
Abstract
Objective:
In psychosis, treatment often focuses on symptom reduction whereas social functioning is also essential. In this study, we investigate positive psychotic symptoms and medication use in relation to social functioning over a 3-year time-period in 531 patients diagnosed with psychosis. Furthermore, relations of positive symptoms with needs for care and quality of life were also investigated.
Method:
Using repeated measures analysis, changes were measured over time. Hereafter, mixed model analyses were performed to determine the associations of social functioning, needs for care, and quality of life with psychotic symptoms and patient characteristics. Finally, we assessed differences in symptoms and medication dose between those with an increase and those with a decrease in social functioning.
Results:
Patients significantly improved in social functioning, while psychotic symptoms increased. Improvement in social functioning was associated with younger age, higher IQ, and lower social functioning at T1, but not with positive symptoms. Also, improvement in social functioning was found to be related to a decrease in the dose of clozapine. Improvement in social functioning occurs despite worsening of positive symptoms.
Conclusions:
The findings suggest the need to further explore the relation between symptomatology, social functioning, and medication use. In the treatment of psychotic disorders, one should reconsider the strong focus on reducing psychotic symptoms. The current focus needs to shift much more toward improving functional outcome, especially when the patient expresses a desire for change in this respect.
Keywords
Introduction
Multiple studies suggest that the severity of psychotic symptoms is negatively related to overall functioning (Grau et al., 2016; Lee et al., 2019; Watson et al., 2018). In addition, both remission of negative symptoms and of positive symptoms were found to be contributors for better functioning in patients with a first-episode psychotic disorder (Jordan et al., 2014). This suggests that the course of the psychotic disorder and the patient’s functional outcome is improved by decreasing clinical symptoms.
Social functioning in particular was found to be affected by negative symptoms (Gerritsen et al., 2020; Hasan, 2019; Stouten et al., 2017; Strassnig et al., 2018), but positive symptoms are also known to affect social functioning (Heering & Van Haren, 2016). Moreover, the use of antipsychotics can hamper social functioning because of its (long-term) side-effects on for example physical health and social inclusion (McGorry et al., 2013; Murray et al., 2016; Tenback et al., 2012).
Besides symptom severity and medication use, several other factors are related to social functioning of patients with a psychotic disorder. It has widely been reported that an overall better social functioning is related to a decrease in number of hospital admissions, less outpatient visits, and more social engagement (Bellido-Zanin et al., 2015). Also, studies in early onset psychosis show that social functioning and patient’s quality of life both improve despite the presence of psychotic symptoms (Albert et al., 2011; Garety et al., 2006). Interestingly, in 177 patients with chronic psychosis no relation between symptomatic remission and functional recovery was found by Oorschot et al. (2012), who therefore suggested that the main focus on symptomatic remission should be re-considered.
Thus, previous studies do not show a consistent relation between psychotic symptoms and social functioning. The aim of this research is to contribute to the enhancement of treatment in clinical practice. Treatment of psychotic disorders mainly focuses on positive symptoms. Therefore, the aim of the present study is to further investigate the relation between positive symptoms (i.e. hallucinations, delusions, thought disorder), antipsychotic medication, and social functioning in a Dutch cohort of patients with a psychotic disorder, over a 3-year period. Medication is prescribed mainly for positive symptoms. It is hypothesized that social improvement occurs despite the presence of persistently high positive symptoms. Also, a negative relation between social functioning and the use of antipsychotics is expected. Additionally, in order to be able to make statements about a broader definition of functioning as well, associations of psychotic symptoms with quality of life and needs for care were investigated. Furthermore, clinical characteristics of patients who improved were compared to those of whom deteriorated in social functioning.
Methods
Patient and data selection
This study uses a subsample of data from the Genetic Risk and Outcome of Psychosis (GROUP) study. GROUP is a naturalistic follow-up study in 1,119 patients diagnosed within the psychotic spectrum, 1059 siblings, 920 parents, and 586 unrelated control subjects. Measurements of the GROUP study were collected at baseline and at 3- and 6-year follow-up (T1 and T2). A detailed description of the study is available elsewhere (Korver et al., 2012).
