
Abstract
Background:
Conflict-induced displacement is a greater risk factor for mental health challenges, especially in countries where people have limited access to mental health services. This study examined the prevalence of mental distress, post-traumatic stress disorder (PTSD), and their relationship with key demographic variables and psychological capital among conflict-induced Internally Displaced People (IDP) in the Wag-Hemra Zone, Amhara Region, Ethiopia.
Methods:
The study used a cross-sectional quantitative design, and simple random sampling was used to recruit 367 IDPs from the Weleh IDP camp in Sekota town. The Psychological Capital Questionnaire (PCQ 12), Kessler Psychological Distress Scale (K 10), and Post-traumatic Stress Disorder–Civilian Version (PCL-C) scales were used to collect data. STATA version 2021 was used to analyze data.
Results:
The prevalence of mental distress and posttraumatic stress disorder (PTSD) was 63% and 48 %, respectively. Mental distress and PTSD were higher among female participants (M = 27.4, 45.7), those who experienced rape (M = 32.6, 55.5), witnessed murder (M = 25.2, 46.1), widowed (M = 30.9, 44.9), illiterate (M = 28.1%, 47.2), and adolescents (M = 27.6, 45.5). Stepwise regression analysis indicated that psychological capital is a significant negative predictor of mental distress and PTSD (p = .000), with 26% mental distress and 20.9% variance in PTSD accounting for psychological capital, with self-efficacy being the strongest predicting component of psychological capital.
Conclusion:
The study underlined that mental health efforts should target enhancing psychological capital as the critical element in mitigating the psychological impacts of war and displacement. Training on improving self-efficacy, utilizing the solid spiritual and religious base of the IDP community to raise hope and optimism, and leveraging the communal culture to foster resilience could help reduce mental distress and the effects of PTSD among IDPs in the study area.
Keywords
Introduction
The 12th century has seen a significant increase in armed conflicts, leading to a rise in forced internal displacement. Internally Displaced Persons are people or groups who forcefully leave their localities due to manmade or natural crises and remain within the borders of their own country (Madoro et al., 2020). According to the IDMC (2022), of 55 million displaced globally, 48 million were displaced due to armed conflict and violence. New geopolitical dynamics intensify these conflicts, leading to more complex and widespread displacement scenarios. The situation underscores the escalating global humanitarian challenge of forced displacement (Batool, 2023).
Ethiopia exemplifies this trend of increasing internal displacement. A report by the IOM showed that, as of June 2024, there are more than 4.5 million IDPs in Ethiopia across 4,240 sites that are assessed and accessible to document (IOM, 2024). The report added that the leading causes of displacement are conflict (73%), drought or climate (12%), and other (15%). Yigzaw and Abitew (2019) further explained that these displacements are driven by political instability, ethnic tensions, and resource conflicts, creating a complex and volatile displacement landscape in Ethiopia. The border disputes and conflicts, particularly in the northern regions, including the Amhara and Tigray regions, have significantly exacerbated this issue (Fisseha et al., 2023). Tigray (1.1 million) and Amhara (1.4 million) regions bear the highest burden of IDPs displaced by conflict and returning IDPs combined. Somalia (1.2 million) and Oromia (1.1 million) are also among the top four regions with IDPs displaced mainly by drought and climate problems (IOM, 2024). This study focuses on Amhara region, particularly the Wag Hemra zone, that hosts around 85 365 IDPs since the conflict began (Makango et al., 2023).
The impact of displacement extends beyond physical relocation, affecting mental and emotional well-being (Tesfaw, 2022). It is well documented that violence-related displacement leads to significant psychological trauma, including anxiety, depression, and PTSD, a situation likely mirrored in the Ethiopian context (Tai et al., 2021). Despite the increasing numbers of IDPs in Ethiopia, Madoro et al. (2021) noted that their mental health needs have been relatively under-addressed. Multiple factors contribute to the lack of mental health-focused services. The health system in the conflict-affected areas has collapsed as health personnel evacuated and medical supplies discontinued due to the war and lack of transportation (Arage et al., 2024). In addition to that, the focus on immediate life-saving issues in displacement contexts overshadows mental health issues. According to Allotey and Reidpath (2019), in such emergencies, mental health is frequently deprioritized in favor of addressing more immediate physical needs and security concerns. This trend is particularly evident in the northern Ethiopian context, where the complexity of displacement challenges often leads to an underemphasis on long-term mental health care and support (Madoro et al., 2020). It was also reported that limited awareness about mental health across local and state-level leadership contributed to the inattention to addressing the pressing needs among IDPs (Makango et al., 2023). Most importantly, limited access to conflict-affected areas not only hindered the provision of services, but also limited efforts to investigate and document the magnitude of mental health crisis among IDPs (Kemei et al., 2023).
Internally displaced people often possess positive psychological capital, which can mitigate mental health issues like PTSD (Idemudia et al., 2020). According to George and Adelaja (2021), despite the challenges they experience, displaced populations often exhibit remarkable resilience and adaptability. They found that hope, optimism, and self-efficacy are crucial in helping displaced individuals cope with trauma and rebuild their lives. However, the specific application of these findings to Ethiopian IDPs remains under-researched. Mainly, there is no known study with a particular focus on mental health challenges among IDPs in the Wag Hemera zone, an area that has been devastated by the conflict. Hence, this study aims to fill this gap by investigating not only the mental health challenges experienced by IDPs but also their psychological capital and coping mechanisms that buffer the grave effects of forced displacement. The study answers the following questions:
What is the prevalence of mental distress and posttraumatic stress disorder among conflict-induced displaced people in the study area?
