
Abstract
Background:
While global studies demonstrated that features of urban living are associated with the risk of developing mental disorders, there remains a significant knowledge gap surrounding this topic in the Middle East and North Africa region.
Aims:
This study aims to assess the prevalence, severity, correlates, and treatment of mental disorders in Riyadh City by examining certain aspects of urban living such as exposure to traumatic events, early exposure to urbanization, and seeking treatment.
Methods:
The Saudi National Mental Health Survey is a community epidemiological survey in a nationally representative sample of citizens aged 15 to 65 in KSA. The World Health Organization Composite International Diagnostic Interview (CIDI 3·0) was used to estimate the 12-month prevalence of common mental disorders.
Results:
The prevalence of any mental disorder in Riyadh City was 29.2%. The most common disorders were anxiety disorders and mood disorders. Female, young, and previously married respondents were at higher risk for developing mental disorders. Exposure to traumatic events was associated with all types of mental disorders. Only 2.9% of those with any mental disorder sought mental health treatments.
Conclusions:
We found a high prevalence of mental disorders in Riyadh City that could be attributed to certain features of urban living. These results may point to potential interventions in urban areas that can mitigate the adverse consequences of urban living and promote the salutogenic aspects of cities.
Keywords
Background
Global population growth is increasingly concentrated in urban areas, specifically in megacities (Andrade et al., 2012; Ventriglio et al., 2021). It is estimated that by 2030, as urbanization continues to increase, two-thirds of the world’s population will be living in urban areas (Jowell et al., 2017).
The capital of the Kingdom of Saudi Arabia, Riyadh City is regarded as one of the biggest urban and commercial capitals in the Middle East (Sambidge, 2021). With a population of over 7.5 million, it accounts for more than 20% of the country’s total inhabitants. According to the Royal Commission for Riyadh City (RCRC), Riyadh City is expected to increase its current population size to 15 to 20 million people and secure a spot among the world’s top 10 biggest economies by 2030 (Sambidge, 2021); a likely scenario given the City’s history of doubling its population size each decade between the 1930s and the 1980s (Sambidge, 2021). This trend is a partial result of increased modernization and industrialization, leading to substantial rural-to-urban migration in search of better access to education, employment, health, and an overall higher quality of life that is often associated with cities (Gruebner et al., 2017).
However, rapid urbanization and population growth is accompanied by psychological, social, and economic changes (Ventriglio et al., 2021). Several reports have discussed the effect of urban living on mental health and have shown that certain aspects of living in cities are associated with a higher risk of mental disorders (Adli, 2011; Andrade et al., 2012; Gruebner et al., 2017; Jowell et al., 2017; Lambert et al., 2015; Peen et al., 2007, 2010; Solmi et al., 2017; Ventriglio et al., 2021). While there is no clear overall association between urban living and mental health, factors such as socioeconomic inequality, social stress, pollution, noise, and crime can all contribute to poor mental health for urban residents (Gruebner et al., 2017).
Previous research has indicated that urban living is associated with increased exposure to traumatic events (Do et al., 2019; Kazantzis et al., 2010; Lambert et al., 2015; Orrego et al., 2020; Ullman & Siegel, 1994), which in turn induces symptoms of mental disorders. Additionally, exposure to the urban environment over the early years of the life course has been linked with a high prevalence of mental disorders (Al-Sughayr & Ferwana, 2012). Previous research also shows that mental health services may be more common in urban areas in comparison to rural areas as a result of increasing availability of mental health services and service providers, higher income and education rates, and less stigma surrounding mental disorders (Thirthalli et al., 2017).
There remains therefore a global need to address the problematic circumstances and negative externalities of urban growth to help achieve a balance between rapid growth and declining mental wellbeing among urban-area dwellers. Most of the previous studies examining the association between urbanization and mental health, including several World Mental Health (WMH) studies (Andrade et al., 2012; Kovess-Masféty et al., 2005; Moreira et al., 2022), have been conducted in western countries, and less is understood about this association in the context of the Arab world. While there have been several studies examining the effects of urban living on mental health in in the Middle East (Al-Sharbati et al., 2003; Al-Sughayr & Ferwana, 2012; Morgan & Mall, 2019), their focus was either on particular population subgroups or on specific mental disorders. Further, we are not aware of previous work that has considered specifically how features of urban living affect mental health.
The aim of this paper is to expand on local findings by using data from the Saudi National Mental Health Survey (SNMHS) to estimate the prevalence, severity, correlates, and treatment of mental disorders in Riyadh City in relation to certain features of urban living, such as exposure to traumatic events, early exposure to urbanization, and seeking treatment, with the prevalence and severity of mental disorders in Riyadh City.
Methods
Study design
The SNMHS is a national household survey of Saudi citizens aged 15 to 65 exclusive of two administrative areas (Jazan and Najran) due to political conflict. Respondents were selected from a multistage clustered area probability household sample. The estimated response rate was 61% based on the American Association of Public Opinion Research RR2 definition (AAPOR, 2016), comparable to that of other WMH surveys in high-income countries (Kessler et al., 2017). A total of 4,004 interviews were completed.
As in other WMH surveys, we used a two-part case–control sampling design to reduce the interview burden on respondents who did not meet criteria for any of the core mental disorders assessed in the survey. All respondents completed Part I of the interview, which assessed core disorders. Part I respondents who met lifetime criteria for any of these disorders plus a probability subsample of other Part I respondents were then administered Part II, which assessed disorders of secondary interest and a wide range of correlates. A total of n = 1,981 respondents were administered the Part II interview. Part I sample was weighted to adjust for differential probabilities of selection within and between households and to match sample distributions to population distributions on the cross-classification of key sociodemographic and geographic data. Part II sample was then additionally weighted for the undersampling of Part I respondents without core disorders, resulting in the prevalence estimates of core disorders in the weighted Part II sample being identical to those in the Part I sample (Mneimneh et al., 2020). Based on our research aim, the sample in this report was calculated using Riyadh City respondents from Part I (n = 812) and Part II (n = 454). Table 1 presents the weighed characteristics of the full study sample as well as for respondents from Riyadh City.
Sociodemographic distribution of SNMH respondents for Riyadh City and full sample.
