
Abstract
Background:
The suicide rate among adolescents around the world has increased rapidly. There are many risk factors for attempting suicide, but not all have been clarified yet. Therefore, it is very important to identify risk factors. This study evaluated adolescents with a history of suicide attempts and their association with chronic diseases. Besides, to check whether they attempted suicide multiple times. Other clinical features related to multiple suicide attempts were investigated.
Method:
This study used a multicentre, retrospective cross-sectional design; 253 adolescents admitted to emergency departments in 2019 for suicide attempts were evaluated.
Results:
Adolescents with chronic disease were at greater risk for both single and multiple suicide attempts and patients had a 6.14 times higher risk of multiple attempts (p = .013). The likelihood of multiple attempts did not differ according to the presence of somatic or psychiatric disease. Multiple attempters were more likely to poison themselves with their therapeutic drugs (p = .002).
Conclusion:
When adolescents with a chronic disease present to the emergency services after a single suicide attempt using their therapeutic drugs, families should be informed regarding the potential for further attempts.
Introduction
One of the most important issues in society today is suicide and it is an important public health problem worldwide (Carballo et al., 2020). Suicide is the fourth leading cause of death among 15–19-year-olds and 77% of global suicides occur in low- and middle-income countries (World Health Organization [WHO], 2021). Suicidality risk is multifactorial and risk factors include chronic psychiatric health problems (such as depression, anxiety, bipolar disorder, substance use disorders, etc.), a previous suicide attempt and family history of suicide (Shain, 2016; Slap et al., 2001). Studies have shown that chronic somatic diseases such as chronic pain, cancer, coronary heart disease and asthma are associated with suicide and that having more than two physical diseases increases suicide mortality (Ahmedani et al., 2017; Greydanus et al., 2010; Juurlink et al., 2004; Ravaioli et al., 2020; K. M. Scott et al., 2010).
In adolescent studies, it is indicated that children with neurological diseases such as epilepsy had greater odds of bipolar disorder, psychosis and suicide attempt/ideation (Thibault et al., 2016). Moreover, there are studies showing that the presence of disease of any organ or physical system significantly increases the risk of subsequent suicide, regardless of gender, individual psychiatric background or socio-economic status (Qin et al., 2013).
In adolescents, self-poisoning is the most common method of suicide (Canner et al., 2018). Children with a chronic disease are usually on one or more medications and in the USA nearly one in five children use medication and 9% receive more than two medications (Hales et al., 2018). As a result, adolescents with a chronic disease can access medicines easily and these are used for suicide attempts.
This study aimed to establish the underlying risk factors for adolescent suicide attempts. Patients with and without a chronic disease who presented to paediatric emergency departments after suicide attempts were compared, examining whether adolescents attempted single or multiple suicides and also noting other clinical features.
Materials and methods
Data sources and management
The study was a multicentre, retrospective cross-sectional, medical record-based study of paediatric patients admitted to <<city name>>Education and Research Hospital and <<hospital name>>Training and Research Hospital Paediatric Emergency Department for suicide attempts with self-poisoning in 2019. Our institutional ethics committee approved this study (Decision number: 2020-309). Adolescent patients aged 10 to 18 years were included in the study.
In the hospitals where the study was conducted, only the cases with poisoning as a cause of suicide attempts are accepted to the paediatric emergency services. Adolescents who attempt suicide due to other traumatic causes, such as firearm injuries, hanging and motor vehicle accidents, are monitored and treated by the trauma department in the adult emergency services. All poisoning cases are accepted as forensic cases in the emergency departments in our country and forensic case reports are compiled by specialist doctors. In paediatric emergencies, the reports are compiled by paediatricians.
