
Abstract
Objectives:
To assess and compare the changes in disability scores associated with Bipolar Depression (BD) and Unipolar Depression (UD) over 1 year.
Methods:
A longitudinal study was taken up in adults diagnosed with unipolar or bipolar depressive disorder with current depressive episode. Diagnosis was made according to Schedule for Clinical Assessment in Neuropsychiatry. Severity scoring was done using Hamilton’s Depression (HAM-D) rating scale and Hamilton’s Anxiety (HAM-A) rating scale. Disability was assessed using Indian Disability Evaluation and Assessment Scale (IDEAS) and London handicap Scale (LHS) at baseline, 6 and 12 months.
Results:
Sixty participants were recruited (42 UD and 18 BD). No significant differences were seen in socio-demographic parameters, except higher education levels and males being overrepresented in UD. Significant differences at baseline were seen in HAM-D (p = .001) and HAM-A (p = .003) scores. The extent of disability was seen to correlate with severity of illness only in case of BD at baseline. No significant differences were seen in the IDEAS scores at baseline. IDEAS score improved at each follow-up assessment (p < .001). LHS showed significant improvement over time in UD (p < .001), but not BD (p = .076). Percentage individuals meeting cut-off for benchmark disability (>40%) were comparable at baseline but were significantly more in the BD at 12-months (p = .049).
Conclusion and implications:
Disability in psychiatry occurs equally amongst unipolar and bipolar depressive disorders and tends to improve over time, although the level of improvement may differ. It may not always correspond to severity of illness. These factors should be considered while certifying disability.
Background
Mental disorders are one of the leading causes of years lived with disability (YLDs) and disability adjusted life years (DALYs) (Sagar et al., 2020). As per the 2018 GBD report, 197.3 million individuals in India are suffering from psychiatric illness (Sagar et al., 2020). The contribution of psychiatric illness in the total DALYs in around 4.7%, with depressive and anxiety disorders contributing to more than half of these DALYs (Sagar et al., 2020). Disability in depression has been seen to be higher than various common medical disorders like hypertension, and diabetes mellitus (Singh & Ajinkya, 2012). A study done on primary care patients estimated higher socio-occupational disability is seen in patients with co-morbid mental disorders than with single mental disorder. After adjusting for socio-demographic as well as clinical factors (including other mental disorders), it was observed that patients diagnosed with phobia, depression, bipolar disorder, and substance use disorder had significantly more disability as compared to patients without psychiatric illness (Olfson et al., 1997).
Efforts have been made by researchers to find the answers on how to segregate unipolar and bipolar depression from each other which has clinical and research implications. People have investigated the pathological process, clinical variables, and even outcome measures of both types but still it is not easy to ascertain the differences with conviction (Smith & Craddock, 2011). The chronic nature of these disorders subjects the individual to spend a significant time of his life with active symptoms and unable to meet the needs of daily life (Forte et al., 2015). It has been emphasized that depressive episode and symptoms in a bipolar disorder largely govern the disability associated in bipolar disorder (Judd et al., 2005). Similarly, unipolar depression is associated with significant psychosocial disability (Judd et al., 2000). While there are studies on course and outcome of the two types of disorders, no studies could be found comparing disability across the two disorders and its longitudinal course.
Longitudinal data comparing disability associated with various psychiatric illnesses are few. A longitudinal study was done in North-east India to compare disability across different diagnostic categories seeking treatment from their institution and reported schizophrenia to be having maximum disability scores with no differences found between other psychiatric disorders (Chaudhury et al., 2006). The authors briefly discussed the longitudinal course of disability in various illnesses which showed improvement at the end of 6 months. Of the various illnesses they assessed, they reported that disability in BD evened out at 12 months while in UD, it worsened. We, thus, aimed to assess and compare the disability associated with bipolar and unipolar depressive disorders over a course of 1 year, and to assess its relationship with socio-demographic and clinical variables.
Methods
After taking ethical clearance from the institutional ethical committee, a longitudinal study was taken up on out-patients presenting in the Department of Psychiatry at a tertiary care center in North India. Participants were recruited by purposive sampling method. Prior to actual data collection, a pilot study was conducted on administration of instruments by the staff recruiting the patients.
