
Abstract
Background:
Decreasing suicide mortality has become an overarching goal for societies worldwide. Suicide registers and other monitoring systems are a valuable source of information that can be used for addressing the suicide phenomenon and evaluating preventative interventions.
Aims:
This scoping review provides an overview of literature published in the last decade that has focussed on the operations (functioning) and characteristics of suicide registers and other suicide monitoring systems.
Methods:
Four electronic databases were searched in 2020 for identifying published material from January 2010 to October 2020. The searches were updated in October 2023 to include material from 2020 to date. Grey literature through Google searches and mental health commissions websites and the reference lists of selected documents were also searched.
Results:
Twenty-five articles were included in this review. Nearly half the articles were from the United States, followed by Australia. Nine countries were identified as having used suicide registers or suicide-specific monitoring systems to inform suicide prevention. Monitoring mechanisms varied across the countries examined. No article provided evidence that definitively linked suicide registers or other monitoring systems for suicide with the prevention of suicide or reduction in suicide rates. However, a variety of benefits of suicide monitoring for preventative and public health interventions were identified.
Conclusions:
The number of nations with surveillance systems for suicide prevention is low. Further, there is a lack of consistency in the systematic collection, analysis and interpretation of suicide-related information across the countries examined. Efforts to establish high-quality suicide surveillance systems that can be accessed in a timely and easy manner are needed to inform tailored strategies for suicide prevention.
Introduction
Suicide is a global challenge that has been recognised as a significant health priority worldwide. The World Health Organization (WHO) estimates that more than 700,000 persons die due to suicide every year. In 2019, suicide was the fourth leading cause of death in people between 15 and 29 years old globally (World Health Organization [WHO], 2023). While most deaths by suicide (77%) occurred in low-and-middle-income countries, high-income countries have the highest age-standardised suicide rate (10.0/100,000), and particularly for men (16.5/100,000) (WHO, 2023). With suicide considered potentially preventable, decreasing suicide mortality has thus become an overarching goal of societies worldwide. The WHO (2014) has identified that Ministers of Health need to bring together stakeholders from health and other sectors and lead the development of national strategies for suicide prevention.
Given the complexity of the suicide phenomenon, public health surveillance is imperative for guiding the efforts of health authorities and policy makers for suicide prevention. Further, timely and effective evidence-based interventions play a key role in preventing suicides; to determine what is effective, robust data are essential. Governments are in a unique position to develop and strengthen surveillance and to provide and disseminate data that can help to inform action. According to the Centers for Disease Control and Prevention, epidemiologic surveillance has been defined as ‘the ongoing systematic collection, analysis and interpretation of health data essential to the planning, implementation and evaluation of public health practice, closely integrated with the timely dissemination of these data to those who need to know’ (Thacker & Berkelman, 1988). In this context, suicide registers and other monitoring systems are valuable tools.
Registering suicide is a complex process that involves different authorities and monitoring mechanisms that vary across jurisdictions. According to the WHO (2016), only a limited group of nations have established suicide registers or specific monitoring systems for suicide surveillance: in 2013, the WHO together with the International Association for Suicide Prevention reported that just 16 countries confirmed the presence of such systems. Meanwhile, around 60 WHO member states had high-quality vital registration data, that can be used to estimate suicide rates (WHO, 2020, 2021b).
This scoping review provides a comprehensive overview of literature published in the last decade that has focussed on the operations (functioning) and characteristics of suicide registers and other suicide-specific monitoring systems. We identify differences in mechanisms such as technical specifications and processes and geographical scope. Finally, we ascertain the known benefits and/or limitations of suicide registers and the application of data from such registers to inform evidence-based suicide prevention strategies and related public health interventions.
Methods
The present scoping review incorporates key methodological guidelines from Cochrane Methods Rapid Reviews (Garritty et al., 2021) and the National Collaborating Centre for Methods and Tools (NCCMT; Dobbins, 2017). We followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping reviews (PRISMA-ScR; Tricco et al., 2018) and the methodology developed by the Joanna Briggs Institute (JBI; Peters et al., 2015).
Review questions
The specific research questions posed in this review are:
RQ1: Which countries/places have used suicide registers to inform evidence-based suicide prevention and/or public health interventions?
RQ2: Are monitoring mechanisms used in the surveillance of suicide different around the world?/Have differences in the monitoring mechanisms been identified in the surveillance of suicide globally, if so, what are those differences?
RQ3: Have these information systems been successful in monitoring suicide to inform strategies for suicide prevention? If so, what are the benefits or limitations reported?
RQ4: Do local needs and benefits to suicide prevention vary from national ones? If so, in what ways?
Search strategy
The search strategy was designed to identify published material on suicide registers and other suicide-specific monitoring systems for suicide prevention. No language restrictions were applied to the searches in an attempt to identify all material published in any language. However, only information available in English, Spanish or French was searched for eligibility. This approach was employed given native speakers of these languages within the authorship team. Further, English is the dominant language in scholarly communication (Liu, 2017; Rao, 2018) and one of the strongest forms of global communication (Tenzer et al., 2017). Together English, Spanish and French comprise three of the six most commonly spoken languages around the world (Dyvik, 2024). Therefore, the expectation was most papers would be published in one of these languages. An initial search was executed in EMBASE (PubMed) to identify existing systematic reviews and/or studies with other designs that provide the necessary information to address our research questions.
Four electronic databases were searched: Cochrane Library, MEDLINE, EMBASE and PsychInfo. Years initially considered for the identification of relevant material were 2010 to 2020. Searches were updated in October 2023 to include material published after 2020. Search terms were introduced with corresponding MeSH Terms, synonyms and appropriate use of controlled vocabulary searched in the Subject Headings field, Boolean operators and filters. Grey literature was examined through Google searches and review of mental health commission websites (i.e. any government organisation that is key in the promotion, improvement and safeguarding of the mental health and wellbeing of their nation’s population and/or key in the prevention of suicide). Commission websites were identified through web links of national statistics and databases provided within the articles cited in the Introduction section of this review and/or through retrieved material. In a further step, the reference lists of selected documents were searched. The search strategy for MEDLINE (PubMed) is provided in Appendix 1.
