
Abstract
Background:
Stigma is a barrier to mental healthcare. Understanding context-specific stigma is important in designing mental health interventions.
Aim:
This study explored the nature and patterns of mental health stigma among community members in Afghanistan.
Methods:
Using cross-sectional data (n = 718), descriptive and inferential analyses were conducted. Multivariable linear regression identified determinants of stigma, as reflected by: (1) preference for social distance in relation to depression and psychosis, and (2) intended stigmatising behaviours in relation to mental illness.
Results:
In descriptive analyses, stigma toward depression and psychosis, especially regarding work and marriage, was found. The label of ‘mental illness’ was especially stigmatising. Most respondents would disclose a mental health problem to family only. Findings of inferential analyses included: stigma was positively associated with higher socioeconomic status, depression and belief in dangerousness; and negatively associated with urban location, female gender, familiarity and belief in a positive prognosis.
Conclusions:
This study provides new insights on stigma, to inform action in Afghanistan, an under-researched context. Further research and actions must prioritise supportiveness at the family level, especially in remote regions and address cultural issues of the social cost of associating with mental illness. More culturally appropriate, non-stigmatising language surrounding mental illness should be developed.
Mental disorders significantly add to the burden of disease in low and middle-income countries, being the leading cause of disability adjusted life years from non-communicable diseases (Mascayano et al., 2015). Afghanistan faces these and added challenges. The country has been in conflict for four decades (Ansary, 2012) and was ranked 170th of 189 countries in the 2019 Human Development Index (United Nations Development Programme [UNDP], 2019). These stressors can serve to further compound the burden, with 17% of Afghans estimated to experience mental disorder (World Health Organization [WHO], 2017). Furthermore, there is a large mental health treatment gap in Afghanistan (Hayward & Babury, 2013).
Stigma is defined as the ‘situation of the individual who is disqualified from full social acceptance due to a deeply discrediting attribute’ (Goffman, 1963). In the case of mental illness, this discrediting attribute could include, for example, the diagnostic label of mental illness, symptomatic behaviour or contact with mental health services. Stigma is a global issue (Patel et al., 2014), recognised as the single greatest barrier to community-based mental healthcare (WHO, 2001). It contributes to the treatment gap by discouraging help-seeking (Shidhaye & Kermode, 2013).
Stigma has been conceptualised as having three components: knowledge, attitudes and behaviour (Thornicroft et al., 2007). It manifests in many ways (Pescosolido & Martin, 2015) – for example, it can be observed at the community level. Attitudes to mental illness in the general population can be studied; one approach is to assess community members’ preference for social distance from, and intended behaviours toward, persons who have a mental illness.
The expression of stigma varies by culture (Yang et al., 2007), and it has been underexplored in Afghanistan. Understanding stigma in context is important in the design of locally appropriate mental health and anti-stigma interventions. While evidence on stigma from low-income settings is emerging (Patel et al., 2014), there is little literature from Islamic countries, and Afghanistan is a unique setting. Several salient features of the context, relevant to the question of stigma, should be highlighted.
First, Afghans are 99.7% Muslim (approximately 84%–89% Sunni and 10%–15% Shia (Central Intelligence Agency, 2021), and Afghanistan is known as a particularly conservative Islamic nation (Pew Research Center, 2013). Associations between stigma and increased religiosity have been found in other (including Islamic) contexts (Abuhammad & Al-Natour, 2021; Peteet, 2019). Fatalistic beliefs about illness (i.e. it is God’s will) are also common in Afghanistan (Eggerman & Panter-Brick, 2010).
Second, Afghanistan is known for its honour culture (Baldry et al., 2013; Gibbs et al., 2019; Mohammadi, 2011), which is based on the concepts of status, reputation and gender-based behaviour codes (Mosquera, 2013; Vandello & Cohen, 2003). In honour cultures, social ostracism and loss of reputation in the community can cause severe economic difficulty (Allan et al., 2018; Thornicroft, et al., 2009; Trani et al., 2016). Honour culture has been identified as a potential amplifier of mental health stigma (Brown et al., 2014).
Third, Afghan women are generally considered to occupy a lower social status than men (Baldry et al., 2013; Manganaro & Alozie, 2011), and are known to face deep gender inequalities which have been described as ‘extreme’ and ‘exceptional’, even in comparison to the challenges faced by women in other low-income settings (Van Mierlo, 2012).
Fourth, Afghanistan is a conflict and post-conflict setting. Afghanistan is a collectivist culture with traditionally strong social support networks (Mohammadi, 2011), which potentially could lessen the impact of stigma. However, conflict is a disruptor of these social support networks, especially through factors such as forced migration and displacement uprooting people from their communities.
Thus, Afghan culture has strengths but also factors that could ostensibly create an environment of high mental health stigma, or at least an environment where the impact of stigma is felt more acutely. However, without research such as this, the exact expression of stigma is largely unknown. Therefore, this study aimed to explore the nature and patterns of mental health stigma among community members in Afghanistan. Specifically, this study examined stigma as reflected in (1) a preference for social distance in relation to depression and psychosis, and (2) intended stigmatising behaviours in relation to mental illness in general.
Methods
This study used cross-sectional data to explore mental health stigma among community members in Afghanistan. These data were collected through a survey conducted in 2017 by the International Assistance Mission (IAM; https://iam-afghanistan.org), an international non-governmental organisation working in Afghanistan since 1966.
Sample and setting
Survey respondents were residents of Herat city in Herat Province, and Qala-e-Naw city in Badghis Province, both in western Afghanistan. Herat is the third largest city in Afghanistan, and is one of the most economically advanced areas there (Leslie, 2015). Qala-e-Naw is a small, impoverished city and Badghis province is overwhelmingly rural, with agriculture the primary income source for most people (World Food Programme, 2017). Herat is more diverse, with a considerable population of internally displaced people. Seven hundred and eighteen community members participated (sufficient sample size for the conducted analyses (Bujang, et al., 2018)). The large sample was intended to provide a broadly representative group of respondents; however, as no data were collected on persons who declined participation, we cannot assess to which extent the sample is representative of the population.
