
Abstract
Background:
Clientele’s attitude toward Persons with Mental Illness (PwMI) changes over a period of time. The aim of this study was to explore and understand how and whether perception about PwMI changes when they are seen working like persons without mental illness among those availing services of ROSes café at NIMHANS, Bengaluru.
Methods:
The descriptive research design was adopted with purposive sampling. Community Attitude toward Mentally Ill (CAMI) a self -administered questionnaire of was administered to measure the clientele attitude towards staff with mental illness in ROSes Café (Recovery Oriented Services). A total of 256 subjects availing services from the ROSes café recruited in the study. Chi-square and Mann–Whitney U test was computed to see the association and differences on selected variables.
Results:
The present study results showed that subjects had a positive attitude seen in health care professionals in the domains of benevolence (BE) (28.68 ± 3.00) and community mental health ideology (CMHI) (31.53 ± 3.19), whereas non-health care professionals had showed negative attitude in the domain of authoritarianism (AU) (30.54 ± 3.42) and social restrictiveness (SR) (30.18 ± 3.05). Education, employment, marital, income, and working status were significantly associated with CAMI domains.
Conclusion:
PwMI also can work like people without mental illness when the opportunities are provided. The community needs to regard mental illness in the same manner as chronic physical illness diabetes mellitus and allow PwMI to live a life of dignity by creating and offering opportunities to earn livelihood which would help them recover with their illnesses.
Introduction
People with Mental Illness (PwMI) may experience violations of their basic right to work in developing countries like in India. Work and employment empowers social inclusion in the community or society (Waghorn & Lloyd, 2005). Thus, vocational rehabilitation, predominantly focuses on the reintegration of PWMI into competitive employment (Watzke et al., 2009). Clinical and community rehabilitation units provide assistance to PWMI by reducing the symptoms, enhancing skills, and transformation into community (Chen et al., 2013).
Studies report that rehabilitation measures emphasize on early recovery and focus on coping with life beyond the illness. Pre-vocational training presumes that it requires a period of preparation before getting into competitive employment for PwMI. It means that a job is paid at the market rate and anyone can compete for it (Crowther et al., 2001). Further, pre-vocational training and supported employment by the rehabilitation team plays a major role in helping the PwMI get back to work. Review of literature reported a range of rehabilitation needs were unmet in PwMI and their caregivers in both out-patient and in-patient settings. One of the major needs consistently reported across studies is employment for PwMI (Chadda et al., 2000; Gandotra et al., 2004; Jagannathan et al., 2011; Kulhara et al., 2010; Murthy & Ramaprasad, 2010; Nagaswami et al., n.d.; Pavithra et al., 2013; Pillai et al., 2010; Singh et al., 2010). To fill this gap, rehabilitation led recovery-oriented services need to work in collaboration with PwMI, their family members and the rehabilitation team effectively to meet the needs of the PwMI and their caregivers (Habhab, 2018). In addition to this, one of the key element is professional attitude towards PWMI which plays an important role in promoting recovery, managing their lives beyond their illness and change of perceptions in the community in general (Legere, 2007; Mead & Copeland, 2000; Noordsy et al., 2002; Tooth et al., 2003). There are a number of studies which have focused on understanding the various rehabilitation needs of PwMI, their caregivers and community attitude towards PwMI, but very few studies have focused on understanding the health care workers, and non-healthcare workers attitude towards PwMI who are already undergoing supported employment services. With this background, the current study aimed to understand the community attitude of health care and non-health care workers towards PwMI who were working in a café in a supported environment in a day care center.
The uniqueness of this café was: Healthy snacks and beverages were prepared by persons with mental illness who worked in the café, it was hand-held by a multi-disciplinary team of psychiatrists, psychiatric nurses, clinical psychologists, psychiatric social workers and managed by an instructor who was a family caregiver who reported to the team about changes in the patient’s behavior and skills, all accounting happened on a computer, all profits were distributed amongst the PwMI who worked in the café. The café instructor received feedback from the team and the service consumers through a google survey platform which helped the instructor to improve services as well as train the PwMI.
