
Abstract
Background and aims:
Students from mental health related programmes may display stigmatising attitudes towards people of schizophrenia, however there are no data available on this population in Cyprus. The purpose of the present study was (a) to examine the levels of contact and stigma towards schizophrenia in Cypriot students of programmes related to mental health and students of other programmes and (b) to examine whether the successful recognition of a person with schizophrenia through a vignette and the estimation of severity levels was related to stigmatising attitudes.
Methods:
The participants were undergraduate students purposively selected across Cypriot universities (N = 152). A vignette depicting a person with schizophrenia, followed by the OMI to examine stigma and the BAE to examine contact with mental illness were used to collect the data.
Results:
The results showed that studying a mental health related programme and being a man was associated with more positive views related to social integration. No further stigma dimensions were predicted by the included variables. Similarly, level of contact and being able to identify the mental condition and estimate its severity was not related to stigma.
Conclusion:
The results emphasise the need to develop educational interventions to tackle stigma across students independently of their study programme and enhance mental health related programmes with opportunities for structured contact with patients with mental illness.
Schizophrenia is likely to affect several aspects of a person’s functioning, such as speech, thinking, mobility and perception and is probably one of the most stigmatised mental disorders (Groot & Hardingham, 2018). In their already difficult path for recovery and integration into the community, stigma can add significant obstacles (Fradelos et al., 2015; Vas et al., 2017). Additionally, as suggested by a relevant review, studies identified significant differences in stigma levels towards several mental illnesses showing that people with schizophrenia are more often considered dangerous, unpredictable or violent in comparison with patients diagnosed with depression or other mental disorders (Jorm et al., 2012). Policy makers and mental health professionals around the globe have been trying to eradicate the public stigma of the mentally ill for more than 50 years. Public or social stigma is often used to denote some form of discrimination towards an individual that is considered different from the norm (Markström et al., 2009). Based on the social cognitive approach, the concept of public stigma has been commonly considered as the combination of stereotypes, prejudice and discrimination (Corrigan, 2000; Kordosi et al., 2015), whereas Thornicroft et al. (2016) adopted a more practical-oriented view, and approached social stigma based on potential anti-stigma intervention outcomes. Attitudes (prejudice), knowledge (familiarity or ignorance) and behaviour (discrimination) were identified as the key components of public stigma and as potential intervention targets.
In line with this, contact with people with mental disorders has been recognised as a buffering factor against the expression of stigmatising attitudes (Thornicroft et al., 2016; Toner et al., 2018), as opposed to social distance (Anagnostopoulos & Hantzi, 2011; Corrigan & Nieweglowski, 2019). Though contact seems to be one of the keys towards tackling stigma, there is contradictory evidence regarding whether future mental health professionals express fewer stigmatising attitudes towards mental illness. One would expect that trainees in the field of mental health, do not experience stigma, as due to their studies they have more contact and display greater knowledge about mental disorders (Altindag et al., 2006; Reddy et al., 2005). However, evidence from previous studies with medical students suggests that they may also express stigmatising attitudes towards mental illness, especially schizophrenia (Economou et al., 2012; Vargas-Huicochea et al., 2017). Though not in a conscious level, students may be influenced by hidden curriculum mechanisms that act during their studies and replicate long preserved negative attitudes within the social and healthcare system, transmitted to the trainees by established professionals (Dubin et al., 2017; Holmes et al., 2015).
To our knowledge, there are no previous studies exploring the attitudes of students from mental health related programmes compared to other not related study fields, thus conclusions on the potential associations of programme curriculum and contents with stigma cannot be reached. Understanding the attitudes of future mental health professionals is very important, as through their future practice they may directly contribute to the results of treatment, rehabilitation and quality of life of patients with schizophrenia and other disorders (Omori et al., 2012; Wahl & Aroesty-Cohen, 2010). As the future mental health professionals may play a major role in correcting misconceptions of the public, promoting up-to-date acceptance and understanding behaviours, they should first be able to recognise and tackle their own stigmatising attitudes and behaviour (Servais & Saunders, 2007).