Eligibility criteria
The documents for inclusion in this review needed to focus on a suicide-specific surveillance/monitoring system(s) and their operations and characteristics, rather than analyses of data collected by these systems. Information such as published papers on the nature and role of suicide registers, organisational or government reports, descriptions of surveillance systems, best practice guidelines, manuals, grey literature, practice reviews and any other published material that provides information on suicide monitoring and data were considered for inclusion.
Selection of sources of evidence
Titles and abstracts of identified material were screened by two independent reviewers (ANF and AM). Updated material was screened by ANF and AN. The full text of the material identified as potentially useful was retrieved and reviewed to determine inclusion. The full text of any potential additional material was also retrieved to determine eligibility. Any inconsistences and disagreements were resolved by consensus, resulting in a final list of publications from which to extract relevant information.
Data extraction and synthesis of the evidence
Data and insights regarding the research questions from eligible articles were extracted into a working table (ANF and AM – initial material, ANF – updated material). Data extracted encompassed basic descriptive information from each article: author(s), year and country of publication; specific data details: type of publication (e.g. systematic reviews, government reports, best practice guidelines and manuals), number and type of included studies (if an empirical study, commentary, review or synthesis article), monitoring mechanisms used (if available), use of data linkage; and any noted outcomes of significance for example, benefits, limitations and success of the suicide register for informing evidence-based suicide prevention strategies and/or public health interventions. A narrative synthesis responding to the research questions posed for this scoping review, was then undertaken.
Results
In 2020, 393 records were identified through the databases and Google searches; an additional 61 records were identified in October 2023. Of all 454 records, 57 were duplicates. Titles and abstracts of the remaining 397 records were screened, with five identified in languages other than English. Fifty-five articles were assessed as eligible for full text review (including two in French), along with a further 12 articles identified through other sources. After full text review, a total of 25 articles were included as meeting all selection criteria. The results of our searches are displayed in Figure 1.
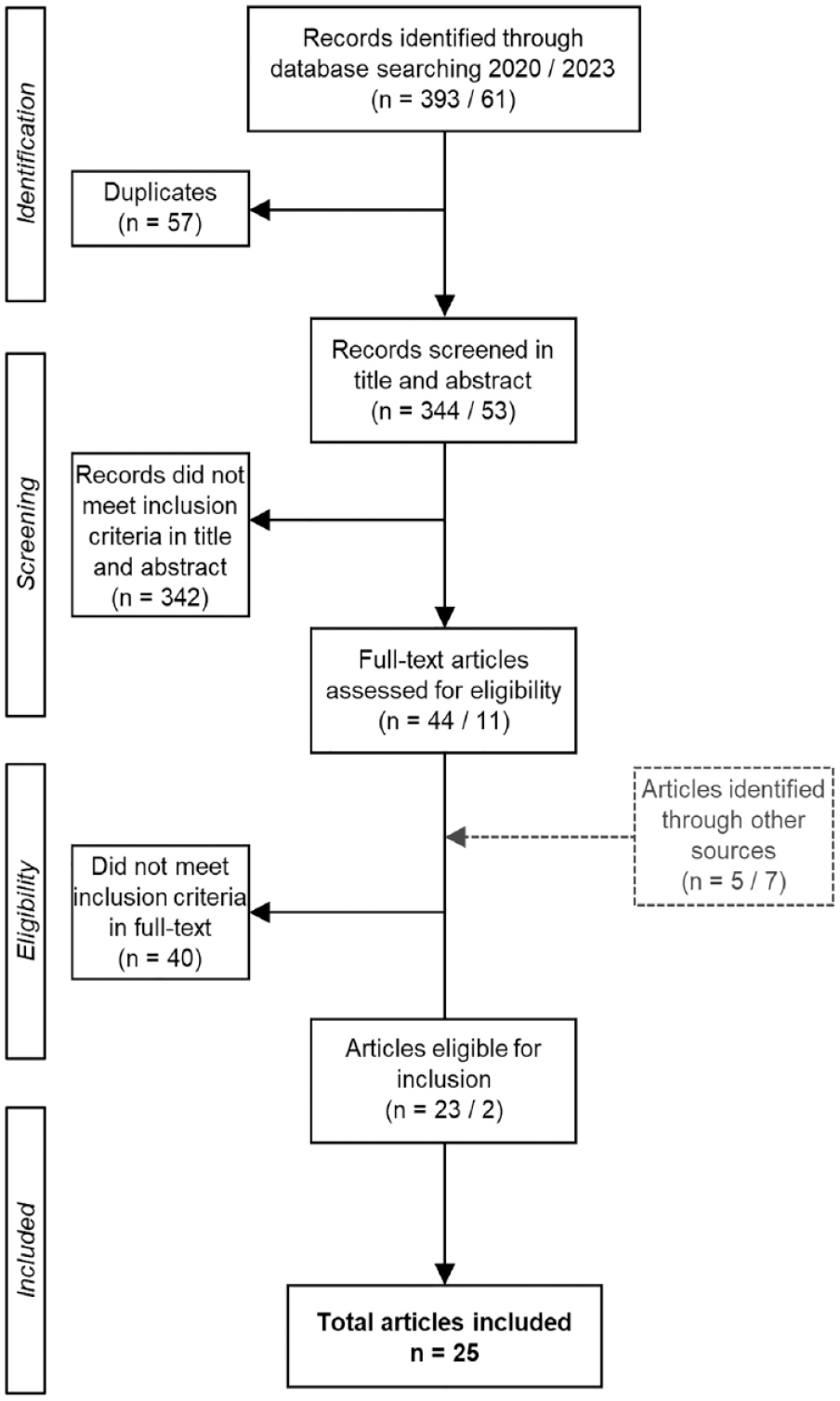
PRISMA flow diagram of article inclusion.
Overview of included evidence
Evidence included in this review came from nine countries. Nearly half of the articles were from the United States (US; n = 12), followed by Australia (n = 5). Journal articles were the most common type of publication (n = 14). Twenty-two suicide surveillance systems were identified through the included publications, including three reported in a Doctoral dissertation. Twelve of 22 suicide surveillance systems were suicide registers, different types of monitoring systems otherwise being employed (see Tables 1 and 2). Of 22 included systems, eight offer national coverage and eight focus on local-level data; the remaining six systems are focussed on death by suicide of specific groups (including Canadian Armed Forces, US military services, veterans, Apache people and people under the recent care of specialist mental health services). A summary of characteristics of articles included in the review and an outline of information by country are provided in Tables 1 and 2. The full characteristics of the included articles can be seen in Appendix 2. Findings by research questions are presented below.