Methodology
The study had adopted the descriptive research design using purposive sampling. The study was conducted in Psychiatric Rehabilitation Services Unit (PRS), National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru. PRS has out patient, in-patient and day care facilities. It has various vocational sections like ROSes cafe, Instrumental activities of daily living (IADL) skill section, Bakery section, Printing section, Green skill section, Weaving section, Computer section, Tailoring section, and Candle section. Patients attend the various activities in the PRS for recreation, engagement, functional improvement and job placement.
As a part of PRS service initiative, the ROSes café was initiated as a supportive employment program in January 2018, with the aim of empowering both in-patients and day boarders in catering skills which is an IADL skill. Of the 87 patients with mental illness trained in IADL skills, 36 patients were day boarders and 51 were in-patients. Two instructors who are family caregivers train the patients in IADL skills like cooking, cleaning, cutting vegetables, cleaning vessels, and communication. They also learn hospitality skills such as welcoming the clientele who visit ROSes café, establishing rapport with them, taking orders, and serving food; yet another skill they learn here is accounting, entering related data in the computer and money transactions with customers as well as the bank. The clientele of this café were mental health care workers such as psychiatrists, psychiatric nurses, psychiatric social workers, clinical psychologists, general health care workers such as dentist, neurologist, and physiotherapist were considered as health care professionals and patient caregivers, multi-skilled staff, security personnel, clerical staff and general public were considered as non-healthcare workers in the present study. The uniqueness of the ROSes Café was, it was run by PwMI (who were receiving rehabilitation services at PRS) with family caregivers.
A total of 256 subjects were recruited using purposive sampling including subjects who utilized ROSes café services frequently, and who spoke Kannada, Tamil and English. Those who were not available at the time of data collection were excluded from the study.
Measures
To measure the community attitude towards mental illness among health care workers and non-healthcare workers, the Community Attitude towards Mentally Ill (CAMI) scale was administered. CAMI scale (Martin Taylor and Michael Dear, 1970) was used to assess the clientele’s opinion about PwMI. This scale includes 40 items rated on a five-point Likert scale from one (strongly agree) to five (strongly disagree) with four domains that is, Authoritarianism (AU), Benevolence (BE), Social restrictiveness (SR) and Community Mental Health Ideology (CMHI). Authoritarianism (AU) refers to a view of the mentally ill person as someone who is inferior and requires supervision and coercion. Benevolence (BE) corresponds to a humanistic and sympathetic view of mentally ill persons. Social Restrictiveness (SR) covers the belief that mentally ill patients are a threat to society and should be avoided. Community mental health ideology (CMHI) concerns the acceptance of mental health services and the integration of mentally ill patients in the community. Taylor and Dear report satisfactory (AU, α = 0.68) to good values (BE, α = 0.76, SR, α = 0.80, CMHI, α = 0.88) for the internal consistency of the subscales. A mean score of 25 ± was considered as a cutoff score for the interpretation based on a previous study (Vijayalakshmi et al., 2013).
In addition, socio-demographic details such as age, gender, education, marital status, employment status, religion, years of experience of working with a person with mental illness, professional qualification of the clientele, and income status of the subjects were also collected.
Data was collected by the corresponding author who was fluent in the above mentioned vernacular languages. Initially subjects were contacted, explained about the study and screened for inclusion into the study. The subjects who met the inclusion criteria were administered the CAMI tool. Data collection took approximately 25 to 30 minutes. Written informed consent was obtained from each recruited subject in the study. Any clarifications raised by participants was clarified. Ethical permission was obtained from the Institute Ethics Committee (NO. NIMH/DO/IEC (BEH.Sc.DIV)/2019), NIMHANS.
Data analysis
While continuous variables were analyzed with mean and standard deviation, for nominal and categorical variables, frequency and percentage were calculated. To find the differences between selected variables, Mann Whitney U test and to find the association Chi-square test was computed. Statistical Software for Social Sciences version 22.0, USA was used. P value was set at 0.05 with Confidence Interval (CI) of 95%.
Results
The results showed that the majority of the subjects 152 (59.4 %) were aged between 26 and 40 years of which majority of the subjects were female 66.4% (n = 170) and males were 33.6% (n = 86). Among 256 subjects, 48.8 % (n = 125) were Post-Graduates (PG) and Doctor of Philosophy (PhD) 51.2%) (n = 131). More than half the subjects 59% (n = 151) were mental health care workers and general health care workers were 7% (n = 18) and the majority 71.5% (n = 183) had more than one-year experience working with persons with mental illness. The demographic details of the subjects are described in Table 1.