Is there a statistically significant mean difference in symptoms of PTSD and mental distress across key demographic variables?
What are the independent contributions of psychological capital components to mental distress and posttraumatic stress disorder?
Methods
Research design and setting
A cross-sectional quantitative design was employed in this study to answer the research questions listed above. The study was conducted in the Wag Hemra zone of the Amhara region in Ethiopia. Specifically, participants were recruited from the Weleh IDP camp in Sekota town. Sekota is the capital of the Wag Hemera zone of the Amhara region in north Ethiopia and is home to one of the largest IDP centers in the country (Mengstie et al., 2023). The study was conducted from the August 25, 2022, to March 17, 2023.
Procedure, sampling and data collection
The study was reviewed and approved by the Research Review Committee of the University of Gondar, and a letter of support was obtained from the Department of Psychology to facilitate recruitment. The questionnaires/measures were pilot-tested with 40 participants to ensure their applicability. Before the primary data collection, participants were oriented about the purpose of the study, confidentiality, and their rights and expectations. Oral consent was gained before data collection. Three MA in psychology students and two BA clinical psychology graduates who work in the IDP camps collected data.
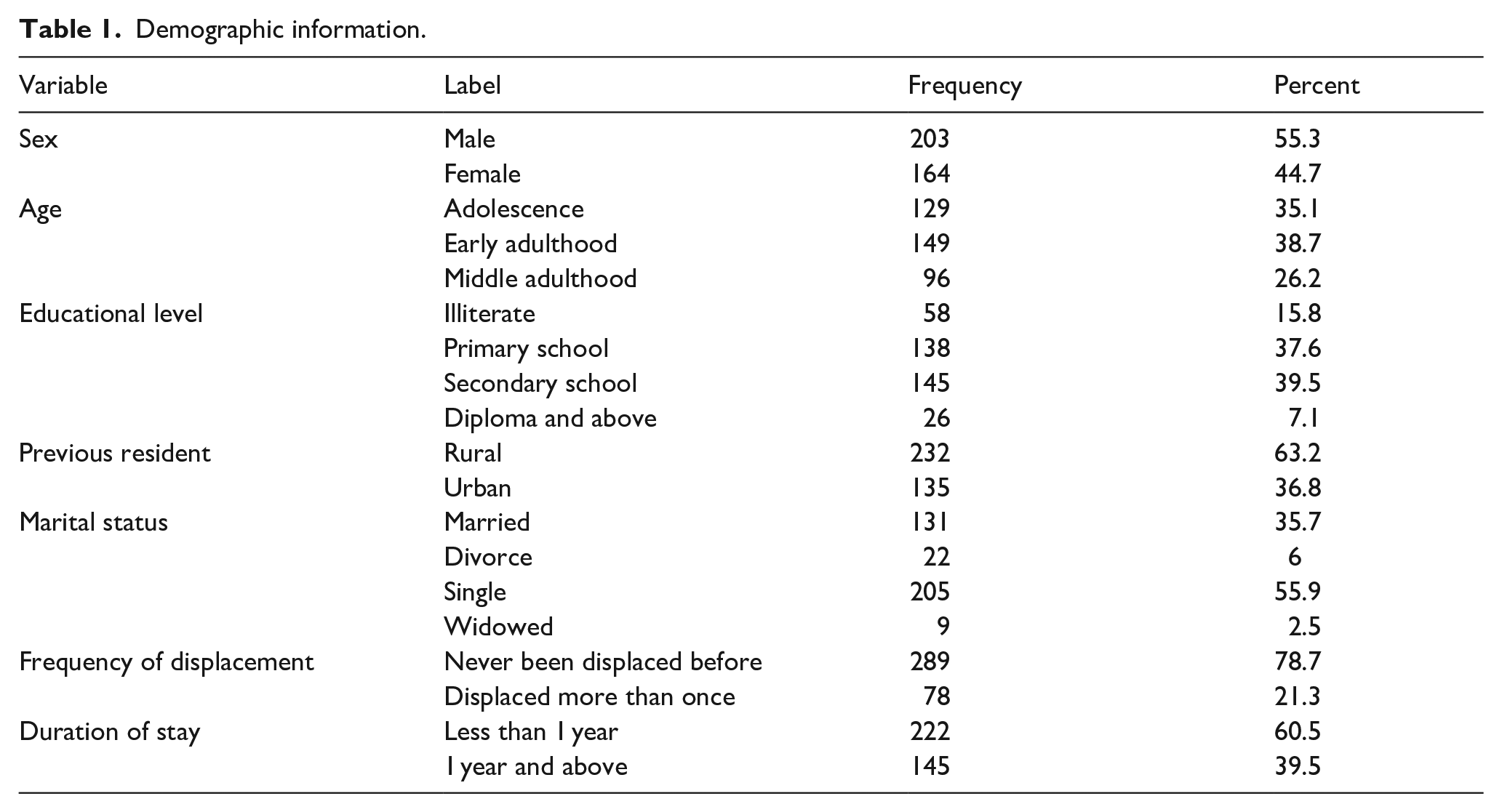
A total of 367 participants were recruited from the Weleh IDP camp based on the Krejcie and Morgan (1970) sample determination formula. See Table 1 for detailed demographic information. All participants were recruited using a simple random sampling technique and aged 18 and above using the IDP list of the Weleh camp. Quantitative data were collected using structured measures, which are presented below.