Selection criteria
Patients of either gender aged 18 years and above, presenting with depressive symptoms (with or without anxiety symptoms) were approached. Those diagnosed as unipolar depressive disorder (F32–33) or Bipolar affective disorder (F31.3–31.5), current depressive episode irrespective of severity of symptoms were recruited. Young’s Mania Rating Scale (Young et al., 1978) (YMRS) was used to screen out patients with active manic symptoms (manic/mixed episodes). The diagnosis was made according to the International Classification of Diseases, 10th edition (World Health Organization [WHO], 1992) using SCAN (WHO, 1994). Patients with mental retardation, chronic debilitating illness, organic brain disease (excluding dementia and alcohol use disorder), psychiatric co-morbidity (other than the primary diagnosis), and non-willingness to participate in the study, were excluded from the study. The patients were then followed up at sixth and twelfth month after recruitment.
Assessment instruments
Semi-structured proforma: A proforma noting details on socio-demographic and clinical profile of the participants was used which was applied only at baseline. Details included: age, sex, number of years of education, marital status, employment status, socio-economic status, type of family, place of residence, and religion, age of onset of illness, duration of illness, course of illness, medications details, current severity of illness, past hospitalizations, and family history of psychiatric illness. In addition to the semi-structured proforma, the following instruments were used in the study.
Schedule for Clinical Assessment in Neuropsy-chiatry (SCAN) (WHO, 1994): The SCAN is a set of instruments and manuals aimed at assessing, measuring, and classifying the psychopathology and behavior associated with the major psychiatric disorders of adult life. The SCAN text has three components: the 10th edition of the present state examination (PSE 10), the Item Group Check list (IGC), and Clinical History Schedule (CHS). PSE 10 itself has two parts. Part 1 covers somatoform, dissociative, anxiety, depressive, and bipolar disorders, and problems associated with eating, alcohol, and other substance use. Part II covers psychotic and cognitive disorders and observed abnormalities of speech, affect, and behavior. The SCAN text is intended for use only by clinicians with an adequate knowledge of psychopathology. It was applied only at baseline for assessing the diagnosis.
For assessment of severity of symptoms, scales used were: Hamilton’s Depression (HAM-D) rating scale for symptoms of depression (Hamilton et al., 1976), Hamilton’s Anxiety (HAM-A) rating scale for comorbid anxiety symptoms (Hamilton et al., 1976). HAM-D and HAM-A are frequently used and validated instruments with good internal consistencies. These two scales were applied at baseline and later at twelfth month after recruitment. In order to recruit only those with bipolar depression for the study, those with YMRS >7, were excluded from the study.
For assessment of disability: a. Indian Disability Evaluation and Assessment Scale (IDEAS) (Thara, 2002): This is a brief scale that has been developed to identify and quantify disability produced by mental disorders for the purpose of determining eligibility for welfare programs. It consists of four items: selfcare, interpersonal activities, communication and understanding, and work. However, the total score also includes a duration score which is calculated from month of illness in last 2 years(MI2Y). b. London Handicap Scale (LHS) (Harwood et al., 1994): This is a standardized simple six item questionnaire seeking information on the person’s mobility, work, leisure activities, self care, and financial position. It has been extensively used in several international studies for assessing disability in various illnesses. It is scored from 0 (most severe disadvantage) to 1 (no disadvantage).
Study procedure
All patients seeking treatment at the Psychiatry out-patient department (OPD) of the institute were eligible for participating in the study. After screening out for inclusion and exclusion criteria, the patients were recruited after taking informed consent. In the initial assessment, semi-structured proforma consisting of sociodemographic and clinical details, and SCAN were applied. After the initial assessment, HAM-A and HAM-D were applied to assess the severity of the illness. This would take around 1 to 1.5 hours. Subsequently, scales to assess disability (IDEAS, LHS) were applied, within 1 week of the initial assessment. The patients were then assessed at 6- and 12-months post recruitment. At 6 months only scales related to disability that is, LHS and IDEAS were applied while at 12 months scales for symptom severity that is, HAM-A and HAM-D were also applied. Those who did not follow up were contacted over phone.