In the first national survey of Greece aiming at monitoring the stigma levels towards people with schizophrenia, participants expressed beliefs such as that people with schizophrenia are dangerous, have a split personality and are unable to marry or work. They also stated that they would be afraid to talk to a person with schizophrenia (Economou et al., 2009). When it comes to the Cypriot context, a recent survey in the country suggested that compared to mental health professionals, general population has fewer negative stereotypes and is more optimistic about the abilities of patients with mental illness (Panayiotopoulos et al., 2013). It is therefore important to examine whether such findings apply to the Cypriot student population, to understand whether the professionals’ attitudes are formed before or through their professional practice. Importantly, the curriculum of undergraduate studies for mental health related programmes (i.e. psychology, social work) in Cyprus does not provide students with opportunities of contact in an established clinical context, as it is theoretically based, training is not compulsory and opportunities for internships in mental health contexts are extremely limited.
Given that there is no evidence to date regarding stigma levels of students from mental health related programmes, there is a need to understand how the students of such programmes view people with mental disorders, so as to plan educational interventions to address any stigmatising attitudes (Wahl & Aroesty-Cohen, 2010), before their debuting to the clinical practice. In an effort to fill such gap and pave the way for future anti-stigma interventions, we adopted the approach of Thornicroft et al. (2016) and examined stigma components that may be potentially modified through interventions (attitudes, knowledge and behavioural intentions), as well as their possible relationship with social contact. Thus, the present study aims to (a) examine the levels of stigma and degree of contact with schizophrenia in Cypriot students from certain programmes related to mental health, as compared to students of other programmes and (b) explore whether the successful recognition or not of a person with schizophrenia through a vignette and severity estimation of the condition is related to stigmatising attitudes.
Hypothesis of the study
Studying a mental health-related subject and having higher contact with schizophrenia will be associated with lower stigma levels beyond sociodemographic variables.
Naming the correct diagnosis and estimating higher disease severity will be associated with higher stigma levels, independently of study programme.
Method
Participants
The total final sample consisted of (N = 152) students, exceeding the minimum required sample size of (N = 129) as calculated using the GPower analysis (Fual et al., 2007). The socio-demographic characteristics of the participants are displayed in Table 1.
Socio-demographic characteristics of the sample.

Measures
Demographic Data Questionnaire
A self-report questionnaire was created that consisted of closed-ended questions regarding gender, age in years, field of study (psychology, social work, law, business, other) and year of studies.
Vignette of schizophrenia (Zissi, 2006)
The following vignette describing a case of a male person with symptoms of schizophrenia was used
‘I will talk to you about Mr NB. He is very suspicious. He does not trust anyone and believes that everybody is against him. Sometimes he thinks that people that he sees in the street are talking about him and are watching him. A couple of times he has attacked people that did not even know. The other day he started swearing at his family, after threatening to kill them, as he says they are plotting against him, as the rest of the world’.
As our sample included students of university programmes not related to mental health, we considered essential to provide a personalised description through a vignette, instead of a mental illness definition. The vignette methodology has been widely used in attitude-exploring studies as it provides an elaborated method for depicting mental illness symptoms (Angermeyer & Schomerus, 2017). The vignette was followed by two questions: (1) ‘In your opinion, what is happening to the person in the above scenario?’), which was open ended and was coded as a dichotomic variable (correct: yes, incorrect: no) and (2) ‘How severe do you consider the condition described in the above scenario?’ followed by a Likert type answer (1 = Not at all severe–5 = Very severe).
Opinion about mental illness scale (OMI) (Cohen & Struening, 1962) – Greek version (Madianos et al., 1987)
This scale consists of 51 items that evaluate self-reported attitudes around mental disorders on a Likert scale (6: strongly disagree to 1: strongly agree) (Cohen & Struening, 1962; Madianos et al., 1987). It consists of five sub-scales: social discrimination (α = .87), social restriction (α = .91), social care (α = .63), social integration (α = .60), rationale (α = .70). Higher scores in social discrimination, social restriction and rationale indicate less stigma, whereas higher scores in social care and social integration indicate higher stigma. The OMI has been widely used to portray mental illness attitudes (Evans-Lacko et al., 2013), also in Greek speaking samples of the general and student population (Tzouvara et al., 2016).