For the current study, data from the 3- and 6-year follow-up were used, given that social functioning was not measured at T0. Patients were included if they were diagnosed with a psychotic disorder and if data regarding the severity of psychotic symptoms were available at both time points (N = 531).
Measures
Severity of psychotic symptoms was measured by the Positive and Negative Syndrome Scale (PANSS; Kay et al., 1987), which assesses the core symptoms of schizophrenia. The PANSS is a semi-structured interview whereby items are rated on a seven-point scale (1 = absent to 7 = extremely severe) over the past week. For this study, items that represent positive symptoms were included. Positive symptom items were grouped according to the 5-factor model as developed by Van der Gaag et al. (2006); delusions, hallucinations, unusual thought content, suspiciousness, grandiosity, somatic concern, lack of judgment and insight, active social avoidance, difficulty in abstraction; total score ranges from 9 to 63.
The level of social functioning was assessed by the Social Functioning Scale (Birchwood et al., 1990). The SFS consists of 76 items, assigned to the following seven subscales: social engagement/withdrawal, relationships, social activities, recreational activities, independence-competent, independence-performance, and employment/occupation. Four items are dichotomous questions, 1 item records the time of getting up, 1 item is rated on a three-point Likert scale, 2 items are rated on a five-point Likert scale, and 68 items are rated on a four-point Likert scale (total score ranges from 55 to 135). A higher score indicates better social functioning.
Quality of life was measured with the WHOQOL-BREF (World Health Organization Quality of Life-Bref; Whoqol Group, 1998). This self-report scale assesses quality of life on four major domains (physical health, psychological health, social relationships, and environmental conditions). The total mean score was used (range 1–5). Higher scores indicate a higher perceived quality of life.
The Dutch 24-item version of the Camberwell Assessment of Need Short Appraisal Schedule (CANSAS; Delespaul et al., 2008; Phelan et al., 1995) was used to assess individual needs for care. Each item was scored 0 (no need), 1 (met need), or 2 (unmet need). Higher scores indicate a higher need for care.
Furthermore, a number of demographic and clinical data were used: age, gender, ethnicity, educational level, employment status, IQ, global assessment of functioning (GAF; American Psychiatric Association, 2000), age of onset of first psychotic episode, duration of psychotic illness, number of psychotic episodes, diagnoses, and antipsychotic medication use.
Statistical analyses
Release 6.0 of the GROUP database was used for the analyses, and all data were analyzed with IBM SPSS Statistics 22. Data from two measuring points were used, 3 (T1) and 6 (T2) years after entering the GROUP study. First, using repeated measures ANOVA, scores over time were compared for positive symptoms, social functioning, needs for care, and quality of life, while controlling for T1. Hereafter, the relation of psychotic symptoms with social functioning, needs for care and quality of life and was analyzed by mixed model analyses with the positive symptom score as predictor variable and subject identifier as random and patient characteristics as fixed effects (gender male/female, employment yes/no, using antipsychotics yes/no), as previous studies suggest these factors are related to functioning (Jaracz et al., 2007; Schennach et al., 2012; Valencia et al., 2015).
Finally, based on the change in total scores over time, subjects were divided into two groups, those with an increase and those with a decrease in social functioning. One patient was excluded, since equal scores for social functioning for T1 and T2 were reported. Patient characteristics were compared to investigate if these differed between groups. In addition, change in social functioning (decrease or increase) was investigated in relation to the dose of antipsychotics. For analyses regarding the specific type and dose of antipsychotics, only the top four most prescribed antipsychotics for patients in this study were used (risperidone, olanzapine, quetiapine, clozapine). Independent T-Tests were performed for comparing continuous variables, chi-square tests were performed for dichotomous variables.
Results
Patient characteristics
Five hundred and thirty-one patients of T1 were included in the study, of which 77% were male with a mean age of 30.7 (SD = 7.3) years old, and an IQ of 99.8 (SD = 16.3). Mean illness duration was 8.3 (SD = 4.2) years, with the onset of the first psychosis at the age of 22.6 (SD = 6.7). The results are shown in Table 1.
