
Abstract
Background:
Family interventions (FI) for schizophrenia were primarily developed and practised in the West. It has been proven that cultural adaptation for FI facilitates its uptake and improves therapy outcomes; however, the majority of literature on the development of FI focussed on outpatient or community settings, and little attention has been paid to in-patient units. There is an opportunity to engage with the family during admission, particularly in Asia.
Aims:
To explore relatives’ and mental health professionals’ views and opinions to inform the cultural adaptation of FI for hospitalised patients with schizophrenia in Oman. It also aimed to gain consensus on items that need adaptation.
Methods:
We conducted semi-structured interviews with the caregivers (n = 20) and two separate focus groups with psychiatrists (n = 7) and nurses (n = 5). Another consensus group was a mix of both (n = 6) to develop agreement and solve discrepant issues. The data were analysed using framework analysis to identify the intervention components and delivery system.
Results:
Modifications to existing components indicated that the cultural adaption of the intervention focussed more on themes such as religious and spiritual causes of mental illness, simplified language, format of delivery as individual sessions and culturally relevant and acceptable problem solving and coping skills. The components of the intervention identified as psychoeducation, problem-solving and emotional support. The consensus group finalised the intervention’s content and delivery system concerning training needs and issues and barriers to implementation. The proposed culturally adapted FI for hospitalised patients requires a flexible approach to meet the family’s needs.
Conclusions:
The findings of the study indicated that FI is an acceptable and feasible approach to be delivered during hospitalisation. The intervention will be accompanied with an intervention manual, which will be tested in a future feasibility study.
Keywords
Introduction
Family interventions (FI) have been found effective in treating individuals diagnosed with schizophrenia and reducing family burden (NCCMH et al., 2014; Pharoah et al., 2010). However, the evidence to support their effectiveness in the Arab world is still emerging (Al-Sawafi et al., 2020). FIs were developed in the West, and cultural adaptation is recommended for application in non-Western cultures (Degnan et al., 2018; Hall et al., 2016; Maura & Weisman de Mamani, 2017). Cultural adaptation is ‘the systematic modification of evidence-based treatment or intervention protocols to consider language, culture and the context in such a way that is compatible with clients’ cultural patterns, meanings and values’ (Bernal et al., 2009).
Each distinct culture provides an explanation of the aetiology and treatment of different illnesses, and shapes the experience of its individuals (Helman, 1984). Therefore, culture is a powerful environmental factor that can significantly affect the course of schizophrenia (Edgerton & Cohen, 1994). Our recent systematic review of psychosocial FIs for relatives of people diagnosed with psychotic disorders in the Arab world found that numerous cultural adjustments are required to improve intervention accessibility and acceptability (Al-Sawafi et al., 2020).
The culture of Oman is steeped in the Islamic religion, tribal organisation and Arabic language and culture. The Omani society is a collective society that values group harmony, and family values override individual needs (Al-Adawi, 2017). In Oman, individuals with mental illness usually reside with their families outside the healthcare system and families are actively involved in their care because of lack of any mental health community services. Families are expected to manage the situation at home despite their lack of basic knowledge and skills.
In Oman, psychiatric treatment is heavily reliant on psychotropic medications, with limited or no focus on psychological or FIs because of many barriers such as lack of resources, stigma and lack of adaptation to Omani culture (Al-Adawi, 2017). However, there is an ideal opportunity to develop and provide FI in one of the tertiary hospitals where the admission policy requires the attendance of a relative with the patient throughout the admission time (Al-Adawi, 2017). The opportunity of having the relative with the patient provided us with a starting point to develop FI in Oman despite the fact that it will be difficult to engage patients because of potential disturbance to them.
Previous studies interviewed carers, patients and health professionals to inform the cultural adaptation of psychosocial interventions in Egypt, China, Pakistan and minority populations in the UK (Edge & Grey, 2018; Hackethal et al., 2013; Li et al., 2017; Naeem et al., 2016; Rathod et al., 2010; Wahid, 2009). However, little attention has been paid in the literature to the development of FIs in the inpatient units. In Western countries, inpatient settings only form a small part of the health care provision for people with schizophrenia and much more of the focus is on community care. Furthermore, in the West the admission length was getting shorter, making it unclear what could be offered to families in such a short time (Lobban & Barrowclough, 2009). However, in non-Western cultures, where community care is limited and much of the treatment is administered in an inpatient setting, there is a need to develop FI during hospitalisation. As the culture of providing FI is new for patients, their families and mental health professionals in Oman, the authors chose to start with the inpatients setting to develop the intervention and then expand it to the outpatient once it proved its effectiveness. Relatives of hospitalised patients usually experience a high level of distress, and their experience could be traumatic (Jagannathan et al., 2010). They usually face enormous pressure before admission and have to deal with the disturbing experiences of their relative (Lobban & Barrowclough, 2009).
The development of the intervention started with a systematic review of culturally adapted FI in the Arab world, which indicated limited evidence in this area (Al-Sawafi et al., 2020). The second stage explored the experience of Omani relatives of hospitalised individuals diagnosed with schizophrenia and the findings indicated that families experienced significant burden, stigma, violence and lack of knowledge and may benefit from FI (Al-Sawafi et al., 2021). However, the findings revealed that further exploration of relatives’ preference regarding the content and delivery of the intervention is required. Furthermore, inpatient staff, including nurses and psychiatrists, have a key role in the delivery of FIs and their views should also be explored before developing the intervention. Therefore, this qualitative study aimed to explore relatives’ and mental health professionals’ views and opinions to identify cultural aspects and modifications to FI for hospitalised patients with schizophrenia in Oman. It also aimed to gain consensus on items that need adaptation.
