toward mental health services (Eisenberg et al., 2012; Jennings et al., 2015; Roh et al., 2009; Zivin et al., 2009). Stigma has also been found to be a significant barrier; students may be reluctant to use services because of fears of being labeled or stigmatized by others, or because of their own feelings about mental illness (Gulliver et al., 2010). For example, Eskin et al. (2016) examined attitudes about suicide in 5,572 university students from 12 countries and found that Japanese students had among the highest suicide self-acceptance scores but the lowest social acceptance scores for a suicidal friend, suggesting stigma made it difficult for suicidal individuals to reach out to social support systems. A study by researchers used data from over 60,000 students at 75 US colleges and universities found that stigma about mental health was associated with suicidal ideation and self-injury (Gaddis et al., 2018).
It is clear that a stronger support system for university students suffering from depression and other mental health problems is urgently needed (Hunt & Eisenberg, 2010). Universities are increasingly prioritizing mental health services in order to treat mental health problems, prevent suicide, and improve overall student performance and well-being. But they are struggling to identify effective, evidence-based and culturally appropriate ways to reduce stigma associated with mental health care among students. This paper describes a content analysis of proposals developed by university students in the Asia-Pacific. As part of a global health case competition, teams were asked to design a campus-based intervention to decrease stigma associated with mental health issues. An analysis of the student-created interventions could provide insight into what strategies might be most appropriate to prevent and treat mental health issues among students.
Material and methods
The association of Pacific Rim Universities
The Association of Pacific Rim Universities (APRU) is a non-profit network of over 50 leading research universities in the region, representing 19 economies and more than two million students. Launched in 2007, the main objective of the APRU Global Health Program (GHP) is to advance global health research, education and training. It organizes an annual virtual Global Health Case Competition, open to undergraduate and graduate students from any university globally. Case competitions are increasingly used as an educational tool to allow students to exercise critical thinking skills to solve a complex, ‘real world’ challenge (Ali et al., 2011; Leon et al., 2015). In 2018, teams of five to six students were asked to develop a program with the main objective of reducing stigma associated with mental health problems on university campuses. The instructions indicated that the intervention plan should incorporate innovative and culturally-appropriate strategies that are based in evidence and that teams should consider real-world opportunities and challenges and come up with a comprehensive plan that is also realistic and could be implemented in practice. The case challenge was written by global health experts from the APRU GHP’s Advisory Group. Teams had 8 weeks to prepare a 10-minute video in English proposing an intervention that could be implemented at a university over 2 years with a hypothetical budget of US$40,000.
All videos submitted on time were assessed by a panel of nine global health experts from six different economies in the Asia-Pacific (China, Hong Kong, Japan, New Zealand, the Philippines, and the US). We conducted a content analysis of the video submissions to explore university students’ perspectives on stigma and mental health and strategies to combat this. Content analysis is a practical method of assessing prevalent themes and content of videos. As media communication becomes an increasingly influential platform for conveying health-related information, it can also be to examine the source of the health messaging, its audience, and how well the messaging is received (Stevens, 2018). Recent studies have employed this methodology on alcohol abuse (Cranwell et al., 2017), tobacco use (Paek et al., 2010), obesity (Puhl et al., 2013), Zika (Basch et al., 2017), generalized anxiety disorder (MacLean et al., 2017), marijuana (Krauss et al., 2017; Yang et al., 2018); PrEP (Kecojevic et al., 2020), and safer sex (Stevens, 2018). Park and Chang (2020) also found that coproduction of videos with adolescents was a beneficial health education method.
To analyze the videos, we developed a broad coding scheme to analyze domains of both tone and content of the videos. All videos were independently viewed at least three times by three members of the research team. A subsequent refinement of the coding scheme was done after the initial viewing period to reflect the dominant content and themes. Discrepancies in coding were resolved through a series of team meetings. However, the team had very high inter-rater reliability with few discrepancies.