Summary statistics of included evidence (N = 25 articles).
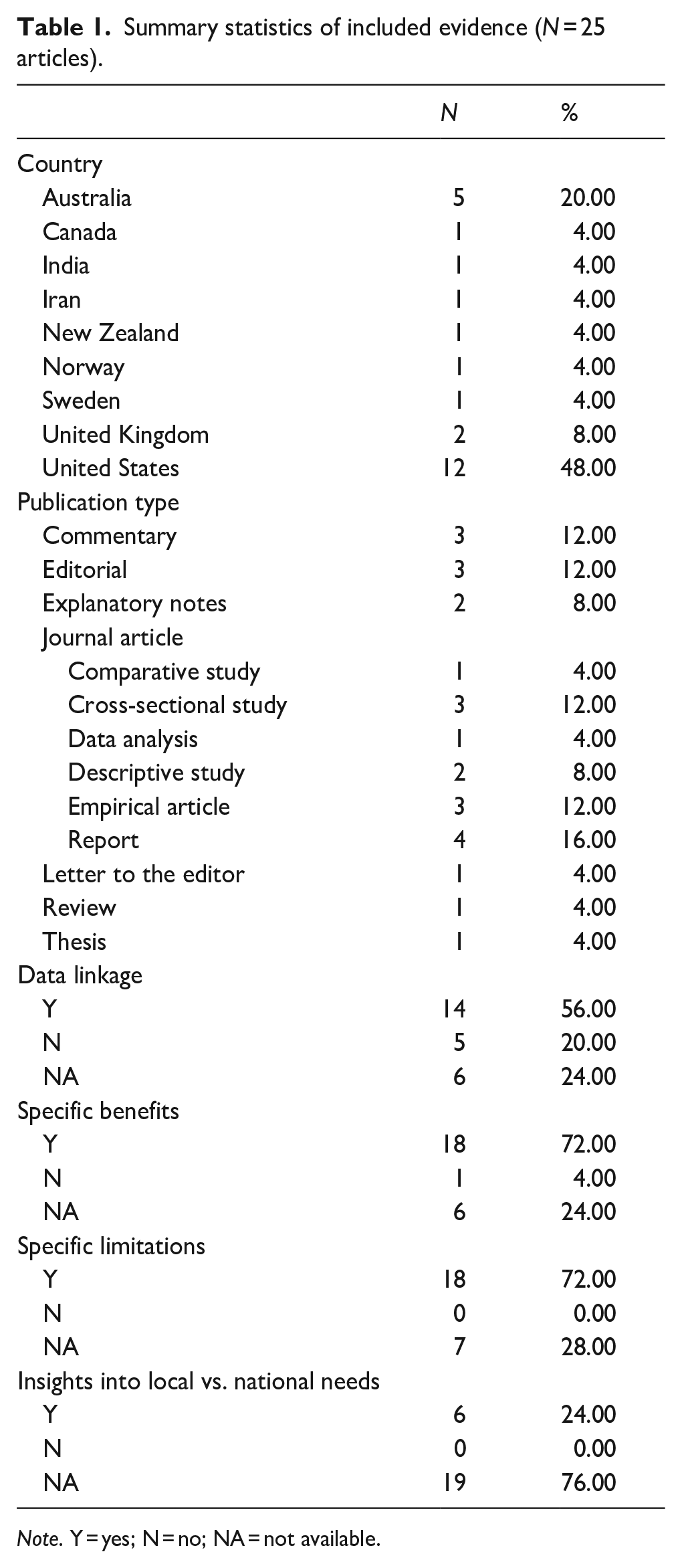
Note. Y = yes; N = no; NA = not available.
Overview of included articles by country of origin, reported against research questions.

Note. ANZSCO = Australian and New Zealand Standard Classification of Occupations; ANZSIC = Australian and New Zealand Standard Industrial Classification; CDC = Centers for Disease Control and Prevention; ICD = International Classification of Diseases; ICD-10 = ICD 10th revision; ICECI = International Classification of External Causes of Injury; N = no; NA = not available; NHDD = National Health Data Dictionary; TOOCS = Type of Occurrence Classification System; US = United States; vs. = versus; WHO = World Health Organization; Y = yes.
Countries/places that have used suicide registers to inform evidence-based suicide prevention and/or public health interventions
Nine countries were identified as having used suicide registers or suicide-specific monitoring systems to inform suicide prevention and/or public health interventions: Australia, Canada, India, Iran, New Zealand, Norway, Sweden, the United Kingdom (UK) and the US. Most articles used data from a suicide register, and they discussed how they were/could be used to inform suicide prevention (see Appendix 2). In contrast, Gunnell et al. (2011) discussed the use of narrative verdicts in England and Wales, and Ikeda et al. (2014) detailed the Data and Surveillance Task Force, a system created to improve and expand existing information about suicide and suicidal behaviour in the US. The National Confidential Inquiry into Suicide and Safety in Mental Health (NCISH, 2023) details the methodology of a research programme into suicide prevention in clinical services in the UK. The NCISH, established at the University of Manchester in 1996, examines the circumstances leading up to and surrounding the deaths by suicide of people under the recent care of specialist mental health services (The University of Manchester, 2024). Meanwhile Vijayakumar et al. (2020) reported on the value and processes of establishing a comprehensive community surveillance system in India.
All but eight articles (Cerel et al., 2016; Gunnell et al., 2011; Hajebi et al., 2013; Ikeda et al., 2014; Jiang et al., 2015; NCISH, 2023; Rolland-Harris, 2019; Vijayakumar et al., 2020) discussed how the data were/could be used to inform public health interventions. These methods encompassed: suicide method controls (e.g. means restriction); service delivery for children of domestic violence-related homicide victims; and services for mental health treatment and substance abuse.
Differences in monitoring mechanisms used in the surveillance of suicide around the world
Monitoring mechanisms used in the surveillance of suicide varied across the countries examined in the included articles. Major differences identified include:
Use of a formal suicide register. Most countries use a formal suicide register, exceptions being India, New Zealand and the UK.