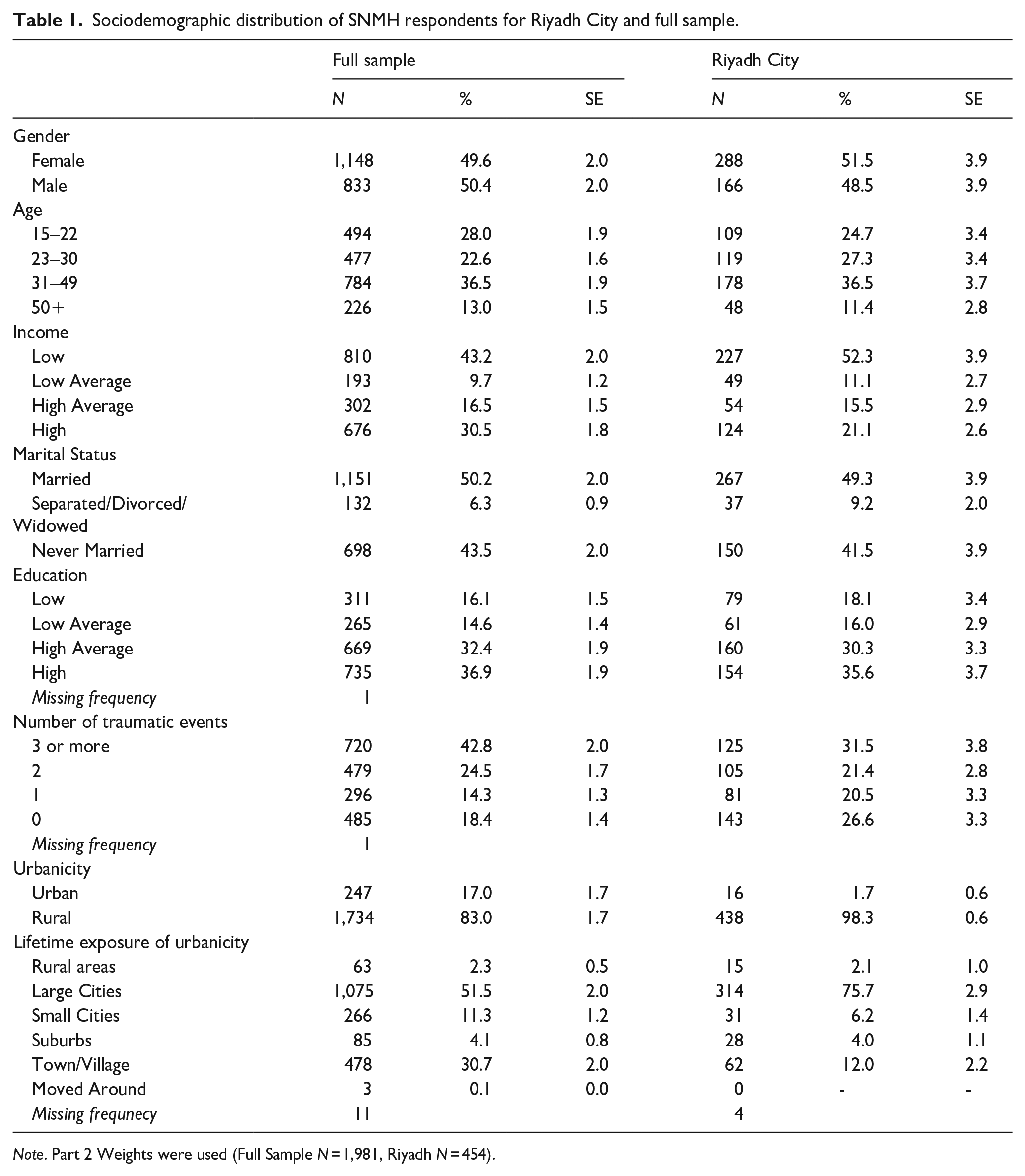
Note. Part 2 Weights were used (Full Sample N = 1,981, Riyadh N = 454).
Measures
Interviews were carried out by trained lay interviewers. The interview schedule and all training materials were translated and adapted using a standardized WHO translation protocol (Shahab et al., 2019; Sorel, 2010). Interviewer training and field quality control procedures were consistent with those in other WMH surveys (Heeringa et al., 2008; Pennell et al., 2008). Diagnoses were based on the WHO Composite International Diagnostic Interview Version 3·0 (CIDI 3·0) (Kessler & Ustün, 2004). The CIDI is a fully structured interview that is designed to be used by trained lay interviewers to generate diagnoses based on both ICD-10 and DSM-IV diagnostic criteria (Kessler & Ustün, 2004). Only DSM-IV criteria were used in the SNMHS (Kessler et al., 2020; Shahab et al., 2019). Details about other SNMHS survey methods for interviewers can be found elsewhere (Altwaijri, Al-Habeeb, Al-Subaie et al., 2020; Altwaijri, Al-Habeeb, Bilal et al., 2020; Aradati et al., 2019; Hyder et al., 2017; Shahab et al., 2017). Written informed consent was obtained from respondents prior to beginning each interview. Consent procedures were approved by the Institutional Review Board at the King Faisal Hospital and Research Center, Riyadh (RAC#: 2091093).
Correlates
Twelve-month diagnosis, severity, and treatment
Disorders assessed in the survey were (i) anxiety disorders [panic disorder, generalized anxiety disorder (GAD), social phobia, agoraphobia, post-traumatic stress disorder (PTSD), adult separation anxiety disorder, obsessive-compulsive disorder], (ii) mood disorders [major depressive disorder, bipolar I and/or II], (iii) impulse control disorder [conduct disorder, attention deficit disorder, intermittent explosive disorder], (iv) substance use disorder (SUD) [alcohol abuse, alcohol dependence, drug abuse, drug dependence], (v) eating disorder [anorexia, binge eating disorder, bulimia].