Results
Teams
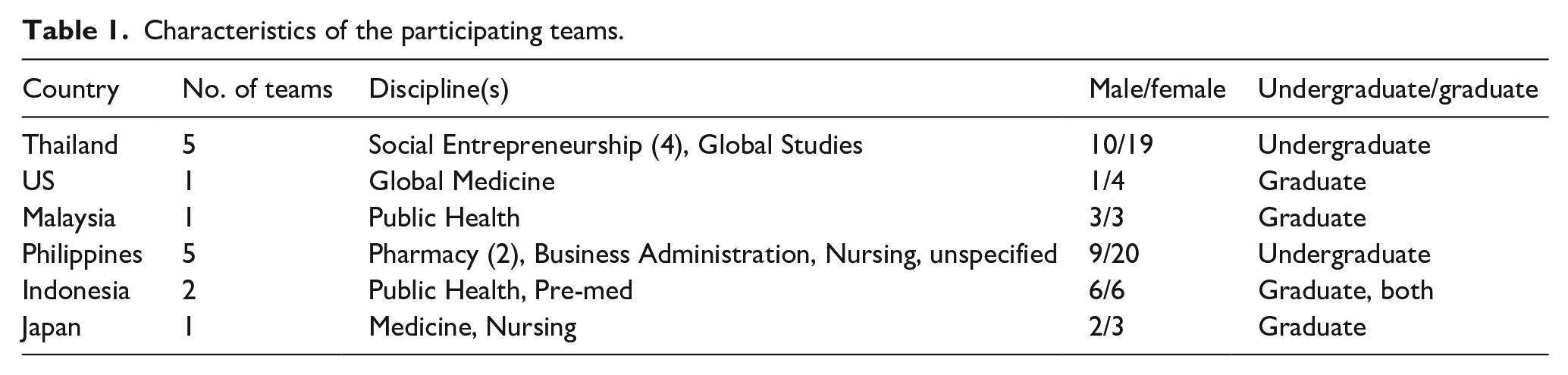
A total of 27 teams from 13 universities in nine economies registered for the competition and received the challenge. However, 15 teams, totaling 86 students, representing nine disciplines, and six countries (Indonesia, Japan, Malaysia, the Philippines, Thailand, and the US) submitted videos. Eleven teams were comprised of all undergraduates (73.3%), four of all graduates (26.6%), and one team had both (0.1%). About two-thirds (64%) of the students were female. Table 1 shows basic characteristics of the teams and participants.
Characteristics of the participating teams.
Five overall domains of the proposals were examined: (1) tone; (2) mention of cultural context; (3) mental health issue of focus; (4) prevention versus secondary prevention as main focus; and (5) main intervention strategies.
Domains
As seen in Table 2, most proposals employed an informational and/or utilitarian tone. The majority (60%) also incorporated dramatic elements such as depictions of suicide, bullying and interpersonal conflict. Many (47%) also included interviews with students about their personal experiences and/or with campus health professionals about the problem and services available. Second, in terms of cultural context, only four teams discussed cultural elements that may contribute to low utilization of help-seeking or increased stigma. However, most included national or international data highlighting the prevalence of mental health issues among university students and the factors that may increase risk, such as academic pressures, family and social expectations, and relationship difficulties. One team from the Philippines discussed culture in detail, including the importance of family and by using terms in the Filipino language. This team mentioned that despite the image of the Philippines being the ‘country of smiles’, anxiety and depression among students are common. Third, in terms of mental health problem of focus, depression (76%) and suicide (76%) were the most common. Fourth, while most incorporated some elements of primary prevention, only two teams’ proposals largely focused on primary prevention while the majority (87%) focused on secondary prevention of mental health issues, such as counseling and self-management.
Intervention proposal domains.

Note. Teams could include more than one sub-category of each domain.
Strategies
Five intervention strategies were most commonly incorporated into proposals: (1) educational campaigns; (2) counseling; (3) peer interaction and support; (4) self-management; and (5) screening. A short summary of each team’s overall concept is shown in Table 3. As seen in Table 4, the most common intervention strategies were education and counseling, incorporated by 87% of teams. A wide variety of educational campaign ideas were mentioned, including campus-wide events, (such as film screenings, yoga classes, and mental health days), informational websites and digital newsletter emails, virtual gaming, and social media sites. Print materials were rarely recommended, although one team suggested adding printed pamphlets to new student orientation packets. Many teams offered creative ideas to reduce stigma of mental illness. For instance, one team from Thailand proposed to conduct a student competition in which students would create films about mental health issues to be showcased in a campus film festival. An Indonesian team’s proposal included a campus talk show with celebrities who had experienced mental health challenges. Several other teams also recommended including personal stories that would be related to students, by either celebrities to classmates. A team from Thailand proposed a social media campaign called #zerostigma where students could share stories of their experiences to ‘sensitize students to this issue, reducing stigma’.