Statistical analysis
Data analysis was conducted using SPSS software version 20 (IBM Corp, 2011). Means, standard deviations, frequencies, and percentages were used to describe the data. Shapiro Wilk test for normality was used to assess the distribution of the data and most variables were found to be not normally distributed. Since most variables were not normally distributed, non-parametric tests were preferred. For comparing characteristics between unipolar and bipolar depressive disorders Mann Whitney U test was applied. Relation between two continuous variables was assessed using Spearman’s correlation. Comparisons in various parameters across time were done with the help of paired tests (Friedman’s test for comparison across three time points and Wilcoxon signed rank test for pairwise comparisons between two time-points). A value of p < .05 was considered statistically significant, and missing value imputation was not carried out.
Results
A total of 60 (42 diagnosed with UD in group I, and 18 with BD, in group II) patients were recruited in the study. Table 1 presents and compares the socio-demographic and clinical characteristics of the two groups. Average age between the two groups were statistically comparable. No significant differences were seen in other socio-demographic parameters except, gender, and years of education. UD group had overrepresentation of male gender and higher education as compared to BD group. In terms of clinical parameters, duration of illness was significantly higher in BD group, and differences in the course of illness were seen. Most patients in BD group had an episodic course and longer duration of illness. The frequency of being hospitalized was also proportionately higher in BD than UD group.