Procedure
For data collection, cities were stratified into areas of relative poverty and wealth. Within each area, a random starting point was chosen and every 15th house on the right side selected for interview. Where no answer occurred, the next house was chosen. Data were collected over 20 days.
All participants gave written consent for their data to be used in research. Ethical approval was obtained from the Government of Afghanistan’s Research Ethics Committee in the Ministry of Public Health (ref. 43998), and the Research Ethics Committee of the London School of Hygiene and Tropical Medicine (ref. 19192).
Measures
Data were collected using a survey developed by the PRIME (Programme for Improving Mental Healthcare, 2020) research group. The instrument was initially validated in India (De Silva et al., 2016), and subsequently translated into Dari. It included vignettes adapted to be culturally appropriate for Afghanistan, reflecting accurate names, routines and typical work settings (refer to Box 1). The full research instrument is available from the authors on request.
Depression and psychosis vignettes.
Sociodemographic data were collected regarding age, gender, years of education, occupation, marital status, home ownership, land ownership and indebtedness. The latter three indicators were combined into one socioeconomic status variable (scored 0–3). Higher scores indicated higher socioeconomic status.
Data on emotional state were collected using the Depression Anxiety and Stress Scale (DASS)-21. Using standard scoring of the scale (Lovibond, 1993), responses resulted in scores for depression, anxiety and stress, which were categorised as ‘normal’, ‘mild’, ‘moderate’, ‘severe’ or ‘extremely severe’.
Social distance in relation to depression and psychosis
These data were collected in response to two vignettes, depicting a person with depression (‘Nasiba’) and a person with psychosis (‘Ahmad’).
Social distance was assessed through five statements on participants’ willingness to engage in relationship at differing levels of intimacy with a person similar to the vignette (i.e. be a neighbour, spend time socialising, develop a friendship, work closely with or have person marry into the family). Responses were scored as ‘strongly agree’ (0), ‘agree’ (1), ‘don’t know’ (2), ‘disagree’ (3) and ‘strongly disagree’ (4), and the items were combined into a ‘Social Distance Score’ ranging from 0 to 20. A higher score represented greater preference for social distance.
Participants responded to statements addressing (i) beliefs about aetiology (four items), (ii) beliefs about prognosis (two items), (iii) beliefs about a person with the condition (three items), (iv) views on the helpfulness of various treatments (six items), (v) familiarity with the condition (one item), (vi) exposure to media concerning the conditions (two items) and (vii) help-seeking behaviours (two items). The two prognosis items were combined into one item in which a positive response to either question counted as belief in the possibility of recovery. Participants responded to some statements with ‘yes’ or ‘no’ and some statements on a 5-point Likert scale from (0) ‘strongly disagree’ to (4) ‘strongly agree’. For inferential analysis, Likert scale variables were considered as ‘agree’/‘disagree’/‘don’t know’.
Intended stigmatising behaviours in relation to mental illness
These data were collected in relation to the concept of mental illness in general, rather than vignettes.
Intended stigmatising behaviours were assessed using the intended behaviours subscale from the Reported and Intended Behaviours Scale (RIBS) (Evans-Lacko et al., 2011). The RIBS is a reliable and valid measure of discriminatory behaviour that is often used to assess effectiveness of anti-stigma interventions. It consists of four statements about a person’s willingness to live with, work with, live nearby and continue a relationship with a person with mental illness. Responses to the items were on a 5-point Likert scale from ‘strongly disagree’ (0) to ‘strongly agree’ (4). A composite score, ranging from 0 to 16, was generated with a higher score representing more positive intended behaviours (i.e. less discriminatory behaviour and greater willingness to engage in relationship) toward persons with mental illness. The RIBS has been found to have strong test-retest reliability (Cronbach’s α = .85).
Participants responded to statements regarding (i) stereotype endorsement (three items), (ii) beliefs about prognosis (two items), (iii) benevolent attitudes (three items), (iv) exposure to mental health information in the media (two items), (v) help-seeking behaviours (one item), (vi) willingness to self-disclose mental illness (two items) and (vii) familiarity with mental illness (two items). For items with many possible responses, dichotomised variables were created. For example, participants could choose from multiple options regarding where they had heard about mental illness in the media (newspaper, TV, radio, etc.). For inferential analysis, this was converted into a binary variable (‘Have you heard about mental illness in the media, yes or no?’). Participants responded to some statements with ‘yes’ or ‘no’ and some statements on a 5-point Likert scale from (0) ‘strongly disagree’ to (4) ‘strongly agree’. For inferential analysis, Likert scale variables were considered as ‘agree’/‘disagree’/‘don’t know’. Statements relating to stereotype endorsement and benevolent attitudes were combined into a composite score; further detail regarding the scoring of stereotype endorsement, beliefs about prognosis, and benevolent attitudes are available in the Supplemental Appendix.
Data analyses
Exploratory descriptive and inferential analyses were conducted. Multivariable linear regression identified determinants of stigma.
Descriptive analyses
Descriptive summaries were generated by reporting percentages and frequencies of all nominal and categorical variables. Means and standard deviations were reported for continuous variables. Wilcoxon signed-rank tests were conducted to assess differences in responses to Likert scale-based variables between the vignettes and differences in the dichotomised help-seeking variable and social distance scores. P-values are reported with results of descriptive analyses.
Inferential analyses
Multivariable linear regression analyses were conducted to assess determinants of stigma, as represented by (1) social distance in relation to depression and psychosis, and (2) intended stigmatising behaviours in relation to mental illness in general. For question (1), the outcome was the social distance score, and predictors were all sociodemographic variables, emotional state and dichotomised responses to the vignettes. For question (2), the outcome was the RIBS score, and predictors were all sociodemographic variables, emotional state and all other general mental health literacy variables from that section of the survey.