In cases of poisoning admitted to the paediatric emergency department there is also sub-diagnosis, such as drug poisoning and exposure to other chemicals or pesticides. Cases of self-poisoning were classified using ICD-10 codes X40 (unintentional) and X60 (intentional self-poisoning). Medical records of patients were assessed through the system. Based on the statements of adolescents and according to the ICD-10 codes in the system, it was decided whether they attempted suicide or not, and if so they were included in this study. Such evaluation was made by paediatricians at the hospitals where the study was conducted. The following individuals were excluded from study: those thought to have taken medication by mistake; cases not considered to be suicide attempts; and diagnostic cases falling under various ICD-10 chapter headings (Chapter XV, pregnancy and childbirth; Chapter XVI, certain conditions of the prenatal period; and Chapters XIX and XX, covering all accidental poisoning).
The demographic characteristics of the cases were obtained from the electronic medical records, including age, gender, marital status, educational attainment, social/legal problems and substance use. Substance use was considered if the substances were found in urine drug level laboratory tests. Urine screening was not performed for all poisoning cases and focused on the identification of substances such as opiates, opioids, cocaine and amphetamine derivatives. Cases that required a high level of care in the intensive care unit or that died by suicide were recorded.
The presence of chronic disease was checked for in all cases. Chronic, non-communicable diseases were classified as psychiatric or somatic. Patients without a chronic disease were classified as having no chronic disease. The number of suicide attempts was also recorded. Patients were classified as a single attempter (SA) if they had made only one suicide attempt and as a multiple attempter (MA) if they had made more than one suicide attempt.
Regarding self-poisoning, the patients were divided into two groups: those who attempted suicide with drugs prescribed for their chronic diseases were classified into the Own medication group; those who used the drugs of another person in the household comprised the Someone else’s medication group.