Demographics and clinical characteristics and functional outcome after 3 (T1) and 6 years (T2) of the GROUP study (N = 531).
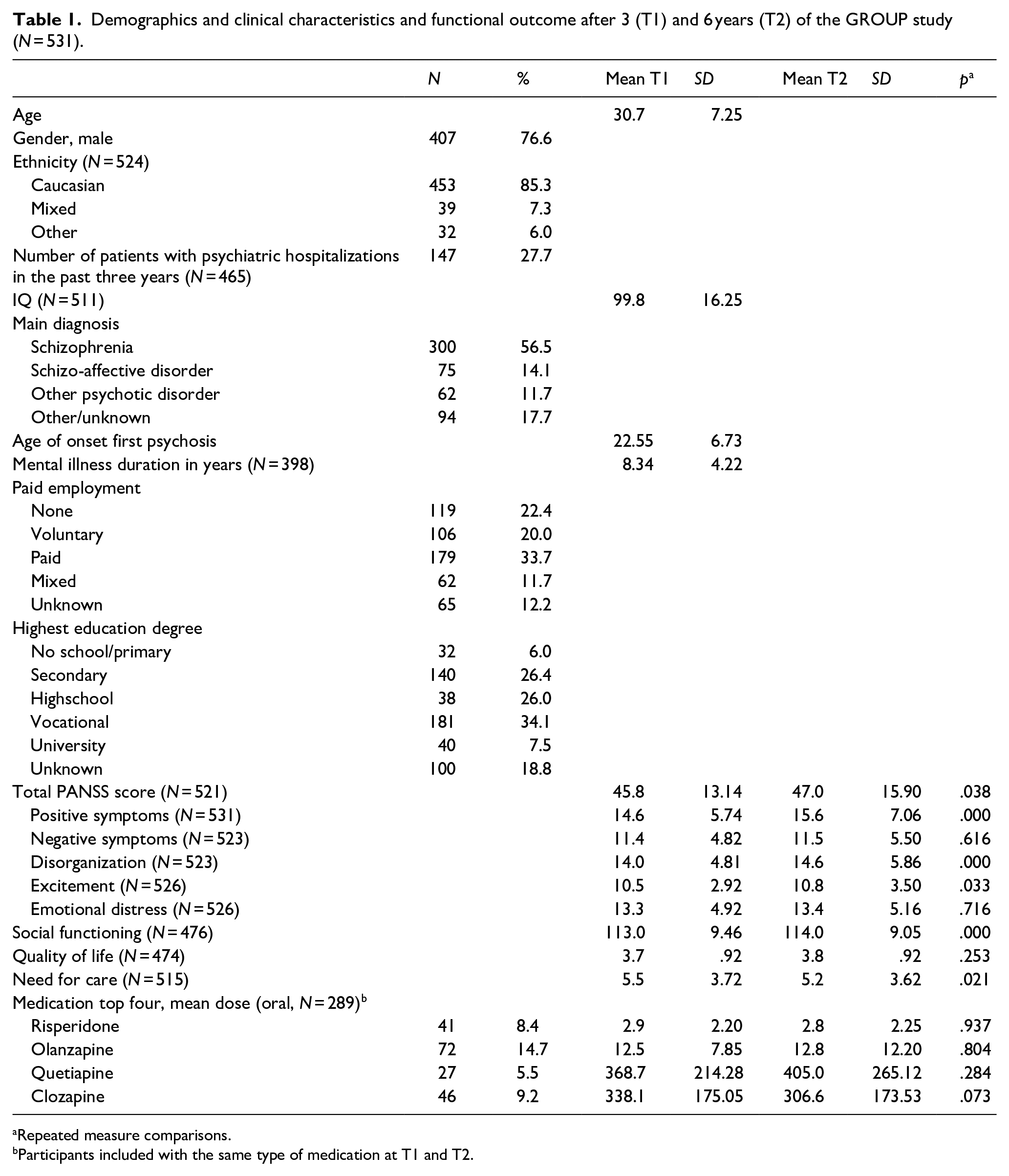
Repeated measure comparisons.