Disorders were classified as severe, moderate, or mild using criteria developed in previous WMH analyses (Kessler et al., 2009). Twelve-month disorders were classified ‘serious’ if they met one or more of the following criteria: (a) The disorder was either a bipolar I disorder or substance dependence with a physiological dependence syndrome; (b) a suicide attempt occurred in the past 12 months in conjunction with the disorder; or (c) the respondent reported severe impairment in at least two of the four areas of role functioning, assessed with a modified version of the Sheehan Disability Scale (SDS) (Sheehan et al., 1996). Disorders not classified “serious” were classified “moderate” if the respondent reported at least moderate impairment in any SDS domain or if the respondent had substance dependence without a physiological dependence syndrome. All other disorders were classified “mild.”
Part II respondents were asked if they ever obtained treatment from each of 14 different types of professionals for problems with emotions, nerves, mental health or use of alcohol or drugs. If so, questions were asked about age at first obtaining treatment, treatment in the past 12 months, and, when 12-month treatment was reported, number of visits from each of these types of professionals. Summary measures of 12-month treatment were created separately for the healthcare sector and the non-healthcare sector. Healthcare sector treatment was divided into treatment in the general medical sector and the mental health specialty sector, while non-healthcare sector was classified into human services and complementary-alternative medicine (CAM). Part II sample (N = 1,956) was used to compare participants from Riyadh City to participants from other administrative areas in KSA seeing as Riyadh City comprises most of Riyadh administrative area.
Sociodemographic
Sociodemographic variables included gender (male/female), age (5–22, 23–30, 31–49, and 50+ years old), and completed years of education classified as: low (0–6 years), low-average (7–9 years), high-average (10–15 years), and high (16+ years). These categories were based on levels of primary school, secondary school, high school, 3 years into college, and college graduates. Family income status was calculated based on the household income divided by the number of people in that household and classified based on the median of the entire sample as follows: low (less than 50% of the median), low-average (values up to the median), high-average (between one and three times the median), and high (values more than three times the median). Marital status classified as married, previously married (separated, widowed or divorced), or never married.
Exposure to traumatic events
Bearing in mind the prevalence of traumatic events in urban areas in KSA, 10 of the top traumatic events in the country associated with urban living were selected from the list of events from the PTSD section of the CIDI 3.0 (see Supplemental Table 1).
Exposure over early years of the life course to urban environment (urbanicity)
Respondents from Riyadh City were asked if they were raised mostly in a large city, the suburbs of a large city, a small city, a town or village, or a rural area.
Analysis
Prevalence of mental disorders and their severity was obtained using cross tabulation with appropriate weights for each type of disorder. The cross tabulation was done using the PROC SURVEYFREQ procedure in SAS 9.2. Multivariate logistic regression models were created for urban and rural areas to obtain their associations with sociodemographics. Binary logistic regression was used to obtain associations of disorder groups with exposure to traumatic events, disorder groups with migration status and professional treatment among different regions. All logistic regression estimates are reported as odds ratios with 95% confidence interval. The significance was calculated using the Wald chi-sq test with p > .05. All models were created using the PROC LOGISTIC procedure.
Results
Prevalence and severity
The proportion of Riyadh City household residents diagnosed with at least one mental health disorder in the past 12 months under study was 29.2%, and 49% of these cases were severe. Anxiety (18%) and mood disorders (11.1%) were the most common types of disorders. Severity was strongly related to comorbidity: an estimated three in ten of the cases (33.3%) with only one disorder qualified as “severe.” In comparison, the severity estimates for comorbid cases with two disorders were 62.2%, and 82.2% for those with more than three active disorders (Table 2).
Estimated 12-month prevalence and severity of DSM-IV/WMH-CIDI disorders in Riyadh.
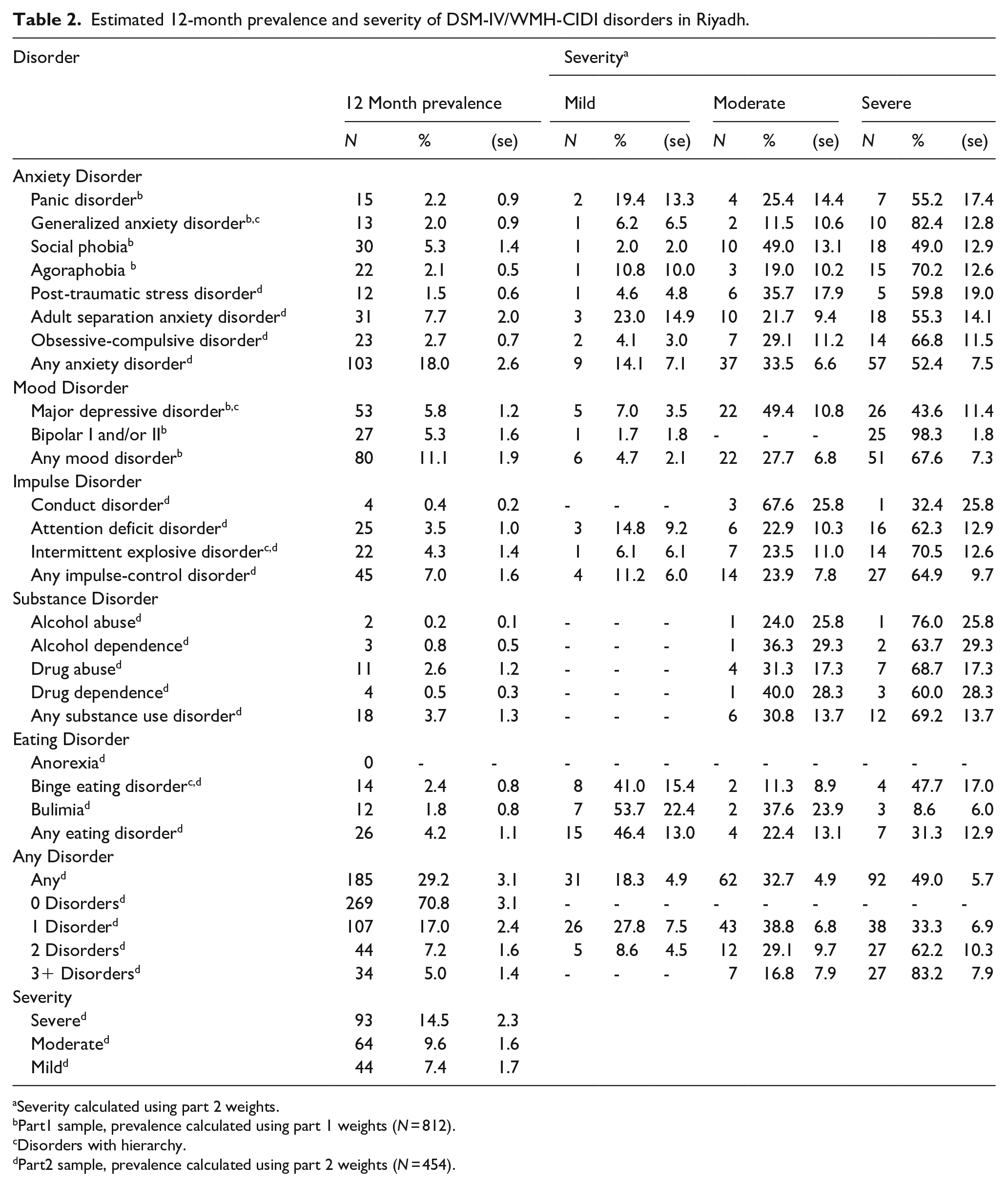
Severity calculated using part 2 weights.
