
Abstract
Background:
There is a current crisis in children’s mental health. Defining social determinants of mental health (SDMH) facilitates investigations of social impact on mental health.
Aims:
To examine associations between nine SDMH and adolescent depression and anxiety in a U.S. nationally representative sample.
Methods:
Poor access to health care, caregiver underemployment, food insecurity, poorly built environment, housing insecurity, household dysfunction adverse childhood experiences (ACEs), racism, caregiver poor education, and poverty/income inequality were assessed from the 2018 to 2019 National Survey of Children’s Health (NSCH) (N = 24,817).
Results:
The likelihood of reporting adolescent depression and/or anxiety was assessed for each SDMH using multinomial logistic regressions. All SDMH, besides caregiver underemployment, were associated with increased odds of reporting adolescent anxiety, depression, or anxiety and depression. Only household dysfunction ACEs and racism had statistically significant associations for all three mental health outcomes.
Conclusions:
Interventions targeting ACEs and racism may be more impactful in mitigating mental health challenges associated with SDMH during adolescence. The NSCH may provide an important public health tool to investigate SDMH in children.
Between 2016 and 2020, diagnoses of anxiety and depression in children have increased significantly while caregiver emotional well-being has worsened (Lebrun-Harris et al., 2022). Correspondingly, there have been increasing rates in suicidal thoughts and behaviors among adolescents (Ivey-Stephenson et al., 2020). During adolescence, higher-order cognitive functioning and emotional regulation undergo a period of critical development (Larsen & Luna, 2018). Exposure to adverse conditions and experiences during these sensitive periods increases the risks of emotional dysregulation and chronic health conditions (Allen et al., 2014; Graf et al., 2021). Suffering through adverse childhood experiences (ACEs) during adolescence has been associated with worse outcomes than other periods of childhood (Andersen, 2021).
Social determinants of health are social and structural factors that influence health (World Health Organization, 2008). Effective understanding of social determinants enables impactful patient-level and community-level interventions (Hohl et al., 2019; Marchis et al., 2019). Defining social determinants of mental health (SDMH) facilitates efforts to address pervasive contextual challenges and inequities associated with poor mental health. Compton and Shim (2015) undertook this task and defined the nine core SDMH: (1) poor access to care, (2) un/underemployment, (3) food insecurity, (4) poorly built environment, (5) housing insecurity, (6) adverse early life experiences, (7) discrimination/social exclusion, (8) poor education, and (9) poverty/income inequality (Compton & Shim, 2015). Within their biopsychosocial pyramid model, the SDMH are directly influenced by healthcare systems, health policy, and distribution of opportunity, and directly influence behaviors, opportunities, stress, genetics, and injury, ultimately leading to worsening of mental health, disease, and mortality.
Individually, SDMH’s association with poor mental health outcomes are clear (Braveman & Gottlieb, 2014; Singh et al., 2017). Compton and Shim’s (2015) framework warrants further investigation on the impact of the core SDMH on the mental health of adolescents (Jeste & Pender, 2022). In our study, we investigated the association between the nine core SDMH and depression and anxiety in a United States nationally representative sample of adolescents.
Methods
Data were extracted from the 2018 to 2019 waves of the National Survey of Children’s Health, a nationally representative parent-proxy survey of non-institutionalized children ages 0 to 17. The comprehensive methodology report can be found online (U.S. Department of Commerce, 2019). Our analysis utilized 24,817 surveys of adolescents between ages 12 and 17 and was determined exempt by our academic Institutional Review Board.