Socio-demographic and clinical characteristics of patients with UD and BD (N = 60).
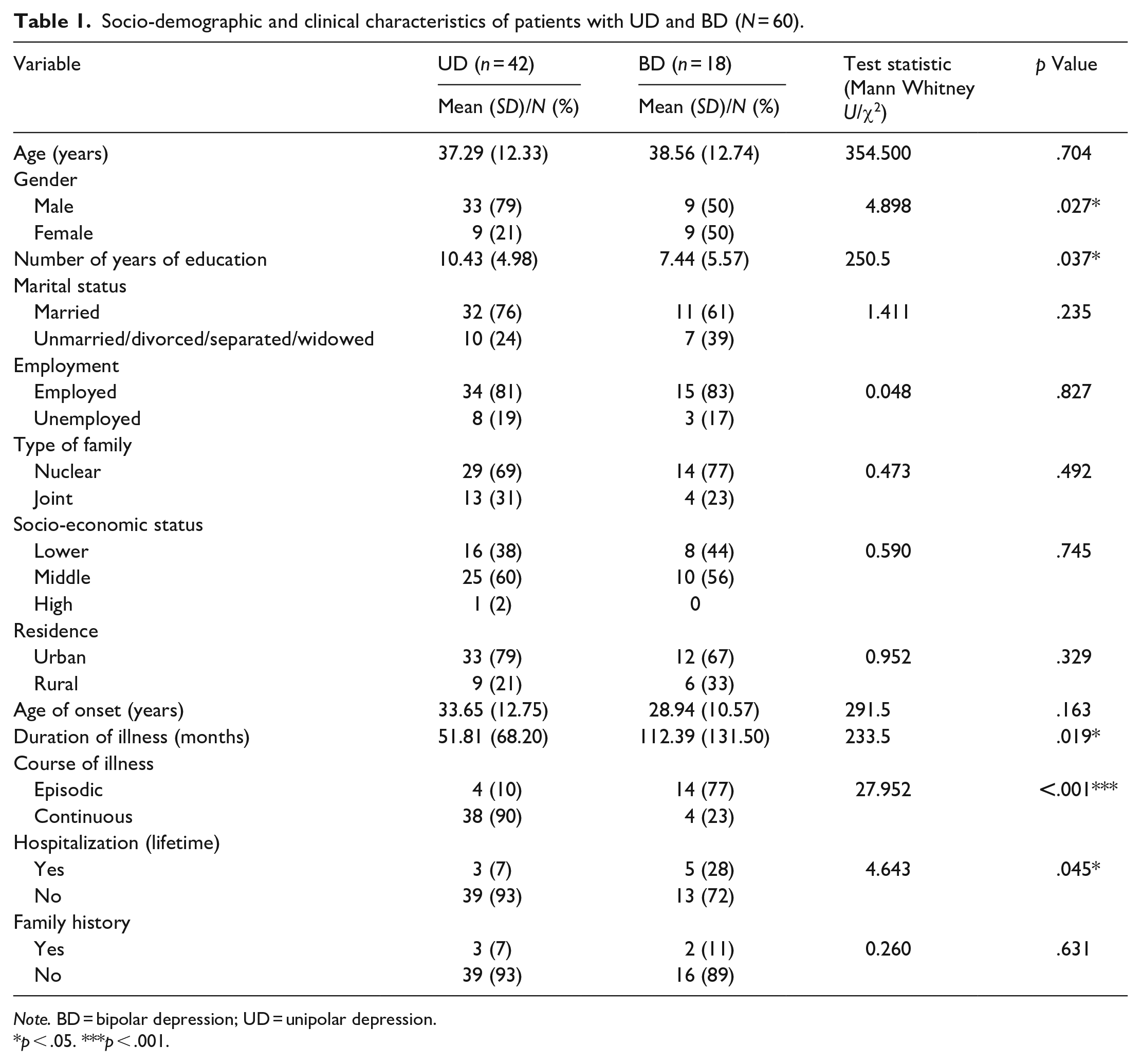
Note. BD = bipolar depression; UD = unipolar depression.
p < .05. ***p < .001.
Table 2 illustrates the differences between the severity scales for depressive and anxiety symptoms on HAM-D and HAM-A scales, respectively. Significant differences were seen at baseline in the scores on both scales between the two groups with UD patients having significantly higher scores on both scales. However, at 12-month follow-up no significant differences were seen in HAM-D scores between the two groups, possibly due to significant improvement and thereby reduction in HAM-D scores in the UD group. Mean HAM-D scores in both the groups was nearly reaching remission values (⩽7). Significant differences continued to remain at 12-month follow-up in HAM-A scores. However, the mean HAM-A scores in both the groups were at sub-clinical level (<8). On applying Wilcoxon signed rank test in each group, significant reductions were seen in both the scales in both UD (HAM-D: Z = −5.49, p < .001; HAM-A: Z = −5.08, p < .001) and BD (HAM-D: Z = −2.67, p = .008; HAM-A: Z = −2.39, p = .016).
Scores on HAM-A and HAM-D at baseline and 12 months in UD and BD (N = 60).
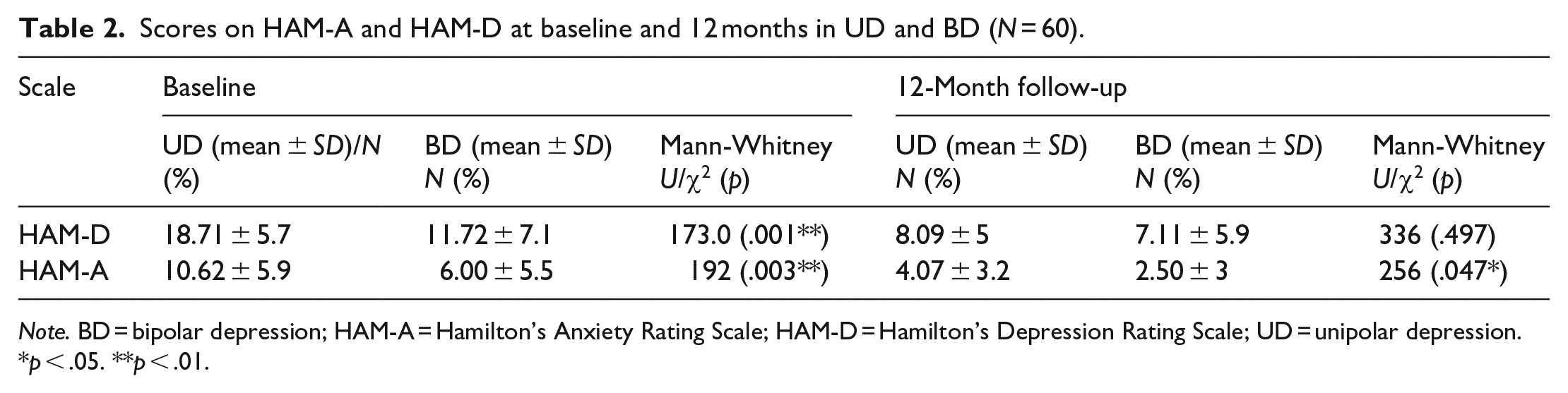
Note. BD = bipolar depression; HAM-A = Hamilton’s Anxiety Rating Scale; HAM-D = Hamilton’s Depression Rating Scale; UD = unipolar depression.