In these analyses, univariable linear regressions were first conducted to explore independent associations between the outcome and each predictor variable. Multivariable regression models were then constructed. Gender and location were included a priori in all models, given the importance of gender inequalities in Afghanistan (Van Mierlo, 2012) and differences in the two data-collection locations. The variables for familiarity and dangerousness were included a priori given their importance in relevant literature (Angermeyer et al., 2004; Corrigan et al., 2012). Additional predictor variables associated with the outcome, as determined by a p-value of less than or equal to .25 (Bursac et al., 2008; Zhang, 2016), were also included in the multivariable model. Results (β coefficients, 95% confidence intervals and p-values) of univariable and multivariable analysis were reported. Analyses were conducted using Stata 16.1.
Results
Descriptive analyses
Table 1 summarises frequencies and percentages of demographic characteristics and emotional state responses.
Descriptive characteristics of sample.
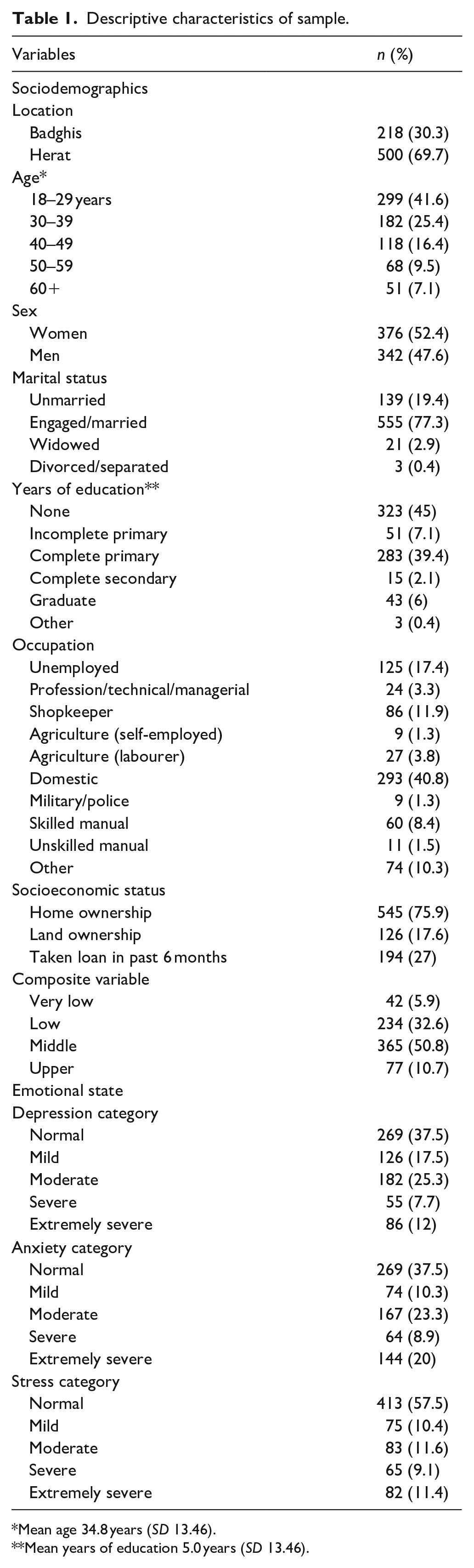
Mean age 34.8 years (SD 13.46).
Mean years of education 5.0 years (SD 13.46).
Figure 1 shows proportions of responses to each vignette, grouped by knowledge domains. The five questions at the bottom of each vignette’s section were combined into a social distance score. Mean social distance scores were 8.82 (SD = 4.92) for the depression vignette and 11.74 (SD = 4.97) for the psychosis vignette. The difference between these scores was statistically significant (p < .001) in Wilcoxon signed-rank test results.
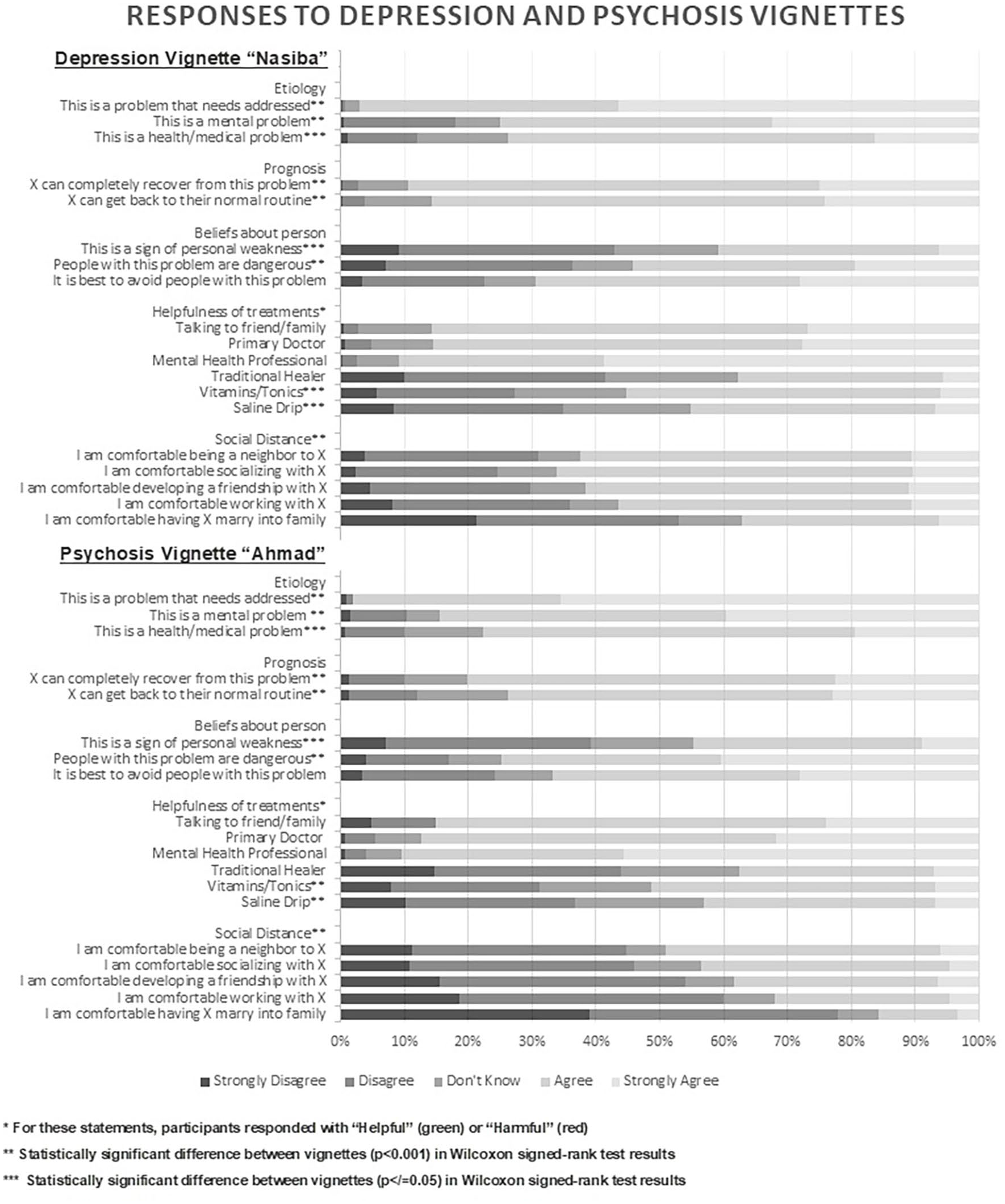
Responses to Depression and Psychosis Vignettes.