Overall concept of each intervention.

Common intervention strategies for each team.
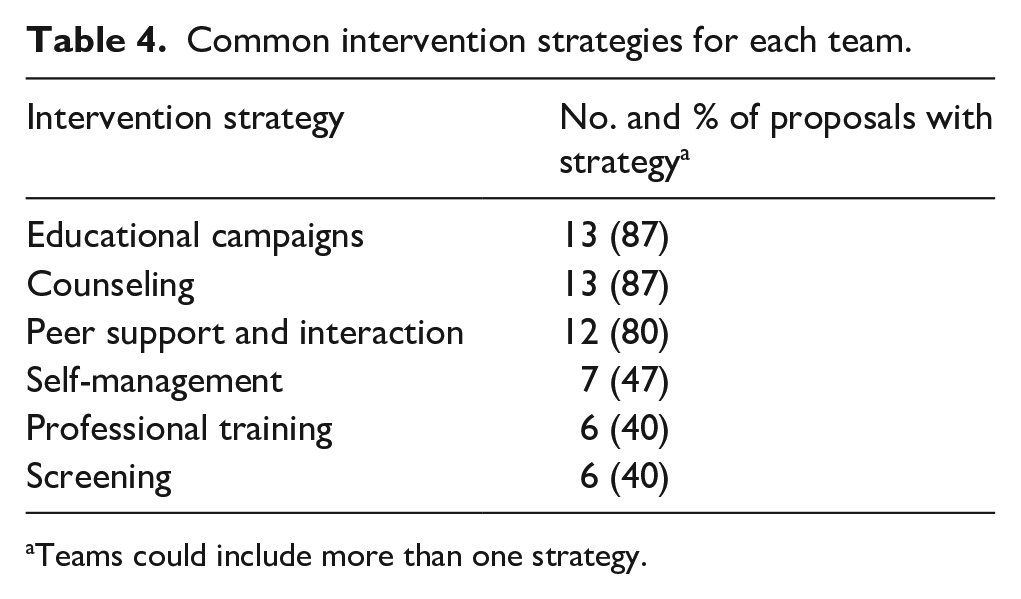
Teams could include more than one strategy.
Counseling was also recommended in 87% of the proposals, with a preference for in-person counseling. Most teams expressed a preference for close contacts, such as family members, neighbors, friends/peers, and faculty/staff, over professionals as the first point of contact. A few teams suggested group therapy sessions and a few proposed web-based, anonymous counseling. Most teams did not discuss existing mental health resources and counseling at their universities.
Peer support was incorporated in 80% of the proposals. Most teams mentioned the need to create a better sense of community among students, proposing events like candlelight vigils, art classes, and organized student social gatherings. For example, common spaces for students to work or socialize was suggested by six teams. One Indonesian team suggested planting a ‘commitment tree’ that would both promote a university commitment to addressing mental health issues, as well as provide a space for students to gather. Another Indonesian team proposed ‘creativity workshops’ through art and other activities to promote social interaction. Programs pairing students with and without mental health issues were also incorporated by almost 50% of teams. A team from the Philippines came up with the ‘BUDDY system’, matching a student who had experienced mental health issues with a student that had not to promote mutual feelings of belongingness. A team from Thailand included an app called ‘talk to me’, which would facilitate anonymous conversations between users and bi-directional learning among people with mental illness and those without. ‘Project EmpowerMental’ by a team in the Philippines paired freshman students with older students in a type of mentorship relationship. Another proposal included bulletin boards (called ‘free walls’) for students to post-it notes and stickers to ‘express themselves’ and share feelings with others. Despite their wide use in university settings, formal ‘gatekeeper’ programs were only recommended by one team.
Most proposals that mentioned screening (40%) integrated technology-based screening as opposed to in-person screening, deemed more efficient and acceptable. Mobile phone screening apps were most widely suggested. The majority concentrated their efforts on anonymous screening platforms that would encourage students with high scores to seek services but none had feedback loops that would be able to alert the university about a student who had scored high. In addition, most targeted incoming freshmen but only two incorporated any screening after the initial matriculation. One Filipino team incorporated a new app called ‘weconnect’, which would allow students to chat live anonymously with university staff for screening and referrals. All new students would be required to register for the app and complete a mental health evaluation.