p < .05. **p < .01.
Table 3 presents the differences in the disability scores (IDEAS and LHS) over time. Significant differences were seen in IDEAS scores which continued to reduce over time in both BD and UD patients. The differences were significant at each time-point (baseline-6 month and baseline-12 month) (p < .001). LHS, however, showed significant improvement over time in UD group, but not BD group (p = .076).
Comparison of disability scales in UD over time.
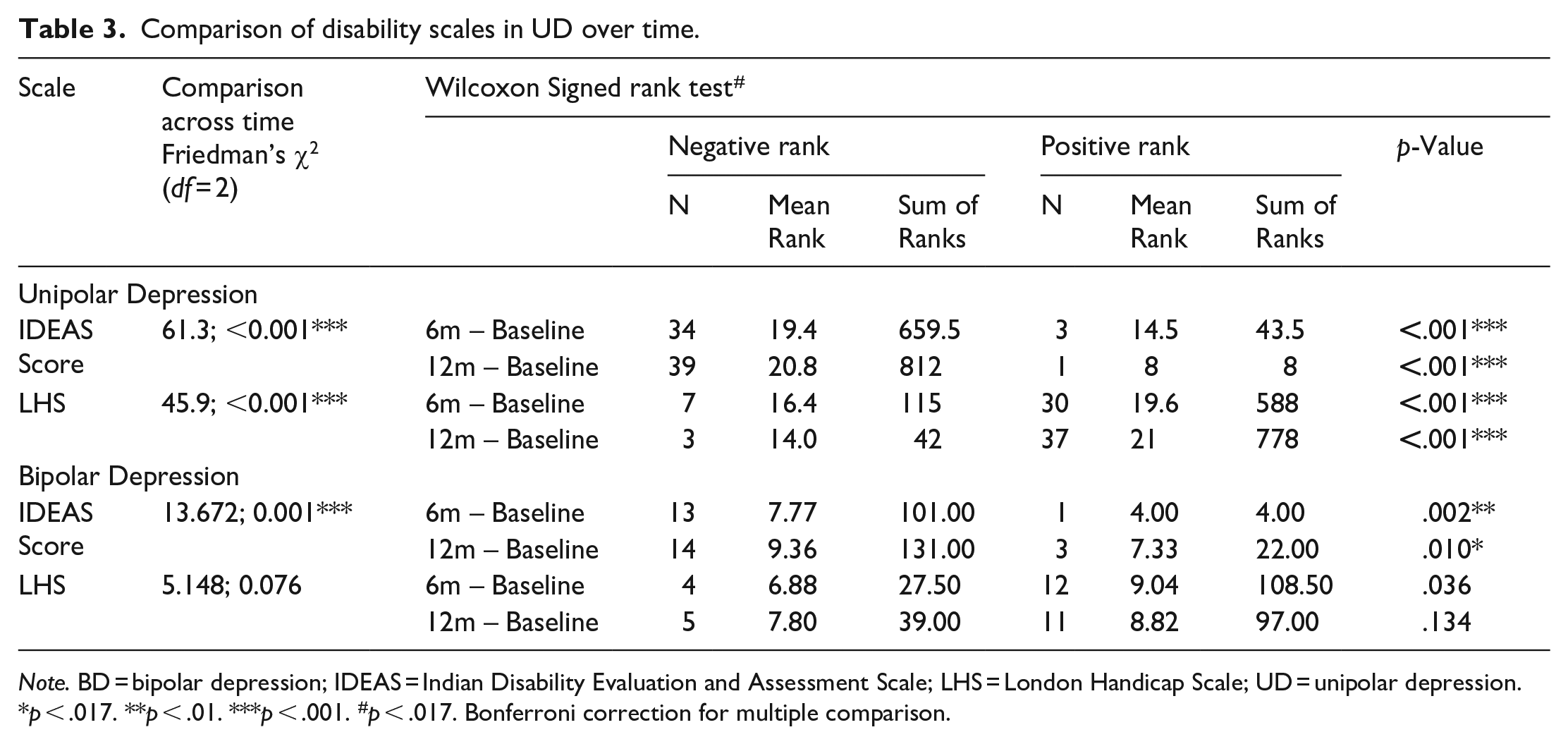
Note. BD = bipolar depression; IDEAS = Indian Disability Evaluation and Assessment Scale; LHS = London Handicap Scale; UD = unipolar depression.