Part1 sample, prevalence calculated using part 1 weights (N = 812).
Disorders with hierarchy.
Part2 sample, prevalence calculated using part 2 weights (N = 454).
The most common types of the anxiety disorders were found to be adult separation disorder (7.7%), followed by social phobia (5.3%). Major depressive disorder was the most common type of mood disorder (5.8%), with most cases categorized as moderate (49.4%) and severe (43.6%); followed by bipolar disorder, with most cases categorized as severe (98.3%). Intermittent explosive disorder was the most common type of impulse control disorder, with most cases categorized as severe (64.9%). Drug abuse was the most common type of SUD (17.3%), with most cases categorized as severe (68.7%). Binge eating disorder was the most common type of eating disorder (17.0%), with most cases categorized as severe (47.7%) (Table 2).
While most respondents had just one active mental disorder, there were some cases of comorbidity: about 7.2% were found to have two disorders and about 5% were found to have three or more disorders (Table 2).
Sociodemographic correlates of disorders and severity
As shown in Table 3, women were more likely to have any anxiety (OR = 3.7, 95% CI [2, 6.7]) and any severe/moderate disorders than men (OR = 2.6, 95% CI [1.5, 4.4]). The three youngest age groups were more likely than the oldest age group to have mood, impulse, and severe/moderate disorders.
Sociodemographic correlates of DSM-IV/WMH-CIDI disorders in the past 12-month in Riyadh.
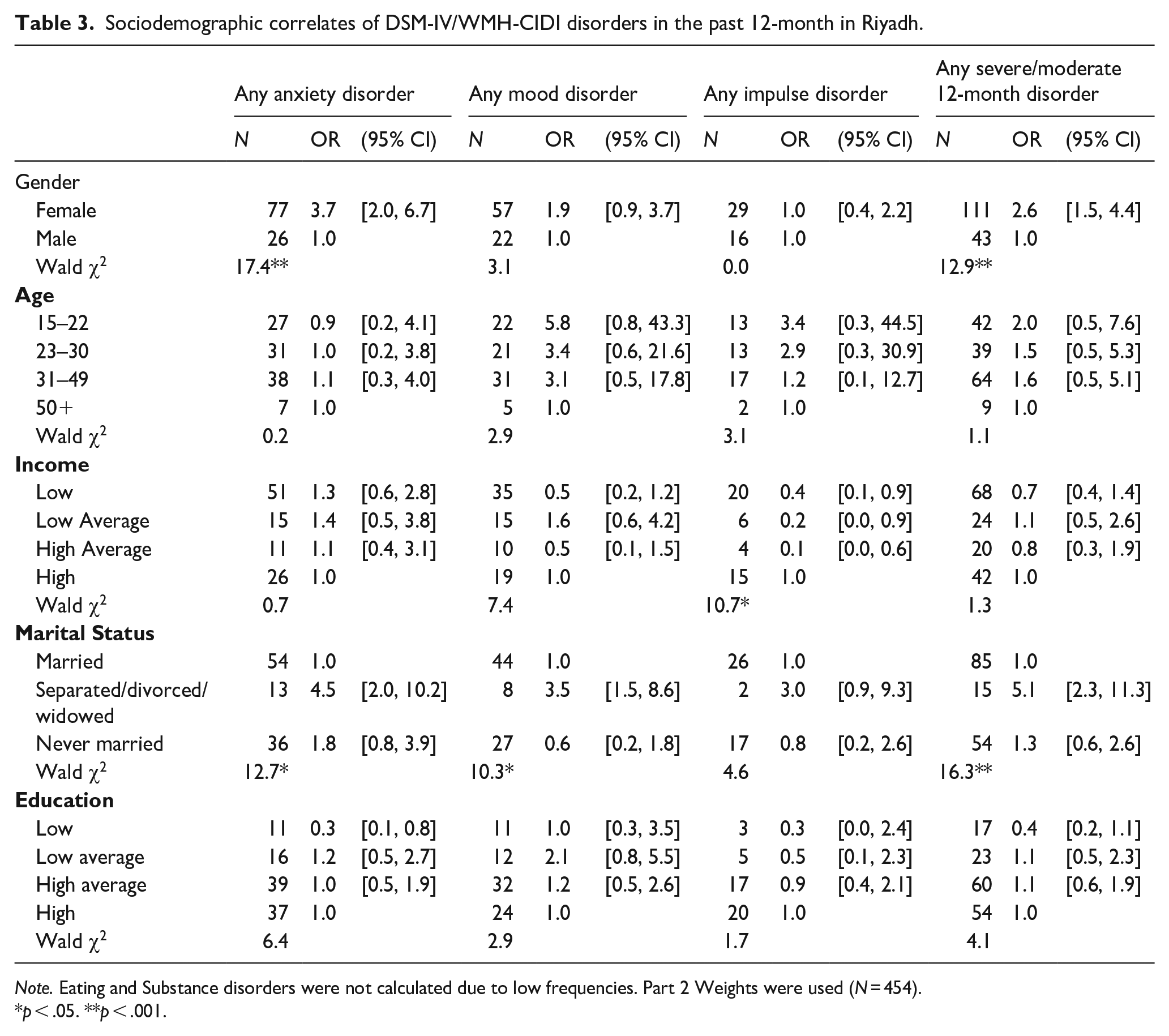
Note. Eating and Substance disorders were not calculated due to low frequencies. Part 2 Weights were used (N = 454).
p < .05. **p < .001.