Demographic information.
Variables and measures
Variables to measure the prevalence of traumatic experience included rape, family or close family murder, witnessing traumatic evidence, property damage/loss, physical abuse, multiple trauma, mental distress, and PTSD. Independent variables included key demographic variables, including education, traumatic experience, marital status, gender, previous place of residence (urban vs. rural), duration of stay, and frequency of displacement. In addition, psychological capital (self-efficacy, hope, optimism and resilience) was used as an independent variable, and symptoms of mental distress and PTSD were assessed as dependent variables.
Psychological Capital Questionnaire (PCQ 12) was adapted to measure psychological capital (Luthans et al., 2007). PCQ 12, which has four components: self-efficacy, hope, optimism, and resilience, was used. In this study, the internal reliability of psychological capital was .789, and the reliability of hope, self-efficacy, resilience, and optimism was .714, .719, .755, and .838, respectively. Kessler Psychological Distress Scale (K 10) was used to measure psychological distress (Kessler et al., 2002). For this study, the reliability was .733. Last, the Post-traumatic Stress Disorder–Civilian Version (PCL-C) scale was also adapted to measure PTSD, and its reliability for all 17 symptoms was .96 (Weathers et al., 1993).
Analysis
Quantitative data were checked for completeness and analyzed using STATA version 2021. We computed descriptive statistics to identify the frequency and prevalence of traumatic experience and conducted one-way ANOVA, independent t-test, and step-wise regression.
Results
Prevalence of traumatic experience, mental distress and PTSD of respondents
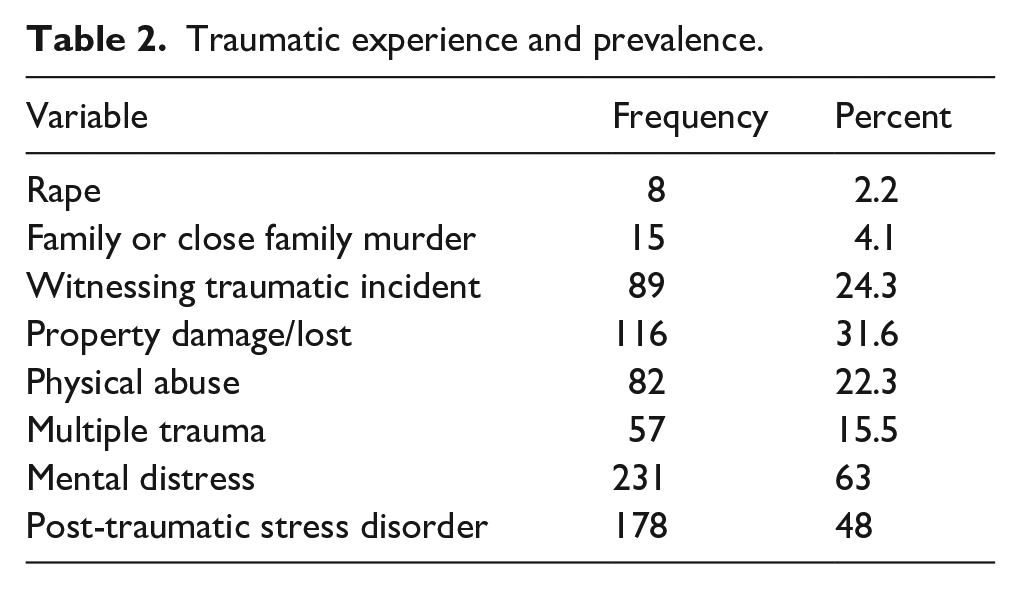
As shown in Table 2, 8 (2.2%) females were forcibly raped during wartime, 116 (31.6%) participants reported that their property was damaged, and 89 (24.3%) participants witnessed while others were abused either sexually, physically, or murdered. Moreover, 57 (15.5%) experienced multiple trauma, and the other 82 (22.3%) experienced physical abuse. Results also showed that 178 (48%) of respondents met the criteria for PTSD, and 231 (63%) respondents reported having mental distress.
Traumatic experience and prevalence.
Differences in symptoms of PTSD and mental distress across key demographic variables
As indicated in Table 3, there was a statistically significant mean difference in mental distress among illiterate (M = 28.10, SD = 7.45), primary schoolers (M = 27.15, SD = 6.23), those who completed secondary school (M = 26, SD = 6.38) and those completed diploma and above (M = 23.8, SD = 6.67, F (3, 363) = 3.252, p < .05). A Turkey HSD test revealed that the mean score of illiterate people in mental distress is significantly different from that of those with a diploma and above. A statistically significant mean difference in mental distress score was also found based on participants’ traumatic experience (F (5, 361) = 7.824, p < .001). The post hoc comparisons test indicated that the mean distress score of forcibly raped respondents (M = 32.62, SD = 3.66) is statistically higher than that of those who witnessed murder (M = 25.16, SD = 5.97) and those who lost property (M = 24.89, SD = 5.78). In addition, respondents who experienced the murder of their family or close family members (M = 30.20, SD = 5.05) demonstrated a significantly higher mean of mental distress compared to those who had lost their property (Table 3).
One-way ANOVA result in symptom of mental distress and PTSD across key demographic variables.