Demographic details of the recruited subjects.

Study findings revealed that the subjects had a negative attitude in the domain of authoritarianism (30.54 ± 3.42) and social restrictiveness (30.18 ± 3.05). On the contrary participants had a positive attitude in the domains of benevolence (28.68 ± 3.00) and community mental health ideology (31.53 ± 3.19). The descriptive statistics of CAMI domains are described in Table 2.
Descriptive statistics of CAMI domains.

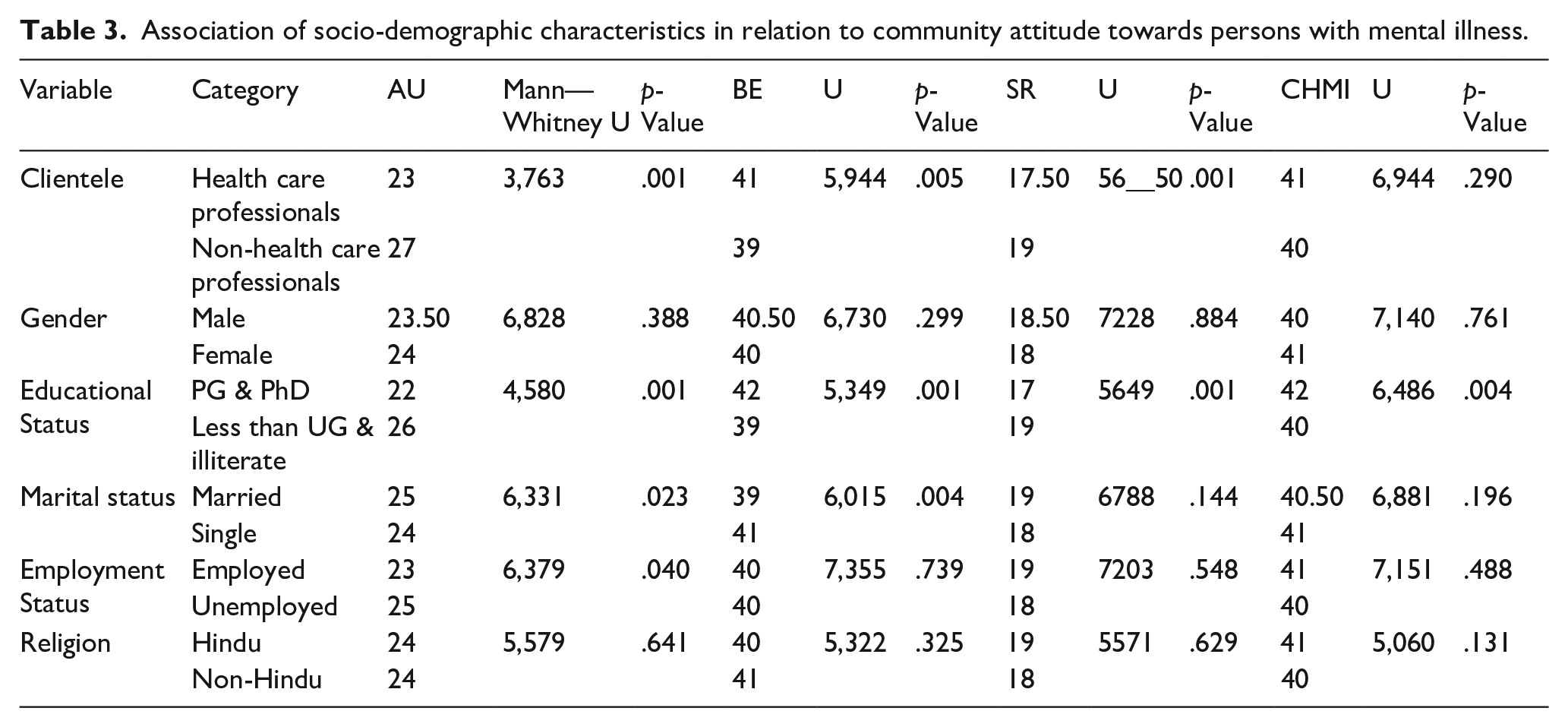
The Mann–Whitney U test was computed to know the differences among demographic details and domains of CAMI. The study results revealed significant difference in the domain of authoritarianism between health care professionals and non-healthcare professionals (U = 3763.5, p < 0.001), social restrictiveness (U = 5650, p < 0.001) and benevolence (U = 5944.00, p < 0.005), no differences were observed in the domain of community mental health ideology (U = 6944, p < 0.290).