Study design
This qualitative study consisted of individual semi-structured, in-depth interviews with carers and focus groups with mental health professionals.
The interview with carers explored their views about the content of the intervention and their preference about the format and mode of delivery. Individual interviews were considered the most suitable for carers due to the sensitive nature of mental illness stigma, while focus groups were more appropriate for mental health professionals because they allowed for clarification and exploration of the practicalities of intervention delivery with a range of participants at the same time (Krueger & Casey, 2009).
The topic guide for interviews was developed from the literature and the systematic review and involved input from three family members and five mental health professionals working at the psychiatric unit (see Supplementary Material). The interview explored caregivers’ beliefs about the illness’s causes and treatments, the intervention’s content and their preference about the format and mode of delivery.
The two focus groups with nurses and psychiatrists discussed the practicalities of intervention delivery. As these two focus groups included either nurses or psychiatrists, another consensus group was a mix of both, to maximise exploration and final thoughts about the items that need adaptation and to develop agreement and solve discrepant issues. Consensus was achieved once all participants agreed on each issue.
The topic guide for focus groups was developed according to the results from other studies conducted by the research team and commenced with an overview of the findings from the previous stages, mainly concerning the components of the intervention (systematic reviews and interviews with caregivers). Then, a dialogue was generated about the facilitators, barriers and delivery system of the intervention with regard to how it could potentially be delivered, by whom and when and whether any training is required and how it could be implemented (see Supplementary Material).
Ethical consideration
Ethical approval was obtained from the University of Manchester Research Ethics Committee (Ref: 2019-5038-9106) and Sultan Qaboos University Hospital Medical Research Ethics Committee (REF.NO.SQU-EU/085L19). The author obtained informed consent and maintained participants’ privacy and confidentiality at all times.
Study participants and their selection
Participants were recruited from the psychiatry inpatient unit at a tertiary care hospital in Oman. A purposive sampling method was used to recruit participants for interviews and focus groups.
Inclusion and exclusion criteria for interviews
- Adult family members of hospitalised patients living with the patients who had been taking care of patients at home for a minimum period of 1 month. The admission policy at this unit requires patients to be admitted with a carer.
- The study excluded family members not living with the patient or any paid caretaker.
Recruitment for interview
Caregivers were provided with the participant information sheet by hospital staff and if they expressed an interest, they met the researcher for clarification and signing consent.
Inclusion and exclusion criteria for focus groups
- All nurses and psychiatrists with a minimum of 6 months experience in the unit. Psychologists were approached but refused to participate due to shortage of staff.
- The study excluded new professionals with less than 6 months experience.
Recruitment for focus groups
The researcher first provided a brief explanation of the study at the morning meeting for both nurses and psychiatrists. Next, they were invited by email from the hospital administration to participate in focus groups. The researcher contacted those who agreed to arrange the time and place of focus groups.
Data collection
The lead author (A) conducted the interviews in Arabic with caregivers, whereas focus groups with mental health professionals were conducted in English because it is the official language used in teaching and documentation.
Data analysis
The data were analysed using framework analysis as the study’s objectives are typically set in advance (Gale et al., 2013; Ritchie & Lewis, 2014). Framework analysis includes the stages of familiarisation; developing a thematic framework; indexing; charting; mapping; and interpretation. NVivo, a computer-assisted qualitative data analysis software, was used to assist with data management and analysis.
The interviews and focus groups were analysed separately and then synthesised together. The recorded interviews and focus groups were transcribed verbatim and then translated into English by the primary investigator, who is bilingual. The first author analysed the data and developed a coding framework of themes. The transcripts were read by two members of the study team (K.L. and N.H.), who agreed with the coding and the framework. Any discrepancies were discussed with the research team to reach a consensus. The data were then charted into the framework matrix using Microsoft Excel to reduce the data into manageable text sections that can be easily visualised. The final step included relating each theme to another to make sense of the data and provide a schematic diagram of the phenomena, leading to the final list of themes.
Rigour
The study followed Lincoln and Guba’s (1986) principles for trustworthiness. Credibility was enhanced by matching the research question with the method and analytic process and providing detailed documentation of analysing and reporting. Transferability was facilitated by providing a thick description of the context, participants, collection procedure and appropriate quotation (Lincoln & Guba, 1986). Dependability was met by holding frequent debriefing sessions with the study team to check the coding, reflect on the experience, recognise any preconceptions or bias and maintain journals that explicated all methodological decisions. Conformability was maintained by means of audit trail and reflexivity.