p < .017. **p < .01. ***p < .001. #p < .017. Bonferroni correction for multiple comparison.
Table 4 demonstrates differences in the disability scales (IDEAS global score, LHS scores, and the percentage of individuals meeting cut-off for benchmark disability of >40%) at each time point (baseline, 6- and 12-month). Figure 1 is a line diagram depicting the trend over time. No significant differences were seen in any of the scale scores at any time point. However, the percentage of individuals meeting cut-off for benchmark disability (i.e. disability percentage >40%) were significantly higher amongst BD as compared to UD at 12 months. On applying Spearman’s correlations, no significant correlations were seen with duration of illness with IDEAS or LHS scores in either group or severity of illness with IDEAS or LHS except significant correlation between IDEAS global score and HAM-D score in BD at baseline (spearman’s coefficient = 0.510* p = .031).
Scores on disability scale at three time points.
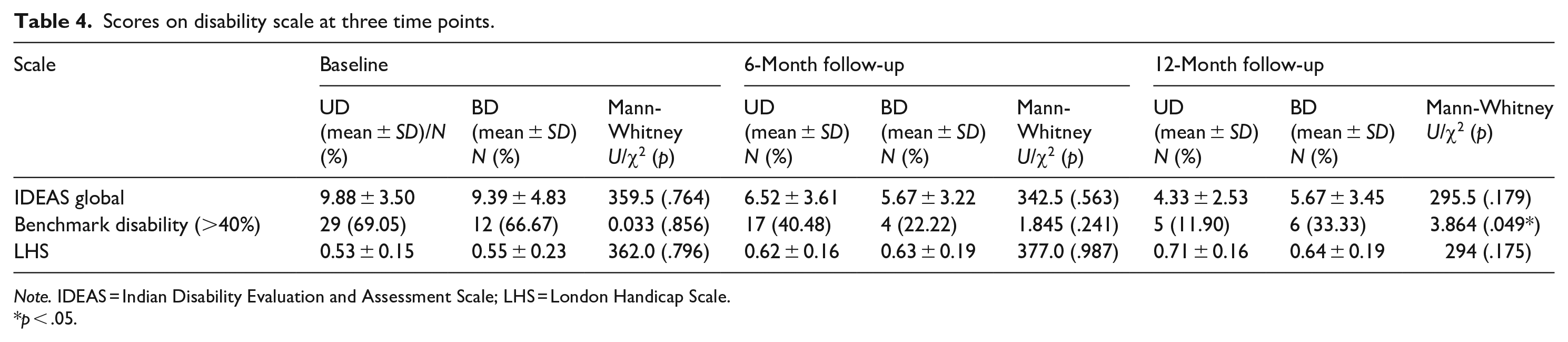
Note. IDEAS = Indian Disability Evaluation and Assessment Scale; LHS = London Handicap Scale.
p < .05.
