
Abstract
Background:
Intergenerational conflict (IGC), characterised by tensions between younger and older generations due to differing values, beliefs, and expectations, is a growing concern that could increase the risk of suicidal ideation/behaviour among youth.
Aim:
The aim of the study was to develop a conceptual framework (CF) to explore the relationship between IGC and suicidal behaviour among youth aged 18 to 24 years in Chennai, South India.
Methods:
Using a mixed methods design, 501 consenting youth from higher educational institutions (HEIs) in Chennai were administered the Intergenerational Conflict Inventory (ICI) and Columbia Suicide Severity Rating Scale (C-SSRS) to assess IGC and suicidal ideation. In-depth interviews (IDIs) were done with 25 youth reporting IGC, recruited from HEIs, workspaces, and urban slums in Chennai.
Results:
Quantitative analysis revealed significant associations between higher IGC scores and suicidal ideation/behaviour (p = .001). Most common areas of conflict were social media use, career expectations and marriage. Three themes identified from the qualitative analysis that explained the CF were, family environment and IGC, suicidal ideation/behaviours and IGC, and coping with IGC. Poor communications, pressures to conform with family role expectations including marriage and restrictions on friendships were major areas of conflict linked to many youths feeling sad, lonely and suicidal thoughts. No resolution of conflicts left youth feeling alone and poorly understood.
Conclusion:
Findings confirm that IGC is a significant contributor to suicidal ideation/behaviour among youth in South India. The CF provides insights into family dynamics and calls for targeted interventions, including family-based strategies and mental health support in the Indian and possibly in other southeast Asian countries contexts.
Introduction
Intergenerational conflicts (IGC) refers to the collective tension and antagonism between older and younger generations often triggered by social changes (Silverstein, 2007). They can include behaviours varying from verbal arguments about differences in opinions to aggression and hostility. Within the familial context, parent-child conflicts arise mainly due to generational differences in values, beliefs, attitudes and expectations. Further, these ideals may be influenced by cultural, social and economic factors (Weymouth et al., 2016). While more autonomy, independence and personal identity are possible reasons of conflict, some attribute IGC to cultural differences, particularly with regard to parenting styles (Lim et al., 2008; Pham et al., 2020).
In India, suicidal ideation and behaviour among youth represents a significant public health concern with profound social, economic and psychological implications (Radhakrishnan & Andrade, 2012). Further, suicide ranks as the fourth most common cause of death in the late adolescent age groups (15–19 years old). The National Crime Records Bureau (NCRB) reported that 10,255 adolescents (those under the age of 18) and 59,823 young adults (18–30 years of age) died as a result of suicide in 2022 (National Crime Records Bureau, 2022). Indian men aged 15 to 29 are reported to have suicide rates twice as high as the global average (25.5 vs. 13.1 per 100,000), and young Indian women have rates almost six times higher (24.9 vs 4.1 per 100,000; Vijayakumar et al., 2022). Notably, South India, particularly states like Tamil Nadu, have historically reported higher suicide rates compared to the national average (Vijaykumar, 2007).
Factors such as academic pressure, family conflicts, relationship issues, socioeconomic disparities and cultural stigma surrounding mental health contribute to the vulnerability of young individuals to suicidal ideation and behaviour. Additionally, rapid socio-cultural changes and the increasing prevalence of technology-mediated social interactions introduce unique stressors and challenges for young people in India (Senapati et al., 2024). These shifts are particularly evident in changing gender roles, where young women increasingly aspire for independence and career opportunities, challenging familial expectations centered on early marriage and household responsibilities. Similarly, globalisation has broadened access to education and urban employment, fostering aspirations that may conflict with traditional cultural priorities (Bakhtiari & Shajar, 2006). These dynamics exacerbate intergenerational tensions, as elders struggle to reconcile their expectations with the evolving aspirations and values of younger generations.
Risk of increased suicidal intention and behaviour are also associated with higher perceived IGC. Suicidal tendencies among young people have been demonstrated to be exacerbated by unresolved intergenerational disputes, particularly when there is a lack of communication, respect and understanding (Orlins et al., 2021). Studies have explored this phenomenon using various terms such as parent-adolescent conflict, parent-child conflict, familial conflicts, intergenerational cultural dissonance and intergenerational acculturative conflict (Madhavan et al., 2024; Meza et al., 2024). In the Indian setting, studies examining patterns in intergenerational relations categorise them into three possibilities, that is, solidarity, ambivalence and conflict (Verma & Satyanarayana, 2012). We recently conducted a scoping review which highlighted the significant positive associations between intergenerational/parent–child conflict and suicidal ideation/behaviour among young people (Akshaya et al., 2024). This preliminary evidence provided the impetus to develop a conceptual framework (CF) for IGC and suicidal behaviour that would provide a comprehensive and holistic understanding of this phenomenon among young people and could guide intervention development for youth in south India.
Methods
Study design and setting
We used a convergent parallel design where the quantitative and qualitative data were collected concurrently. The study was conducted in Chennai, a metropolitan city, in the state of Tamil Nadu, India which has a high suicide rate of 22.2 per 100,000 population (Vijaykumar, 2007).
Study participants
Quantitative: Undergraduate and post graduate students, aged between 18 and 24 years, who could read Tamil and were studying in higher educational institutions (HEI) in Chennai were eligible for inclusion. Study participants were approached through the use of flyers, posters and information sessions delivered by the research team in five HEIs located in and around Chennai which included both arts and science-based institutions. The selected institutions were either co-educational or those that admitted only men or women. Consenting participants were invited to fill in the assessment questionnaires which was carried out in their classrooms.