The processes for determining the cause of death, including certification of death by physicians and medical death certificates (Sweden), Coroner and medical examiner records (US), multiple documentary sources (Australia).
The physical location of suicide registers/systems and variations in wider data access, and the roles of data custodians and data protection laws in governing access.
Comprehensiveness of data/extent of data collection extensions/data linkage options to enable identification of risk factors. Registers in Norway and Sweden tended to have the most comprehensive data linkage options via other national data infrastructure (e.g. connections to longitudinal and population level statistics).
Use of data linkage. Three suicide monitoring systems (India, New Zealand and the UK) did not report use of data linkage in conjunction with suicide register/monitoring system data.
Extent of integration with national data infrastructure. For example, connections to longitudinal and population level statistics in Norway and Sweden was more comprehensive than in other countries.
Inclusion of surveillance of non-fatal incidents of suicidal behaviour.
The success, benefits and limitations of information systems in monitoring suicide to inform strategies for suicide prevention
While none of the reviewed articles provided evidence that definitively linked suicide registers or other monitoring systems for suicide with the prevention of suicide or reduction in suicide rates, a variety of benefits of suicide monitoring for preventative and public health interventions were identified. These benefits included the ability to understand risk factors to inform suicide prevention in occupational, local and national contexts (a process facilitated through data linkage to large population data sets; Dodds et al., 2014; Olds et al., 2018; Saar et al., 2017); and the ability to provide support and other suicide postvention services to family and communities bereaved by suicide Clinical Advisory Services (Aotearoa, 2016). Data from reporting systems has been also used to inform policy change regarding services for children of domestic violence-related homicide victims and to inform and support homicide prevention efforts (Blair et al., 2016). Further, information from reporting systems has been used to make recommendations to improve mental health services and the safety of patients under specialist mental health care (NCISH, 2023).
A range of limitations of the suicide monitoring systems reviewed were also identified (see Table 2 and Appendix 2). These limitations generally pertain to data extraction and quality of source data, social factors affecting decisions and reporting and timeliness of data.
Data extraction and quality
Variability in quality of source data included data collected in the course of death investigations not being designed for surveillance purposes; variations between police and coroners’ reports; non-standardised post-mortem reports; the amount of missing data; and inconsistencies in information for the same variable from different sources. These concerns were identified at local and national levels.
Other identified issues included misclassifications of cause of death (Gahm et al., 2012) and under-reporting, notably given the burden of proof required for reaching a suicide verdict. This issue related to primacy rules employed in the US National Violent Death Reporting System (NVDRS) which is based upon assumed reliability of the sources (in order of importance: death certificate, coroner /medical examiner, law enforcement; Barber et al., 2013; Blair et al., 2016; Kaplan et al., 2017; R. T. Liu et al., 2013). Further, the ability to extract data from systems was also limited by coding and/or system backlogs and ethics requirements (Dodds et al., 2014; Olds et al., 2018; Saar et al., 2017).
Social factors affecting decisions and reporting
Social stigma related to suicide was identified as a limitation of systems, as it impacts the use of ‘open/unknown’ or ‘accidental’ verdicts by coroners in the belief that this will minimise a family’s distress (Hajebi et al., 2013). Similarly, the role of health and life insurance policies and related financial impact on families was noted as a factor in the under-reporting of suicide as cause of death (Hajebi et al., 2013).
Timeliness of data
The lack of ability to provide a cause of death for ‘open’ cases (Sutherland et al., 2018) and problems with inter-departmental collaboration to facilitate data sharing/and or linkage (health and justice) can limit real-time monitoring. In addition, research approvals to gain access to registries are time-limited (Stene-Larsen et al., 2018).
Variation between local versus national needs and benefits related to suicide prevention
Both local and national needs must be factored into suicide prevention strategies. However, only six of the reviewed articles provided direct insights into local versus national needs and benefits. Local needs included active local outreach and postvention services and assessment of current local patterns of suspected suicides to discern the likelihood of a possible suicide cluster or contagion effect (Clinical Advisory Services Aotearoa, 2016). Also considered important are the potential role of neighbourhood/regional factors (Kaplan et al., 2017) and wider social circumstances (Sutherland et al., 2018). Such circumstances can be reflected with targeted screening at the national level. For example, the Canadian Armed forces have their own surveillance system (referred to as ‘more than just counting deaths’) which is evolving to include a range of complementary data collection methods and sources that value-add to the evidence generated (Rolland-Harris, 2019).
Coordination between reporting authorities was also identified as key to national suicide prevention efforts in Australia and the US. For instance, standardising death investigation practices across the US (Ikeda et al., 2014) and the coding of ‘intent’ across Australia (Dodds et al., 2014) require better alignment. Meanwhile, in Iran, the quality of suicide registration was considered more accurate in local areas compared to national ones (Hajebi et al., 2013) with local registration processes more efficient and often more comprehensive (Hajebi et al., 2013).
Discussion
This scoping review is the first to provide an overview of the literature on suicide registers and other formal monitoring systems for suicide, and to describe the benefits and limitations of these systems for suicide prevention and public health interventions. The review included studies from nine countries reporting on 22 monitoring systems (national and local). No conclusive evidence was found that linked suicide registers or other suicide monitoring systems to the prevention of suicide or reduction in suicide rates. However, a number of benefits of monitoring systems in supporting suicide prevention efforts were identified.
Specific learnings from this review are that the number of countries with surveillance systems for suicide prevention is low. Further, the mechanisms used differ across the countries examined. For instance, the processes for determining the cause of death vary, ranging from third-party key informants (India) to certification of death by physicians and the medical death certificate (Sweden), to multiple investigative sources (US). These processes will influence the rates of suicide, particularly if the mechanisms/causes of death are not clear. Further, a lack of consistency between local and national information limits robust intra-country comparisons.
It was noted that death investigations that involve multiple agencies can result in delays in determinations, making the implementation of timely suicide prevention efforts difficult (Ikeda et al., 2014). In contrast, when information is accessible for analysis immediately after a death by suicide is registered, real-time surveillance can be implemented (WHO, 2021a) and this should be considered as a key element of any suicide surveillance system as reflected in Benson et al. (2022).