Statistical analysis
The statistical analyses were performed using SPSS software (version 21.0; IBM Corp., Armonk, NY, USA). The normality of the data was tested with the Shapiro–Wilk’s test. Numerical variables are expressed as the mean ± standard deviation (SD). Groups with normally distributed data were compared using Student’s t-test whereas groups with non-normally distributed data were compared using the Mann–Whitney U test. Categorical variables were compared using the chi-square (χ2) test. Univariate logistic regression analyses were performed and p ⩽ .05 indicated statistical significance.
Results
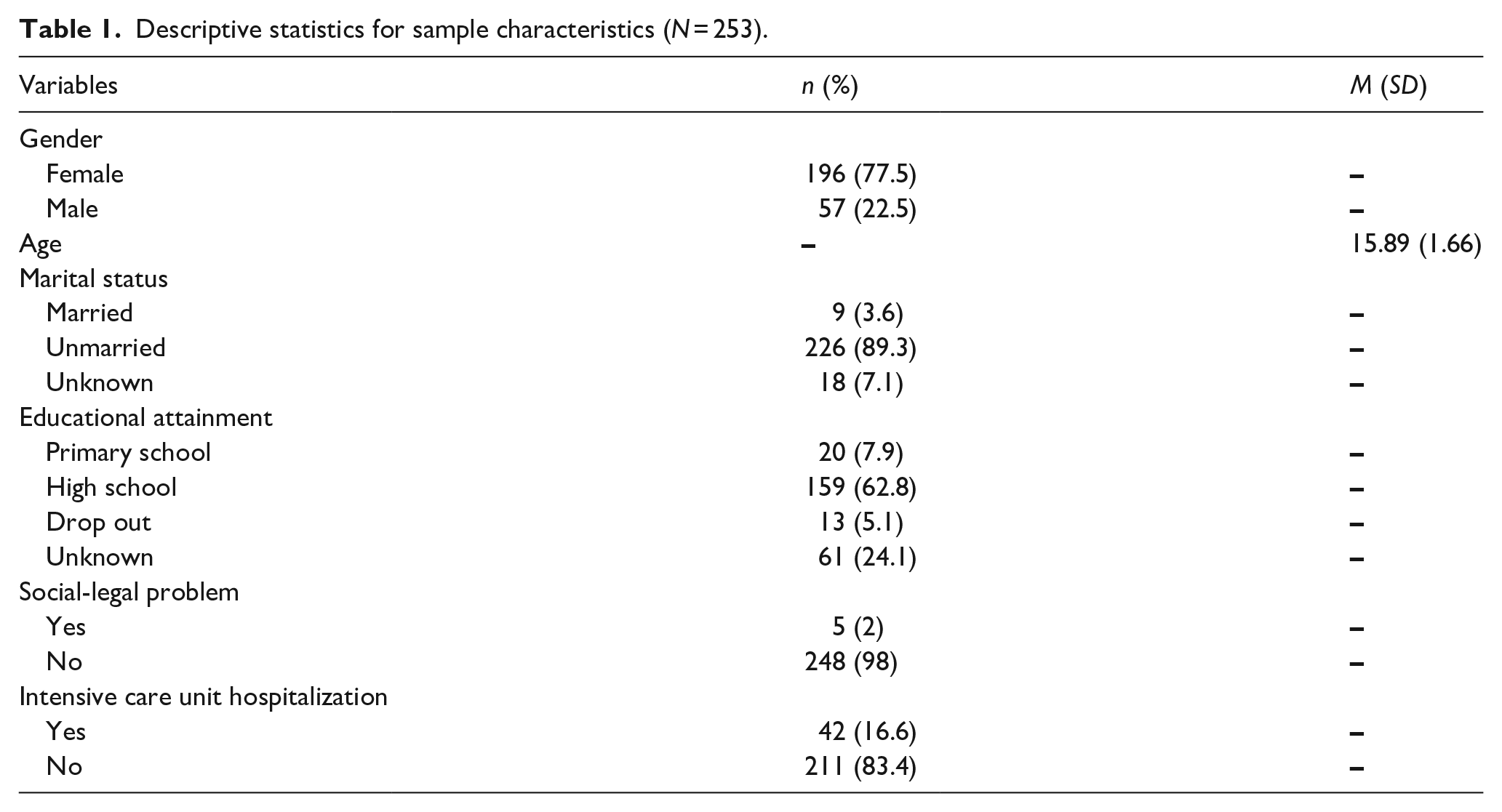
The sociodemographic and clinical characteristics of the patients are summarized in Table 1. It was found that approximately 2% of the patients abused substances. Death due to suicide occurred in 1 of 253 cases (0.4%). Of the patients, 227 (89.7%) made a single suicide attempt and 26 (10.3%) made multiple attempts. Age, gender, marital status, social/legal problems, intensive care unit hospitalization and education status were not associated with the number of suicide attempts (p > .05).