Results
Participants’ characteristics
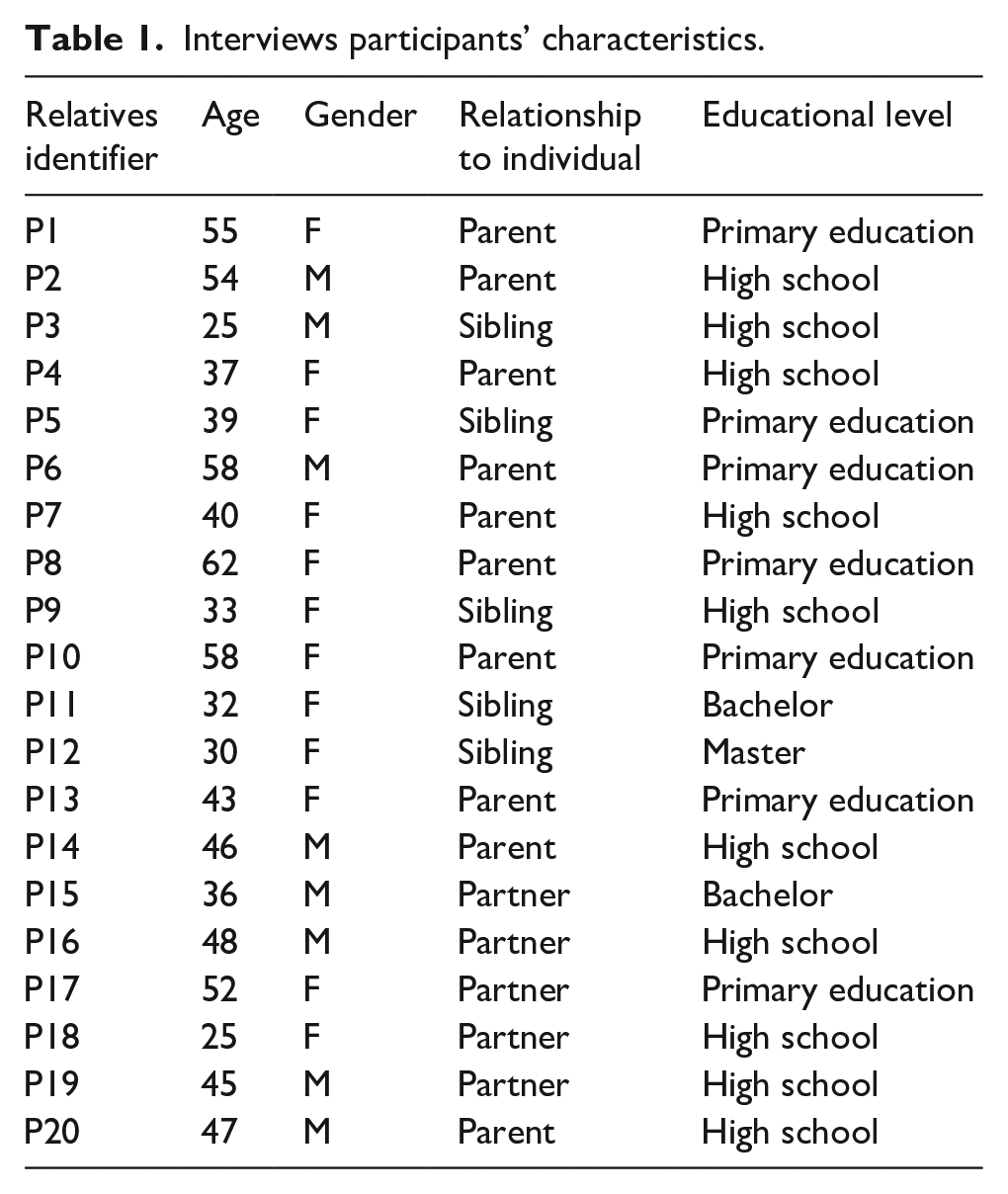
Over the 8 months period (June 2019–February 2020), 20 out of 25 eligible caregivers agreed to participate in the study: 10 were parents, 5 siblings, 5 partners and 11 of the total sample were female (see Table 1).
Interviews participants’ characteristics.
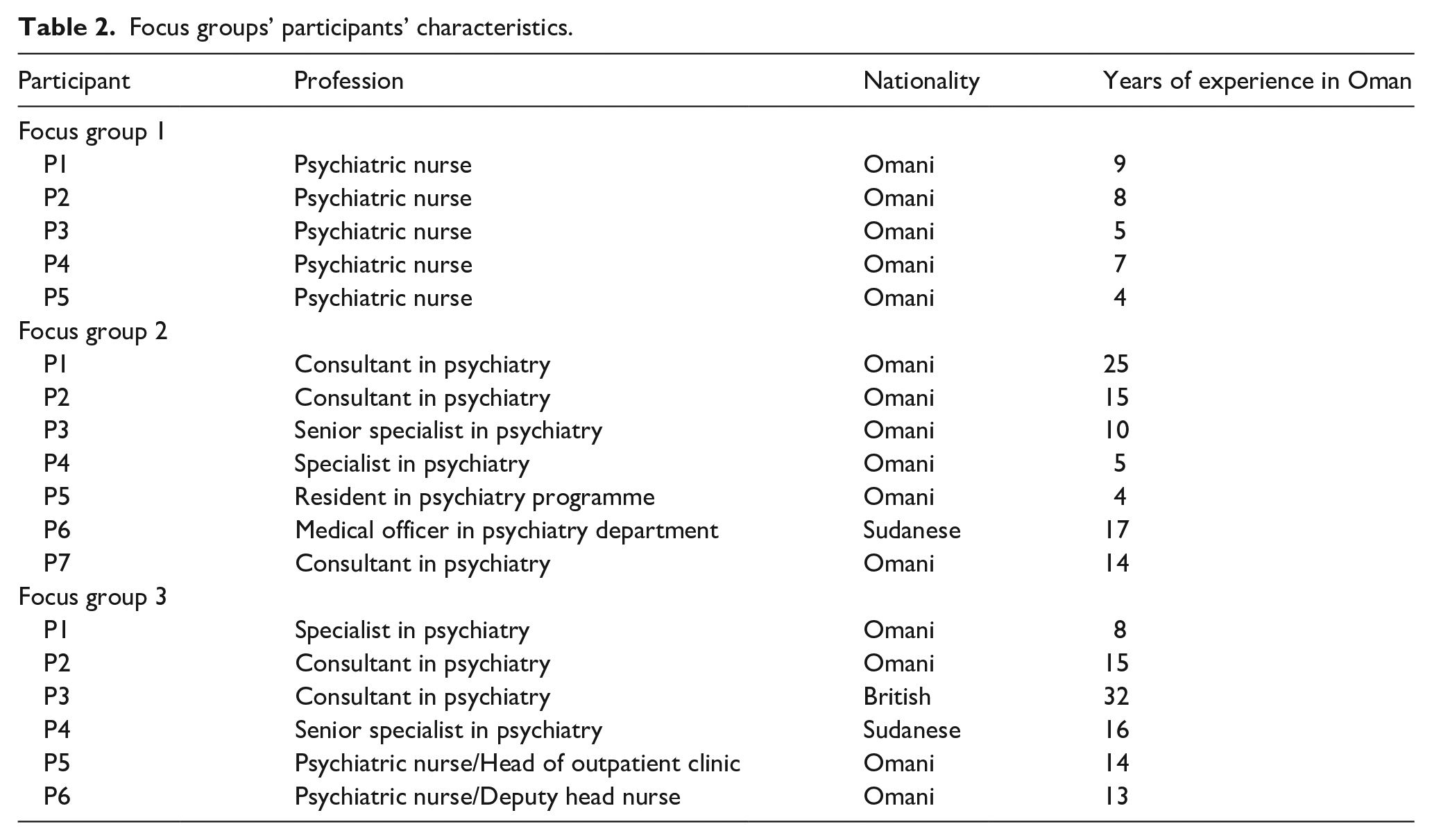
Additionally, 15 nurses and 20 psychiatrists were invited to participate, and three focus groups were conducted with a total of 7 nurses and 11 psychiatrists (see Table 2). The nurses’ and psychiatrists’ focus groups were conducted over 1 month, and the consensus group was conducted after 5 months due to the COVID-19 pandemic.