About 40% of the proposals incorporated self-management techniques for mental health issues. Preferred methods included web-based platforms and journals/diaries to track stress levels. Stress reduction was recommended, through gaming and stress management techniques, such as yoga.
Discussion
Content analysis of student-created videos provided insight into the intervention approaches perceived to be most appropriate for their own demographic to improve mental health seeking among university students. As the recent COVID-19 pandemic has illustrated, students around the world are experiencing increasing mental health challenges. Understanding students’ ‘consumer perspectives’ may prove valuable in identifying appropriate approaches that may be overlooked by researchers and policymakers.
Among the 15 proposals reviewed, a focal point to tackle stigma of mental illness and promote mental health help-seeking were educational campaigns, which often included campus-wide events to raise awareness and the use of social media to disseminate information and personal stories. Increased awareness was viewed as the primary way to reduce stigma, which aligns with research demonstrating that education is effective in reducing stigma of mental illness among university students (Gaddis et al., 2018; Mittal et al., 2012; Thornicroft et al., 2016). Our results suggest low mental health literacy among students. The fact that so many proposals focused on severe mental illness issues, such as schizophrenia and suicide, also suggests that students may not be aware of the range and severity of possible symptoms of mental illness. Therefore, it may be beneficial to raise awareness about when it is appropriate to seek formal help. Universities should aim to reduce stigma of mental illness and encourage help-seeking behavior by providing students with more factual information about mental health in creative ways, including campus-wide events that may capture more attention than traditional methods, such as print campaigns. Universities should capitalize on the technological innovations available through telemedicine and other digital health tools to explore ways to provide education, as well as screening (King et al., 2015). However, expecting depressed students to actively seek out online resources may not be realistic. Indeed, one study found that despite the belief that the internet is often a preferred resource for young adults, few (10%) had used it to actually seek help (Arria et al., 2011).
Counseling was recommended by 87% of the teams. The fact that few teams mentioned available services on campus suggests a lack of awareness about existing resources and counseling at their universities. Counseling by professional mental health care specialists was almost exclusively preferred in-person versus online. Most commonly, teams proposed training of close contacts that depressed students may have contact with on a daily basis, such as family members, neighbors, friends/peers, and faculty/staff. It is possible that people with mental health problems would first contact family members or friends in these settings, and professional counselors might be perceived to be appropriate for severe, long-term mental health problems. The need to develop a more comprehensive and holistic plan for universities to address mental health was mentioned several times and usually focused on the lack of engagement between faculty, staff and students.
The third most widely incorporated intervention strategy was peer interaction or ‘social contact’, included in 80% of the proposals. Most teams incorporated some strategy to build or increase student interaction and supportive networks. Common spaces were commonly featured, suggesting that students may be feeling isolated or disconnected and could benefit from increased social interactions with peers for both primary and secondary prevention of mental health issues, as well as to reduce stigma associated with mental health issues. The idea of pairing a student that has experienced mental health challenges with one that has not was also commonly proposed to reduce stigma by increasing empathy through personal connections and dispelling myths and negative stereotypical beliefs about mental health problems. Evidence also shows that contact with persons with mental illness may be more effective than general education on reducing the stigma of mental illness (Corrigan et al., 2012). Three large literature reviews on interventions to reduce mental health stigma both found that social contact was very effective in improving stigma-related knowledge and attitudes in multiple studies from around the world, at least in the short term (Griffiths et al., 2014; Mehta et al., 2015; Thornicroft et al., 2016). Also widely recommended, personal narratives from celebrities and others who have experienced mental health problems have demonstrated effectiveness in reducing stigma in previous studies (Clement et al., 2015; Couture, 2003; Pettigrew, 2006). Universities should aim to increase opportunities for students to feel connected and part of the campus community that supports mental health. With internet ubiquitous, universities can explore new creative ways to leverage technological solutions to link students on and off campus to build more community.