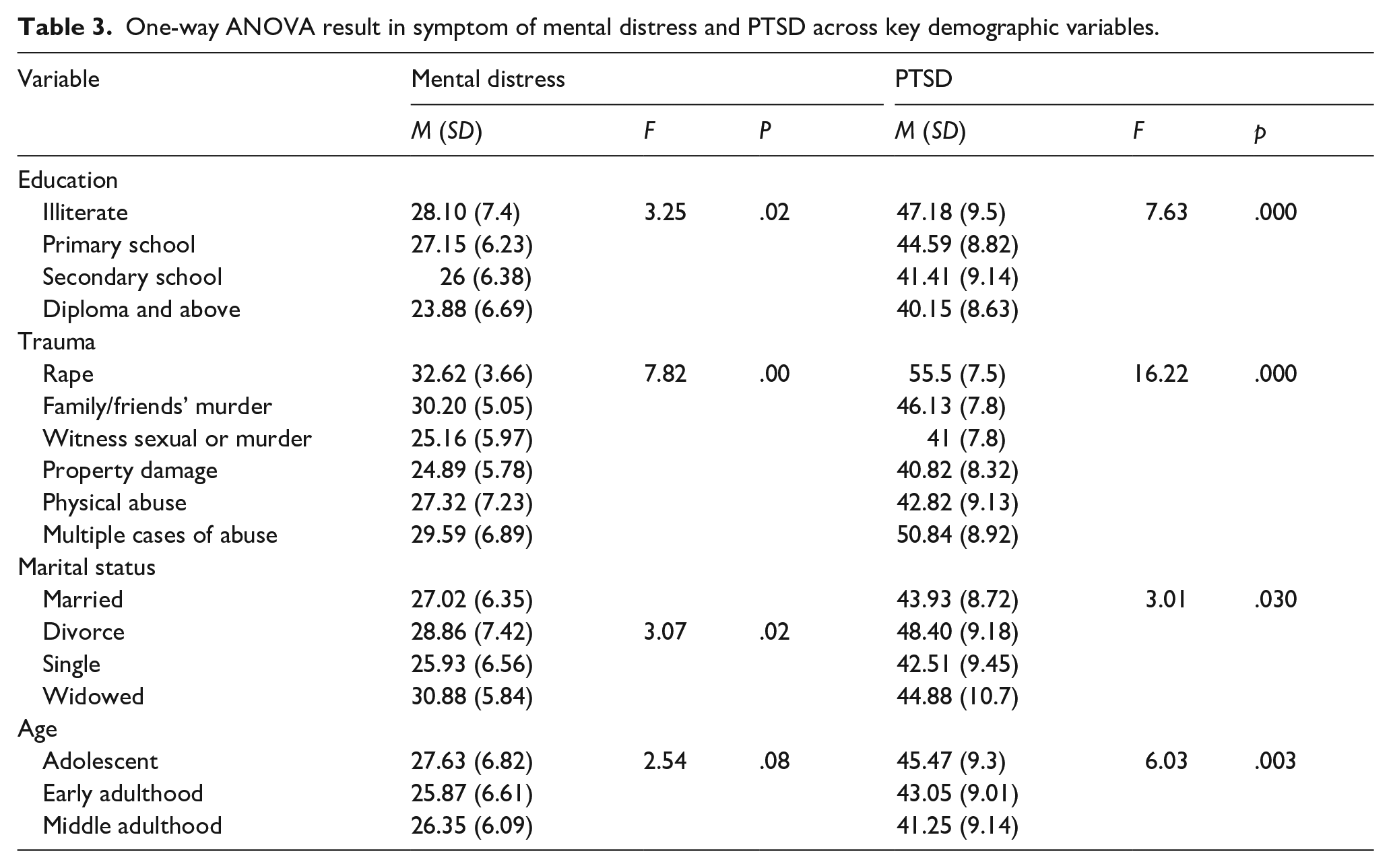
A statistically significant mean difference in the scores of mental distress between those who witnessed trauma and people who experienced multiple traumas (M = 29.59, SD = 6.87, p < .05 was observed. The mean score for PTSD symptoms differs significantly across traumatic experiences (F(5, 361) = 16.228, p = .000). There was also a statistically significant difference between displaced respondents who were forcibly raped (M = 55.50, SD = 7.5) and those who witnessed sexual or murder trauma (M = 41, SD = 7.81, p = .001). Furthermore, there was a significant difference in PTSD symptoms between those who had been subjected to multiple forms of abuse (M = 50.84, SD = 8.92) and those who had witnessed traumatic events (p < .001). Those who had witnessed murder (M = 40.82, SD = 8.32, p < .001) and experienced physical abuse of IDPs (M = 42.82, SD = 9.13) had higher mean PTSD scores than those who had lost their property (Table 3).
Table 3 also shows there is a significant difference in the mean score of PTSD based on marital status (F (3, 363) = 3.014, p < .05). However, there is no significant mean difference in PTSD symptoms across other groups (p > .05). There was a statistically significant mean difference in the score of PTSD symptoms across educational levels (F (3, 363) = 7.63, p < .001). Illiterate participants (M = 47.18, SD = 9.50) showed significant higher PTSD than secondary school (M = 41.41, SD = 9.14, p = .000) and those who completed a diploma or higher (M = 40.15, SD = 8.63, p < .05). In terms of age difference, the mean score of PTSD symptoms differed significantly across adolescence (M = 45.47, SD = 9.34), early adulthood (M = 43.05, SD = 9.01), and middle adulthood (M = 41.25, SD = 9.14) (F (2, 364) = 6.034, p < .05).