Descriptive statistics for sample characteristics (N = 253).
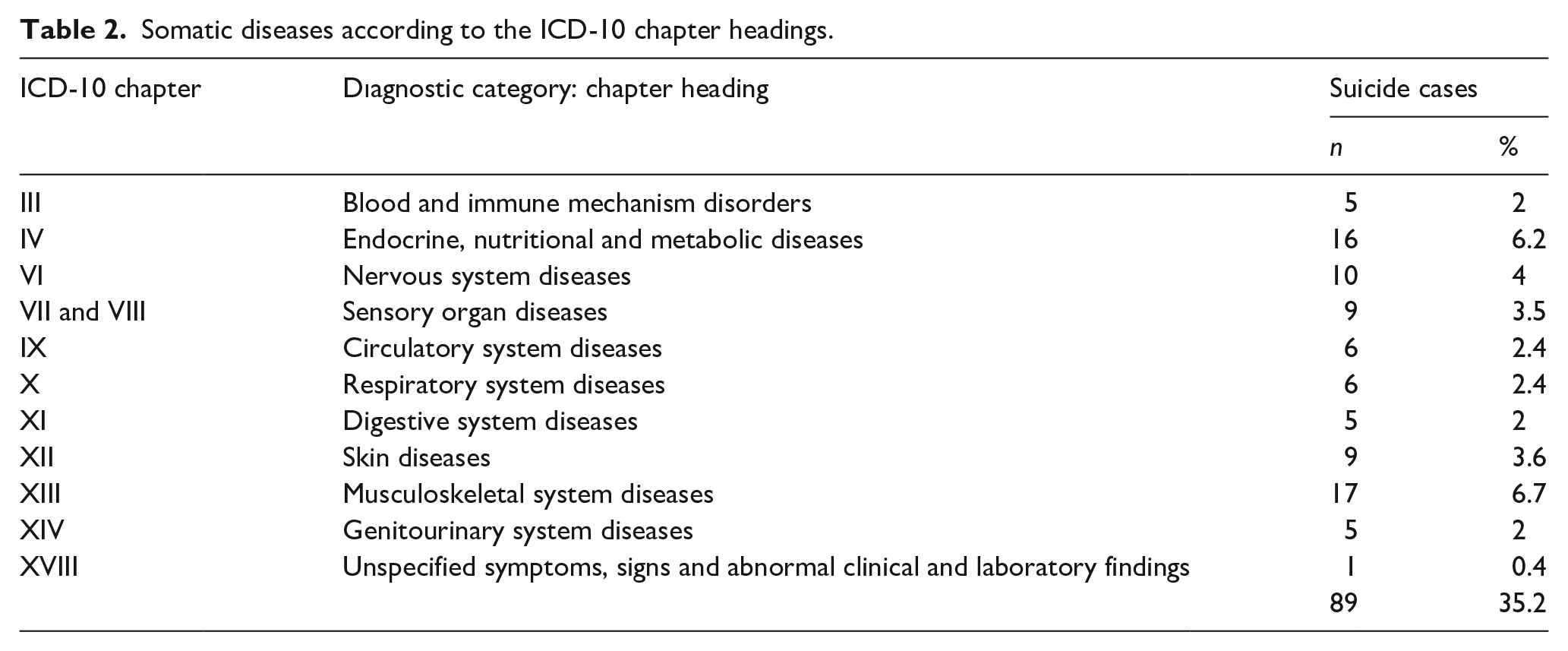
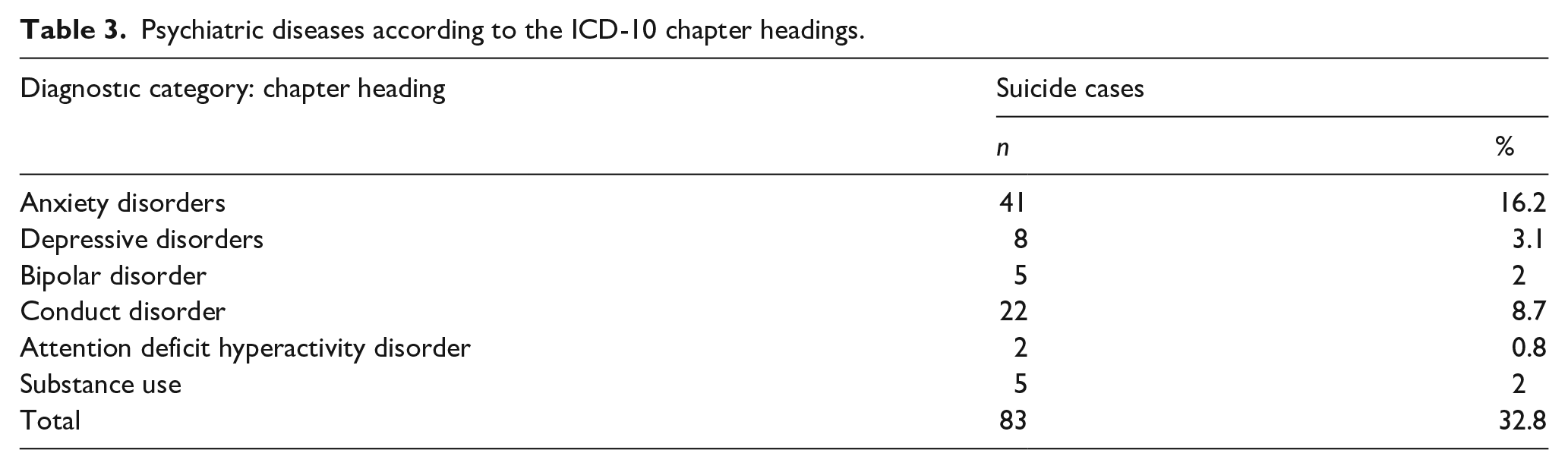
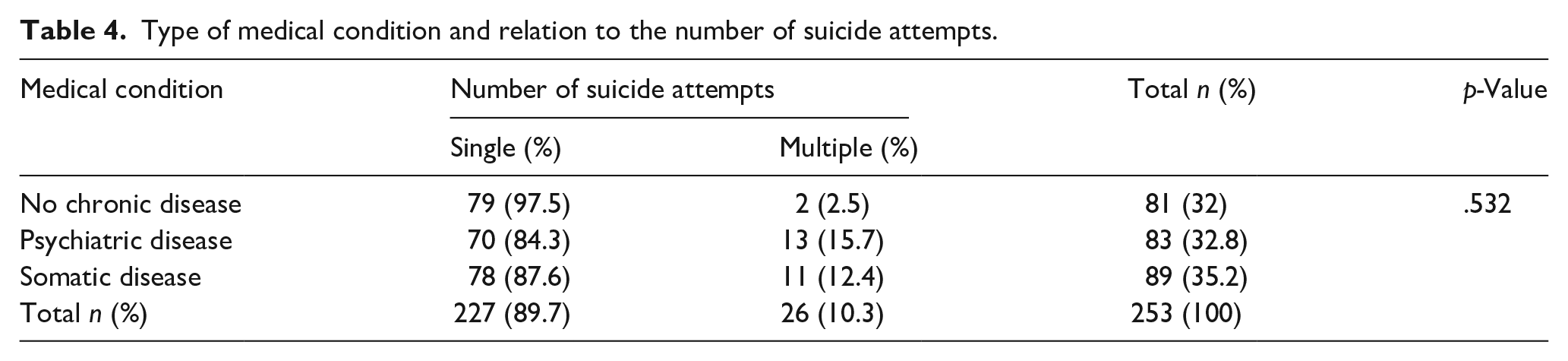
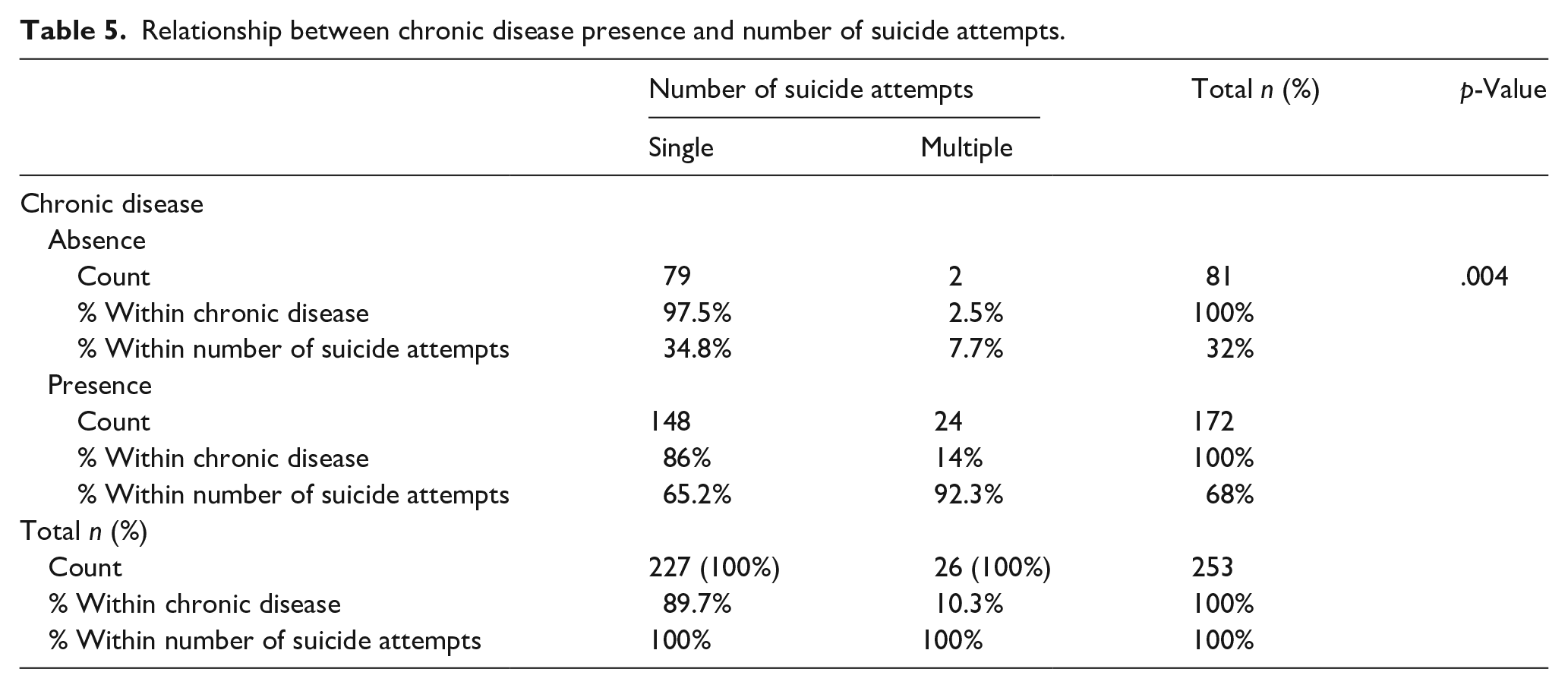
Chronic disease was detected in 172 (68%) patients: 35.2% had a somatic disease and 32.8% had a psychiatric disease. Tables 2 and 3 summarize the somatic and psychiatric diseases, respectively, along with the relevant ICD-10 chapters. Musculoskeletal, endocrine, nutritional and metabolic diseases were among the most common somatic diseases whereas anxiety and conduct disorders were among the most common psychiatric diseases. Table 4 summarizes the relationship between medical condition and the number of suicide attempts. There was no statistically significant difference between the proportions for no chronic disease, psychiatric disease and somatic disease (p = .532). Table 5 summarizes the relationship between the presence of chronic disease and the number of suicide attempts; 65.2% of the SAs and 92.3% of the MAs had a chronic disease. The presence of chronic disease in the patients was significantly associated with suicide attempts in both SAs and MAs, regardless of the type of disease (p = .004). Additionally, we also evaluated the relationship between chronic disease presence and the number of suicide attempts. Using univariate logistic regression analysis, the patients with chronic disease had a 6.14-fold higher risk of multiple attempts compared with those with single attempts (p = .013; 95% CI [0.036, 0.678]).
Somatic diseases according to the ICD-10 chapter headings.
Psychiatric diseases according to the ICD-10 chapter headings.
Type of medical condition and relation to the number of suicide attempts.
Relationship between chronic disease presence and number of suicide attempts.
The number of suicide attempts was also evaluated according to drug group, as shown in Table 6. The majority of patients in the SA group attempted suicide with someone else’s medication (79.3%). In contrast, in the MA group, 50% of patients attempted suicide with their own medication. It was found that those who attempted suicide with both their own and someone else’s medicine were more likely to attempt suicide once (p = .002).
Number of suicide attempts and relation to drug groups.