Focus groups’ participants’ characteristics.
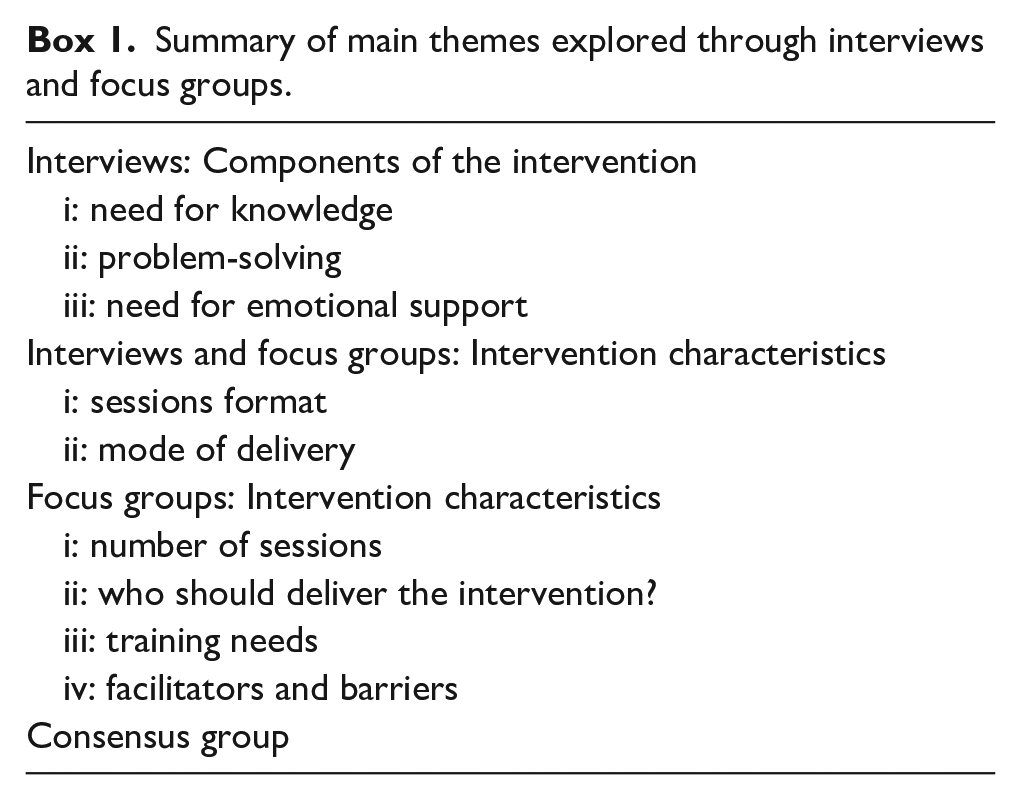
Findings from the interviews and focus groups were organised under different themes and subthemes. See Box 1:
Summary of main themes explored through interviews and focus groups.
Interviews
Components of the intervention
It was essential to understand the caregivers’ cultural beliefs, existing knowledge and specific needs to identify priorities for the intervention content and the required modification to enhance the acceptability. Caregivers were interviewed to explore their experience of caring for a relative with schizophrenia. Many of them felt confused when their relatives first became ill and tried desperately to understand the change in their relatives’ behaviours.
“At the beginning, we didn’t know what was going on or where to ask for help, we thought this might be magic or Jinn. We took him to traditional healers in different regions of the country. Everywhere you can think of, without any benefit. We felt lost, and then by chance, we were guided to a private clinic with a psychiatrist, and he diagnosed him with schizophrenia and OCD.” (PC3)
The beliefs of the majority of carers determined what they did. For example, the majority sought understanding from traditional healers, believing in their ability to deal with the unknown. Half of the participants reported going to traditional healers in addition to using hospital treatment, and 16 of them believed in the spiritual-social model as the cause of the illness before coming to the hospital. One of the participants stated: “We all thought at the start that it was Jenn or magic. You know, when she finished high school many people proposed to her. I think others were envying her.” (PC 5)
However, with frequent admission and contact with mental health professionals, some family members reported other possible causes for the illness as one participant reported: “I know that genetics, stress and other family issues could play a role in causing a mental illness” (PC10)
Thirteen caregivers did not know the diagnosis even after multiple admissions. One parent, when asked about the diagnosis, said:
“I don’t know. I have never asked them” (PC6)
The rest, who knew the diagnosis, did not understand the nature of the illness and more than half failed to ask or try to understand. A few caregivers were aware of psychological treatment and expressed their wish to receive it.