Figure 2 shows proportions of responses to items related to mental illness generally, including responses to the RIBS.
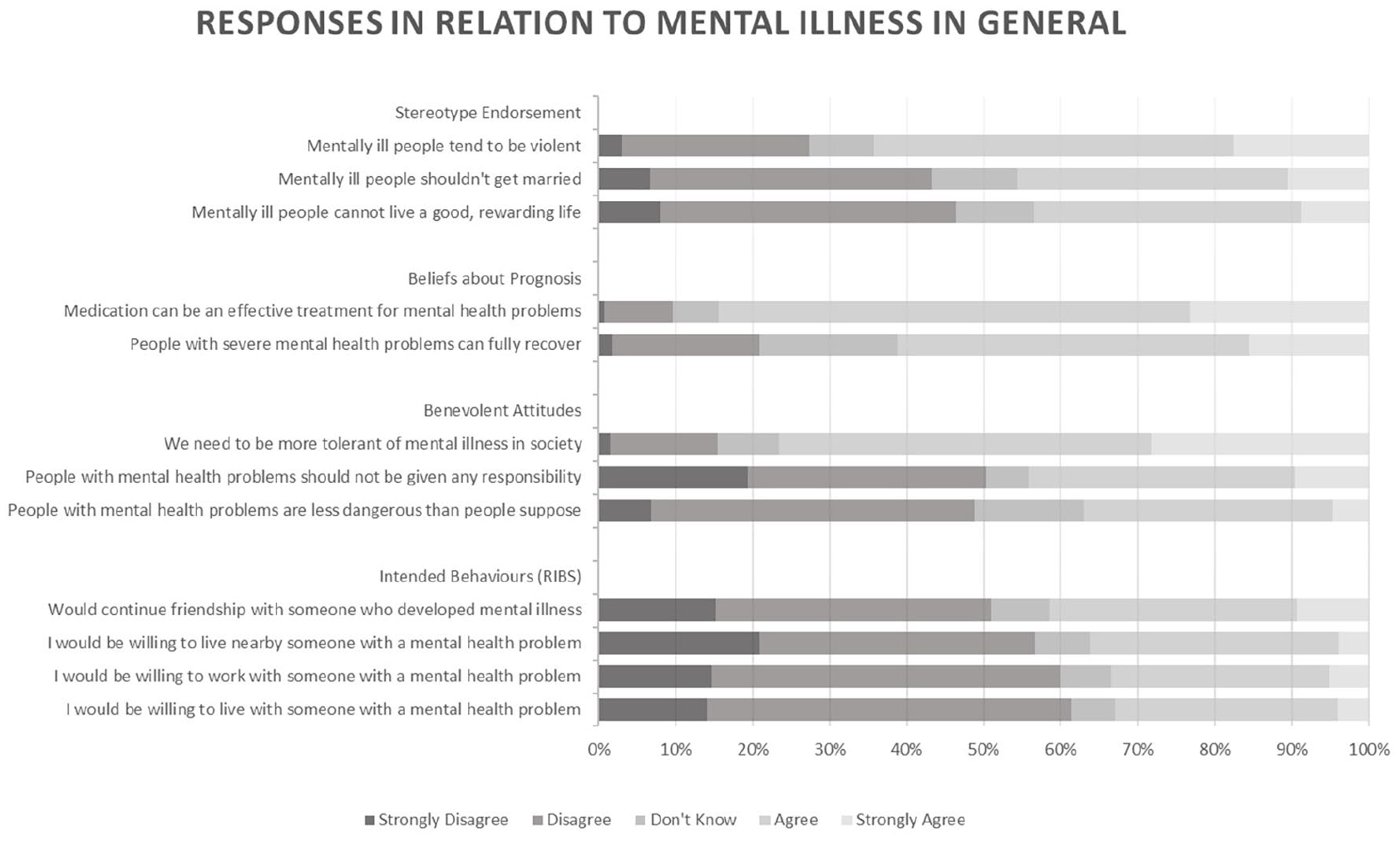
Responses in Relation to Mental Illness in General.
Table 2 shows proportions of responses to additional, non-Likert based items on the survey relative to both questions (1) and (2). Summary scores for composite variables based on the statements from Figure 2 are displayed.
Additional variables.