Level of Contact Report (LCR) (Holmes et al., 1999) – Greek version (Arvaniti, 2008)
This self-report scale includes 12 sentences that assess the degree of familiarity of people with a person with mental illness (Arvaniti, 2008; Holmes et al., 1999). Participants are asked to circle the phrase or phrases that represent them, but only the sentence with the highest rating is taken into account. For the purposes of the study, the term ‘mental illness’ was replaced with ‘schizophrenia’. The instrument showed high reliability (α = .83).
Procedure
Following approval by the National Bioethics Committee of Cyprus participants were approached in the majority of the universities of the non-occupied Cyprus. The data collection was held in the classrooms and lasted approximately 20 minutes. Participants were initially given the Information sheet, containing information related to the research, its procedures and the protection of their personal data, followed by the Consent Form. Participants that accepted to take part in the study signed the consent form and were administered the questionnaire booklet. This included the vignette depicting the person with schizophrenia followed by the questionnaires. At the end participants were thanked and debriefed. Participation in the research was voluntary and anonymous. All the necessary requirements of the European General Data Protection Regulation (GDPR) of 2018 were observed.
Data analyses
IBM SPSS Statistics, Version 23 was used to perform the analyses. To test the first hypothesis a series of multiple regression analyses were performed, with the OMI subscales as the outcome variables and the type of study programme (mental health-other), contact with mental illness (LCR) and sociodemographic characteristics (gender, age, year of study) as the independent variables. Similarly, to test the second hypothesis a series of multiple regression with the OMI subscales as the outcome variables and naming the correct diagnosis (yes/no) and disease severity estimation based on the vignette as the independent variables were performed.
Results
Sample levels of stigma, contact, diagnosis and severity estimation
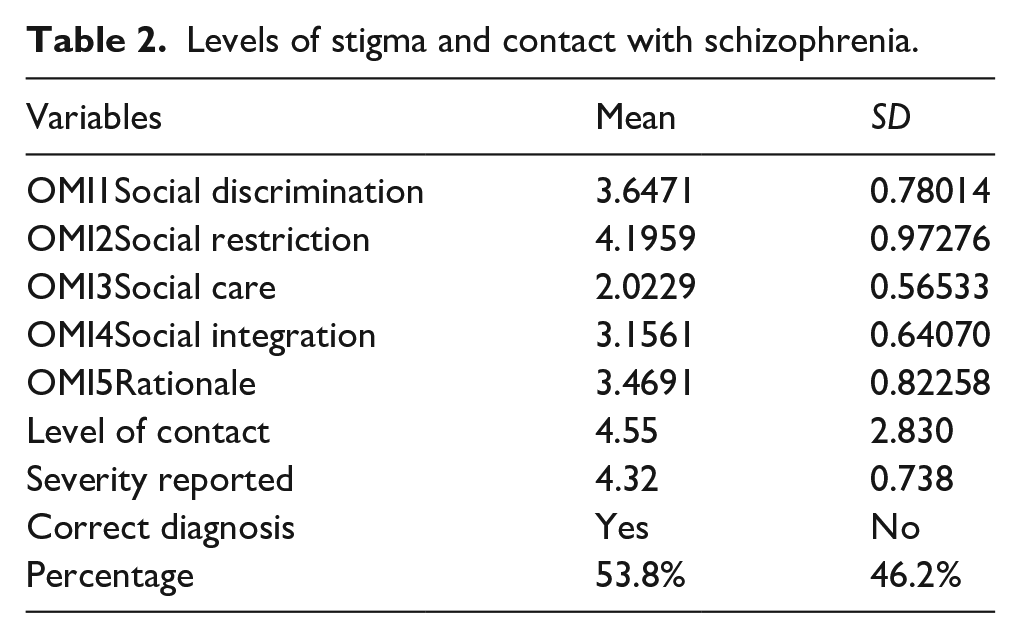
Participants expressed average levels of stigma across the dimensions of social discrimination, social integration and rationale, whilst their stigmatising attitudes towards social care and social restriction were somewhat low. Also, they reported a relatively low level of contact with people with schizophrenia. Finally, more than half of the sample was able to name the correct diagnoses of the case depicted in the vignette and considered that the condition was quite severe (Table 2).