Most participants reported a good level of satisfaction with the existing services. As one relative commented: “We are very satisfied with the services provided” (PC12)
However, when asked about the suggestion of providing family intervention, more than half of the participants reported a lack of information about the illness and its management. Some felt excluded from the treatment process. Mainly siblings and spouses reported that receiving information about schizophrenia is an important part of the intervention because understanding seemed essential to reduce the burden, confusion and frustration.
Need for knowledge
Participants made it clear that lack of knowledge about the illness resulted in low tolerance and high frustration regarding their relatives’ behaviour. When asked about what specific information they needed, they requested information about the nature of the illness, causes, symptoms, prognosis, medication and side effects, non-pharmacological treatment, symptoms management, signs of relapse, care after discharge and guidance on the available resources. Some caregivers emphasised the importance of including a session discussing the cultural and religious beliefs about the causes of illness and suggested incorporating traditional healers within the programme.
“Magic and Jinn are essential topics to discuss. Families should understand that we believe in their existence, but they are not the cause of mental illnesses.” (PC 11)
Problem-solving
Caregivers expressed their need for clear guidance on dealing with some issues such as non-compliance with medication, aggressive and demanding behaviour, unpredictable behaviour and symptoms like hallucinations, wandering and lack of interest in self-care.
“My children have no idea how to deal with their sick brother or mother. There should be a clear plan for families on how to deal with different issues” (PC16)
Participants also verbalised their need to learn to cope with day-to-day practical problems associated with the illness, such as neglecting self-hygiene or isolating self. They reported that such strategies should match their ‘real world’ and include religious and cultural practices that could fit their daily life routine.
Emotional support
Carers expressed their need for emotional support. They felt abandoned by mental health professionals and expressed frustration due to the lack of information and support. Families additionally expressed their need for a deeper level of understanding of their experience and support for them as carers.
“We need to talk to someone who can listen to us without any fear of judging. It is very difficult to keep it to ourselves” (PC18)
Interviews and focus groups: Intervention characteristics
Session format
Participants were asked about whether a group or individual intervention would be more acceptable. The majority of relatives preferred individual sessions because of their difficulty in talking about private family matters in front of other people. One of the participants said:
“I do not want other families to be involved. As few people as possible should know about the illness to avoid stigma.” (PC6)
Mental health professionals supported this and felt that individualised sessions would help tailor the intervention for the specific needs of the family.
“The needs of each family may differ in regard of how they deal with the patient, level of education and everything else.” (H, FG2)
Some family members showed an interest in group interventions because they could benefit from sharing their experience with others. This was supported by health care professionals who suggested covering some topics in groups and others individually.
“Sharing their experience about the burden of care and how they are coping or dealing with the challenges could be helpful and make them feel less miserable.” (N, FG2)
Mode of delivery
Carers and health professionals suggested a combination of face-to-face sessions with booklets, leaflets, videos or phone application for easy access. They requested simplified language and explanations. Health professionals proposed using social media as a refresher to help families reach out for appropriate support and resources to ensure the programme’s continuity.
Participants were asked their views about involving their ill relatives in the sessions. The majority preferred excluding the patient for the following reasons:
“To discuss our problems and concerns without limitation” (PC4),
“Patients could be psychotic and very disturbed and would interrupt the intervention” (PC6), “They might be afraid to know the details of their illness” (PC3),
“Their feelings could be hurt because they would feel that they are a burden on the family which may make them feel bad” (PC10),
“May feel uncomfortable and embarrassed” (PC17),
“They may get upset and start arguing” (PC5), and
“They might not be willing to attend or participate” (PC9).
Other caregivers and mental health professionals felt that patients should attend because they should be part of the plan and learn self-management. Furthermore, professionals suggested that including patients while in the hospital can help to observe family dynamics. One psychiatrist stated:
“I think patients can be included later on after discharge during outpatient follow up” (H, FG 2)
Focus groups
Number of sessions
Some health professionals suggested a very structured programme with a specific number of sessions so progress could be monitored. Others suggested a more flexible approach, with the provider deciding from a list of topics according to the family’s needs. They suggested that the programme should be long enough to cover the main topics and tailor-made to maximise the benefit, as one participant said:
“You can’t decide the same number of sessions for all families. It will be difficult because you will face a different range of expressed emotions, anxiety and other factors. I think it should be flexible.” (F, FG1).
Who should deliver the intervention?
Nurses and psychiatrists believed that specialised nurses with mental health diploma are best suited to deliver the intervention: “they are aware of patients within the team, and it will be easy to deliver and tailor the intervention for the specific case.” (I, FG1). Others suggested including psychiatrists as well: “investing in both specialised nurses and residents will enrich the discussion and residents can help in introducing the intervention to other parts of the country when they go back to their hospitals.” (I, FG2).
Training needs
Participants expressed that pre-qualification training for most professionals provides them with little or no contact with carers, and therefore they would lack the skills for delivering FIs. They suggested that training should incorporate a detailed knowledge of psychoeducation and other components of delivering the intervention.