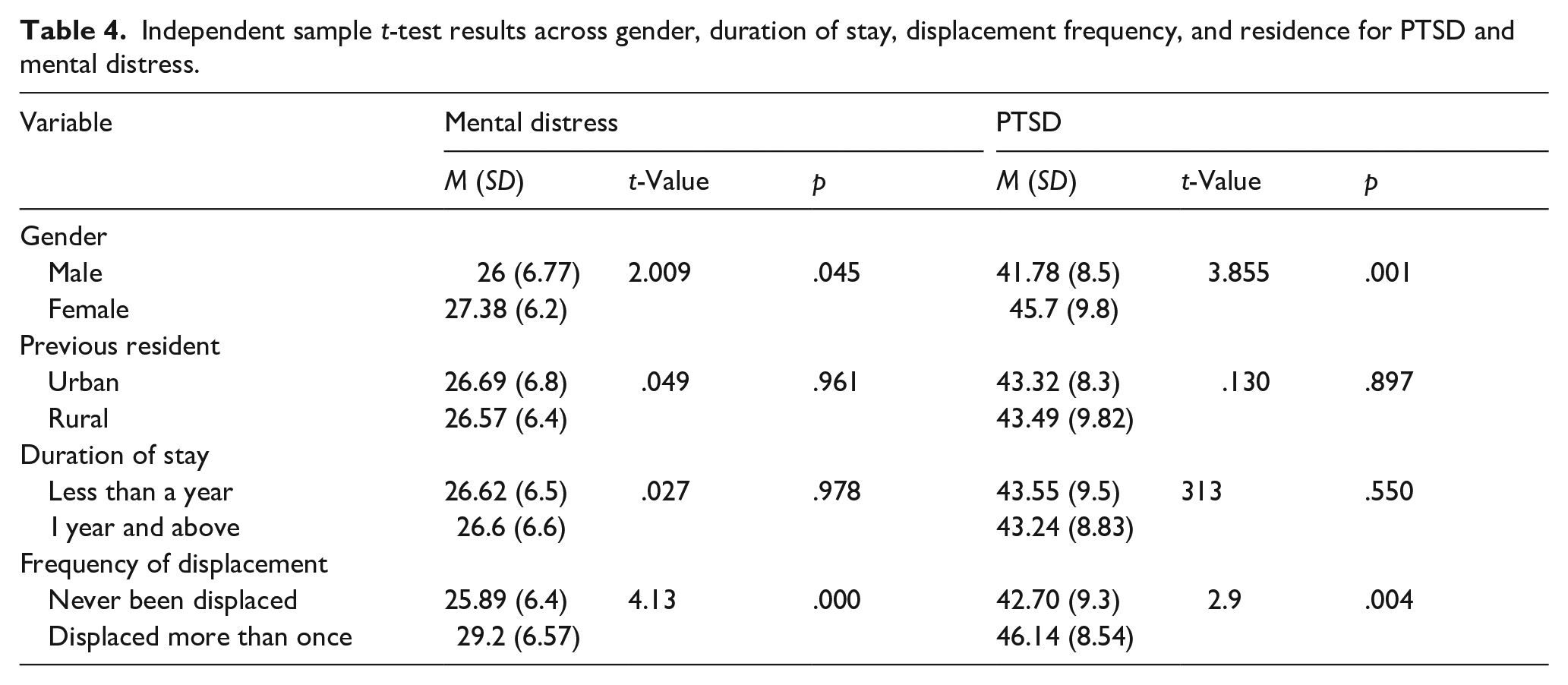
As indicated in Table 4, there is a significant mean difference in mental distress between females (M = 27.38, SD = 6.28) and males (M = 26, SD = 6.77); t (364) = 2.009). In addition, a significant difference in mental distress between participants who had never been displaced before (M = 25.89, SD = 6.41), and those who had been displaced more than once (M = 29.29, SD = 6.57; t (365) = 4.131, p < .01) was found. Regarding PTSD score, females score significantly higher (M = 45.47, SD = 9.81) than males (M = 41.78, SD = 8.52) (t (364) = 3.855, p < .01). There is also a significant difference based on the frequency of displacement.
Independent sample t-test results across gender, duration of stay, displacement frequency, and residence for PTSD and mental distress.
Independent contribution of psychological capital variables on mental distress and post-traumatic stress disorder
Stepwise regression analysis was conducted to determine the independent prediction of psychological capital variables, including hope, resilience, optimism, and self-efficacy on mental distress and PTSD. The four variables have been found to have multiple associations of 0.51 with dependent variables, which may imply a moderate level of prediction, as indicated by the R-value in model four (Table 5).
Multiple linear regressions stepwise method result of psychological capital to mental distress and PTSD.