Levels of stigma and contact with schizophrenia.
Hypothesis 1
Multiple regression analyses conducted for stigma subscales with study programme and level of contact as predictors revealed that study programme was significantly associated with social integration, whilst level of contact was not significant. When sociodemographic variables were entered to the model results showed that students from mental health related programmes together with being a man displayed more positive attitudes, [F (3, 130) = 3.430, p = .02] accounting for 27% of the variance of social integration (Table 3). No significant associations were found between the examined factors and the rest of stigma subscales (social restriction, social discrimination, social care and disease rationale).
Multiple regression for association between ΟΜΙ factors with level of contact, education and gender.

Hypothesis 2
Multiple regression analyses with the correct diagnosis and severity degree based on the vignette as predictors of stigma dimensions revealed no significant associations for any of the stigma subscales.
Discussion
The aim of this study was to examine the levels of stigma associated with schizophrenia in Cypriot students and explore whether studying a mental health programme (psychology, social work) plays a role, as compared to other programmes (e.g. law, business administration) beyond the influence of sociodemographic variables. Likewise, we explored whether the level of contact, naming the correct diagnosis and estimating symptom severity are related to the stigmatising attitudes. The stigma levels of our sample were overall within the average range, with participants displaying relatively more positive attitudes in the dimensions of social care and social restriction, in line with studies deriving from Greek and Greek Cypriot samples (Tzouvara et al., 2016), whereas their levels of contact with schizophrenia were relatively low, as compared to previous studies (Arvaniti et al., 2009). Almost half of the participants recognised the symptoms of the disorder in the vignette and the majority of them considered the condition of great severity.
The results partially confirmed the first hypothesis of the study, showing that being a man and studying a mental health related programme is associated to more positive attitudes towards the social integration of people with schizophrenia. Study programme or contact with mental health patients was not associated with any other stigma dimensions, indicating that university students share similar views when it comes to the social restriction, social discrimination, social care, or rationale of the disease for patients with schizophrenia. Also, familiarity with these patients does not determine the student’s views either. Similarly, being able to identify the symptoms of schizophrenia through a vignette and evaluating the severity of the depicted mental health condition does not seem to play a role on the students’ attitudes.
Social integration is characterised by the encouragement of equal social participation and inclusion of the people suffering from mental illness in every aspect of community life (Madianos et al., 2005). Stigma and consequent lack of social integration of people with mental illness may stem from the traditional notion of risk and disability (Ottati et al., 2005), which is even more evident in the case of severe disorders such as schizophrenia (Vargas-Huicochea et al., 2017). Based on our findings, receiving education in the context of a mental health related programme makes students more prone to normalise community inclusion of the mentally ill. This is consistent with previous studies, where students were less likely to express stigmatising attitudes after participating in educational interventions about mental disorders (Ahuja et al., 2017; Altindag et al., 2006). Still, findings from comparisons between the general population and mental health professionals are contradictory, with some studies reporting better attitudes in those professionals (Stuber et al., 2014), and others stating that the general public displays fewer negative stereotypes and more optimism about the abilities of the patients, as compared to mental health professionals (Economou et al., 2012; Panayiotopoulos et al., 2013).
When it comes to gender, our findings are not consistent with previous studies with students, with women showing a more humane attitude towards the mentally ill (Pascucci et al., 2017). However, our findings are in line with studies performed within the same sociocultural context. Specifically, a study conducted in Greece with health and mental health students, suggested that men do not support the notion that patients should be socially limited (Arvaniti et al., 2009). Similarly, a survey among Cypriot mental health professionals found that men are more optimistic about the abilities of mentally ill patients (Panayiotopoulos et al., 2013). A feasible explanation was provided by Arvaniti et al. (2009) suggesting that in the Greek and Greek Cypriot context women are more reluctant towards the social integration of people with mental illness, holding more reserved views regarding their care.