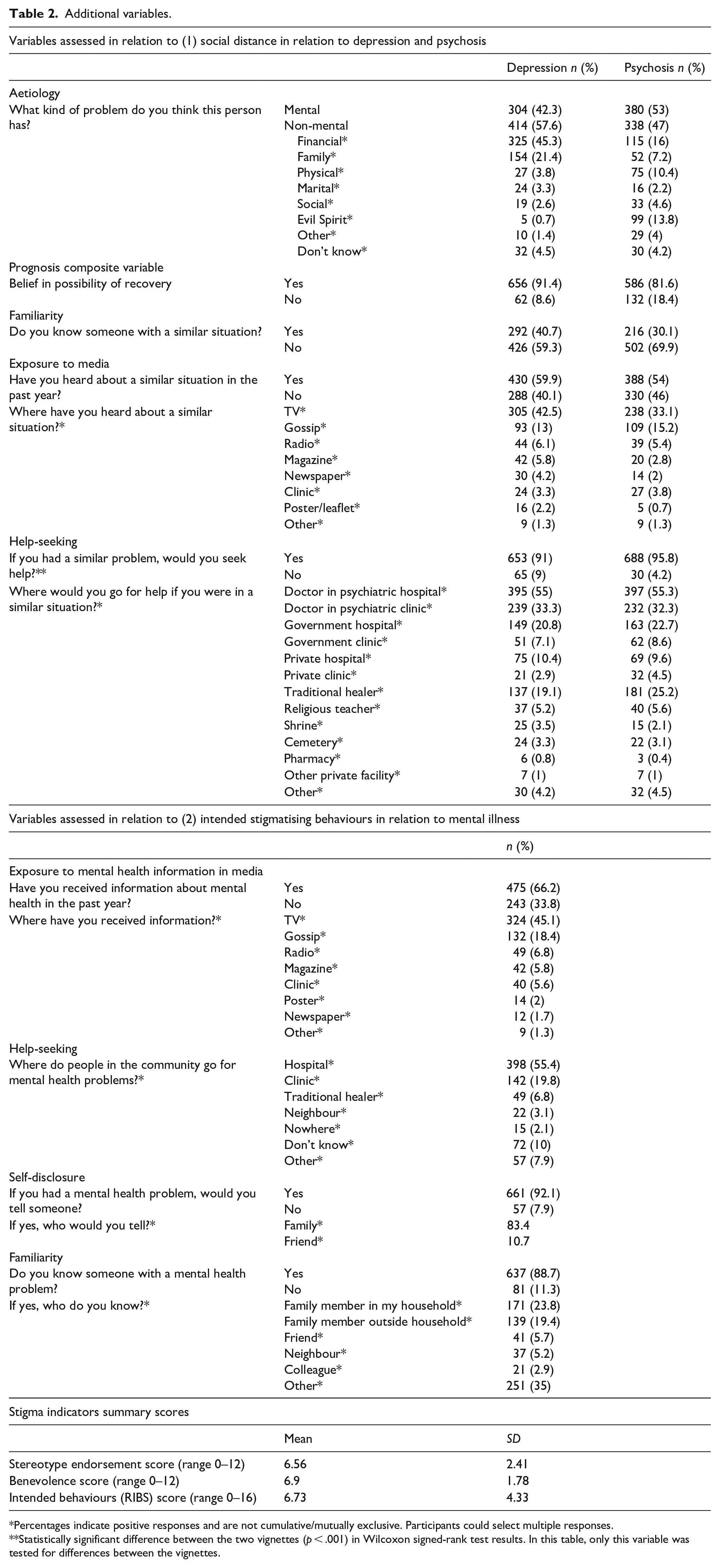
Percentages indicate positive responses and are not cumulative/mutually exclusive. Participants could select multiple responses.
Statistically significant difference between the two vignettes (p < .001) in Wilcoxon signed-rank test results. In this table, only this variable was tested for differences between the vignettes.
Inferential analyses
Social distance in relation to depression and psychosis
Table 3 shows results of linear regression for both vignettes, with the outcome of Social Distance Score and predictor variables being sociodemographics, emotional state and responses to statements about the vignettes.
Predicting social distance in relation to depression and psychosis.
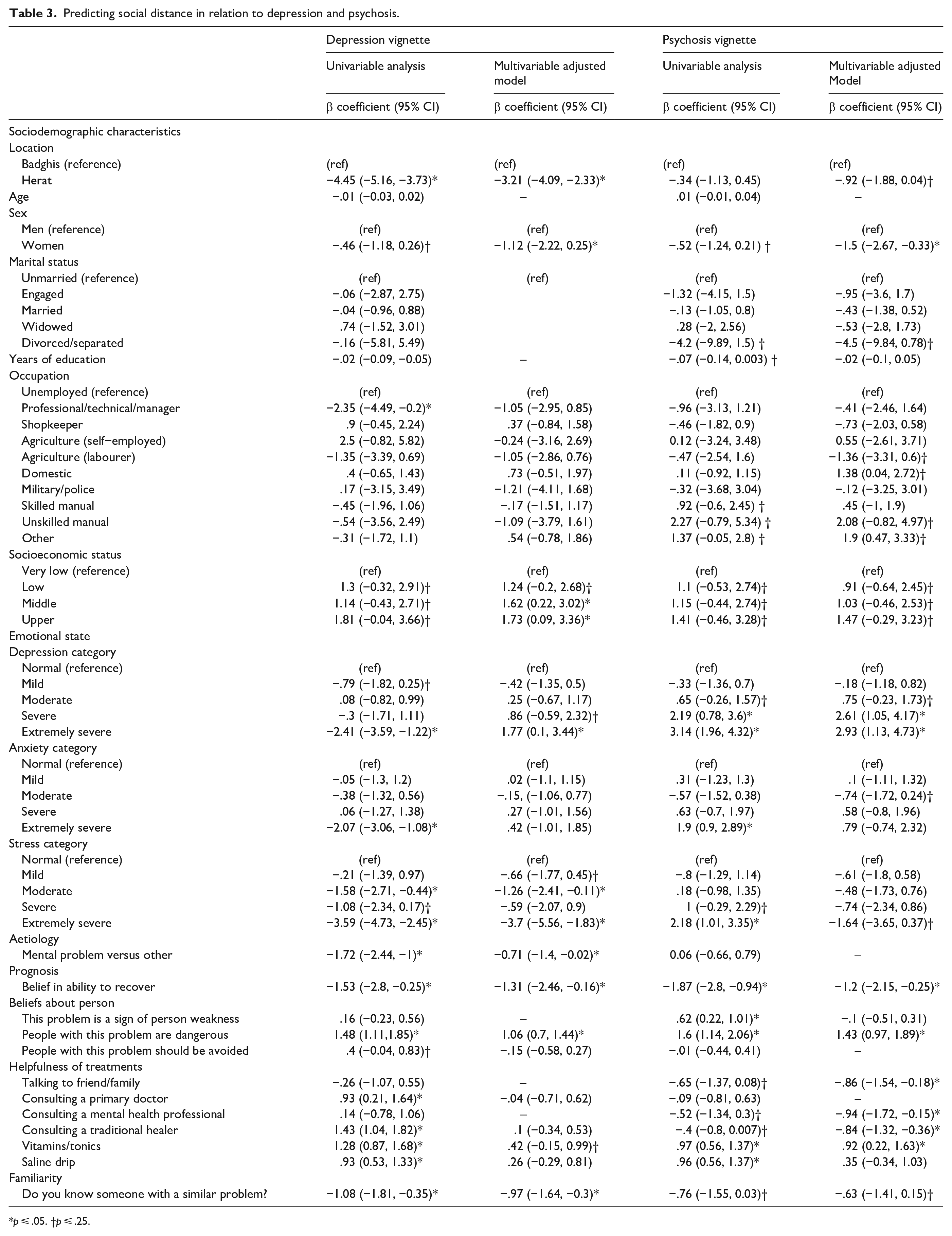
p ⩽ .05. †p ⩽ .25.