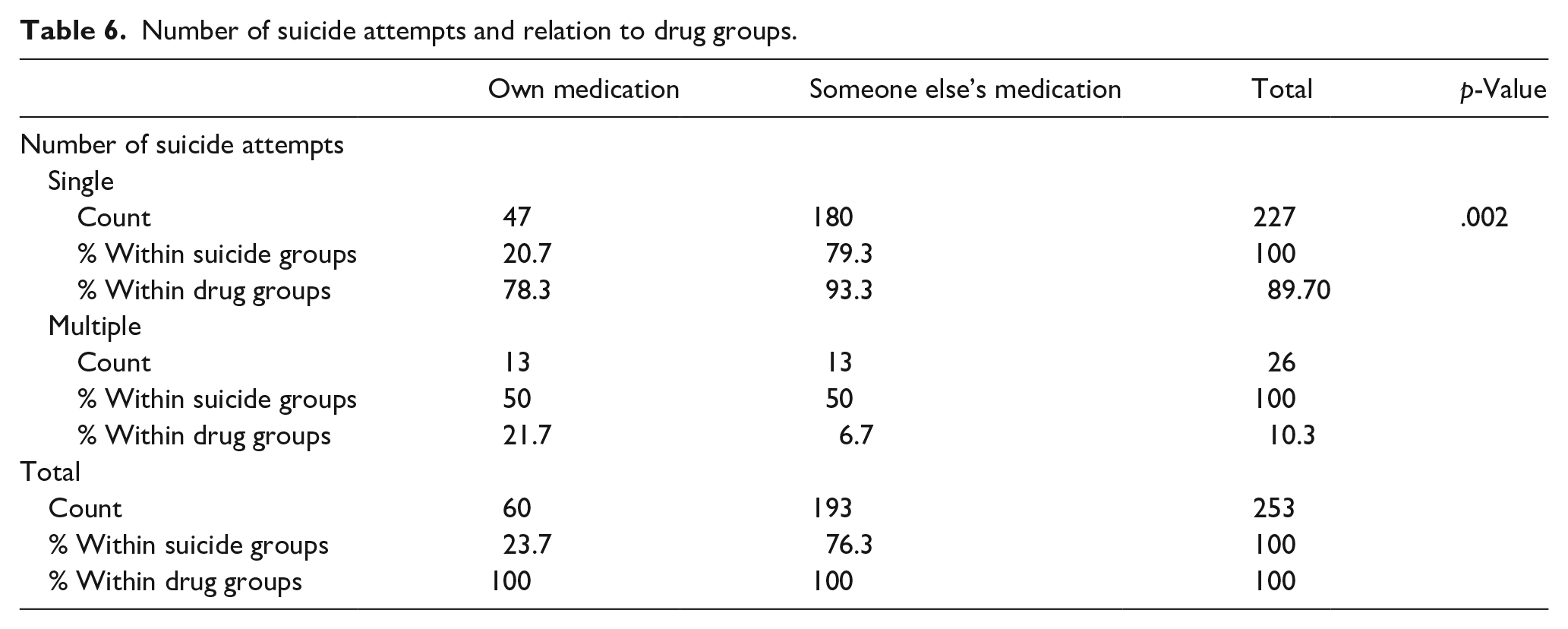
According to drug group, when the cases of suicide attempts were evaluated it was found that 60 (23.7%) attempted suicide with their own treatment drug, 193 (76.3%).
In Someone else’s medication group (193 patients) there were 180 patients (93.2%) who were SAs. Of the 227 patients in the SA group, 180 (79.3%) attempted suicide with someone else’s medication and 47 (20.7%) attempted with their own medication.
On the other hand, in the MA group 13 patients (6.7%) attempted suicide with someone else’s medication and 21.7% attempted with their own drugs; the difference was significant (OR = 3.83, 95% CI [1.66, 8.81], p = .002).
Discussion
The main result of the present study was that having a chronic disease increases suicide rates regardless of the number of suicide attempts. Over 20 years, it is known that chronic disease and poor physical health increased suicidal thoughts directly or indirectly. Having a chronic disease increased the feelings of lack of control, hopelessness/entrapment and pain intolerance, while also negatively impacting coping (Joiner, 2007; O’Connor & Kirtley, 2018). It has been shown that suicide attempts increase in children with psychiatric or chronic somatic diseases, but the surprising part of this study is that having a somatic disease is a risk factor for suicide as well as psychiatric disease. It is believed that patients with psychiatric diseases are more likely to attempt suicide (Chou et al., 2016; Dickerson Mayes et al., 2015; Goldston et al., 2009; Halfon et al., 2013), but the reported suicide rates among those with psychiatric and somatic diseases are very similar to our findings, especially in MAs.