None of the factors examined in the present study was found to be associated with the rest of stigma dimensions, indicating that participants in our sample were displaying similar attitudes independently of their study programme or sociodemographic characteristics. Importantly, though the contact levels for our participants were low, it seems that the mere contact with people suffering from schizophrenia is not enough for tackling misperceptions regarding these patients, as contact was not associated to any of the stigma dimensions. It seems that education regarding the characteristics of schizophrenia combined with the level of contact, significantly predict the formation of attitudes (Ahuja et al., 2017), only when students have frequent and high degree of contact with this population (Eack & Newhill, 2008), which is not the case for Cypriot undergraduate students due to the above-mentioned curriculum limitations. In fact, a recent study revealed that postgraduate students of mental health related programmes showed less desire to social distance from people with mental illness compared to undergraduate students, possibly due to opportunities for interaction with these patients provided within the post-graduate curriculum (Pranckeviciene et al., 2018).
Οur results also showed that whether or not students were able to identify the diagnosis and assess the condition severity in the clinical case depicted in the vignette was not related to any of the stigma dimensions. The hypothesis that recognising the symptoms of schizophrenia is not related to stigma levels has been supported by previous research (Wright et al., 2011). And although the symptoms of schizophrenia are usually assessed as much more severe than other mental disorders (Zissi, 2006), our findings suggest that considering the condition severe does not play a role in the students’ views either.
To the best of our knowledge, this is the first study examining stigma levels on a wide range of study programmes and after taking into account a series of factors frequently reported as stigma correlates. The fact of including participants from the majority of the universities across the country makes this study the first of its kind within the Cypriot context and adds to the previous mental health related literature in this community, which is currently scarce. However, the present study does not come without its limitations. First, the fact that participants reported stigma levels within the average range may be due to social desirability effects, as the data collection was held within their classroom and students may have felt under pressure to provide a more positive evaluation of their attitudes (Economou et al., 2009). Second, two of the stigma subscales showed relatively low reliability and perhaps a more recently created instrument, with higher reliability would have increased the analyses strength. Third, the gender of the person portrayed through the vignette may have affected the responses, as previous studies have reported higher stigma levels towards males with mental illness (Dolphin & Hennessy, 2014). Future research should control for potential gender influences by perhaps using both male and female vignettes. Fourth, the cross-sectional nature of the study does not allow for the establishment of causal relationships. Fifth, the question regarding factors that may be associated with stigma in these students was partially answered. A comparison with post-graduate students replicating previous findings (Pranckeviciene et al., 2018), or the assessment of stigma levels of Cypriot postgraduate students before and after a training period in mental health related facilities may offer further insight on specific elements that may underlie stigmatising attitudes in Cypriot students.
The findings of the present study indicate the need to reduce stigmatised beliefs in students. Future, as well as existing mental health professionals such as psychologists, social workers and others, act as role models and public opinion leaders on mental health issues. They are also the ones who will meet people with mental disorders in their vulnerable moments and on whom those patients will rely for their recovery, thus the way professionals treat people with mental illnesses is likely to have a significant impact on their treatment process and their overall quality of life. However, a review of stigma levels of mental health professionals also reveals an ‘inconsistent picture’, which has not changed throughout the years. The authors conclude that we will need to focus on the training of future mental health professionals and enhance its components with strategies that ‘might help to generate greater acceptance and understanding’ (Wahl & Aroesty-Cohen, 2010). One of such strategies may be the direct exposure of students to cases of patients with mental disorders through their internship or specialised courses (Morgan et al., 2018). Α recent meta-analysis suggested that internships offering direct contact with people with mental illness, appear to play a major role in shaping students’ attitudes, acting as a means of experiential learning and a powerful tool for the fight against stigma (Petkari et al., 2018). Importantly, a previous report highlights the content of the messages conveyed during contact, more than the contact per se (Nguyen et al., 2011). Thus, structured sessions that combine clinical observation and question and answer modules may help to dispel the myths around mental illness.
In conclusion, the present study points towards the curriculum revision of mental health related programmes in Cyprus, incorporating stigma-buffering strategies. Currently, the fundamental goal of the national mental health policy is to decentralise the existent mental health services by expanding community care and this way shift the focus from the medical aspects of psychiatric disorders to social inclusion. For this transition to succeed, we believe that future mental health professionals that are stigma free and well equipped with recovery promotion tools are key agents of the process.