Being in the high-average income group was associated with reduced odds of having impulse control disorders in comparison to the other income groups. Being previously married was significantly associated with having any anxiety, mood, and severe/moderate disorders in comparison to being married (Table 3).
Exposure to traumatic events
Out of the 10 traumatic events examined, most were more prevalent in urban versus rural areas (Supplemental Table 1). Respondents in Riyadh City had high exposure to various intentional traumatic events including being beaten up as a child by a caregiver (13.7%) and automobile accidents (12.4%) (Supplemental Table 1).
As shown in Table 4, respondents in Riyadh City exposed to three or more traumatic events were at highest risk for any impulse control disorder (OR = 21.6, 95% CI [3.8, 124.3]), followed by any substance use disorder (OR = 13.5, 95% CI [1.6, 113.1]), and at lowest risk to develop any anxiety disorder (OR = 2.8, 95% CI [1.4, 5.4]). Participants exposed to three or more traumatic events were six times more likely than their counterparts to develop any severe/moderate 12-month disorder (OR = 6.9, 95% CI [3.6, 13.6]).
Associations of exposure to traumatic events with 12-month DSM-IV/WMH-CIDI disorders and disorder severity in Riyadh.
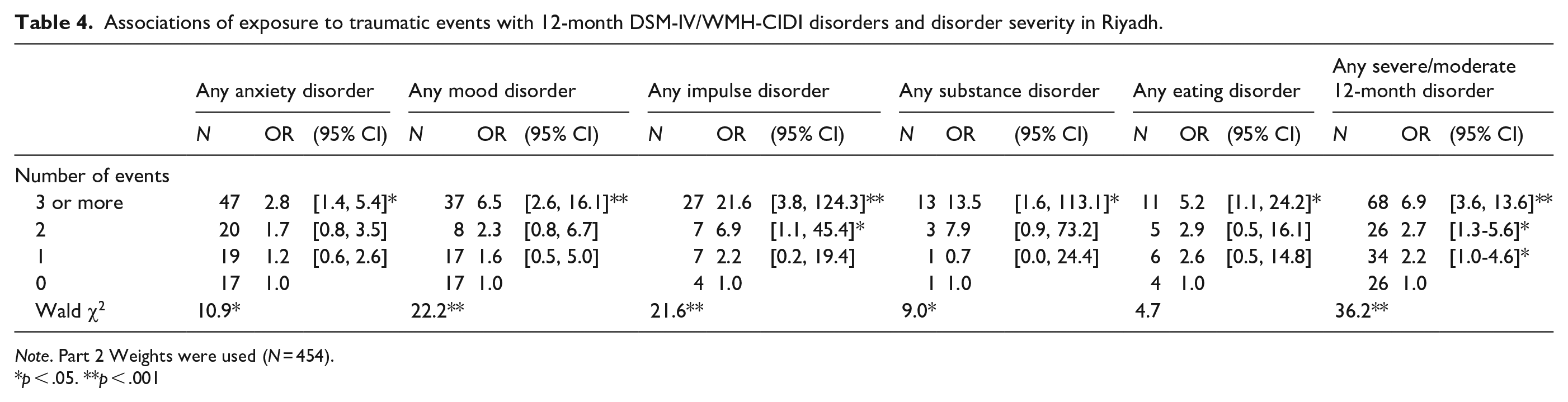
Note. Part 2 Weights were used (N = 454).
p < .05. **p < .001
Respondents exposed to two or more traumatic events were six times more likely than participants not exposed to any event to develop any impulse control disorder, and almost three times as likely to develop any severe/moderate 12-month disorder (OR = 2.8, 95% CI [1.3, 5.6]).
Respondents exposed to only one traumatic event were twice as likely than participants not exposed to any event to develop any severe/moderate 12-month disorder (OR = 2.2, 95% CI [1.0, 4.6]).
Exposure over early years of the life course to urban environment
Occurrences of anxiety disorders (OR = 3.2, 95% CI [0.2, 42.6]), mood disorders (OR = 3.5, 95% CI [0.1, 102.4]), and any 12-month severe/moderate disorder (OR = 3.7, 95% CI [0.4, 38.2]) were found to be almost three times more likely to appear in respondents raised in large cities versus rural areas; however, this association was not significant (Table 5).
Associations (odds-ratio) of lifetime exposure of urbanicity with 12-month DSM-IV/WMH-CIDI disorders.
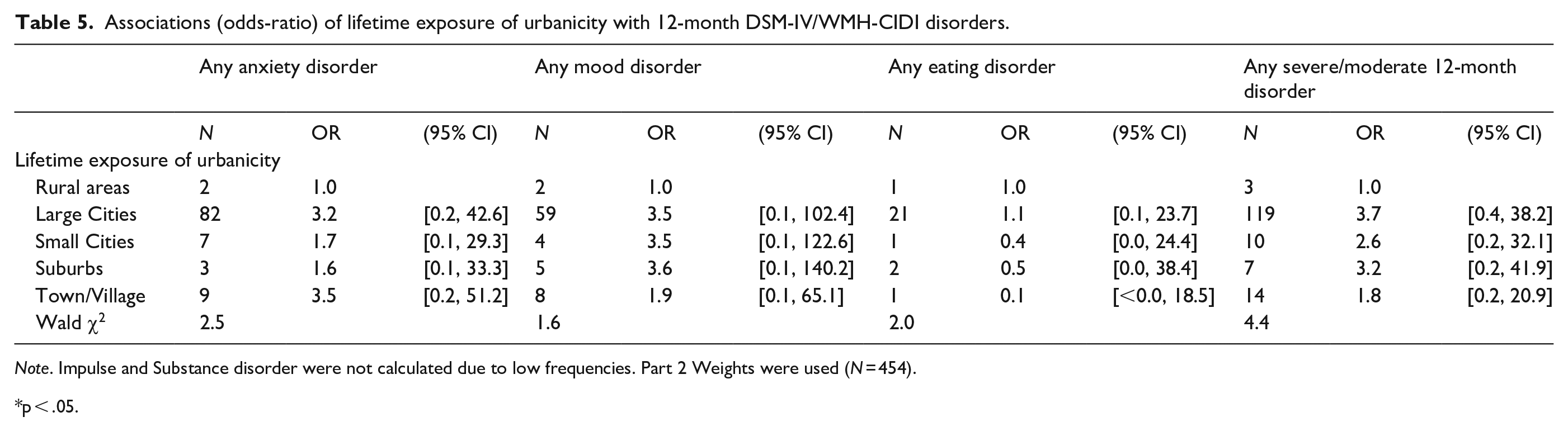
Note. Impulse and Substance disorder were not calculated due to low frequencies. Part 2 Weights were used (N = 454).
p < .05.