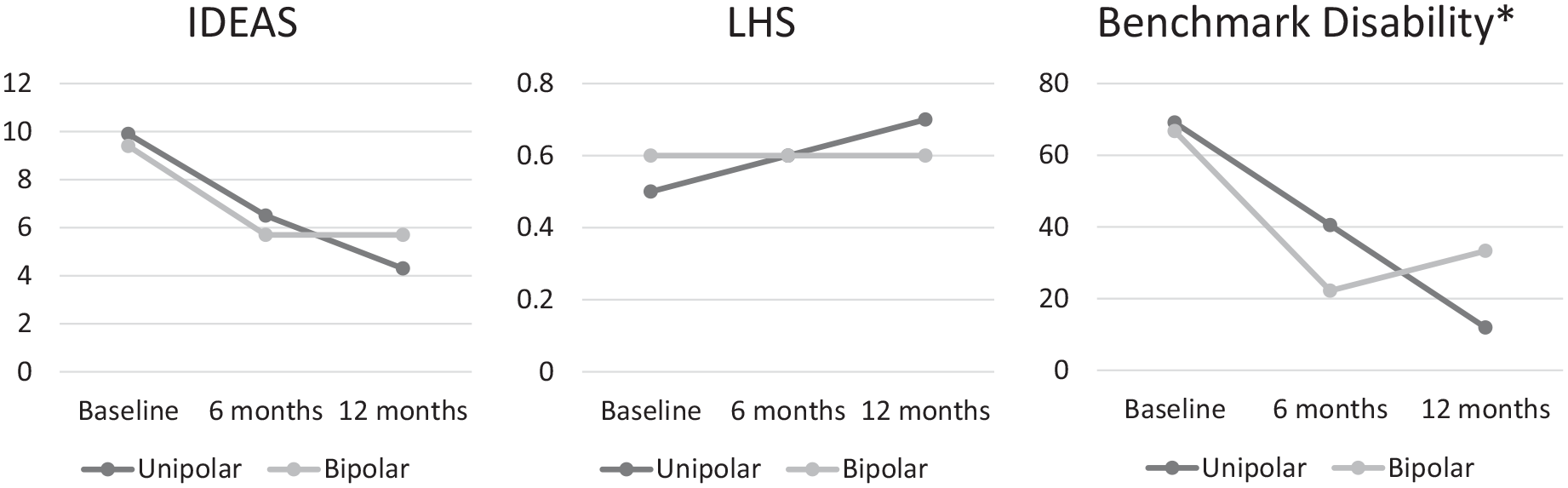
Scores on disability scale at three time points (*p < .05).
Discussion
The present study is among the few which has looked into the profile and nature of disability, its relationship with the mental disorder and its course over the time longitudinally. We found no significant differences at any time point (baseline, 6-or 12-month) in the total disability scores (IDEAS/LHS) on either of the two scales used in the study. However, on categorizing the scores according to the benchmark disability (>40%) as defined in the Rights of Persons with Disability Act, 2016 (RPWD), significant differences could be seen on 12-month follow-up, where significantly higher percentage of individuals with the diagnosis of BD fell within the cut-off of benchmark disability as compared to UD. This explains the prevailing clinical practice of a greater number of certificates being issued to patients with BD than UD (Chadda et al., 2021; Jadhav et al., 2021). These findings could be associated with or even confounded by certain results from the study, such as higher education level and shorter duration of illness in UD group (however duration of illness did not show any significant correlations with IDEAS or LHS scores), and greater number of past hospitalizations in BD group. Previous studies have shown that education level and duration of illness play a significant role in determining functioning and level of disability (Chang et al., 2012; Green et al., 2000; Mowbray et al., 1996). In fact, IDEAS also incorporates duration of illness score for calculating the total disability (Indian Psychiatric Society, 2002) which may not be ideal for longitudinal assessments. Overall, significant improvements were seen in the disability scores on IDEAS in both the groups. This is in support of common clinical practice of temporary certification for disability in psychiatry as illnesses are known to show improvement in functioning over time.