There was significant difference between educational status and the domains of AU (U = 4580, p < 0.001), BE (U = 5349, p < 0.001), SR (U = 5649, p < 0.001) and CMHI (U = 6486, p < 0.004). There was significant difference between marital status and domains of AU (U = 6331, p < 0.023) and BE (U = 6015, p < 0.004). In addition, results revealed that there was a significant difference between employment status and domain of AU (U = 6379, p < 0.040). Table 3 showed the Mann Whitney U test results on CAMI differences between health care professional and non-healthcare professionals and their demographic characteristics.
Association of socio-demographic characteristics in relation to community attitude towards persons with mental illness.
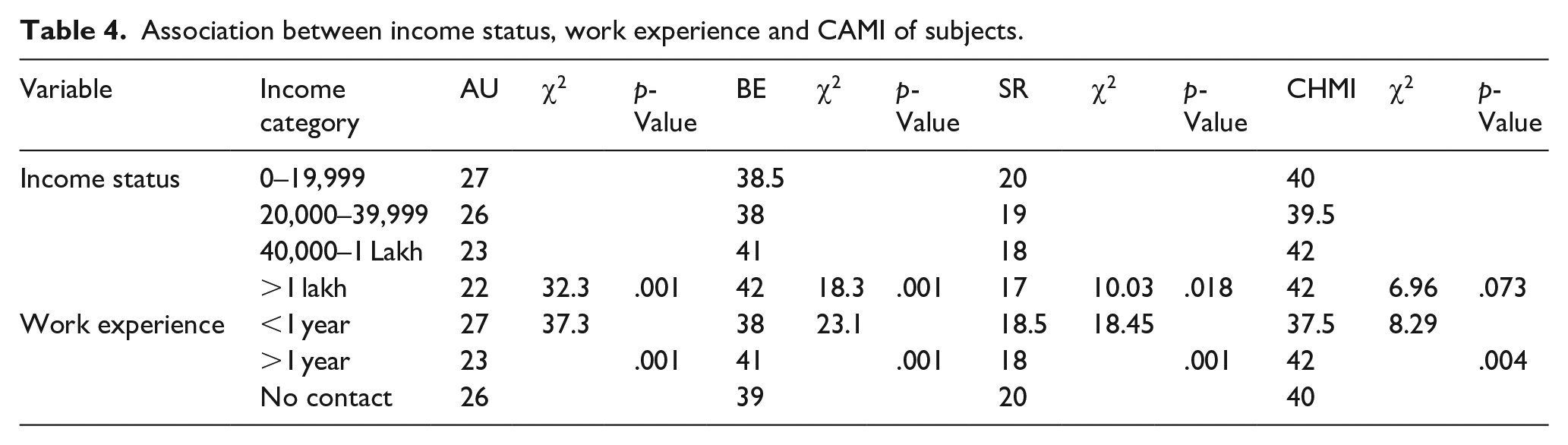
The Chi-square test was computed to see the differences between income, work experience of the subject, and various domains of CAMI. The result showed that income status was significantly associated with AU (χ2 = 32.29, p < 0.001), BE (χ2 = 18.26, p < 0.001), and SR (χ2 = 10.03, p < 0.018). Yet results also depicted that subjects work experience was significantly associated with AU (χ2 = 37.26, p < 0.001,), BE (χ2 = 23.07, p < 0.001), SR (χ2 = 18.45, p < 0.001) and CMHI (χ2 = 8.29, p < 0.004). Table 4 showed the Association between income status, work experience and CAMI of subjects.
Association between income status, work experience and CAMI of subjects.
Discussion
The current study aimed to measure the community attitude among health care workers and non-healthcare workers who were availing services of ROSes Café at PRS unit, NIMHANS. Many studies were found focusing on the various rehabilitation needs of PwMI, their caregivers, and the general public community attitude towards PwMI in general. But there are only a handful of studies which have explored the health care and non-healthcare workers attitude towards persons with mental illness. In this regard, the current study holds significance in the field of mental health rehabilitation in India.