Participants included with the same type of medication at T1 and T2.
Clinical and functional differences between T1 and T2
Psychotic symptoms, social functioning, needs for care, and quality of life were compared for T1 and T2. As shown in Table 1, patients experience significant more overall psychotic symptoms, positive symptoms, disorganization, and excitement at T2 compared to T1.
In contrary to the worsening of psychotic symptoms, a small but significant improvement was found in social functioning. In particular, better functioning was found for the subscales employment/occupation (mean difference = 2.6, SD = 11.9, p < .000), social engagement/withdrawal (mean difference = 1.1, SD = 10.4, p = .026), recreation (mean difference = 1.89, SD = 13.0, p = .002), and independence-performance (mean difference = 1.9, SD = 9.64, p < .000).
The total number of needs for care decreased (mean difference = 0.3, SD = 3.8, p = .021). However, unmet needs increased. At T2, more unmet needs were reported for psychotic symptoms (χ2 = 53.1, p < .000), medication side effects (χ2 = 21.4, p = .042), and personal hygiene (χ2 = 28.4, p < .000).
Use of antipsychotics
A large group of the patients (93%) used antipsychotics prior to inclusion; 7% of the patients did not use antipsychotic medication or medication use was unknown. Most patients used risperidone (32.7%), olanzapine (30.4%), clozapine (11.8%), or quetiapine (10.5%), primarily in oral form (N = 392). Depot medication was used by 45 (9.1%) patients. Of all patients, 446 used medication at T1 and T2, of which 289 used the same medication at both time-points. Although no significant differences were found regarding the medication dose between T1 and T2 (T1: M = 125.6, SD = 196.2, T2: M = 123.3, SD = 202.8, N = 213, p = .685), or medication type, a trend was found for a decrease in clozapine dose. Results of the top four medication used are shown in Table 1.
Relation between positive symptoms functional outcome
In the mixed model analyses, while controlling for gender, employment, and use of antipsychotics, positive symptoms (based on the PANSS) were significantly associated with social functioning, needs for care, and quality of life. Nevertheless, the control variables were also significantly associated with the social outcome measures (see Table 2 for all results).
Association of positive symptoms and patient characteristics with functional outcome.