Treatment prevalence
Only 9.4% of Riyadh City respondents sought any type of treatment, and out of those respondents, 7.7% sought any treatment from the health sector, and only 2.9% sought any mental health treatment (Supplemental Table 2).
Riyadh City participants were found to have the highest odds of seeking any professional treatment in comparison to other areas (Figure 1). Moreover, individuals living in Al-Madinah, Al-Qaseem, Aseer, Eastern Region, and Makkah, had significantly lower odds of seeking treatment than individuals living in Riyadh (Table 6).
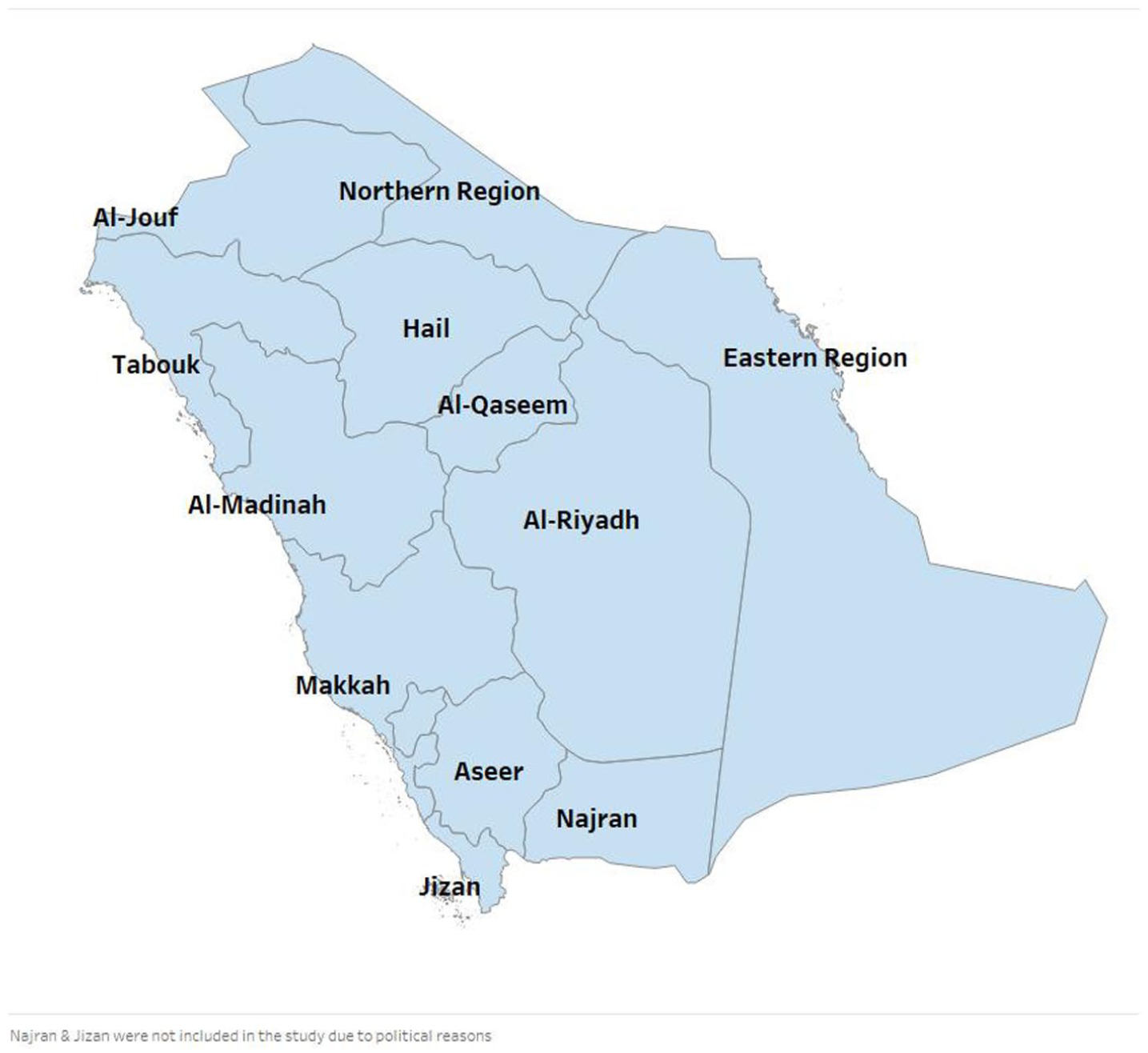
Map of the different administrative regions in the KSA.
Associations of treatment prevalence of 12-month DSM-IV/CIDI mental disorders across different administrative regions in KSA.
