
Abstract
Introduction:
France has been impacted by the COVID-19 pandemic. Anxiety, depression, burn out and the high proportion of post-traumatic stress disorder proved to be the most expected troubles caused by this pandemic and the confinement. Medico-psychological emergency units (CUMP) have been solicited at the very early stage of the pandemic because CUMP units are very well known by the French government and systematically associated to emergency plans.
Methods:
In this article we describe the process which has been developed to cope with the psychological needs in the general population. At a first level, platforms of volunteers specialised into listening were available. Then those platforms could directly mobilise the CUMP in case of psychiatric disorders. It ran over the whole first wave and it has been reactivated because of the second confinement in France.
Results:
During the first wave, approximately 1% of all the calls made on the national Covid number required to be redirected to the listening platforms. Of this group, 4% were related to reactive pathology or a psychiatric decompensating that required adapted and specialised care.
Conclusion:
The high rates of psychological distress detected in the general population in recent scientific literature seem discrepant with our findings of relatively low reorientation towards the CUMP. Nevertheless, our study highlights that the response of the CUMP network in France during the first wave was supportive. The second wave displays its adaptability to the public health policies.
Introduction
Among all European countries, France has seriously been impacted by the COVID-19 pandemic with more than 3,100,000 cases confirmed and more than 74,800 deaths (results from late January; Santé Publique France, 2021). As well as other countries, French government has imposed a strict and generalised confinement in order to slow down the spread of the SARS-COV-2 Corona virus for its first wave. This first confinement lasted almost 2 months (17th of March 2020–11th of May 2020). As the circulation of the virus has run out of control again, on October the 30th the French government decided a new confinement (at least until middle December) for the so called second wave.
Meanwhile, the pandemic itself, the impact of the confinement associated with the lack of specific protections during the first wave, the growing feeling of weariness during the second one, the general communication felt as ‘being ambiguous’ or ‘inducing illogical rules’ could induce psychological repercussions or even lead to specific psychiatric disorders : anxiety, depression, burn out and the high proportion of post-traumatic stress disorder could be the most expected troubles (Brooks et al., 2020).
Medico-psychological emergency units (CUMP) have been solicited at the very early stage of the pandemic even though their specific target is trauma (terrorist attack, accidents among big communities, natural disaster) (Rerbal et al., 2017) because CUMP units are very well known by the French government and systematically associated to emergency plans combining pre-hospital and hospital emergency care. In addition CUMP units professionals are particularly experienced, specifically trained for reactive pathologies and have a very efficient territorial network also overseas in other French territories.