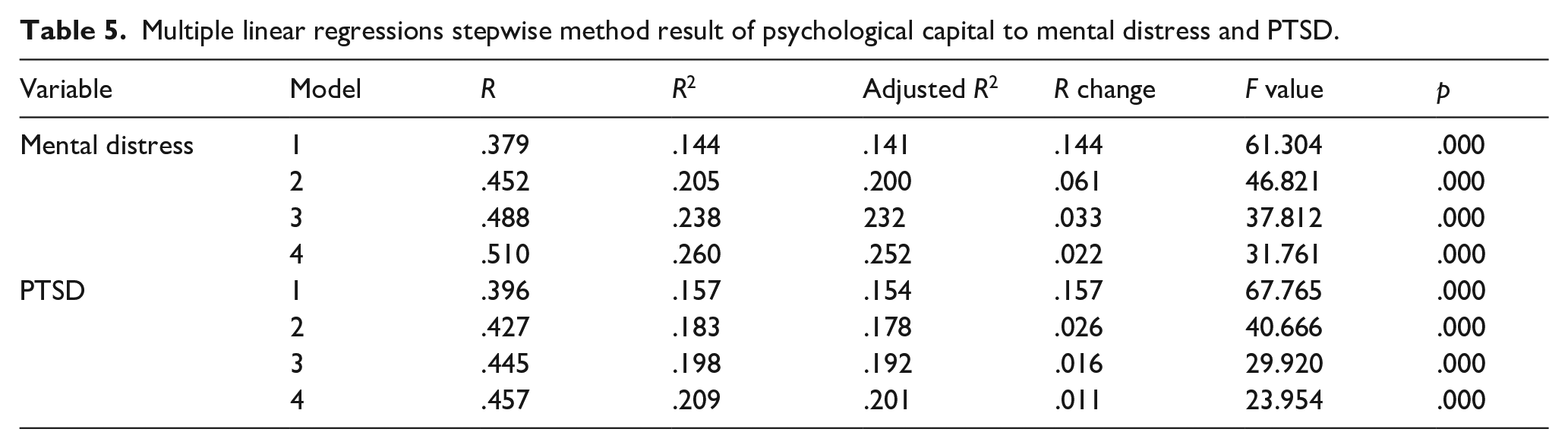
As indicated in Table 6, self-efficacy is the variable with a maximum prediction for mental distress with a t-value (−3.149) significant at 0.01 level. As such, about 14.4% of the total variance in mental distress is predicted by self-efficacy (F (1, 365) = 61.304, p < .01), as the R2 change value indicated. In model 2, a regression test was conducted, adding hope with efficacy so that the explained variance in mental distress increased from 14.4% to 20.5% (F (2,364) = 46.82; p < .01). Self-efficacy and hope together account for 20.5% of the variance in mental distress variable. Hope predicted an additional 6.1% of the variance in mental distress. In model 3, optimism was added to the model with hope and efficacy, and the explained variance increased from 20.5% to 23.8% at (F (3, 363) = 37.81, p < .01). Independently, optimism predicts 3.3 % of the variance in distress. Resilience alone accounts for 2.2% of the variance in mental distress (F (3, 362) = 31.761, p < .01).
Coefficient table of stepwise method result.
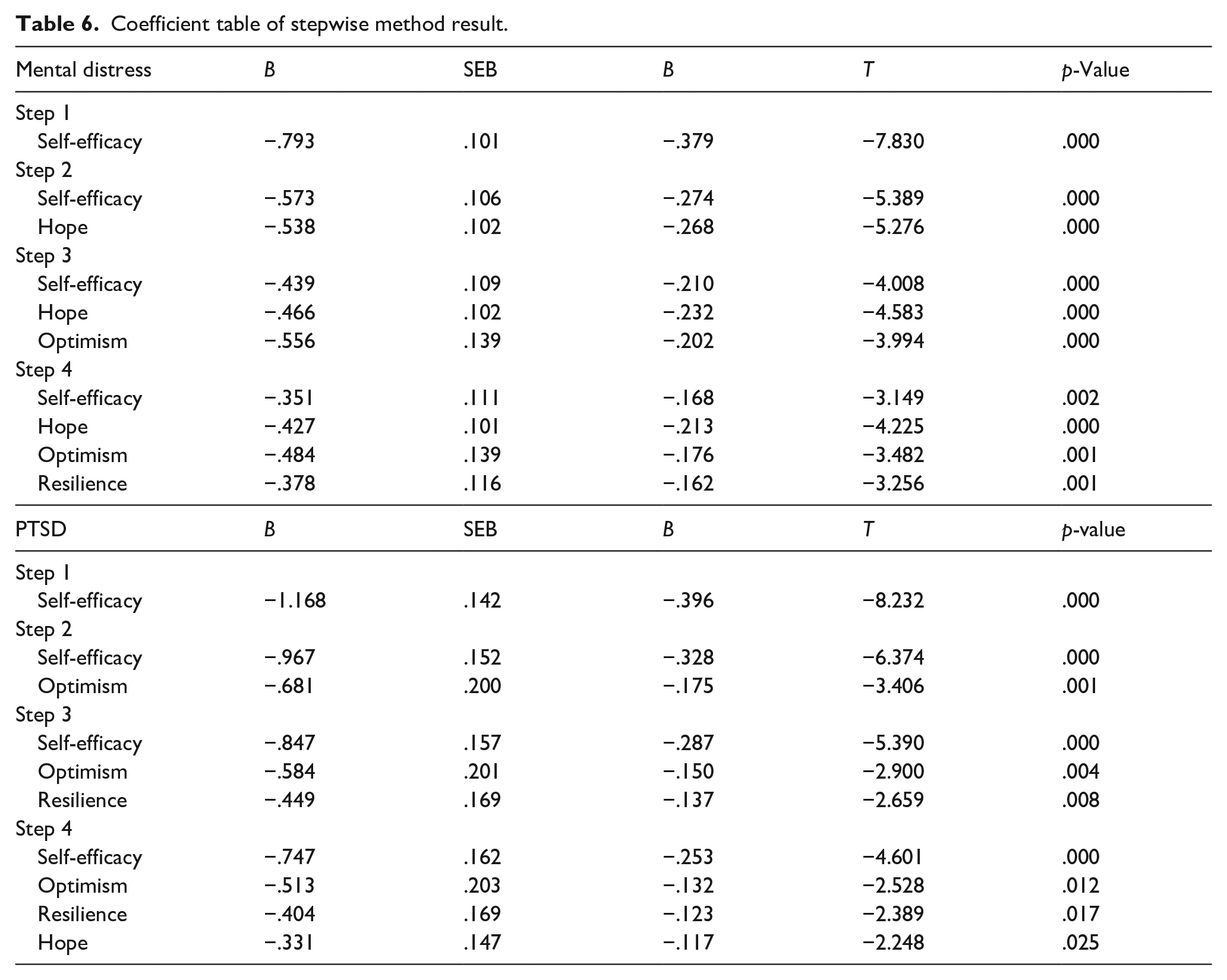
In model 4, the explaining variance increased from 23.8% to 26%. Therefore, taking hope, resilience, efficacy, and optimism together explains 26% of the variation in mental distress. The ANOVA results in model 4, with all variables considered (hope, self-efficacy, resilience, and optimism), showed that the regression model was a good fit for the data (significant) with (F (4, 362) = 31.761, p < 0.01). The coefficient table in model four revealed that the beta (β) value of self-efficacy was −.168, t = −3.149, p < .001. This refers to an increase of one unit in self-efficacy associated with a decrease of −.168 standard deviation in mental distress among IDPs. The beta (β) value of hope was −0.213 (β = −.213, t = −4.225, p = 000). An increase of one unit standard deviation in the predictor variable (hope) will result in a decrease .213 standard deviations in the criterion variable (mental distress). The optimism beta (β) value was −.176, and one unit increase in optimism resulted in a.176 unit decrease in mental distress. For the rest of the variables, the change of one standard deviation in resilience, efficacy, and optimism resulted in decreasing .162, .379 and .202 standard deviations in mental distress, respectively. Independently, 14.4%, 6.1%, 3.3% and 2.2% of distress were predicted by self-efficacy, hope, optimism, and resilience, respectively.
Table 6 also shows the stepwise multiple linear regression method for determining the independent contribution of psychological capital to PTSD. The multiple correlations between dependent and independent variables were .457. Self-efficacy accounted for 15.7% of the variance in posttraumatic stress disorder (F (1, 365) = 67.765, p < .01). In Model 2, after adding optimism along with self-efficacy, the two variables explained 18.3% of the variance (F (2, 364) = 40.66, p < .01). Optimism significantly explained 2.6% of PTSD. In Model 3, efficacy, optimism, and resilience were account for 19.8% of the total variance. Resilience alone predicts 1.6%. In the last model (4), total psychological capital explained 20.9% of the variance in PTSD. As the coefficient Table 5 showed, in the last model, self-efficacy (β = −.253, t = −4.601, p < .01) was the strongest predictor, followed by optimism(β = −.132, t = −2.528, p < .05), resilience (β = −.123, t = −2.389, p < .05) and hope (β = −.117, t = −2.248, p < .05). In addition, an increase of one unit standard deviation in self-efficacy, optimism, hope and resilience resulted in a decreasing .253, 132, .117 and .123 standard deviation of PTSD respectively.