“We need a deep understanding of the illness itself, and how to deal with any issues they may encounter with the family.” (A, FG1)
Facilitators and barriers for the intervention
Health professionals were motivated to deliver the intervention and believed that the study site is an ideal setting for providing the intervention as family members are available throughout the admission time. One participant reported: ‘It makes it easier to access family members because it is difficult to depend on calling them or waiting for them in the outpatient clinic’. (A, FG3).
Another added: “the severity of cases admitted at SQUH is less, which makes it easy to include patients in the intervention.” (F, FG3)
Another facilitator is the availability of specialised nurses with every team and the reduced workload compared to other hospitals. One participant said, ‘As this is an academic hospital, the availability of manpower is better, and they have multidisciplinary teams’. (W, FG3). Another significant facilitator is that there is less stigma and greater acceptance at this hospital because it is a tertiary care general hospital, not a psychiatric hospital.
Staff were afraid that they may not be able to systematically deliver the intervention due to issues such as time pressures, lack of clinical supervision and minimal support from administration. Moreover, other barriers such as stigma and cultural beliefs in magic and Jinn caused families to prefer traditional healers and arrive at hospital after a long period of untreated psychosis. Health professionals reported having no proper place to conduct the intervention, which should be addressed.
They added that patients and their families are more focussed on physical health and expect only medication when they visit mental health professionals. They often expect quick remedies and may reject an intervention with no immediate effect. Although most professionals talked about families’ supportive role, some described the difficulties and challenges in dealing with families who might be a barrier to implementing such an intervention.
Consensus group
The group included the head of the department, three consultants, the head nurse and his deputy, all of whom greatly influence decision making. The main sources of discrepancies were the content of the intervention, number of sessions, involving the patient in the intervention, who should deliver the intervention and the needed training.
Health professionals admitted that the current practice of psychoeducation is unstructured, and some receive it while others do not. Therefore, they argued for a more structured approach to providing families with the necessary information related to their relative’s illness. Nevertheless, they agreed that knowledge would be an acceptable component of the intervention. They particularly emphasised the need for information about medication, medication compliance and relapse prevention to reduce the current high re-admission rate in the hospital. The consensus group suggested:
“It is important to use simplified language that can be understood by family members.” (W, FG3)
Health professionals suggested that families’ educational levels might prevent them from accessing the problem-solving and communication skills found in FIs manuals, or they might be culturally inappropriate. They discussed that family dynamics in Omani societies are hierarchical, with parents’ decisions and communication accepted without questioning. The traditional rules prohibit young family members from participating in decision making. Furthermore, the traditional communication pattern discourages easy expression of emotions, relying more on non-verbal communication to express feelings or messages. Professionals suggest that these communication patterns could be a barrier to acceptance of communication techniques in Western manuals. They recommended including culturally relevant and acceptable coping skills:
“It is better to include spiritual and religious aspects like prayers, reciting the Quran or talking to religious people to improve the acceptability of the intervention.” (M, FG3)
Mental health professionals agreed on the importance of emotional support for families and were happy to provide it if given training on FI and the appropriate time and resources. They also suggested having caregivers support groups for sharing feelings with others.
Regarding the number of sessions and including the patient in the intervention, the group suggested flexibility depending on the patient’s readiness and the family’s needs, as one participant stated:
“There should be a list of topics to be discussed, and the provider should have the ability to judge the priority” (A, FG3)
Concerning the delivery of the intervention, they agreed on involving both specialised nurses and residents. However, they insisted on having an expert in FI as a lead person and the trainee’s trainer. They suggested having a follow-up for each family.
Participants suggested training providers on delivery of the intervention, which is a dynamic process that may include addressing feelings and reactions. One professional said: “You cannot assume that their knowledge is enough, or they are confident in providing such interventions, because it is not about delivering information; it is about making it more structured and providing a proper course on how to deliver it.” (A, FG3).
Mental health professionals suggested collaborating with an expert in FI to train the providers and supervise them during the initial stage. They suggested proper preparation with follow-up, evaluation and modification.
The group agreed that having a protected time for the interventions and getting approval from administrative authorities may overcome barriers and ensure commitment.
See Figure 1 for the proposed framework for the intervention.
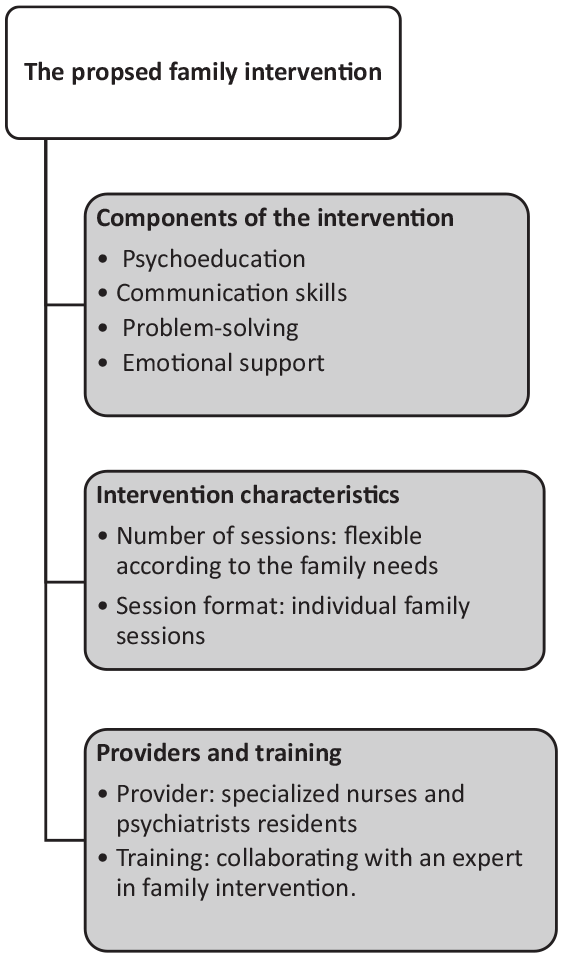
Framework for the intervention.