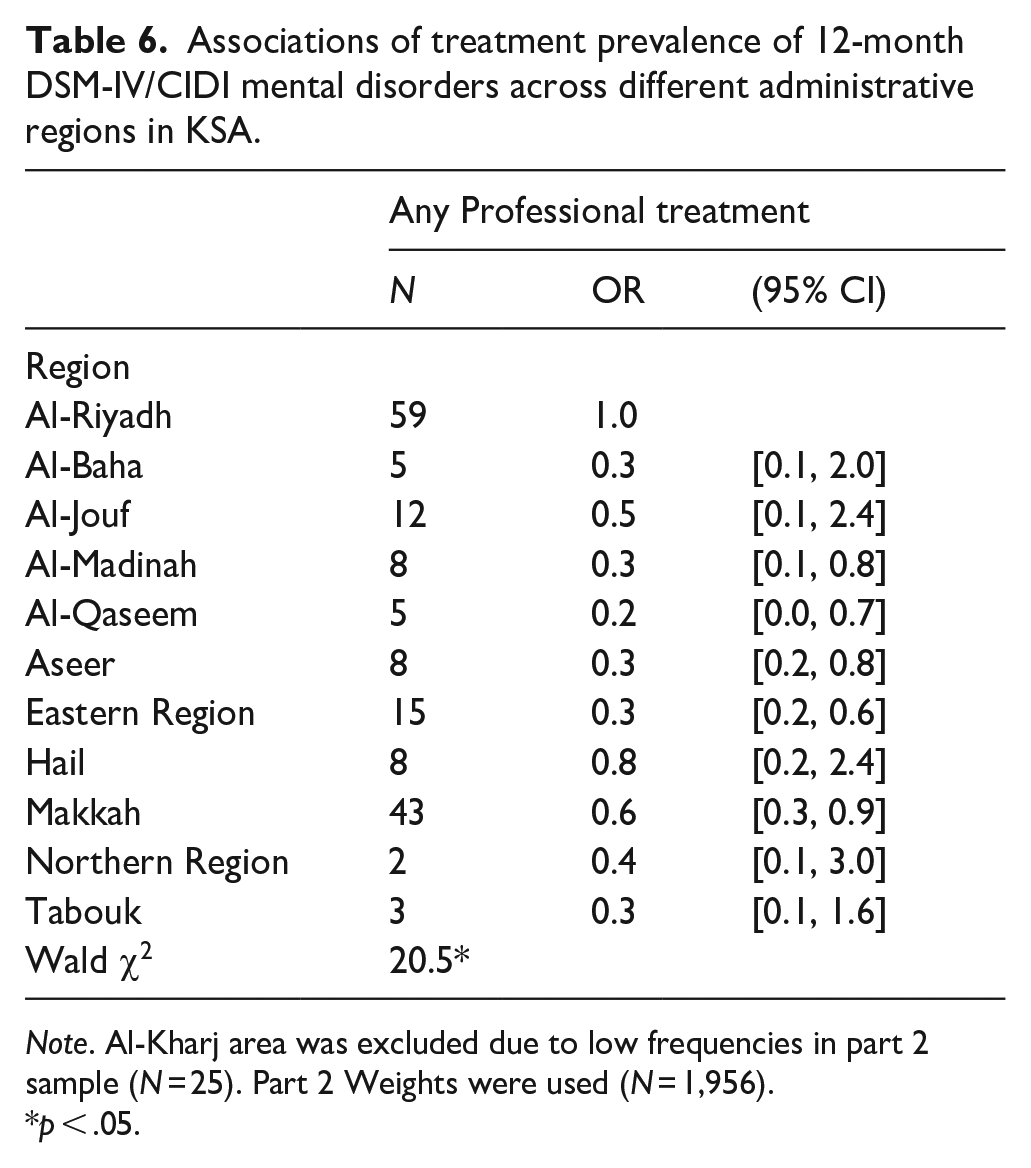
Note. Al-Kharj area was excluded due to low frequencies in part 2 sample (N = 25). Part 2 Weights were used (N = 1,956).
p < .05.
Discussion
This is one of the first studies in the MENA region to investigate mental disorders in a large urban area: Riyadh City. We found that mental disorders are highly prevalent among the Riyadh City population, in line with global reports of the relationship between mental disorders and urban living (Andrade et al., 2012; Gruebner et al., 2017; Jowell et al., 2017; Kovess-Masféty et al., 2005; Peen et al., 2007, 2010). Additionally, we identified several risk factors linked to the urban social or physical environments that were negatively associated with mental wellbeing.
In our study, anxiety disorders were the most prevalent mental conditions documented, followed by mood disorders, underscoring previous findings suggesting that mood-anxiety disorders are highly prevalent in urban areas (Andrade et al., 2012; Peen et al., 2010). Within mood-anxiety disorders, adult separation anxiety disorder and major depressive disorder were the most prevalent conditions. These findings were consistent with evidence suggesting that mood, anxiety, and psychotic disorders were found in higher rates in urban versus rural areas (Jacobi et al., 2014; Sharifi et al., 2015). While SUD was less common than mood-anxiety disorders in the city, all instances of its occurrence were recorded as severe, with drug abuse being the most prevalent. Prior research suggests that certain features of the urban environment such as social stress, income inequality, access to health and social services, the presence of social networks that enable drug use, and a poor infrastructure may encourage drug abuse as a coping mechanism (Galea et al., 2005). Additionally, with respect to comorbidity, among respondents with three or more disorders, 83.2% of them suffered from severe disorders.
Regarding sociodemographic correlates of mental disorders, women in general had a higher risk than men for developing any disorder and anxiety-mood disorders, while men had a slightly higher risk than women for developing impulse control disorders, consistent with global findings (Andrade et al., 2012; Ishikawa et al., 2016; Seedat et al., 2009; Solmi et al., 2017). However, further research is needed to define the contextual features influencing the observed prevalence of mental disorders among women in Riyadh City.
Respondents with high-average income were less likely than respondents with low and low-average income to develop impulse control disorders. The observation that persons with lower income are more likely to report more mental disorders than persons with higher income is consistent with a large body of recent literature (Ettman et al., 2020). This trend may be linked to the greater challenges of urban living and increased social stress faced by persons with fewer resources in these contexts (Adli, 2011). Further, respondents who had been previously married were at higher risk of developing all types of disorders, in line with previous studies (Andrade et al., 2012; Kawakami et al., 2005).
We found that apart from anxiety disorders, which were consistently prevalent across all age groups, most mental disorders were common in early adulthood and midyears. These findings are consistent with similar studies that found that younger-aged urban dwellers had a higher risk of developing mental disorders in comparison to their older counterparts (Kovess-Masféty et al., 2005). High prevalence of mental disorders among young adults could be due to their increased risk of interpersonal violence in urban areas, as well as their engagement in antisocial behavior as a result of living in deprived neighborhoods (Trivedi et al., 2008). These findings suggest that mental disorders could negatively affect role-functioning during the crucial years of employment (Kessler & Frank, 1997).