Discussion
The current study examined the prevalence of mental distress and PTSD among IDPs in the Ethiopian Amhara region, with particular emphasis on the Wag Hemera zone. The findings demonstrated that participants experienced a significant level of mental distress (63%) and PTSD (48%) because of the conflict and forced displacement. Compared to findings from the neighboring Sudan Darfur IDPs, where mental distress was 72% and PTSD 54% (Musa & Hamid, 2010), the findings from the current study seem lower. The difference could be attributed to the timing of data collection, specifically to the fact that the data from Darfur was collected during an active war scenario, and our data was collected after participants arrived in a safer area in an IDP camp. However, the prevalence of mental distress and PTSD is significantly higher than IDPs in non-African settings, for example, among IDPS in Ukraine with 27% PTSD (Shevlin et al., 2018) and Syria with 35% PTSD (Hendrickx et al., 2020). One of the potential reasons for such a difference can be the availability of mental health services, which is almost non-existent in the Ethiopian context compared to the 26% of IDPs who have accessed mental healthcare in Ukraine (Chikovani et al., 2015). However, our findings are comparable to a PTSD prevalence that ranged from 42% to 54%, as reported in a review study of IDPs in Africa (Owoaje et al., 2016).
The findings revealed that demographic and contextual variables contribute to variations in mental distress and PTSD among IDPs. For example, there is a significant gender disparity in mental distress, where female IDPs scored higher than male participants. The findings substantiate previous studies that compared to men; women experience a unique set of risks during wartime, which increases their mental distress (Farhood et al., 2018; Salah et al., 2013). Female IDPs are likely to have higher anxiety and sensitivity and could severely interpret traumatic events, and as a result, they may develop PTSD (Hantsoo & Epperson, 2017). As the findings indicated, within female IDPs, PTSD is higher among those who experienced and witnessed sexual abuse and rape. When it comes to residence, there was no significant difference, unlike reports from Sudan that indicated higher PTSD among IDPs from urban areas (Salah et al., 2013). Contrary to studies from Sudan (Sanhori et al., 2020) and Nigeria (Idemudia et al., 2020) that reported severe PTSD among IDPs who stayed for longer times in IDP camps, findings from the current study showed those who resettled recently demonstrated higher PTSD. This could be because those who recently joined the camps might have fresh memories of traumatic experiences that elevated their PTSD scores, but this needed further investigation.