Despite their wide use in university settings, formal ‘gatekeeper’ programs were only recommended by one team. However, the emphasis on peer support and training is suggestive of this approach. Gatekeeper programs, among the most common strategies used at the university level to improve mental health awareness and reduce suicide, aim to train ‘gatekeepers’ (such as friends, peers, family and university faculty, and staff) to recognize potential warning signs and intervene if necessary (Burnette et al., 2015; Chan et al., 2014). But, despite their wide used in universities in several economies, studies have had contradictory findings about their effectiveness (Rallis et al., 2018). Hashimoto et al. (2016) implemented a gatekeeper training program for 76 university staff in Japan and found significant improvements in management of suicidal students. Further, one-third of the participants had one or more chances to utilize their skills within a month of the training. Likewise, Katsumata et al.’s (2017) study of a gatekeeper program for Japanese university students also had positive results. Studies in universities in the US have shown that gatekeeper interventions have improved students’ ability to identify suicidal peers and increase their willingness to intervene (Samuolis et al., 2020), as well as increase the number of referrals to mental health specialists, especially among females (Rallis et al., 2018). However, some studies in Australia, US, and Netherlands have demonstrated no increase in help-seeking (Chan et al., 2014; Harrod et al., 2014; Lipson et al., 2020; Rallis et al., 2018; Terpstra et al., 2018). More research is needed in Asia-Pacific settings to explore the effectiveness of these interventions.
While several teams (40%) incorporated screening for mental health problems, they were almost exclusively directed at incoming students, and usually accomplished through online testing. Regular screening of students was rarely proposed. It is possible that incoming students were emphasized because they may have difficulty adjusting to new life changes. However, this suggests that more education is needed to alert students to the fact that mental health problems can affect students in all years. Among the teams that proposed screening, most proposed online, self-administered tests, which might not be sufficient to identify all students experiencing mental health issues, especially those less severe. More screening for mental health issues should be conducted among students presenting at student health clinics with physical complaints, such as headaches or sleep disorders, which could indicate mental health challenges (Fan et al., 2012). Our results also suggest that students lacked awareness about the mental health services available on campus, highlighting the need for universities to provide more information on where students can access mental health services on campus, and to ensure that adequate mental health services are available if they choose to use them. Further, students may be more likely to seek help outside of the university setting. Therefore, bridging connections with community-based organizations could help meet the need for services.
Another interesting finding is that most teams believed that mandating students to engage in activities such as educational workshops and app-based screening was preferred over voluntary activities. This may help ‘equalize’ the possibility of stigma due to self-selection in these activities; no students would be singled out for voluntarily participating, which they may fear could alert others that they were experiencing mental health issues. It may also suggest that students perceive a lack of openness surrounding discussions and information about mental health challenges and feel like everyone could benefit from increased attention to this issue. It is also possible that students feel that the programs will be underutilized if they are not obligatory. Indeed, a study from the US that utilized an optional online training for suicide prevention had very low participation (Manning & VanDeusen, 2011). Many proposals focused on individual, self-management approaches, such as anonymous apps to facilitate discussions or virtual diaries to track moods, corresponding with the literature indicating that young adults prefer to rely on themselves rather than to seek external help for mental health problems (Gulliver et al., 2010; Rickwood et al., 2007). These findings again suggest that stigma of mental illness may inhibit students from seeking formal mental health services unless the problem becomes severe.
Finally, our results highlight more investment is needed to support research on appropriate interventions to reduce stigma of mental illness and encourage help-seeking behavior (Thornicroft et al., 2016). The coordination of efforts across the global community to build evidence could inform policies (Hunt & Eisenberg, 2010). The use of standardized measures to compare interventions across countries will improve these efforts (Gaddis et al., 2018).
This study has some limitations. First, some countries were represented by numerous teams whereas others only had one team. In addition, numerous teams that had registered did not submit videos, which may have been due to the sensitive nature of this topic. Our data may reflect over-representation by norms and perspectives in those countries. While our findings may not be representative of the larger youth/student population, we feel that they provide potential avenues that merit further exploration. In addition, teams may have interpreted the case challenge differently, which may have influenced their intervention approaches. Finally, proposals may have been subject to social desirability bias and may have been designed in order to win the competition instead of reflecting students’ actual views.
Conclusions
Universities should foster a more supportive campus environment for mental health across the university community, making the mental health of students as important as physical health. To reduce stigma and encourage help-seeking behavior, more information about mental health could be provided in creative ways, such as campus-wide events and competitions. Our results suggest that students may feel isolated and disconnected, which may contribute to mental health problems. A greater commitment to provide students with a range of resources is warranted. Universities should reconsider the entire campus climate surrounding stigma of mental illness and mental health issues, aiming to build stronger support networks.