Likewise, data quality - including the comprehensiveness of data or extent of data collection - was also identified as a key element of effective suicide monitoring systems. The ability to understand risk factors to inform suicide prevention strategies in occupational, local and national contexts, is deemed as imperative. A comprehensive database will enable the identification of suicide patterns and trends; characteristics and means of suicide (WHO, 2023); and psychosocial factors that can contribute to suicide. The inclusion of such information may be facilitated through data linkage. For example, the links between the health registries in Norway enable access to a range of variables through which associations between specific factors and death by suicide can be established and used to inform suicide prevention in occupational, local and national contexts. Moreover, access to databases of suicides needs to be facilitated for monitoring and research purposes. Rigorous research is needed to understand the suicide phenomenon and provide a solid evidence-base for suicide prevention strategies.
The main limitation of this study lies in the fact that most of the evidence included was obtained from the peer reviewed literature, implicitly embodying a ‘researcher’ perspective. From this perspective, constraints imposed by ethics and other access considerations can be a key issue. Another limitation is that only evidence that focussed on a suicide-specific surveillance system(s) and their operations and characteristics was included. The relevance of suicide-specific surveillance lies in their ability to enhance the availability and quality of data on suicide, allowing for the monitoring of patterns and assessment of trends in a timely manner. For this reason, analyses on suicide using vital statistics data collections were not included. However, we recognise that high-quality vital statistics are also important for suicide prevention research, as they can provide information that can assist in monitoring. For instance, the Danish register (Helweg-Larsen, 2011) generates a comprehensive database of all deaths among Danish residents, Greenlanders and Faroese, allowing mortality research that can contribute to suicide monitoring. Likewise the national sample-based mortality surveillance system from China (S. Liu et al., 2016), contributes to suicide research as the only option for generating mortality estimates in China. Finally, we acknowledge that the exclusion of commission websites in languages other than the ones included in our searches, could have potentially led to the omission of some important data.
Conclusion
Registers of suicides are crucial in collating and tracking suicide trends over time, and establishing patterns in terms of sociodemographic factors, means, service contacts and other risk factors. Understanding these issues at an aggregate level, locally to nationally, can help inform policy and practice initiatives and allow assessment of the efficacy or otherwise of such initiatives. However, the reporting of suicides and reporting of data for suicide registers need to be sensitive to the stigma and blame that can accompany suicide. Therefore, efforts for establishing high-quality surveillance systems need to be culturally and ethically sensitive, while enabling timely access to inform tailored strategies for suicide prevention and postvention.
Footnotes
Appendix
Main characteristics of included studies.

| Publication | Register/monitoring mechanism | Informed | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author(s), year | Country | Type of publication | Name | Overview | Data linkage used | Specific benefits | Specific limitations | Insights into local vs. national needs and benefits | SP | PHI |
| Barber et al. (2013) | US | Editorial | National Violent Death Reporting System (NVDRS). Collects comprehensive data on suicide and homicide; provides far more detailed, accessible and actionable data to guide prevention and policy than are available from the individual data sources | Incident-based system. Captures all deaths that occur in a single event, rather than each in isolation | Y (Including death certificates, medical examiner/coroner reports and police records) | Lead to a plan to improve physicians’ ability to identify and treat suicidal older adults; helped secure funding for a new programme under which officers who respond to domestic violence calls conduct a lethality assessment and connect those scoring high to domestic violence services; courts that handle criminal charges may be valuable partners for suicide prevention | Not all the states have implemented NVDRS; larger states have raised the concern that they will be unable to implement the system | An expansion of NVDRS will provide better national information and equip more states and municipalities with local data for local action | Y | Y |
| Blair et al. (2016) | US | JA/Report | NVDRS | Incident-based system (see above). Cases are identified using ICD-10 codes, or by using the manner of death assigned by the coroner, medical examiner or law enforcement | Y | Creates a comprehensive picture of the circumstances surrounding violent deaths; has a primacy rule based upon assumed reliability of the sources (death certificate, coroner /medical examiner, law enforcement); informs and supports homicide prevention; The North Carolina VDRS data were used to inform stakeholders about statewide trends in suicide rates, populations at increased risk for suicide and circumstances surrounding suicide deaths. VDRS data have also been used to study suicides among veterans and active duty personnel | It is not nationally representative; availability, completeness and timeliness of data from all three required sources depends upon partnerships; for toxicology data not all decedents are tested routinely and results can be affected by differences in testing frequency across coroner /medical examiner offices; abstractors are limited to the information they received; inconsistencies in the manner of death in source documents may pose challenges, medical information regarding health conditions may be limited; variations in coding may exist | The system is not available in all states | Y | Y |
| Brooke et al. (2017) | Sweden | JA/Report | The Swedish cause of death register, a high quality virtually complete register of all deaths in Sweden since 1952. It uses the international version of the ICD codes and the rules of the WHO. Data is always recorded according to the current version of the ICD | Certification of death is by physician’s ‘notification of death’ which does not include cause of death (to the Swedish Tax Agency) and, the medical death certificate (to the National Board of Health and Welfare). Deaths should be reported to the police when: obvious or suspected unnatural death (i.e. accidents, suicides or homicides), unclear identity, suspicion of malpractice and in obscure cases | Y (The register can be linked to other national registers using the unique personal identity number [PIN] assigned to all individuals registered in Sweden) | High completeness and long history of the register means that data analysed can cover a long period of time; the use of sophisticated software to aid the coding of death certificates and identification of the underlying cause of death | A small proportion of deaths are missing an underlying cause of death; the quality of the cause of death register is affected by the quality with which the responsible physician certifies the death; the quality is also affected by the quality with which the agencies responsible for coordinating the statistics process the death certificates | NA | Y | Y |
| Cerel et al. (2016) | US | JA/ Comparative study | Kentucky Violent Death Reporting System (KVDRS). Collects information from multiple investigative sources statewide as part of the NVDRS | The Office of Vital Statistics provides a monthly electronic death certificate file to the KVDRS. Violent deaths are extracted using the ICD-10 codes meeting the CDC and Prevention’s definition of homicide and suicide from 1 January 2008, to 31 December 2010 | Y (Electronic death certificate data and coroners’ reports; all reported ED records, including observation visits, for calendar years 2008 through 2010) | NA | NA | NA | Y | N |