SDMH and mental health outcomes
See the Supplemental Material for the complete outcome documentation. Caregiver underemployment was defined as unemployed caregivers for at least 50 of the last 52 weeks. Lower caregiver education was defined as caregivers’ education being less than completing high school. Food insecurity was defined as the household was either often or sometimes not able to afford enough to eat in the past year. Poorly built environment was defined as two or more detracting features or two or fewer positive features of seven neighborhood features. Housing insecurity was defined as mold or mildew inside the home or pesticide use once a week or more in the past year. Household dysfunction ACEs were defined as if at least two of the six items were reported. Racism was defined as the child was ever discriminated against based on race/ethnicity. Poverty was defined as very hard to cover the basics on the family’s income since the child was born or the family received any one of four cash and food assistance programs in the past year. Poor access to healthcare was defined as the child needed to see a healthcare provider but could not or the child was not covered by insurance in the past year. Mental health outcomes were defined as if a healthcare provider ever said that the child had depression and/or anxiety.
Analysis
Accounting for the complex survey design, weighted proportions of SDMH were summarized for each composite outcome. Using R 3.6.3, the outcomes were regressed against each social determinant of mental health, individually using a multinomial logistic regression model. Odds ratios (OR) and 95% confidence intervals were obtained.
Results
Participants were 49.8% White and 85.3% spoke English as their primary language. Full demographics are reported elsewhere (Data Resource Center for Child & Adolescent Health, 2022). Between 0% and 5% of responses for each SDMH were removed due to missing data. Table 1 details the likelihood of having anxiety, depression, or depression and anxiety with each SDMH exposure. Increased likelihood of reporting anxiety (p < .05) was associated with housing insecurity (OR = 1.49; 95% CI = 1.05–2.12), poor access to health care (OR = 1.53; 95% CI = 1.24–1.88), racism (OR = 1.57; 95% CI = 1.11–2.23), and two or more household dysfunction ACEs (OR = 1.59; 95% CI = 1.22–2.07). Increased likelihood of reporting depression (p < .05) was associated with poverty (OR = 2.02; 95% CI = 1.31–3.12), experienced racism (OR = 3.58; 95% CI = 1.75–7.34), food insecurity (OR = 4.3; 95% CI = 1.89–9.79), and two or more household dysfunction ACEs (OR = 4.97; 95% CI = 3.06–8.06). Increased likelihood of reporting anxiety and depression (p < .05) was associated with poorly built environment (OR = 1.29; 95% CI = 1.06–1.59), poverty (OR = 1.62; 95% CI = 1.32–1.98), housing insecurity (OR = 1.64; 95% CI = 1.27, 2.11), caregiver underemployment (OR = 1.83; 95% CI = 1.39–2.41), poor access to health care (OR = 1.83; 95% CI = 1.49–2.24), experienced racism (OR = 2.57; 95% CI = 1.66–3.95), food insecurity (OR = 2.65; 95% CI = 1.86–3.76), and two or more household dysfunction ACEs (OR = 4.47; 95% CI = 3.57–5.6).