Discussion
This study is the third stage in the process of developing a FI for Omani relatives caring for hospitalised individuals with schizophrenia (Al-Sawafi et al., 2020, 2021). The current study is the first to explore relatives’ and health professionals’ views and opinions to inform the development of a FI in the inpatient unit. Carers gave their opinions and preferences about the intervention’s content, drawn from their personal experiences while caring for a relative diagnosed with schizophrenia. Concurrently, mental health professionals discussed the intervention delivery system from a clinical standpoint concerning issues and barriers to implementation. The consensus regarding content of the intervention was to include psychoeducation, problem solving and emotional support. The component of emotional support has not been reported in previous studies in the Arab world (Al-Sawafi et al., 2020) because the interventions were delivered during follow-up in outpatient clinics. However, the current study was conducted during hospitalisation and the emotions of families at this stressful time need to be addressed (Lobban & Barrowclough, 2009).
Similar studies of culturally adapted interventions for schizophrenia used the same approach of interviewing patients, carers and health professionals to inform the development of the intervention (Edge & Grey, 2018; Hackethal et al., 2013; Li et al., 2017; Naeem et al., 2016; Rathod et al., 2010). However, the significant difference in this study is the lack of patients’ input. Although the views of the patients are very important for informing the development of the intervention, it was not possible because interviews were conducted during hospitalisation in the acute psychiatric unit, and patients were acutely unwell. This exceptional circumstance made it challenging to involve patients. However, further work will explore patients’ views in the outpatient clinic to inform adjustments to the developed intervention.
The focus of this study was different from in previous studies since the intervention was centred more on relatives because they stayed with patients throughout the admission time. The experience of being in the psychiatric inpatient facilities can be intimidating, and relatives need help to understand what is going on with their loved ones during admission (Lobban & Barrowclough, 2009).
Moreover, family members in collective societies such as Oman usually determine the help-seeking behaviours and the treatment pathway, which is different from the Western societies that emphasise individual autonomy (Al-Adawi, 2017; Al-Krenawi & Graham, 2000). Therefore, exploring the views of relatives first could ensure the acceptance of involving patients later on.
The majority of participants in interviews and focus groups reported that FIs would be applicable and acceptable if culturally adapted. The findings from interviews and focus groups indicated that the cultural adaption of the intervention focussed more on themes such as religious and spiritual causes of mental illness, simplified language, format of delivery as individual sessions, culturally relevant and acceptable coping skills and communication skills. This confirms our previous findings in the systematic review (Al-Sawafi et al., 2020) and agrees with some existing literature about adapting CBT in China, Pakistan, Saudi Arabia and Bahrain (Algahtani et al., 2019; Li et al., 2017; Naeem et al., 2016).
Families living with individuals diagnosed with schizophrenia in Oman emphasised the role of religious and spiritual causes, which also confirms our previous findings in the systematic review (Al-Sawafi et al., 2020). Nearly all nurses and psychiatrists highlighted the importance of incorporating spiritual and cultural beliefs because these influence caregivers’ understanding of illness causes, health-seeking behaviours and attitude towards treatment. Our results agree with existing literature on cultural adaptation (Barrio & Yamada, 2010; Edge et al., 2016; Naeem et al., 2015). Integrating social and biological models is important because just focussing on the biological model may not be acceptable (Hackethal et al., 2013). This study supports the view of previous studies on collaborating with traditional healers to meet the spiritual needs of participants (Al-Sawafi et al., 2020).
Mental health professionals emphasised that language also required adapting instead of just translating. Algahtani et al. (2019) found that using classic Arabic terms can cause a communication barrier, and they recommended culturally sensitive translation of the content. Previous cultural adaptation studies argue that it is essential to make adjustments, but it should be kept close to theoretical underpinning (Li et al., 2017). Relatives prefer the individual family sessions because Omani people feel sensitive discussing their relative’s details in front of other families, which is congruent with the findings of our systematic review (Al-Sawafi et al., 2020). Furthermore, health professionals supported this view and found it as an opportunity to tailor the intervention to each family’s needs.
The health professionals discussed the need for modifying the communication and problem-solving skills to fit the sociocultural context of Omani families. This finding is consistent with the Egyptian study that found the hierarchy of power within the Arab families can hinder the application of communication skill techniques (Wahid, 2009). It is documented in the literature that Arab communication styles are restrained and formal (Al-Krenawi & Graham, 2000). This is the opposite of Western culture, where communication patterns are personal and expressive. Therefore, communication techniques in Western manuals have limited application to Arab populations (Al-Krenawi & Graham, 2000). In a study about the Omani family dynamics, parents expressed that they still have full control over their children’s lives and their children obey and respect their parents’ wishes (Al-Barwani & Albeely, 2007).
Our results show that relatives and mental health professionals agree on major issues, but opinions diverged about involving patients in the sessions. While the current study did not interview patients, most caregivers and some health professionals suggested not including the patient in the intervention sessions because they are acutely unwell during admission or are concerned about hurting their feelings. The rest of the caregivers and most health professionals suggested including the patients in some sessions once they have improved and are willing to attend. The available data regarding patients’ involvement in the sessions have varied in the previous studies, with the majority including the patients, while some used a mixed approach of including the patients in some sessions (Al-Sawafi et al., 2020; Wahid, 2009). The decision regarding including or excluding patients was not evident in the literature, and the majority of studies involved participants during outpatient follow-up. However, the consensus group suggested a flexible approach depending on each family’s needs assessment, which was one of the main points discussed by Lobban and Barrowclough (2009) in their Casebook of FIs for Psychosis. They suggested a structured approach for the intervention but flexible enough to respond to the family’s needs (Lobban & Barrowclough, 2009).