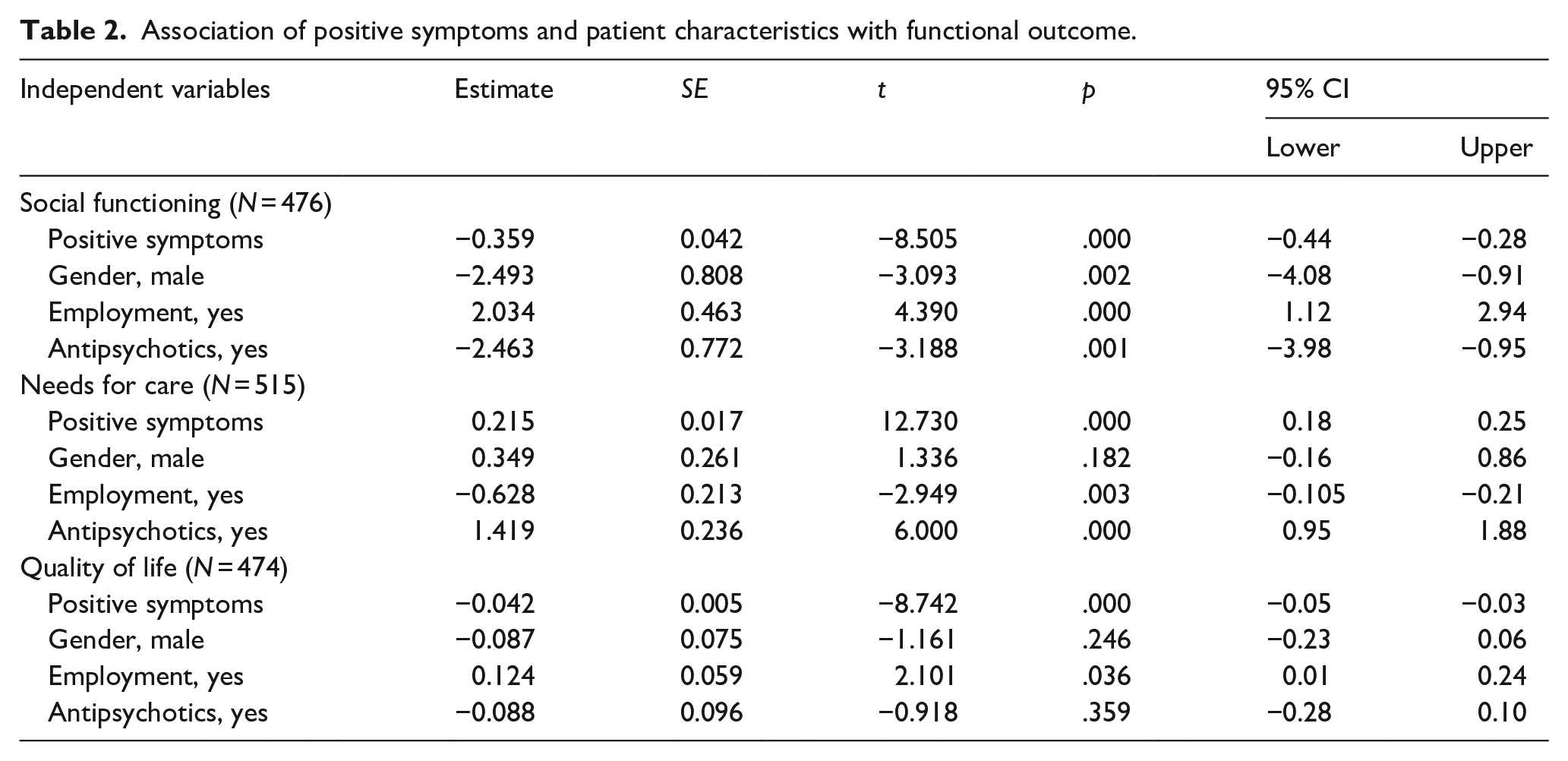
Compared to the control variables, the association between positive symptoms and social functioning is relatively small. For example, having employment at T1, is associated with a higher social functioning score of approximately two points (a change of 2.5% on the SFS-scale). In our sample, 241 (50.6%) patients had voluntarily or paid employment during both time points, and another 98 patients obtained employment (information on social functioning was missing for 81 patients). However, a higher social functioning score of two points is associated with a decrease in positive symptoms of about six points, which equals a change of 10.7% of the positive symptom scale of the PANSS. In our sample, this change was seen only in 7.8% of the patients. Furthermore, a change of 25 points (44.6%) in the positive symptom scale is associated with improving quality of life by one point. In our sample, this was only the case for one patient. Thus, considering the small association, a large improvement in psychotic symptoms is needed for a change in functional outcome.
Social functioning, improvement versus deterioration
Based on change in social functioning between T1 and T2, patients were divided into two groups: those who improved (N = 205) and those who deteriorated (N = 207). Comparisons were made for the following variables at T1: age, gender, ethnicity, IQ, illness duration, GAF, positive symptoms, and use of antipsychotics, all factors known to influence social functioning. Improvement in social functioning was observed in 57% of the patients. Those who improved showed a lower mean score (M = 110.8, SD = 9.7) in social functioning at inclusion compared to those who deteriorated (M = 115.9, SD = 8.4; t(473) = −5.974, p < .000). Also, they were younger and had a higher IQ compared to those who did not improve.
Change in social functioning was not related to the use of antipsychotic medication, the cumulative dose of medication at T1, or an increase or reduction in medication over time (see Table 3 for all outcomes). However, patients who improved in social functioning had a lower prescribed dose of clozapine over time (N = 24; T1 M = 368.8, SD = 178.50; T2 M = 320.8, SD = 190.35, p = .040). No differences over time were found for change in social functioning in relation to the other types of antipsychotics.