We used two scales for assessment of disability in our study, viz., IDEAS and LHS. IDEAS is a commonly used scale for assessment of disability in psychiatric illnesses in Indian settings. LHS has been derived from the descriptive framework of handicap developed by the World Health Organization (WHO) in the international classification of impairments, disabilities, and handicaps (ICIDH) (Jenkinson et al., 2000). The dimensions in LHS (mobility, orientation, occupation, physical independence, social integration, and economic self-sufficiency) differ from IDEAS (selfcare, interpersonal activities, communication and understanding, and work) taking into account physical and economic dependence in addition to social functions which predominate in IDEAS. We observed that improvement occurred on IDEAS in both disorders, but LHS showed improvement only in UD. This could be attributable to various factors like higher neurocognitive deficits (Smith et al., 2006), physical co-morbidities, and metabolic derangements (Moreira et al., 2017; Silarova et al., 2015) in BD patients in comparison to UD patients. Moreover, baseline differences were seen in HAM-D scores between the two groups which could have cofounded the results as mild to moderate depressive episodes are known to respond poorly and slower to pharmacological therapies than moderate to severe depressive episodes (Khan et al., 2002). Both scales have been used in Indian studies on various psychiatric illnesses (Chaudhury et al., 2006) and it is important to understand the consistency between the two scales. IDEAS, which is commonly used for assessing disability for providing certification to avail disability benefits in India. It would, therefore, be worth exploring the factors in BD which contribute to greater disability in BD patients which may not be captured in IDEAS.
The study has various clinical implications. It is important to assess disability in psychiatric illnesses regularly as it has been seen to improve over time. The disability and dysfunction of patients with UD may be as high as BD and they should not be deprived of the benefit from the administrators and policy makers. Mental disability is not visible and thus there is decreased awareness about the government schemes for the needy. Patients usually do not avail disability benefits optimally and there is overall underutilization of the services (Chadda et al., 2021). It is important for the clinicians to identify the predictors of disability, which can then be targeted for intervention and rehabilitation. It is also important to estimate the level of disability using standardized disability scales as disability may or may not correlate with the severity of illness. Hence, it is not obvious to extrapolate the severity of illness to estimate the disability in all kinds of psychiatric illnesses. The current disability empowerment schemes are not as well catered for psychiatric disabilities as they are for physical disabilities. This is probably because the course of illness and related disability in psychiatric illness is often difficult to predict. Thus, a different approach is required to empower those suffering from psychiatric disorders which may be equally disabling as physical disorders. In light of our study findings, we would like to recommend a few disorder-specific approaches which may be of greater benefit to the affected individuals. For illnesses like unipolar depression, where the disability is equally severe but short-lasting, the focus of the government should be to provide short-term disability aid/relief in addition to covering the medical expenses incurred by the patient. While for bipolar depression, in which the psychiatric disability is relatively longer-lasting, the government should include disease-specific programs, for example, long-term rehabilitation and care facilities, vocational training, and disability pension.
The study has various strengths to it, use of a standardized instrument for diagnosis, assessing disability across different types of depressive disorders longitudinally for over a year, and using different scales to verify the concordance. However, modest sample size with unequal distribution of samples across diagnosis, excluding individuals with psychiatric comorbidities are some important limitations of the study. Physical factors which might also be contributing to disability in the patients were also not evaluated. In addition, taking sample from a tertiary care center limits generalizability of the results at large. In future, it may be worthwhile to observe the findings in a large sample, and across different diagnosis taking into account both psychiatric and physical co-morbidities.
Conclusion
Disability in psychiatry occurs equally amongst unipolar and bipolar depressive disorders. However, the extent of disability was seen to correlate with severity of illness only in case of bipolar disorder at baseline. Various clinical and socio-demographic factors may be associated with the severity of disability. The treating psychiatrist should keep in mind the factors which might predict the extent of disability in an individual with psychiatric illness, which might help in better monitoring of patients, and timely initiation and delivery of psychosocial interventions.
Footnotes
Acknowledgements
We acknowledge the support/thank all the research staff and all other persons involved in the study. We extend the gratitude to all the respondents and families for their cooperation and participation in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the WHO (India) (Sticker No. SE/02/413325).