Health professionals provided specific suggestions to facilitate the implementation of FI. They were motivated to implement the intervention because of caregivers’ availability during admission and the reduced workload and stigma in the studied hospital. While many of the barriers mentioned in the previous studies are related to engagement, and travelling distance and expenses (Algahtani et al., 2019; Naeem et al., 2016; Wahid, 2009), these barriers were overcome because of the timing of the intervention delivery and the availability of relatives throughout the patient’s admission time.
One of the possible barriers that emerged from the interviews and focus group is the staff culture and the culture of psychiatric institutions in Oman. Many relatives revealed common problems of knowing little about the illness and having difficultly engaging with the staff in the treatment plan. When these issues were discussed with mental health professionals, they reported that lack of time, training and skills to provide such interventions were the reasons. Furthermore, in most cases, families were not convinced with the diagnosis and believed more in the spiritual causes, which made them uninterested in learning about the disease.
Although clinicians are keen to implement such intervention, they lacked the knowledge and skills of psychosocial interventions, they expressed their need for proper training to ensure commitment to and continuity of the programme. Studies have shown that clinicians can deliver FIs even after brief training, but it takes time and persistence for them to become part of the health care system (Lobban & Barrowclough, 2009). Mental health professionals suggested having workplace clinical supervision by an experienced practitioner to enhance the training outcome. This model of training and supervision was tested in one study using practitioners in the student’s own workplace to deliver supervision, which enhanced the potential for implementation of psychosocial intervention in routine practice (Bradshaw et al., 2007).
Although staff are motivated to implement such interventions and the authors are planning for proper training to provide them with the required skills, the mental health institutions’ culture may work as a barrier. However, the development and implementation of the intervention will be slow and reflective to include all the stakeholders in ensuring the integration of FI into the mental health care system in Oman.
The study provided the basis for developing FI in the inpatient setting. The present study identified the intervention’s key components and delivery system, but consensus about the content has still not been reached and requires further work. This step will help prepare the written training materials for the intervention before conducting a feasibility study to test the acceptability of the intervention. If the feasibility study is successful, definitive and adequately powered, randomised controlled trials will be required to test the efficacy of the intervention.
Strength and limitations
The process of gathering data from relatives and mental health professionals was underpinned by methodological rigour. Furthermore, the study provided insights into the development of a FI in the inpatient settings. The study included views and opinions of parents, siblings and spouses to address the different caring needs. However, it has some limitations. First, sampling for interviews and focus groups was conducted in one setting only, which could impact generalisability. Second, the interviews were translated from Arabic to English, and some cultural nuances may have been lost in the translation process. Third, the study lack the view of patients, but further research in outpatient settings can address their needs and experiences.
Implications
The study produced valuable findings regarding developing FI in the inpatient setting. The addressed barriers and facilitators can inform the implementation process of the intervention. Individuals with schizophrenia and their families should be empowered to advocate for their needs and enhancement of the health care system. Individualisation of the intervention based on needs assessment is highly recommended for a better outcome. Staff in the inpatient facilities have a crucial role to play in the delivery of family work. However, support from the hospital administration is critical to reduce the workload and implement the intervention effectively. Further studies should explore the development of such interventions for outpatient settings using the guidelines developed from this study. There is also a need to develop culturally sensitive interventions for other mental illnesses.
Conclusion
The study identified the proposed intervention based on views from relatives and mental health professionals. The findings of the study and the highlighted supporting literature indicated that FI is an acceptable and feasible approach to be delivered during hospitalisation. The information gathered from this study can be used to inform the development of FI in other Arab countries or minority populations in high income countries. Furthermore, the study confirms that understanding cultural factors and each family’s specific needs will enhance the process of engagement with the intervention.
Supplemental Material
sj-docx-1-isp-10.1177_00207640211060694 – Supplemental material for Exploring views of relatives and mental health professionals to inform the cultural adaptation of a family intervention for schizophrenia in Oman: A qualitative study
Supplemental material, sj-docx-1-isp-10.1177_00207640211060694 for Exploring views of relatives and mental health professionals to inform the cultural adaptation of a family intervention for schizophrenia in Oman: A qualitative study by Aziza Al Sawafi, Karina Lovell, Laoise Renwick and Nusrat Husain in International Journal of Social Psychiatry
Supplemental Material
sj-docx-2-isp-10.1177_00207640211060694 – Supplemental material for Exploring views of relatives and mental health professionals to inform the cultural adaptation of a family intervention for schizophrenia in Oman: A qualitative study
Supplemental material, sj-docx-2-isp-10.1177_00207640211060694 for Exploring views of relatives and mental health professionals to inform the cultural adaptation of a family intervention for schizophrenia in Oman: A qualitative study by Aziza Al Sawafi, Karina Lovell, Laoise Renwick and Nusrat Husain in International Journal of Social Psychiatry
Footnotes
Author contributions
AA conducted the interviews and analysed and interpreted the data, and was a major contributor in writing the manuscript. KL, LR and NH contributed to the conception and design of the work and substantively revised the manuscript. All authors read and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declarations
The content has not been published or submitted for publication elsewhere.
Ethics approval
Ethical approval was obtained from the University of Manchester Research Ethics Committee (Ref: 2019-5038-9106) and Sultan Qaboos University Hospital Medical Research Ethics Committee (REF.NO.SQU-EU/085L19).
Data availability statement
Data available on request from the authors
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.