Demographic variables at T1 and change in social functioning (deteriorated vs. improved).
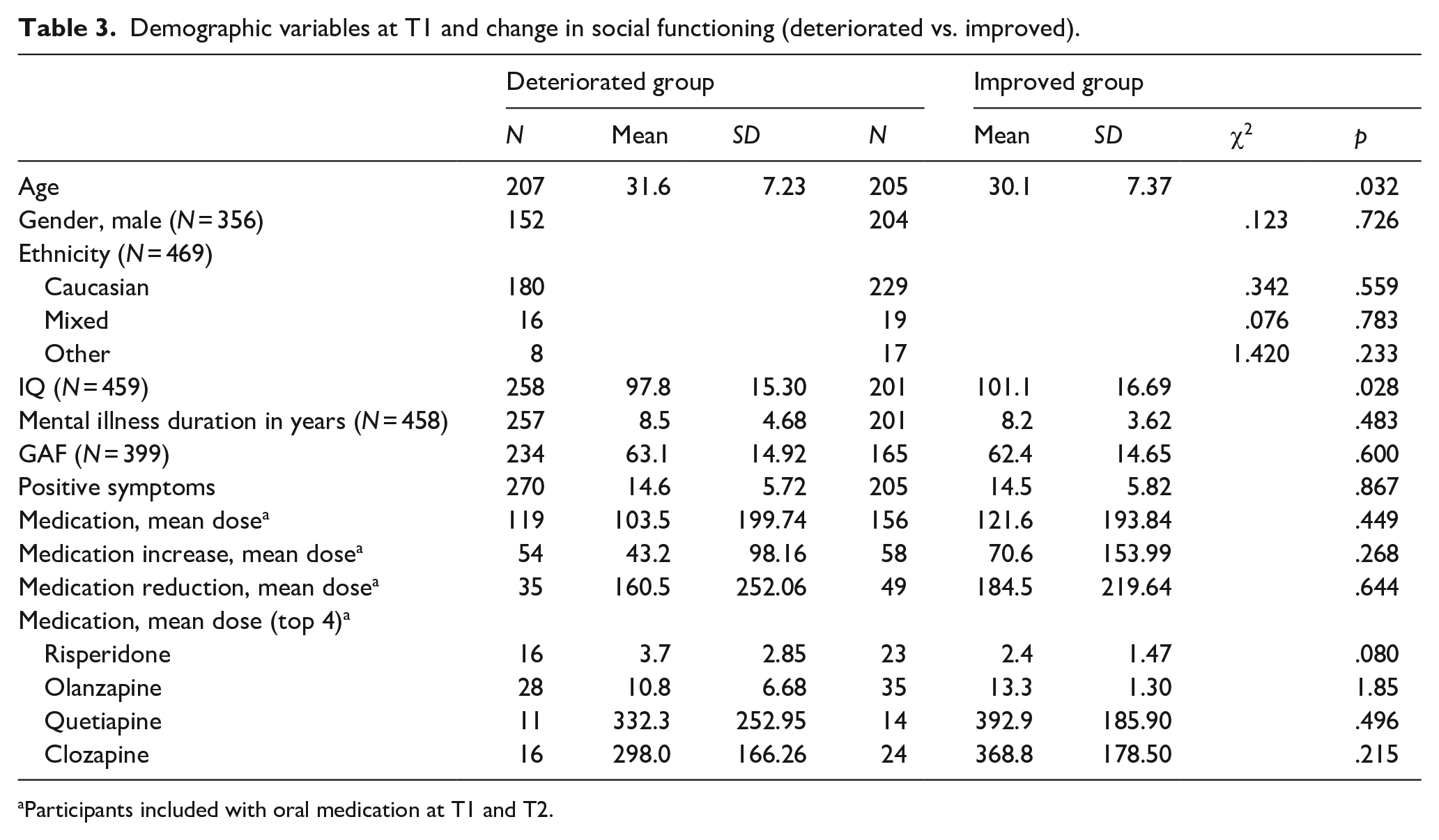
Participants included with oral medication at T1 and T2.