In the adjusted model for depression, people in Herat were more likely to have a lower preference for social distance from the person in the vignette. Women and persons with moderate or extremely severe stress were more likely to have a lower preference for social distance. Belief in the potential for recovery, describing the vignette as a ‘mental problem’ and familiarity were associated with slightly lower preference for social distance. Participants of higher socioeconomic status, those with severe depression, and those who believed the person in the vignette was dangerous, were more likely to have a greater preference for social distance.
In the adjusted model for the psychosis vignette, women were again more likely to have a lower preference for social distance. Belief in positive prognosis and in the helpfulness of talking to a friend, consulting a mental health professional and consulting a traditional healer, were associated with a slightly lower preference for social distance. Believing the person in the vignette was dangerous, having severe depression and believing in the helpfulness of vitamins/tonics were associated with a greater preference for social distance.
Univariable regression results are displayed in the first and third columns, and the multivariable adjusted models in the second and fourth columns.
Intended stigmatising behaviours in relation to mental illness
Table 4 shows results of linear regression for the outcome of intended stigmatising behaviours (RIBS) score and predictor variables being sociodemographics, emotional state, responses to statements about mental illness (representing general mental health literacy), and the composite stigma indicators of stereotype endorsement and benevolence scores. In the final model, being in Herat, believing that mentally ill persons can recover, and more benevolent attitudes were associated with a higher RIBS score (i.e. more willingness to engage in relationship). Increasing socioeconomic status and severe depression were associated with a lower willingness to engage in relationship. Univariable regression results are displayed in the first column, and the final multivariable adjusted model in the second column.
Predicting intended stigmatising behaviours in relation to mental illness.
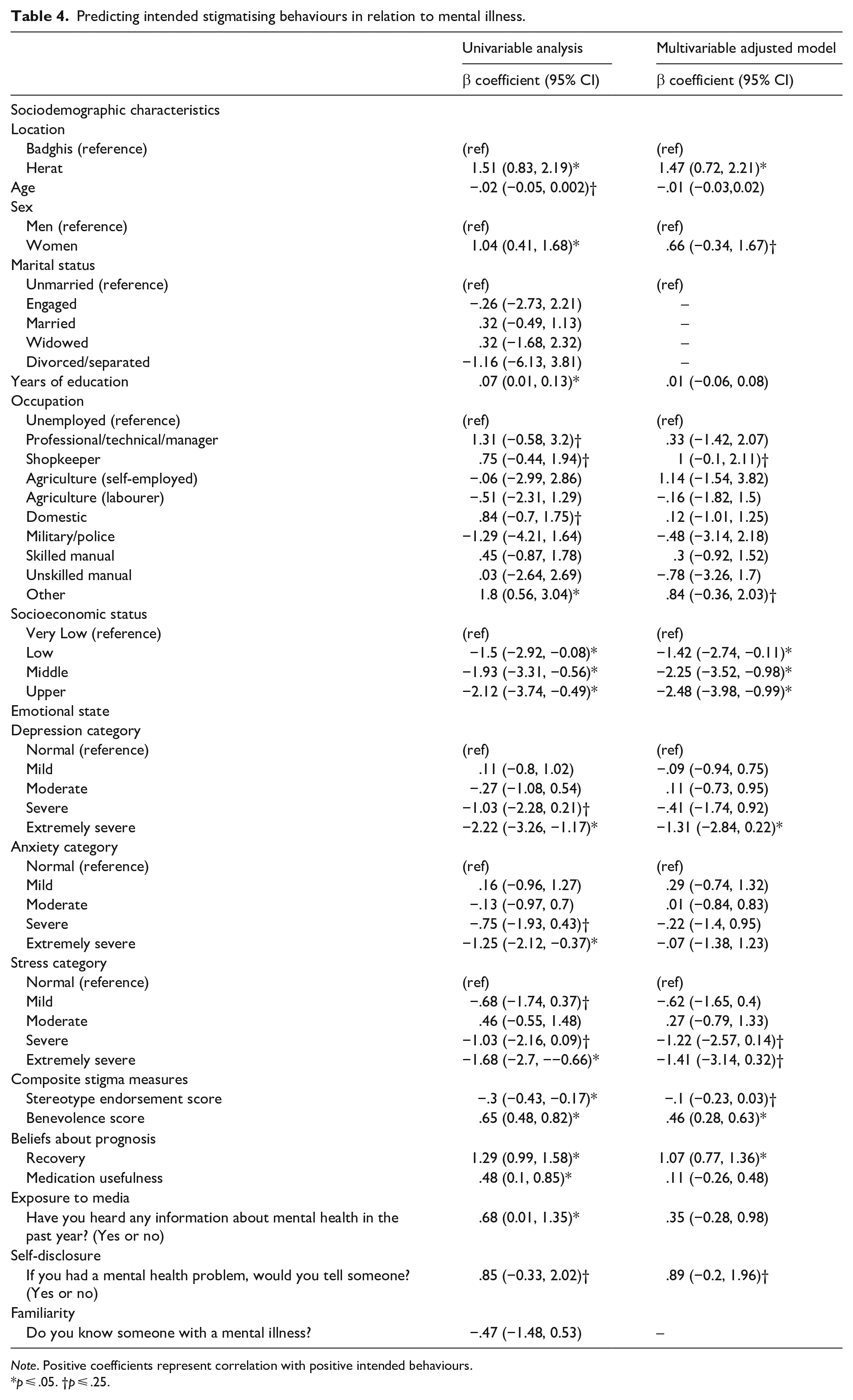
Note. Positive coefficients represent correlation with positive intended behaviours.