A previous suicide attempt is the most important indicator of future attempts (Ribeiro et al., 2016), but not all suicide cases attempt multiple times. Some studies have examined the relationship between adolescent chronic diseases and multiple suicide attempts, finding that patients with physiological and functional impairment were more likely to be MAs (Defayette et al., 2020; Payne et al., 2009; Vajda & Steinbeck, 2000). In the present study, it was found that if an adolescent has a chronic somatic disease and has attempted suicide once, there is an increased risk of multiple attempts.
When the literature was reviewed, it was seen that the suicide attempt is associated with a specific disease (Ikeda et al., 2001; Wang et al., 2009). It was shown in this study that the main risk factor for a suicide attempt is the presence of any chronic disease, not the specific type of disease (somatic or psychiatric). This may be due to a reduction in the ability of children with chronic disease to cope, either due to pain or because adolescents are more vulnerable to chronic disease-related stress (Dean-Boucher et al., 2020). If a disease in an adolescent causes social isolation or prevents communication with peers, they may feel hopeless and lacking in control and thus may be more vulnerable than their peers to suicidal thoughts and behaviours (Sawyer et al., 2007; Suris et al., 2004).
One of the reasons for the low number of MAs among our patients with no chronic disease might be related to the patterns of suicidal behaviour seen in adolescents. Childhood traumatic experiences and impulsive behaviour are powerful determinants of suicidal ideation in teenagers (Koyama et al., 2020), therefore adolescents with no underlying disease may make a single attempt secondary to impulsive behaviour.
This study analysed adolescents with chronic diseases from a novel perspective. Self-poisoning is the most common method of suicide in adolescence, making adolescents a high-risk target group for secondary prevention (Geulayov et al., 2019; Hawton et al., 2020; Suris et al., 2004). Suicide risk is increased for many years after the first suicide attempt, therefore sustained prevention efforts are very important (Finkelstein et al., 2015). Many studies have shown that children and adolescents with a chronic disease need pharmacotherapy and long-term treatment (Merandi et al., 2017; Rappaport et al., 2011). In this study, it was found that SAs performed suicide attempts with drugs belonging to other people in their household, whereas 3.83-fold more MAs than SAs attempted suicide with their own medicines. Therefore, adolescents with a chronic disease who receive pharmacotherapy and attempt suicide should be followed closely due to the risk of additional suicide attempts. Families of adolescents should perhaps supervise the ingestion of therapeutic drugs. If parents use medications for chronic disease, they should take precautions to prevent easy access to these medicines for their adolescent children. When adolescents present to the emergency services with a single suicide attempt and have a chronic disease, especially if they have attempted suicide using their own therapeutic drugs, emergency doctors should inform their families about the risk of additional suicide attempts. Before discharging the patient, the paediatrician and parent should discuss a safety plan and review how to safely store the medicines (J. Scott et al., 2018). It can be life-saving for families to have information on how adolescents use their medicines and to be warned about the storage of medicines (Horowitz et al., 2020).
Limitations and future directions
The main limitation of this study is that it is a retrospective, cross-sectional study and the case details extracted from the clinic’s database cannot be verified in terms of data accuracy. Also, the sample size was not very large and only the self-poisoning cases were included. Further studies should investigate all suicide cases, including other traumatic causes such as firearm injuries, hanging and motor vehicle accidents. Despite these limitations, the relative strength of this study was that it was found to be a new risk factor for suicide in adolescents with a chronic disease and taking medication.
Conclusions
Paediatricians play an important role in preventing adolescent suicides. Paediatric emergency departments are pioneering ways to successfully identify and manage suicide risk. Adolescents with a chronic disease who receive pharmacotherapy and attempt suicide should be followed closely due to the risk of additional suicide attempts. It can be life-saving for paediatricians to pay attention to this detail.
Footnotes
Acknowledgements
Our warmest thanks go to Başak N Akyıldız for encouraging us to conduct this study. We also thank Gamze Talih, Şaban Tubaş, Aydın Esen, Esra Ermiş Turak and Fırat Demirci for their help.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.