Discussion
This present study shows that the contribution of positive symptoms is limited in relation to social functioning, needs for care, and quality of life. Patients experienced more positive symptoms over time, whereas social functioning slightly improved, and quality of life and needs for care did not significantly change. Moreover, patients whose social functioning improved were taking a lower dose of clozapine over time. These findings suggest the need to further explore the relation between symptomatology, social functioning, and medication use, as it is possible that the current focus to reduce clinical symptoms in psychiatry needs to shift much more toward improving functional outcome. It indicates more complex relationships between the three areas. Additional qualitative research could provide even better insight into how symptoms, functioning, and medication may be related.
Our findings are consistent with studies in which no clear association between positive symptoms and social functioning was found (Albert et al., 2011; Cacciotti-Saija et al., 2018; Carrión et al., 2016; Oorschot et al., 2012). In addition, a likewise association was also found in a previous study with the GROUP data (Simons et al., 2016), which explored the relation between the positive symptom score at baseline and social functioning at T1 (B = −2.97, 95% CI [−3.86, −2.080], p < .01). Furthermore, in the present study the found associations were relatively weak compared to employment (yes/no), gender, and use of antipsychotics (yes/no), which are also known to affect social functioning. The inconsistencies with studies that report a strong relation between social functioning and psychotic symptoms (Erol et al., 2009; Startup et al., 2010) could be explained by the use of different rating scales, research designs, duration of psychosis, and a shorter follow-up period (6–24 months).
The finding that positive symptoms increase over time is also found in a study of Górna et al. (2014). They found that psychotic symptoms decreased after 13 months but increased at follow-up 8 years later. The increase of psychotic symptoms in chronic patients could be explained by patients being less well monitored and treated by mental health care providers over time as compared to an acute phase of the disease, but also by the progressive nature of the disease (Van Haren et al., 2016). Moreover, clinicians and patients might look for an optimum balance between effects and side-effects of medication in order to prevent medication discontinuation.
In our study, we found better social functioning with less clozapine over time, but with increasing psychotic symptoms. These findings need to be interpreted with care, but others have also suggested that functional outcome is better with less medication. Wunderink et al. (2013) were the first to report that after dose reduction/discontinuation of antipsychotics in a 7-year follow-up study social functioning improved. Also, dosages of antipsychotic medication that are used for the maintenance treatment of psychotic disorders may be too high, as suggested by the findings of Read and Sacia (2020). They found that 57.5% of 650 users of antipsychotics had only negative experiences using medication. This was mainly caused by the side effects. To gain more insight into the effects of antipsychotics on personal and social functioning, psychotic symptom severity, and health-related quality of life, the HAMLETT study has been set up (Begemann et al., 2020). Hopefully, this study will shed more light on the relation between social functioning, symptomatology, and medication continuation and dose. An explanation for not finding relations with other antipsychotics in the current study may be caused by a lack of power. Also, medication side effects may be of interest here, since clozapine has more serious side effects that interfere with social functioning (De Berardis et al., 2018; McEvoy et al., 2006).
Furthermore, we examined if clinical characteristics differed between patients who improved compared to those who deteriorated in social functioning. Fifty-seven percent of the patients improved in social functioning. This was related to worse social functioning at inclusion, younger age, and higher IQ at baseline and in line with other studies that found younger age was associated with better outcome in social functioning in patients with schizophrenia (Martin et al., 2015), and higher IQ associated with better social functioning through time (Leeson et al., 2009). Also, no relation was found for improved/deteriorated social functioning and change in the positive symptoms scale.
In this present study, we did not find a relation of social functioning with illness duration, gender, ethnicity, GAF, and medication dose. Although associations between GAF and SFS are found in previous research, the SFS measures different aspects of social functioning and is less influenced by clinical symptoms (Hellvin et al., 2010). Contrary to other studies (Thorup et al., 2007; Vila-Rodriguez et al., 2011), we did not find gender differences. This may be caused by differences in populations. In our subjects, men are in the vast majority (77%). The same accounts for ethnicity, where 87% of the patients are Caucasian. Also, we found no differences in dose of antipsychotics, but this can again be explained by limited power.