| Clinical Advisory Services Aotearoa (2016) | New Zealand | Explanatory notes | Coronial Suspected Suicide Data Sharing Service (CDS) established to securely notify District Health Boards of instances of suspected suicides in their regions | Notifications consist of brief identifying information on suspected suicides sourced from Coronial Services New Zealand who obtain the information when the death is notified to the Coroner (coronial data) | N | Provide timely and appropriate active outreach, support and other suicide postvention services to family and communities bereaved by suicide; coordinate inter- agency collaboration and community involvement in suicide postvention responses designed to identify potentially vulnerable persons and ensure that they are linked with appropriate supports and services; reduce community distress and anxiety and minimise risk contributing to any further suicidal behaviour; enable an accurate assessment of current local patterns of suspected suicides in order to discern possible suicide cluster or contagion | NA | NA | Y | Y |
| Cook (2012) | US | Thesis | Systems and data sources presented in the thesis: NVDRS; Ohio Mortality Public Use Statistical File (ODH), a statewide file; the Summit County Criminal Justice Information System (SCCJIS), an on-line criminal justice and court record database developed in cooperation with the three municipal courts and the Summit County Clerk of Courts which combined cover the entire urban county; Medical Examiner Data, public records on file in the Summit County Medical Examiner’s office from all suicides in Summit County from 2000 to 2005 | ODH: compiles and codes death certificates from each county; SCCJIS: includes all criminal, civil, traffic, domestic violence and appeals cases in the three municipal courts and the County court; Medical Examiner Data: data from psychological autopsies, case records and suicide notes were scanned for evidence of recent legal troubles along with a wide range of precipitating and predisposing factors | Y (NVDRS, links death certificates to other public records; SCCJIS, records across the courts are linked together using a standard format for identifiers, case descriptions and dates) | NVDRS, is especially valuable for its assessment of mental health status and utilization near the time of death based on coroner and medical examiner’s records. | NVDRS, limited in its ability to assess overall involvement in the criminal justice system (at the time when the thesis was undertaken); ODH, does not include the small number of resident deaths which occurred outside the state; SCCJIS, some offenses and claims among Summit County residents, particularly among those who live on the borders of contiguous counties, will occur outside the county | NA | Y | Y |
| Cwik et al. (2016) | US | JA/Report | The Celebrating Life surveillance system, mandates that all persons, departments and schools are responsible for reporting individuals at risk for self-injurious behaviours | An initial report describes the behavior (suicide ideation, nonsuicidal self-injury, binge substance use, suicide attempt or suicide death). The Apache Behavioral Health Services is notified and offers formal treatment services to the individual. Simultaneously, a Celebrating Life community mental health specialist seeks out the individual to complete an interview to validate the initial report and facilitate linkages to and compliance with care. The Celebrating Life team reviews the information and reaches consensus on final coding (based on the attempt method and documentation of intent to die from interview, medical charts or police reports) of the event. For deaths, police reports are the primary data source. Surveillance data are entered into an online database accessible only to Celebrating Life staff | Y | NA | NA | NA | Y | Y |
| Dodds et al. (2014) | Australia | JA/Cross-sectional study | National Coronial Information System (NCIS) | Utilises a customised classification system based upon fields and elements adapted from NHDD and the WHO-developed ICECI. Records the description of the injury and circumstances and methodology surrounding it. Information is collected in the form of free-text autopsy reports, coronial findings, police narrative reports and toxicology findings | NA | NA | One of the more problematic data fields contained within the NCIS database relates to the classification of ‘intent’ (i.e. unintentional, intentional self-harm, undetermined intent) | NA | Y | Y |
| Gahm et al. (2012) | US | Commentary | Department of Defence Suicide Event Report (DoDSER), a standardised suicide surveillance system for military services (Air Force, Army, Navy, Marine Corps), to provide data that can help refine suicide prevention approaches and ultimately prevent suicides | A web-based data management application, with standardised data collection items and analytic reporting features. The military services ask designated professionals to collect standardised records after suicides and other suicide behaviors, review the records for information related to the DoDSER items and submit the information online as determined by the Armed Forces Medical Examiner System, and for suicide attempts that result in a hospitalization or evacuation from a combat theater; suicides attempts are defined by the CDC Self Directed Violence Classification System | NA | The DoDSER collects information on suicides and suicide attempts for all branches of the military. Data collected includes suicide event details, treatment history, military and psychosocial history and psychosocial stressors at the time of the event | The use of death certificates for surveillance purposes; death certificates had misclassifications of deaths and suicides, a limited amount of information included; problems associated with existing sources of information on suicide attempts information; systems utilised different definitions for a ‘suicide attempt’ and other self-harm behaviors, therefore creating problems with standardization, comparison and synthesis of data | NA | Y | Y |
| Goodwin et al. (2015) | US | Commentary | The Historical Administrative Data Study (HADS), provides data for the U.S. Army to assess the prevalence of suicidal ideation and suicide attempts in Army personnel and to identify risk factors | Comprises historical health and administrative records from personnel in active duty between 2004 and 2009 and includes data from more than 38 different Army and Department of Defence (DoD) data systems | Y | Using HADS overcomes the issue of self-reporting and can also inform other military populations | NA | NA | Y | Y |
| Gunnell et al. (2011) | UK | Editorial | The Office for National Statistics (ONS), produces the official suicide statistics | Suicide statistics in England and Wales are derived from death certificates issued after coroner’s inquest into unnatural or unexpected deaths. The ONS combines suicide and open verdict deaths. | N | NA | Underestimation of suicide rates (suicides may be difficult to identify when some methods are used and intent is unclear); narrative verdicts present coding difficulties for the ONS (when suicide intent is unclear such deaths are coded as accidents) | NA | N | N |