Social determinants of mental health association with adolescent anxiety and depression from the National Survey of Children’s Health 2018 to 2019 (N = 24,817).
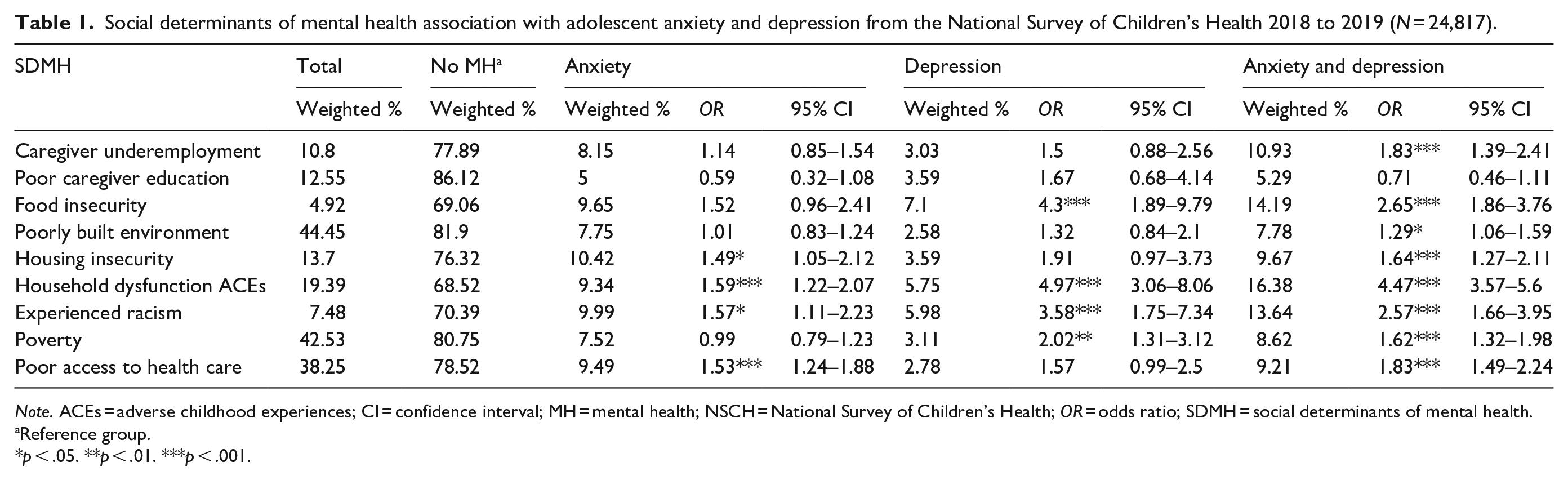
Note. ACEs = adverse childhood experiences; CI = confidence interval; MH = mental health; NSCH = National Survey of Children’s Health; OR = odds ratio; SDMH = social determinants of mental health.
Reference group.
p < .05. **p < .01. ***p < .001.
Discussion
Besides poor caregiver education, all other SDMH captured in the NSCH were associated with adolescent anxiety and/or depression. Addressing mental health inequities requires comprehensive biopsychosocial understanding and management from childhood. Our findings demonstrate mitigating childhood trauma and racism may provide the greatest benefit to adolescent mental health. Community collaborative healthcare models, with mental health integration, can both address community-specific SDMH and treat its mental health consequences, particularly in diverse communities (Rafla-Yuan et al., 2022).
Several limitations exist within the NSCH dataset when assessing SDMH. Social and structural challenges and mental illness exist in a cyclic relationship and the NSCH’s cross-sectional study design cannot infer causal relationships (Alegría et al., 2018). Caregivers’ education level influences their children’s education level; however, it may be an inappropriate proxy to assess their children’s education as a SDMH (Dubow et al., 2009). Caregiver underemployment, the other caregiver proxy question, may be too closely related to adolescents’ experiencing poverty. Childhood abuse and neglect ACEs were not assessed in the NSCH and have been shown to have more significant impact on mental health than household dysfunction ACEs (Negriff, 2020). The NSCH also does not include housing insecurity questions on experiencing homelessness, which is strongly associated with serious mental illness (Greenberg & Rosenheck, 2008).
The NSCH could provide an important dataset to investigate associations of social determinants in children, however, more work is needed to strengthen the questionnaire to better assess for social determinants. Future work with the NSCH could be used to understand SDMH clusters, necessary to efficiently combat mental health and health disparities associated with social determinants (Jeste & Pender, 2022).
Supplemental Material
sj-docx-1-isp-10.1177_00207640221119035 – Supplemental material for Social determinants of mental health and adolescent anxiety and depression: Findings from the 2018 to 2019 National Survey of Children’s Health
Supplemental material, sj-docx-1-isp-10.1177_00207640221119035 for Social determinants of mental health and adolescent anxiety and depression: Findings from the 2018 to 2019 National Survey of Children’s Health by Phillip Yang, Brian S Hernandez and Kristen A Plastino in International Journal of Social Psychiatry
Footnotes
Acknowledgements
We would like to acknowledge Jennifer Todd, JD; Nicole Dierschke, DrPH; and Maria Peché of UT Teen Health at UT Health San Antonio for their editorial assistance.
Conflict of interest
The authors do not have any potential conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.