The findings showed significant differences in the score of mental distress across participants’ educational level, family size, age, marital status and traumatic exposure. Sexually abused women scored a higher degree of PTSD symptoms, followed by those who experienced multiple traumas, family murder, physical abuse, witness trauma and property damage, and the results were statistically significant. Similarly, a previous study by Madoro (2021) suggested that those who witnessed family murder and property damage were more vulnerable to PTSD. The findings demonstrated that PTSD and mental distress issues can be exacerbated due to a lack of professional mental health assistance and adverse conditions in IDP camps. The findings also support a previous study that reported married IDPs experience higher mental distress than unmarried IDPs (Musa & Hamid, 2010).
Additionally, marital and household responsibilities coupled with the loss of their partners and children during conflict intensify distress among married IDPs. With regard to age, adolescents showed the highest PTSD and mental distress scores. The findings are consistent with a study from Nigeria that reported adolescent IDPs to have higher mental distress. However, our findings on PTSD contradict the results of the same study that reported lower scores of PTSD among adolescent IDPs (Sheikh et al., 2016). The study from Nigeria indicated that the adolescents lived with their parents, which could potentially help in reducing PTSD and caused the contradiction. Those with lower education reported higher levels of mental distress and PTSD, consistent with findings from a previous study (Chukwuorji et al., 2017). However, the findings also suggested that the differences in mental distress and PTSD become lower as IDP’s educational level increases, as also reported in a previous study (Lawrence, 2021).
In support of previous studies, psychological capital was found to be a significant negative predictor of both PTSD and mental distress (Bhat, 2017; Idemudia et al., 2020; Krasikova et al., 2015). Although all the components of psychological capital (self-efficacy, hope, optimism, and resilience) had a significant effect, self-efficacy was the strongest predictor for both mental distress and PTSD, as reported in other studies as well (Chung et al., 2017; Morina et al., 2018). Increasing the rest of the components, particularly hope, among IDPs can significantly decrease PTSD and mental distress, as demonstrated in the findings as well as extant literature (Umer & Elliot, 2021; Yıldırım et al., 2022).
Implications
The comparatively higher rates of mental distress and PTSD among IDPs in northern Ethiopia and other parts of Africa, in general, speak to the global disparities in the psychological impacts of conflicts and the mental health services provided to IDPs across different regions. This study will contribute to addressing the knowledge gap on psychological distress and PTSD experienced by IDPs in less-researched parts of the world, such as Ethiopia. The findings call for improved efforts from international agencies, such as the United Nations High Commission for Refugees, the International Organization for Migrants, the World Food Program, and the International Rescue Committee to expand mental health services in underserved areas like northern Ethiopia. Locally, recruitment, training, and deployment of mental health workers who can provide culturally and contextually relevant services is essential.
The study underlined that mental health efforts should target enhancing psychological capital as the critical element in mitigating the psychological impacts of war and displacement. Training on improving self-efficacy, utilizing the solid spiritual and religious base of the IDP community to raise hope and optimism, and leveraging the communal culture to foster resilience could help reduce mental distress and the effects of PTSD among IDPs in the study area. Particular attention should be given to improving self-efficacy as the strongest determinant by empowering and enhancing the problem-solving skills of IDPs that help them be resilient and bounce back from the distress inflicted by the displacement. The findings also demonstrated the need for special attention to specific groups, including those who are females, adolescents, widows, less educated, and experienced sexual abuse and trauma, as they scored higher scores on mental distress and PTSD. These groups are the most vulnerable, and their mental distress and PTSD experiences are exacerbated by multiple compounding socioeconomic, cultural, and social factors, which require the application of an integrated approach to providing mental health services.
Despite its important contribution in bringing attention to the mental health challenges of one of the most understudied IDP groups and sites, this study has its limitations. As a cross-sectional study, the study captured the realities of IDPs at one point in time and could not demonstrate the long-term impacts of the displacement. Future research needs to pay attention to the timing of data collection when studying mental distress and PTSD among IDPs. It is essential to recognize the potential variations between those who are recently displaced IDPs and those who have stayed for a while in IDP camps. As the current study focused on camp-based IDPs, it is also important for future studies to examine IDPs in the community or non-camp settings.
Conclusion
The study uncovered the high prevalence of mental distress and PTSD among IDPs in Ethiopia’s Amhara region, particularly in the Wag Hemera zone, revealing critical insights into the psychological impact of conflict and displacement. The findings revealed that socio-demographic aspects, such as marital status, age, and education, are influential, with widowed and divorced, less educated, and adolescent IDPs being particularly vulnerable. The levels of mental distress and PTSD are influenced by factors like gender, with women, especially those exposed to sexual abuse, showing higher rates. The study underscored the importance of psychological capital, especially self-efficacy, in mitigating distress and PTSD. These findings advocate for enhanced mental health services in underserved areas like northern Ethiopia and targeted interventions focusing on the most vulnerable groups. The research also points to future areas of focus, including the timing of data collection and the exploration of mental health among non-camp IDPs, highlighting the need for comprehensive strategies to address the mental health needs of IDPs.
Footnotes
Acknowledgements
The authors would like to thank the IDPs who participated in the study.
Authors’ contributions
GEM was involved in designing the study, collecting data, analyzing, and drafting the methods and analysis sections of the article. GMT drafted the background and discussion and reviewed and edited the article. MB was involved in designing the study, supervising data collection and data analysis. MY reviewed, revised and edited the article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study was reviewed and approved by the Research Review Committee of the University of Gondar. Participants gave consent to participate.
Consent for publication
Not applicable.
Data availability statement
Data available on request due to privacy/ethical restrictions.