The medico psychological emergency units: CUMP
The CUMP units are organised structures that have been created over the full French territory and put in place in 1997 after the terrorist attacks in Paris in 1995. Integrated into the pre-hospital emergency medical services (SAMU) of each French province, they are composed of psychiatrists, psychologists, specialized nurses in psychiatry and could be quickly mobilised on site at a very early stage with the SAMU units and are able to cover the medical psychological support needed on a short to middle term.
The alert and the mobilisation of the CUMP is always done through the SAMU via a call centre that regulates the emergency phone calls (dial 15). This number (dial 15) is the same over the full French territory but is allocated to each province locally. This way the response to an emergency situation can be quickly made on site through a medically equipped vehicle (SMUR). This response matches the French civil pre-hospital emergency medical service (Carli et al., 2003; Figure 1).
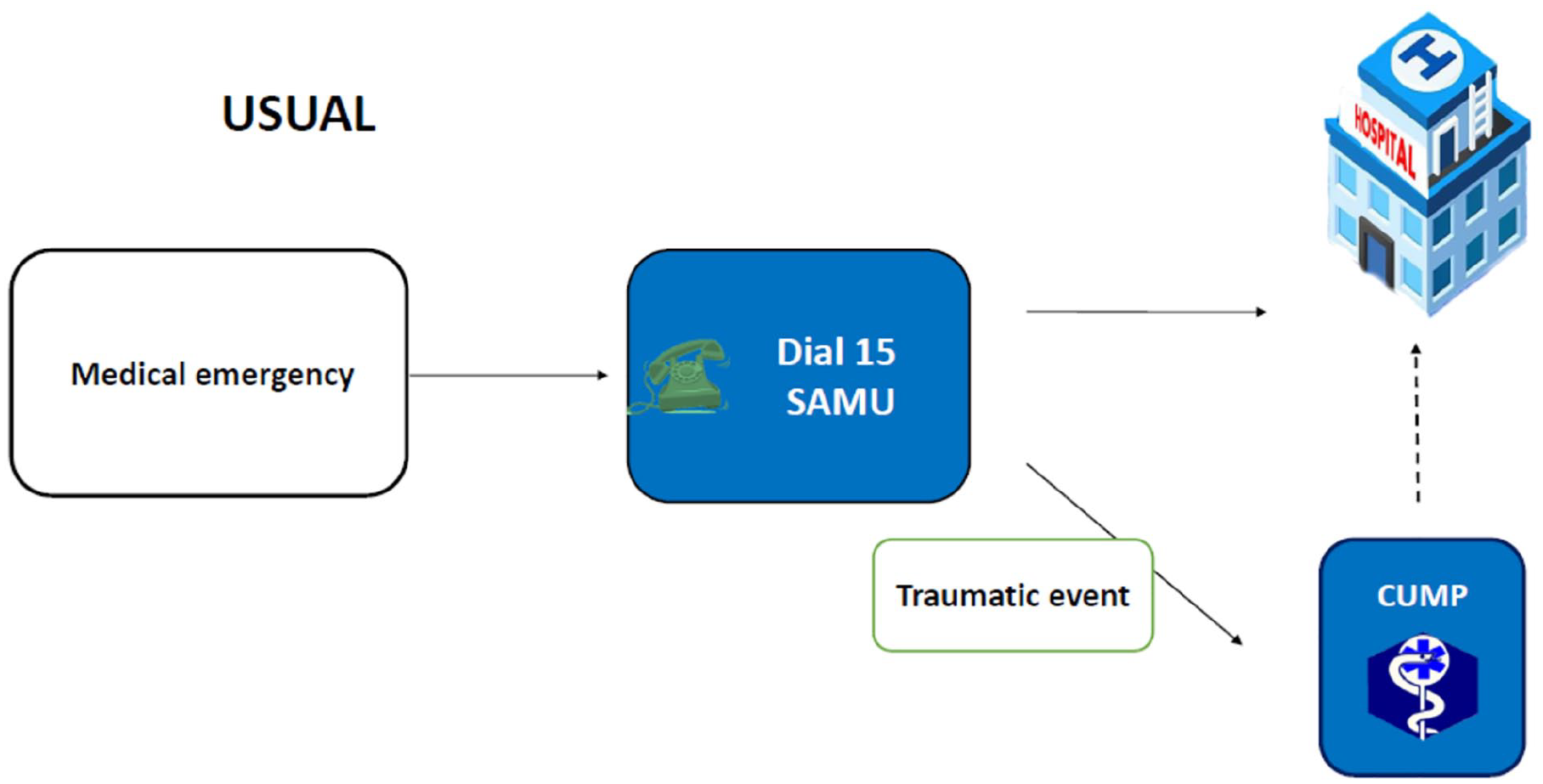
Incoming calls on the 15.
Incoming calls on the 15 and the green line number free of charge
In this particular crisis of the COVID-19, the call centre of the 15 has quickly been saturated due to the magnitude of this pandemic and because the first recommendations were to dial 15 in case of COVID-19 symptoms, when actually the majority of the calls were very often related to anxiety caused by the pandemic or for seeking information regarding the Coronavirus.
On another hand, a green line number, free of charge, has been created by the government over the French territory specifically for COVID-19 related matters. But quickly this green line also encountered a lot of calls for psychological troubles. Then the CUMP were solicited for this kind of calls but as mentioned previously the only formal way of mobilising the CUMP is through dialing the 15. This was a problem to solve.
The innovation in the COVID-19 response by the CUMP has been the creation of a relay using the platforms of volunteers specialised in listening (such as the Red Cross listening, and later by other similar platforms). This way the Red Cross could directly mobilise the CUMP on bigger geographic zones than provinces to simplify the process. This has been based on the hypothesis that a minority of cases would be related to reactive pathology or psychiatric decompensation. This hypothesis proved to be correct. This process required a close collaboration between the CUMP, the Red Cross, knowing that volunteers from the Red Cross have a huge experience of listening and have been trained since many years. For this partnership a proper training given by the CUMP, has allowed to easily identify cases thanks to a codified process: using standardised worksheet inspired by the Depression and Anxiety Stress Scale 21 (DASS 21) (Lovibond and Lovibond, 1995a, 1995b). Also those volunteers from the listening platforms had a specific awareness to detect immediate emergencies (such as suicides, serious behaviour problems) to redirect the calls on the 15 number as usual (Figure 2).