Our results indicate that traumatic events were associated with all types of mental conditions and disorder severity, in line with previous findings that substance abuse disorder, mood disorders, PTSD, and impulse control disorders are common among persons exposed to traumatic and violent events (Andrade et al., 2012; Do et al., 2019; Jowell et al., 2017; Ullman & Siegel, 1994). Consistent with the literature, high incidents of childhood abuse and automobile accidents are common in urban areas (Cabrera-Arnau & Bishop, 2021; Trivedi et al., 2008), underlining how the exposure to threatening or unpleasant life events can play a significant role in the development of mental distress, particularly among women and youth (Jowell et al., 2017; Kazantzis et al., 2010; Orrego et al., 2020).
Regarding the effects of urbanicity on mental health, our study found that mood and anxiety disorders were more prevalent among respondents raised in large cities. These results are in line with previous studies that have found increased odds between childhood urbanicity and depression (Andrade et al., 2012; Howdon et al., 2019).
When it comes to seeking treatment in Saudi Arabia, persons living in Riyadh City had higher odds of seeking any treatment than persons living in other areas in KSA, but that could be a result of both a larger population size in the city as well as increased availability of health services in comparison to other areas (Jowell et al., 2017). However, only a small portion of those who sought any treatment sought any type of mental health treatment despite the reasonable availability of services. A study examining the barriers to mental health treatment in Saudi Arabia found that attitudinal barriers, such as stigma and the desire to handle problems independently, played a major role in the prevention of treatment in the country (Alangari et al., 2020). In contrast, certain studies have found no significant differences in the seeking of mental health services and duration of untreated illness between patients in urban and rural areas (Thirthalli et al., 2017). Further, factors associated with urban settings, such as general education level and the proximity and accessibility of mental health services, have not been shown to influence treatment seeking (Thirthalli et al., 2017).
The implications of our study can further assist policymakers in recognizing the interactions between urban stressors and mental health and inform subsequent intervention and treatment plans for the promotion of urban mental wellbeing throughout the Middle East and North Africa (MENA) region.
Limitations
These results should be interpreted considering several limitations. First, our sample may not be representative of the entire population as only household residents were interviewed, not including homeless and institutionalized individuals. Further, people with mental disorders might have been less eager than others to participate in the survey due to perceived biases regarding mental health disorders and differential morality, among other reasons. Such biases have been similarly documented in previous studies (Pennell et al., 2008). However, in order to minimize the risk of underreporting bias, certain sensitive sections, such as those for substance use and conduct disorders, were delivered via Audio Computer-Assisted Self-Interviewing mode and the responses were self-reported by participants. Second, generalizability should be applied with caution given our sample size that was taken from a larger nationwide sample. Finally, due to the cross-sectional design of our study, our data cannot be used to determine the direction of association of sociodemographic variables with the disorders examined in our study.
Conclusions
Consistent with observations from other large cities, we found a high prevalence of psychiatric morbidity in Riyadh City; further supporting previous claims that particular urban characteristics pose a mental health risk for urban and large cities dwellers. This is of particular significance given the active strategies set in motion to increase Riyadh’s population to 15 to 20 million by 2030. Therefore, we aim for our findings to guide policy makers, urban designers, and clinical practitioners in recognizing that with continued growth in urban sprawl and density, there will be emerging mental health issues in large and urban cities. Further research is needed to provide policy makers with the knowledge to promote initiatives to reduce and control the risk factors associated with elevated mental distress in the densely populated cities of KSA. Further studies may also fruitfully explore the mechanisms that underlie some of the observations made here about the determinants of mental disorders in the MENA region.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231152202 – Supplemental material for Urbanization and mental health: A perspective from Riyadh City, Kingdom of Saudi Arabia
Supplemental material, sj-docx-1-isp-10.1177_00207640231152202 for Urbanization and mental health: A perspective from Riyadh City, Kingdom of Saudi Arabia by Yasmin A Altwaijri, Abdullah S Al-Subaie, AbdulHameed Al-Habeeb, Sandro Galea, Marya Akkad, Mohammad Talal Naseem and Lisa Bilal in International Journal of Social Psychiatry
Footnotes
Acknowledgements
We thank the staff of the WMH Data Collection Coordination Centre in the Survey Research Center at University of Michigan and the WMH Data Analysis Coordination Centre in the Department of Health Care Policy at Harvard Medical School for assistance with design, instrumentation, fieldwork, and consultation on data analysis. A complete list of all WMH publications can be found at ![]() . We also acknowledge with gratitude the work and dedication of the SNMHS staff both current and past for their contributions to the study. We further appreciate constructive feedback from Sanaa Hyder during the preparation of this paper.
. We also acknowledge with gratitude the work and dedication of the SNMHS staff both current and past for their contributions to the study. We further appreciate constructive feedback from Sanaa Hyder during the preparation of this paper.
Author contributions
YAA, ASA, AHA made substantial contributions to the conception and design of the work. YAA and LB made substantial contributions to acquisition of the data. NMT made substantial contributions to analysis of the data. YAA, MA, SG made substantial contributions to interpretation of the data. YAA and MA drafted the text. YAA, ASA, HAH, SG, MA, NMT, and LB worked on revising the text critically for important intellectual content. YAA, ASA, HAH, SG, MA, NMT, and LB gave final approval for this version to be published. YAA agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Availability of data and materials
A public use dataset is not available because of restrictions in the informed consent language used to recruit respondents. However, a de-identifed minimal dataset for quality assurance can be obtained by contacting the corresponding author.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The SNMHS is conducted by the King Salman Center for Disability Research. It is funded by Saudi Basic Industries Corporation (SABIC), King Abdulaziz City for Science and Technology (KACST), and King Saud University. Funding-in-kind was provided by King Faisal Specialist Hospital and Research Center, and the Ministry of Economy and Planning, General Authority for Statistics. In addition, work at Harvard Medical School was funded by a service agreement from the King Faisal Specialist Hospital and Research center. None of the funders had any role in the design of the study, data analysis, interpretation of results, or preparation of this paper. The SNMHS is carried out in conjunction with the World Health Organization World Mental Health (WMH) Survey Initiative.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.