| Hajebi et al. (2013) | Iran | JA/Cross-sectional study | National Registration System of Suicide Behaviors in Iran, a registration system for suicide behaviors, designed in the Mental Health Office of the Ministry of Health in Iran | Deputy of Health is responsible for registering, analysing and controlling suicide behaviors in the catchment areas of national Universities of Medical Sciences. A case report questionnaire in the form of software with users’ manual was prepared to ensure systematic and uniform portal data collection. The universities were responsible for data collection in their public and private health centres | NA | NA | Could be some obstacles during data collection: the societal stigma of mental disorders and suicidal behaviors; insurance companies could inhibit suicide registration in the health system because patients who attempt suicide are not covered by the insurance companies; a limited cooperation between the Forensic Medicine Organization and the Ministry of Health; cases primarily referred to the private health sector may remain unreported | The quality control of data collection is more accurate in local studies compared to national ones; therefore, the registration process is more efficient | Y | NA |
| Ikeda et al. (2014) | US | JA/Report of 28 data systems | Data and Surveillance Task Force (DSTF), established to help improve and expand the information available about suicide and suicidal behavior. For improving national data systems for suicide surveillance | NA | Death records: intensive investigation by medical examiners/ coroners for some causes of deaths; intent of the injury is specified; ongoing data collection. Health care provider records: narrative fields can provide more detailed information; data are derived from existing records, no de novo data collection required; some data on charges or cost of care are available; includes geographic details; might be helpful for emerging health issues. Population-based surveys: flexible, but changes to the structure of the survey might take time; anonymity of the respondent may promote truthful responses; can be designed to focus on factors associated with suicidal behavior such as socioeconomic status; timeliness. Health insurance claims: can detect small changes in the occurrence of events because of the large number of records; both initial visit and outcomes can be tracked; may provide information on the patient’s medical history prior to the event; may be able to track continuity of care; timeliness | Death records: capture limited information; cannot be easily modified owing to the need to conform to national and international standards; processing of data can delay timeliness; some demographic factors could potentially be misclassified because information is collected from next of kin or friends of the deceased; there can be variation among medical examiners/coroners in death investigation and certification practices. Health care provider records: limited to inform available in the medical record; the number of records specific to suicide could be small; comparison of data across systems can be difficult because systems may collect data in diverse formats or differ in how records are organised; timeliness can be an issue owing to delays in processing administrative records; key data elements are frequently missing or not collected; may only contain data on events or cases (numerator), rarely has information on the population at risk (denominator); generation of the surveillance data is not the primary function of the system. | NA | N | N | |
| Because the information is collected for other purposes, the use of standardised case definitions and the quality of the data collected can be challenging. Population-based surveys: the ability to provide estimates for subpopulations might be limited; can be expensive to administer; analysis can be complicated if the survey uses a complex sampling design; relies on self-report, which may be inaccurate; as response rates decline, selection bias may increase, resulting in a reduction in the representativeness of the responses (particularly with telephone surveys); time/space constraints of survey administration may limit the number and types of questions that can be included. Health insurance claims: is not designed for surveillance; only the population of persons insured by the carrier are included in the data set, patients who change insurance providers are no longer in the system; external cause of injury may be missing or limited; access to the data may be limited depending on the affiliation of the user | ||||||||||
| Jiang et al. (2015) | US | JA/Empirical article | Rhode Island Violent Death Reporting System (RIVDRS), a population-based surveillance system that collects all violent deaths that occur in Rhode Island. | RIVDRS collects violent death data from four major data sources: death certificates; medical examiner reports, including toxicology reports; law enforcement reports, including Supplementary Homicide Reports and National Incident-Based Reporting System reports, where available; and, crime laboratories. Details demographic characteristics, mechanisms of injury, location of death, toxicology information, circumstances preceding the deaths, etc. Data are collected and stored in a nested manner. RIVDRS data can be analysed at incident, victim or suspect levels | Y | The system combines information from the different data sources and provides a complete picture of violent deaths; is able to link records on violent deaths that are related and happened within 24 hours of each other; annual RIVDRS data sets allow for trend analyses in Rhode Island; the same data are collected in 32 states allowing comparison with other states; the NVDRS implemented a new web-based system, which is an improved system and has enhanced data entry; is state-based, therefore states can choose to capture data beyond what the CDC collects | In Rhode Island, law enforcement does not release homicide data until the case has been adjudicated, and this can result in very long time lags; Rhode Island has not been able to obtain data from the Massachusetts Violent Death Reporting System on Rhode Island victims who died in Massachusetts; RIVDRS is in the process of determining how to best evaluate timeliness, completeness and data quality of the programme, and the level of missing data after a given time period | NA | Y | NA |
| Kaplan et al. (2017) | US | JA/Empirical article | NVDRS | The NVDRS uses data from coroner and medical examiner reports, death certificates, law enforcement reports and toxicology reports | Y | Provides accurate, timely and comprehensive surveillance data, neighbourhood factors. | The system is not national (32 states); lack of standardization in collection of the circumstances preceding death and in collecting mental health and substance use information; death certification process is sometimes influenced by assumptions of individual C/MEs | NVDRS is limited by the assortment of medicolegal death investigation systems in the participating states | Y | Y |
| Kemp and Bossarte (2012) | US | Editorial | The Veterans Affairs’ (VA) suicide event reporting system, known collectively as the Suicide Prevention Applications Network (SPAN) | It has transitioned from an aggregate spreadsheet submitted monthly to an electronic reporting system capable of achieving near ‘real time’ surveillance of suicide events among veterans | Y (SPAN and DoDSER) | Standardised nomenclature increases the utility of suicide event data by providing a mechanism for comparability across systems and time | NA | NA | Y | Y |
| R. T. Liu et al. (2013) | US | JA/Cross-sectional study | NVDRS | Incident-based system | Y | NA | Is not nationally representative | Regional variability in access and tendencies to adopt different suicide means | Y | Y |
| NCISH (2023) | UK | Explanatory notes (meth-odology) | National Confidential Inquiry into Suicide and Safety in Mental Health (NCISH) | The NCISH is a project that collects information on all suicides in the UK since 1996. The core dataset is a national consecutive case series that examines the circumstances surrounding the deaths by suicide of people under the recent care of specialist mental health services. To collect relevant information, the NCISH has developed a questionnaire encompassing demographic and clinical information. The questionnaire is regularly updated to reflect current concerns in suicide prevention and changes in practice. | NA | Allows the identification of common factors in the management and care of people that recently attended specialist mental health services and died by suicide. Further, the NCISH enables providing recommendations to decrease suicide rates among people receiving specialist mental health care. The safety of all people attending specialist mental health services can also be improved. | NA | NA | Y | Y |