Strengths and limitations
This study has several strengths and limitations. The main strength is the use of a large verified longitudinal dataset with extensive phenotyping. Data from a large number of patients were available over a 3-year time period. By using the mixed model method, within each patient, it was possible to account for the variation over time and missing data. Another strength is the use of the positive symptom category according to the 5-factor model (Van der Gaag et al., 2006). Five-factor models are thought to be more representative of the syndromes than the original subscales of the PANSS (Jerrell & Hrisko, 2013). Thus, by using the positive symptom scale following the 5-factormodel, we can assume that we measured what we intended to measure – that is psychotic symptoms.
There are also some limitations. First, not all measures were obtained at enrollment in the GROUP project and therefore, this present study could not examine the relation between psychotic symptoms and functional outcome between T0 and T1. Measures obtained at the start of the GROUP project would have provided additional information on the change in social functioning and the associations with psychotic symptoms, in particular during the early course of the disease. Second, patients had a relatively high IQ, which could represent a selection bias with patients with a lower IQ dropping out during the follow-up of the GROUP project. However, previous research with data from the GROUP project found a relatively high estimated IQ of 94.9 at baseline (Meijer et al., 2012), indicating that the overall level of intelligence was relatively high from the start. Third, a relatively small number of data was available regarding the type and dose of antipsychotics. Although medication use (yes/no) at T1 and T2 was known for 84% of the patients type and dose of medication was only known in 55% of the cases. Nevertheless, to our knowledge, this is the first study that has examined the relation between clozapine dose reduction and social functioning.
Conclusions
Positive symptoms were associated with social functioning. However, this effect was relatively small and improvement in social functioning occurred despite a worsening of positive symptoms. This suggests that a reduction of positive symptoms is only partly related to social functioning, and that optimizing medication (effects vs. side-effects) is needed to find the right balance between the two. In mental healthcare one should reconsider whether a strong focus on symptom reduction warrants the attention it gets in daily practice. Further research is needed to examine the use, type, and dosage of antipsychotics and its relationship with symptomatology and social functioning.
Footnotes
Acknowledgements
We are grateful for the generosity of time and effort by the patients, their families, and healthy subjects. Furthermore, we would like to thank all research personnel involved in the GROUP project, in particular Joyce van Baaren.
Conflict of interest
The authors declare that there is no conflicts of interest with respect to this study. All authors approved the manuscript in its current form.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The infrastructure for the GROUP study is funded through the Geestkracht programme of the Dutch Health Research Council (Zon-Mw, grant number 10-000-1001), matching funds from participating pharmaceutical companies (Lundbeck, AstraZeneca, Eli Lilly, Janssen Cilag), and universities and mental healthcare organizations (Amsterdam: Academic Psychiatric Centre of the Academic Medical Center and the mental health institutions): GGZ Ingeest, Arkin, Dijk en Duin, GGZ Rivierduinen, Erasmus Medical Centre, GGZ Noord Holland Noord. Groningen: University Medical Center Groningen and the mental health institutions: Lentis, GGZ Friesland, GGZ Drenthe, Dimence, Mediant, GGNet Warnsveld, Yulius Dordrecht, and Parnassia psycho-medical center The Hague. Maastricht: Maastricht University Medical Centre and the mental health institutions: GGZ Eindhoven en De Kempen, GGZ Breburg, GGZ Oost-Brabant, Vincent van Gogh voor Geestelijke Gezondheid, Mondriaan, Virenze riagg, Zuyderland GGZ, MET ggz, Universitair Centrum Sint-Jozef Kortenberg, CAPRI University of Antwerp, PC Ziekeren Sint-Truiden, PZ Sancta Maria Sint-Truiden, GGZ Overpelt, OPZ Rekem. Utrecht: University Medical Center Utrecht and the mental health institutions: Altrecht, GGZ Centraal, and Delta.