The present study showed that participant’s age ranged between 26 to 40 years, predominantly female (66.4%) when compared to male subjects and most of them having (48.8%) completed their higher education. The findings of our study were similar reported by (Bhugra, 1989; Hannigan, 1999; Vibha et al., 2008).
In the present study, there were no significant gender-wise differences. On the contrary, review found in their study that women had a more positive attitude, were less socially restrictive and had higher benevolence toward persons with mental illness (Morrison, 2011; Poreddi et al., 2017).
The descriptive results showed that health care workers and non-healthcare workers had a mixed attitude towards PwMI, higher level of authoritarianism and social restrictiveness, they also had higher level of benevolence and good community mental health ideology. This could be because both health care workers and non-health care workers were working with PwMI and their perceptions too could have influenced the findings. The current study result was supported by the reports of the previous studies which showed that nurses who were working in the psychiatric units had more positive attitude than the nurses working in the general hospital. (Björkman et al., 2008) Another study finding reported that psychiatric ward attendants were less socially restrictive and had better community mental health ideology when compared to general ward attendants. This result reflects better community acceptance by the health care workers working in psychiatric units. (Vibha et al., 2008) Our present study findings were supported by a study conducted among medical doctors and the general population, which revealed that medical students had a better attitude than the general population. (Winkler et al., 2016) The study conducted on medical students who had their first postings in psychiatric wards had a higher level of stigmatization which was equal to the stigma level found in first-year medical students and non-medical students (Totic et al., 2012).
The study results showed that educational status, marital status, and employment status had a significant influence on the community attitude of health care workers and non-health care workers towards PwMI. Significant differences were found in the domains of AU, BE, SR, and CMHI. There was no significant difference between gender and attitude towards CMHI. In the present study, health care workers had lower authoritarianism, higher benevolence, less social restrictiveness, and better community mental health ideology towards PwMI when compared to non-healthcare workers. In contrast to our study finding, a study conducted among medical and nursing student’s attitudes towards mental illness revealed that people with mental illness encounter stigma and negative attitudes not only from the society but also from mental health care professionals. Further, nursing students had a higher benevolence towards PwMI compared to medical students (Poreddi et al., 2017).
Participants who had higher education showed lower levels of authoritarianism, better benevolence, lower levels of social restrictiveness, and better mental health ideology. Further, community attitude differed based on the employment status of participants in the domain of Authoritarianism. People who had higher education and were employed had a more positive attitude when compared to people who had less education and who were unemployed (Evans-Lacko, 2012)
Married participants had shown higher authoritarianism, lower level of benevolence, higher social restrictiveness, and lower mental health ideology when compared to single status health care and non-healthcare workers. Similar to our findings, married subjects had higher authoritarianism and negative opinion about the community mental health attitude (Vibha et al., 2008). On the contrary, a study conducted by (Wolff et al., 1996), reported that married people with children had shown a more positive attitude than unmarried people.
The study result showed that income level and work experience were significantly associated with AU, BE, SR, and CMHI. This infers that higher-income participants had lower levels of AU, higher levels of BE, and lower level of social restrictiveness, subjects with more working experience with PwMI had less levels of AU, higher levels of BE, less levels of SR and better mental health ideology. The present study goes in line with the findings which reported that individuals who had PwMI as friends and family members, had a positive attitude when compared to the subjects who never had contact with PwMI (Corrigan et al., 2001; Holmes et al., 1999; Link & Cullen, 1986; Song et al., 2005).
Future directions
The study can be replicated among the employers in a community setting and also among health care professionals in a general hospital setting where such services exist to know their perception/attitude about the working ability of persons with mental illness. Interventional studies can be conducted to create awareness among the general public and follow up can be conducted to evaluate the effectiveness of the intervention.
Conclusion
The current study explored the perception of ROSes café clientele about persons with mental illness working in the café at Psychiatric Rehabilitation Services, NIMHANS, and Bengaluru. The professionals can take a wider perspective and work towards creating awareness about mental illness, and the need to reintegrate them into the community. They may be empowered by supported employment helping them to lead a dignified life in the society.
Footnotes
Acknowledgements
Researchers acknowledge all the subjects who consented for the interview and their valuable contributions. We are thankful to the Institute Ethics committee, Department of Psychiatry and Psychiatric Rehabilitation Services, NIMHANS.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.