p ⩽ .05. †p ⩽ .25.
Discussion
This study explored the nature and patterns of mental health stigma among community members in Afghanistan; as represented by preference for social distance from persons with depression and psychosis, and intended stigmatising behaviours toward persons with mental illness generally.
Results highlighted significant discriminatory attitudes toward persons with depression and psychosis, with preference for social distance increasing as intimacy level increased. The most common stereotypes were that mentally ill people are dangerous and that they cannot marry. Following the ‘what matters most’ approach (Yang et al., 2007), work and marriage are important to address in anti-stigma programmes in this context, as these seemed to be the areas where even people with depression were most likely to be excluded. It is particularly important that anti-stigma programmes improve the possibilities for poorer women with mental illness to be able to marry, as they are among the most marginalised in the Afghan context. With regard to psychosis, it would seem important to promote beliefs in the ability of persons with psychosis to live good lives, as perceived by Afghan culture, and to target negative beliefs around dangerousness, also a common stereotype in other settings (Angermeyer et al., 2003, 2004; Corrigan et al., 2012; Kermode et al., 2009).
In comparing responses to the vignettes, to participants’ intended stigmatising behaviours toward persons with mental illness generally, the results showed particularly negative attitudes toward the label of mental illness (Dari = taklif-e rowani). For example, nearly half of participants said they would be willing to be a neighbour to the person in the psychosis vignette, but regarding intended behaviours toward mental illness generally, only a third of participants said they would be willing to ‘live near someone with mental illness’. While referring to conditions as mental illness may demonstrate greater mental health literacy (Rüsch et al., 2012), the label of mental illness can lead to more severe stigma (Angermeyer et al., 2003; Corrigan, 2004). One fruitful area of anti-stigma research and practice could be the development of local, context-appropriate descriptions of mental illness which could make discussion of these topics less stigmatising.
Nearly all participants reported they would share with someone if they had a mental health problem; however, only a small minority said that this would be to someone outside their family. This highlights the social dimensions of stigma and concerns about loss of ‘face’ (Ho, 1976) and reputation in the community. Programmes to increase mental health literacy for the general public (i.e. family members of persons with mental illness) are important, as their responses to disclosure are likely to meaningfully impact help-seeking (Tay et al., 2018).
Location was a key factor associated with social distance in relation to depression, with residents in Herat expressing a lower preference for social distance. It seemed the population of Herat is much more accepting of persons with depression, but this greater acceptance disappeared regarding psychosis. An effect of location was also present in relation to intended stigmatising behaviours; being in Herat, as compared to Badghis, was associated with more positive intended behaviours. This indicates that anti-stigma work might be especially needed in smaller, rural locations. This is in line with the current National Mental Health Strategy of Afghanistan (Government of Islamic Republic of Afghanistan: Ministry of Public Health, 2019) which prioritises the poorest and most remote areas of Afghanistan.
Women had a slightly lower preference for social distance in response to both vignettes, mirroring findings from other studies (Holzinger et al., 2012). If women are already marginalised, then the negative social impact of contact with persons with mental illness may be less. Holman (2015) has also suggested that this common finding could be related to an interaction between gender and social status or class.
There was a trend of increasing preference for social distance for the depression vignette with increasing socioeconomic status. This association was also found regarding intended stigmatising behaviours toward mental illness generally. This was an unexpected finding given that many studies have found the opposite association (Bhavsar et al., 2019; Cechnicki et al., 2011; Corrigan & Watson, 2007; Hansson et al., 2016; Robinson & Henderson, 2019; Wang et al., 2007), possibly due to lower education levels and less access to mental healthcare among those of lower socioeconomic status (Potts & Henderson, 2020).
A few studies, however, have found associations of increased stigma with high income (Alexander & Link, 2003; Martin et al., 2000; Venkatesh et al., 2015). Foster (2021) has suggested that those of higher socioeconomic status may hold more stigmatising views because they view mental illness as more controllable and therefore, mentally ill individuals are blamed for their illness.
It’s possible these dynamics are also at work in Afghanistan, but we would suggest an additional possibility, that the findings are related to reputation, honour culture and social status. The only other study from south Asia (India) to find a similar association also suggested this reason (Venkatesh et al., 2015). In a culture where economic opportunity is often tied to relationships and one’s social positioning and family honour (Eggerman & Panter-Brick, 2010), then we surmise that contact with persons with mental illness could be seen as more threatening to those in higher positions (in other words, they have more to lose by associating with mental illness). Social exclusion related to stigma has been suggested to have a greater impact on those of higher social standing and those from majority ethnic groups in Afghanistan, as they are more likely to be constrained by social expectations; and that rich and poor are equally affected by social exclusion in Afghanistan, in contrast to findings from other countries (Trani et al., 2016).