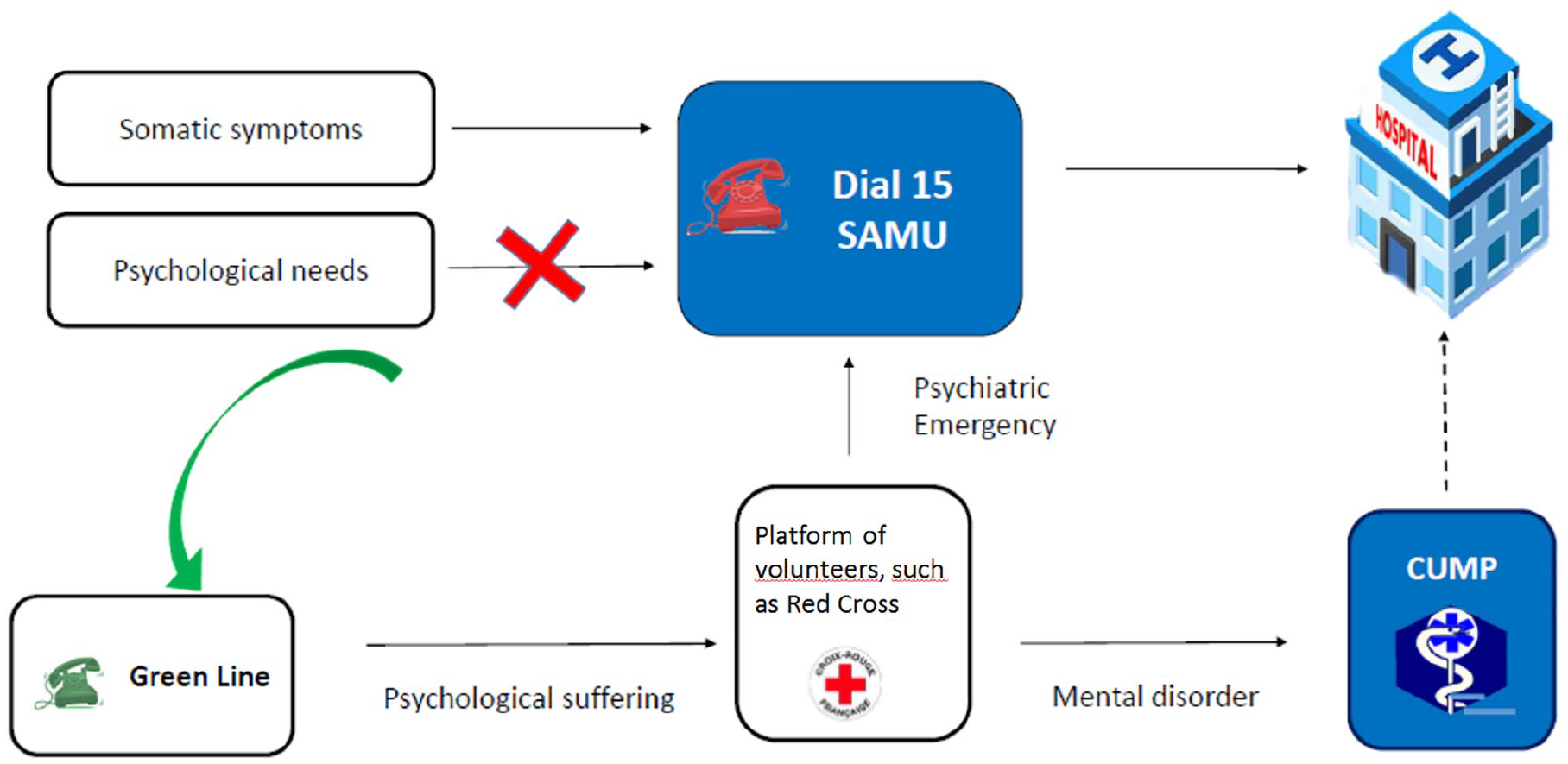
Specific process for COVID-19.
An innovative system for supporting a psychological distress on the general population
The CUMP have worked locally to take care of the COVID-19 infected patients, bereaved families and also affected professional caregivers. However, it’s on a national level and for the general population that this measure has got its most important effect. On the one hand it allowed to considerably discharge the 15 call centre; on the other hand, it sorted efficiently out the calls that were only related to minor anxiety from the ones that required a psychiatric care or even an emergency treatment.
During the first wave, the result showed that among all the 892,143 calls made on the national Covid number (various information, request information related to employment during confinement), 8496 (0.95%) required to be redirected to the listening platforms and among this 1%, 357 (4.2%) were related to reactive pathology or a psychiatric decompensating that required adapted and specialised care.
The confinement related to the second wave started on October the 30th and should run at least until middle December. It could last longer, depending on how the circulation of COVID-19 slows down in the French territory. Thus, the French Ministry of Health wanted this psychological platform to be open again and it could be reactivated very quickly.
To conclude, two important aspects should be highlighted. Firstly, during the first wave, the high numbers of psychological troubles detected in the general population during the COVID-19 pandemic and the confinement in the scientific literature (Brooks et al., 2020; Gandré et al., 2020) seem to be contradicting the low reorientation towards the CUMP, only 4% observed in our survey. It therefore appears that despite the significant psychological stress posed by COVID-19 to the general population, our findings suggest that the case-burden is not as severe as reported by cross-sectional population studies and that the distress did not very often require specific psychiatric treatment. Alternatively, this discrepancy may represent a gap between those experiencing psychological distress and those seeking help. The question whether the second wave will display similar results is of interest. Secondly, not only does the response of the CUMP network seem appropriate to the psychological needs of the general population in the COVID-19 pandemic, but it has also displayed a crucial reactivity in the context of the current second wave. This would deserve to be greatly known and to inspire health care policy for other countries and possible supplementary waves.
Footnotes
Author contributions
NP wrote the first draft of the manuscript. NP and PV managed the literature searches. RD and EC performed every figures and table. JMP corrected the first draft. All the authors contributed to the final manuscript and all authors approved it.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.