| Rolland-Harris (2019) | Canada | Commentary | Medical Professional Technical Suicide Reviews (MPTSR), register/database comprising each probable or confirmed suicide reported to the Canadian Armed Forces | Investigation collects information on demographic and risk factors, it is based on the US DoDSER. The MPTSR section of the annual suicide report presents descriptive data on the frequency of a number of relevant factors related to suicide, including access to care prior to death and pre-enrolment risk factors | Y (links to recruitment and other health records) | N | Ecological and atomistic fallacy of suicide evidence (case level vs. population level) | NA | Y | N |
| Saar et al. (2017) and Olds et al. (2018) | Australia | Review Letter to the Editor | National Coronial Information System, a national internet-based database of coronial information | Information on deaths reported to coroners is entered as coded fields, structured free text and four searchable full text documents are attached for each case (police report of death notification to the coroner, autopsy and toxicology reports and coroners’ findings). A standardised classification structure is used. Coding schemes are derived from: the NHDD, ICECI and internally developed schemas. Other classifications employed include the ANZSCO, the ANZSIC, the TOOCS and the ICD-10 | NA | Quality assurance process ensures that the data complies with the standardised code sets and accurately reflects the facts of the death; the comprehensive data allows users to search and review the death event and the involvement of risk factors and the contribution of additional factors; user guides are available to all new users to facilitate optimal use of the database | Olds K, et al: the database is limited by the information that is provided to it; the ability to extract data was limited by jurisdictional ethics requirements to access data and data not having been uploaded; lack of standardization of post-mortem examination reports between and within coronial jurisdictions | NA | Y | Y |
| Stene-Larsen et al. (2018) | Norway | JA/Descriptive study | Nationwide registry on primary health care use, established to explore the role of the primary health care services prior to suicide and in the follow-up of the suicide bereaved | Links the four national health registries: the Norwegian Cause of Death Registry, provides information about the cause and date of death; Norwegian Prescription Database, collects and process data on drug consumption; the Primary Health Care Database, contains data on claims for reimbursement of fee-for-service among GPs and specialists in emergency units and in primary health care services; Norwegian Patient Register, covers both inpatient and outpatient treatment for specialist health care services | Y (the four national health registries and Statistics Norway) | Access to a large population representative sample, with long follow up and potential to link a range of variables from other data-sources if necessary; potential to study associations between rare exposures and rare outcomes in a very large population with almost complete follow up | It is challenging to gain access to each registry; restrictions with regard to possible research themes must be expected; all research approvals are time-limited; the large amount of data involved in registry-based research requires specialised expertise; do not cover as much information as would have been optimal | NA | Y | Y |
| Sutherland et al. (2018) | Australia | JA/Descriptive study | Victorian Suicide Register (VSR), a state-based suicide surveillance system to store detailed and up-to-date information on all people who die by suicide. The VSR is placed within the Coroners Court of Victoria | Information coded are from the coroner’s investigation material, including police report, post-mortem forensic medical and scientific reports and the coronial brief prepared by the coroner’s investigator. All data are recorded in Microsoft Access. Coders record the presence or absence of a particular event or circumstance, additional information is entered as free text | Y | Affords opportunities to explore new avenues for prevention; high sensitivity, high data quality few missing observations; fidelity processes for quality; accessible | Several data fields; sources of info are multiple and complex; delays in open cases and time issues can impede ‘real time’ monitoring; variability/quality in informant or source information; cross sectional data interpretation; no ability to do case by case comparisons | Can stimulate local action on suicide prevention planning and inform community. Comprehensive information about those who die by suicide and their wider social circumstances is a necessary prerequisite for guiding local decisions on suicide prevention planning and action | Y | Y |
| Vijayakumar et al. (2020) | India | JA/Data analysis | SPIRIT’s Suicide Surveillance System | A community suicide surveillance system established to collect baseline data on suicidal behaviour as part of the Suicide Prevention and Implementation Research Initiative (SPIRIT) project. The SPIRIT trial allowed the development and implementation of the system in the period from August 2018 to July 2019 | N | The comprehen siveness of suicide data was improved and the number of suicides under-reported reduced. The system can complement the health system or registration system records and provide data where such systems do not exist | Use of third-party informants; the obtention of information on suicide attempts; and the incomplete recording of all suicide attempts registered at the hospitals. Informants were concerned about confidentiality of information of suicide attempts that could result in conflict with survivors and their families and/or in being involved in legal problems | NA | N | N |
| Williams et al. (2010) | Australia | JA/Empirical article | Queensland Suicide Register (QSR), a comprehensive data base of suicide mortality, managed by the Australian Institute for Suicide Research and Prevention (AISRAP) at Griffith University | Information is gathered from: the police report to the Coroner, the post mortem report, and toxicology results. Police report, contains demographics, the circumstances surrounding the death and a psychological autopsy questionnaire | NA | May lessen underreporting | NA | NA | Y | Y |
Note. ANZSCO = Australian and New Zealand Standard Classification of Occupations; ANZSIC = Australian and New Zealand Standard Industrial Classification; CDC = Centers for Disease Control and Prevention; C/ME = coroner and medical examiner; Des = descriptive; ED = emergency department; GP = general practitioner; ICD-10 = International Classification of Diseases 10th revision; ICECI = International Classification of External Causes of Injury; JA = journal article; Mun = municipalities; N = not; NA = not available; NEISS = National Electronic Injury Surveillance System; NHDD = National Health Data Dictionary; PHI = public health interventions; SP = suicide prevention; TOOCS = Type of Occurrence Classification System; UK = United Kingdom; US = United States; WHO = World Health Organization; Y = yes.
Acknowledgements
The authors acknowledge the contribution of Tim Albion and Brian Stokes who provided technical assistance in the development of the original review. We would also like to acknowledge the general support provided by Prof Brett McDermott and Prof Lisa Foa, Co-Directors of the Tasmanian Centre for Mental Health Service Innovation with DC and to other members of the Tasmanian Centre for Mental Health Service Innovation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Evaluation of the Tasmanian Suicide Register, Tasmanian State Government [2020-2021]; the Evaluation of the Tasmanian Suicide Prevention Strategy 2023-2027 Implementation Plan One [2023].