It would seem especially important that anti-stigma programmes understand and mitigate concerns around this social cost (loss of reputation and thus, loss of economic opportunity) of contact with persons with mental illness. Again, using the ‘what matters most’ approach (Yang et al., 2007), it would seem that this matters a great deal in Afghanistan. It is recommended that qualitative research be conducted into these topics. While some qualitative research in Afghanistan has focused on those who experience stigma (Allan et al., 2018), to our knowledge, a qualitative inquiry into attitudes of ‘stigmatisers’ and their reasons for holding stigmatising attitudes, has not been done.
This research could help identify what makes mental illness ‘dishonourable’ and reputation-damaging in the eyes of Afghans, and then address that in anti-stigma programmes. The relationship of gender to honour needs addressed in relevant ways, responding to intracultural variations across Afghanistan, especially in conservative rural areas. We also recommend that people from diverse socioeconomic backgrounds have the opportunity to contribute to policy decisions around mental health. Further research to confirm reputation and honour culture as a mediator of the relationship between socioeconomic status and stigma could also be conducted.
It was surprising that familiarity only predicted a slightly lower preference for social distance in the depression vignette. Contact with persons with mental illness is seen as an effective component of many anti-stigma interventions (Corrigan & Watson, 2002; Maunder & White, 2019). A pair of similar studies from another Islamic country, Turkey, also found no association between direct personal contact and decreased stigma (Arkar & Eker, 1994; Arkar et al., 2004). Given similar findings from Egypt (Coker, 2005), the reason for this could be that certain behaviours associated with mental illness are viewed as threats to community social cohesion in some cultures (Thornicroft, 2006). It is also reported that there are, in general, certain optimal conditions during which social contact is most effective in reducing prejudice (Pettigrew et al., 2011). The finding that familiarity only had a slight impact on preference for social distance possibly indicates that in Afghanistan, familiarity alone is not enough to reduce stigma, and further exploration is needed to better understand what specific type of social contact might be most effective. Future anti-stigma campaigns using contact (e.g. stories of lived experience of mental illness in the media), need ongoing evaluation to ensure stigma is actually reduced in the Afghan context. Anti-stigma educational programmes should also take the ongoing conflict into account, highlighting for community members that the prevalence of mental distress will be high and common in conflict settings, and that people should therefore be aware of mental health concerns and support help-seeking for those experiencing distress.
There was no evidence of association between social distance and views on the helpfulness of different treatments in the depression vignette. This suggests that depression might be seen as a normal life experience, related to financial or other stressors and not requiring any special therapeutic help (Roberts et al., 2020) – whereas for psychosis, participants had stronger opinions about what kinds of help are appropriate. Regarding psychosis, believing in the helpfulness of talking to a friend, and consulting either a mental health professional or traditional healer, all predicted a lower preference for social distance. On the other hand, believing that vitamins/tonics would be helpful predicted a greater preference for social distance. This perhaps indicates that if one believes an illness can be helped by talking to someone, it is seen as a more transient problem; whereas if a person needs to ingest medication, then the problem is seen to represent an inherent biological flaw. Other studies have shown the limitations of biological explanations for reducing stigma because it can increase beliefs that mental illness is a fundamental flaw (Angermeyer et al., 2003; Jorm & Oh, 2009; Kermode et al., 2009; Schomerus et al., 2012).
This discussion has highlighted key findings. Other associations with small effect sizes were also observed in inferential analyses, for example, stress in oneself was associated with decreased social distance in relation to the depression vignette; depression in oneself was associated with increased social distance (for both vignettes) and with more intended stigmatising behaviours. These findings regarding emotional state were inconclusive, but the consistent association with depression in oneself is noteworthy and could be further explored.
This study has many strengths. It reports on novel findings for this context regarding determinants of stigma, where issues around stigma and discrimination have thus far been underexplored. These findings are based on a large, representative sample for the context. These insights serve as a basis for further research and anti-stigma interventions in Afghanistan, and contribute to the literature on stigma within the field of global mental health through providing insights from a unique cultural setting. These findings do, however, need to be considered in view of some limitations. The survey tool contained a mixture of items taken ad hoc from a variety of validated measures. This presents challenges when comparing findings to other research. However, the data still provide important insights regarding stigma in this context. Also, responses to hypothetical vignettes only provide a proxy measure of discrimination and need validation against actual behaviour. However, this type of survey is an important first step before moving on to intervention studies.
In conclusion, this study provides much needed new insights on stigma to inform action in Afghanistan, a unique and under-researched context characterised by trauma and conflict, where mental health interventions (including those to reduce stigma) are especially critical. We hope this study provides value to decision makers in designing locally owned and culturally relevant anti-stigma campaigns.
Supplemental Material
sj-docx-1-isp-10.1177_00207640211036169 – Supplemental material for Mental health stigma among community members in Afghanistan: A cross-sectional survey
Supplemental material, sj-docx-1-isp-10.1177_00207640211036169 for Mental health stigma among community members in Afghanistan: A cross-sectional survey by Sean B Nine, Abdul Fattah Najm, Emily B Allan and Petra C Gronholm in International Journal of Social Psychiatry
Footnotes
Acknowledgements
IAM is grateful to Tearfund UK, TEAR Australia, MCCN and Digni for providing support to grow research capacity in Afghanistan. Tearfund UK and TEAR Australia support IAM’s work in mental health. The authors thank Said Javid Sadat, Ehsan Ahmad Ahmadzada and the team members at IAM who conducted data collection, and the participants who provided data for this study. Thanks to Kaaren Mathias for providing support with the idea and design, and to PRIME for sharing the survey format of this research. The authors also thank the King’s College London Biostatistics Advisory Service for advising regarding data analysis.
Author’s Note
Sean B Nine is now an Independent Scholar.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PCG is supported by the UK Medical Research Council in relation the Indigo Partnership [MR/R023697/1] award.
Data accessibility statement
The data that support the findings of this study are available on request from IAM. Consent was not sought to share data publicly.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.