Qualitative: Young people aged between 18 and 24 years living in Chennai, were recruited from diverse settings like HEIs, workspaces and urban slums. The assistance of community-based organisations were used to recruit participants from community and work space settings while participants from HEIs were selected from among those colleges where the survey was conducted. Using criterion sampling, consenting participants who reported experiencing IGC in their families, with or without suicidal ideation/behaviour- elicited through a brief interview -were included. The IDIs were conducted at the locations from where the respondents were recruited.
Assessments
Quantitative
Demographic profile of the participants: A semi-structured questionnaire was developed to collect demographic characteristics of study participants such as age, gender, education, family type, relationship status, residence, presence of any physical disability and history of psychiatric illness if any.
Intergenerational conflict: We measured IGC using the Intergenerational Conflict Inventory (ICI; Chung, 2001), a 24-item questionnaire with 3 sub-scales namely, Family Expectations, Education and Career and Dating and Marriage. The questionnaire underwent a process of translation into Tamil (the language of communication in Chennai city) and back-translation into English to check for comparability. As part of its cultural adaptation, we carried out cognitive interviews with 15 youth aged between 18 and 24 years (7 men, 8 women), which enabled evaluation of the adequacy of the translations, its relevance and the comprehensiveness of the items to our population. This process yielded an additional 12 items that addressed issues ranging from social media usage, dressing styles, spending time with friends to religious practices as being sources of conflict in families. The final instrument comprising 36 items was subject to validity and reliability assessments.
Aspects of IGC were assessed by calculating the percentage of respondents who reported experiencing conflict in each specific area covered by the items in the ICI. To calculate the mean ICI score, responses to each of the 36 items on the modified ICI were assigned numerical values based on a Likert scale. The sum of these values for each participant was then calculated. The mean ICI score represents the average of these total scores across all participants in the study. This provides an overall measure of the level of IGC experienced by the sample population.
Five mental health experts who reviewed the modified ICI found the items both relevant and applicable to measuring the construct of IGC. The modified ICI exhibited strong reliability with a Cronbach’s α of .9404. The determinants of the correlation matrix were <.001, and Bartlett’s test yielded a Chi-square value of 8809.567 (p < .001), confirming good intercorrelations between the items.
Suicidal ideation and behaviour: Suicidal ideation/behaviour was measured using the Columbia Suicide Severity Rating Scale (C-SSRS; Posner et al., 2008). This 14-item questionnaire measures suicidal ideation/behaviour, intensity and frequency of suicidal thoughts, plans, preparatory behaviours and attempts. The Tamil version of the C-SSRS scale that was used in the study exhibited good psychometric properties. It demonstrated high internal consistency (Cronbach’s α) of .8690. Bartlett’s test of sphericity yielded a Chi-square value of 791.257 (p < .001), confirming significant intercorrelation between the items.
Qualitative
An IDI guide was developed which explored the perceptions of young people regarding their family environment, the nature of their relationship with parents/grandparents, reasons for conflicts with elders in the family, in what ways these conflicts affected them including whether it contributed to suicidal ideation, and how young people coped with such conflicts. All IDIs were audio-recorded, translated into English where necessary and transcribed verbatim. Quality checks were performed to ensure accuracy and consistency.
Data analysis
Quantitative: We performed data analysis using STATA 16.0. Categorical variables were summarised as frequencies and percentages, while continuous variables were presented as means with standard deviations. Statistical significance was defined as a p-value less than .05. Independent t-test was used to compare differences between groups.
Qualitative: Data were analysed using NVIVO, guided by Clarke and Braun’s (2013) thematic analytical approach. Two coders (SK and RM) inductively coded five transcripts, the codes so derived were merged, reviewed and a codebook was developed. This codebook was used while coding the remaining transcripts, with new codes added as needed. Codes were then organised into categories, from which themes were derived that best explained the findings. Relevant quotes were selected and placed under appropriate themes.
Participatory approach and co design
We employed a participatory approach; wherein young people were involved in the design and development of the CF. Workshops were conducted through which they were encouraged to contribute their ideas and perspectives and provide feedback. This collaborative process allowed us to integrate the participants’ lived experiences and preferences thereby helping to ground the CF, enhancing its relevance and applicability to this population.
Ethical considerations
Prior scientific and ethics committee approval was obtained from the SCARF Scientific Advisory Committee (SCARF-SAC) and subsequently from the SCARF Institutional Ethics Committee (SCARF-IEC) with the approval number SRF-SR/11/Aug-2022. Recruitment of participants was purely voluntary and written informed consent was obtained from each participant both for the quantitative survey and the qualitative IDIs. Participants with suicidal ideation/behaviour and/or distress were provided immediate psychological support and treatment by mental health professionals.
Results
Quantitative
Demographic characteristics
Supplemental Table 1 presents the characteristics of the HEIs from where participants were recruited for the survey. Supplemental Table 2 describes the demographic characteristics of survey participants. There were 501 participants aged 18 to 24 years, with 51% (N = 256) males and 48% (N = 243) females. Nearly 81% (N = 404) were undergraduates while the remaining were postgraduates.
Qualitative
Demographic characteristics
We conducted a total of 25 IDIs (10 men, 15 women) with young people of which 12 were recruited from HEIs (men = 5; women = 7), 8 were from work spaces (men = 3; women = 5), and 5 were from urban slums (men = 2; women = 3). Their mean age was 22.4 ± 1.8.
Themes of analysis
The phenomenon of IGC and suicidal ideation/behaviour, identified from our data, can be conceptualised in terms of three main themes, namely, (1) Family environment and IGC, (2) IGC and suicidal ideation/behaviours and (3) Coping with IGC. Findings from the quantitative survey and the qualitative IDIs are presented for the first two themes while only qualitative findings are described for the last theme.
Family environment and IGC
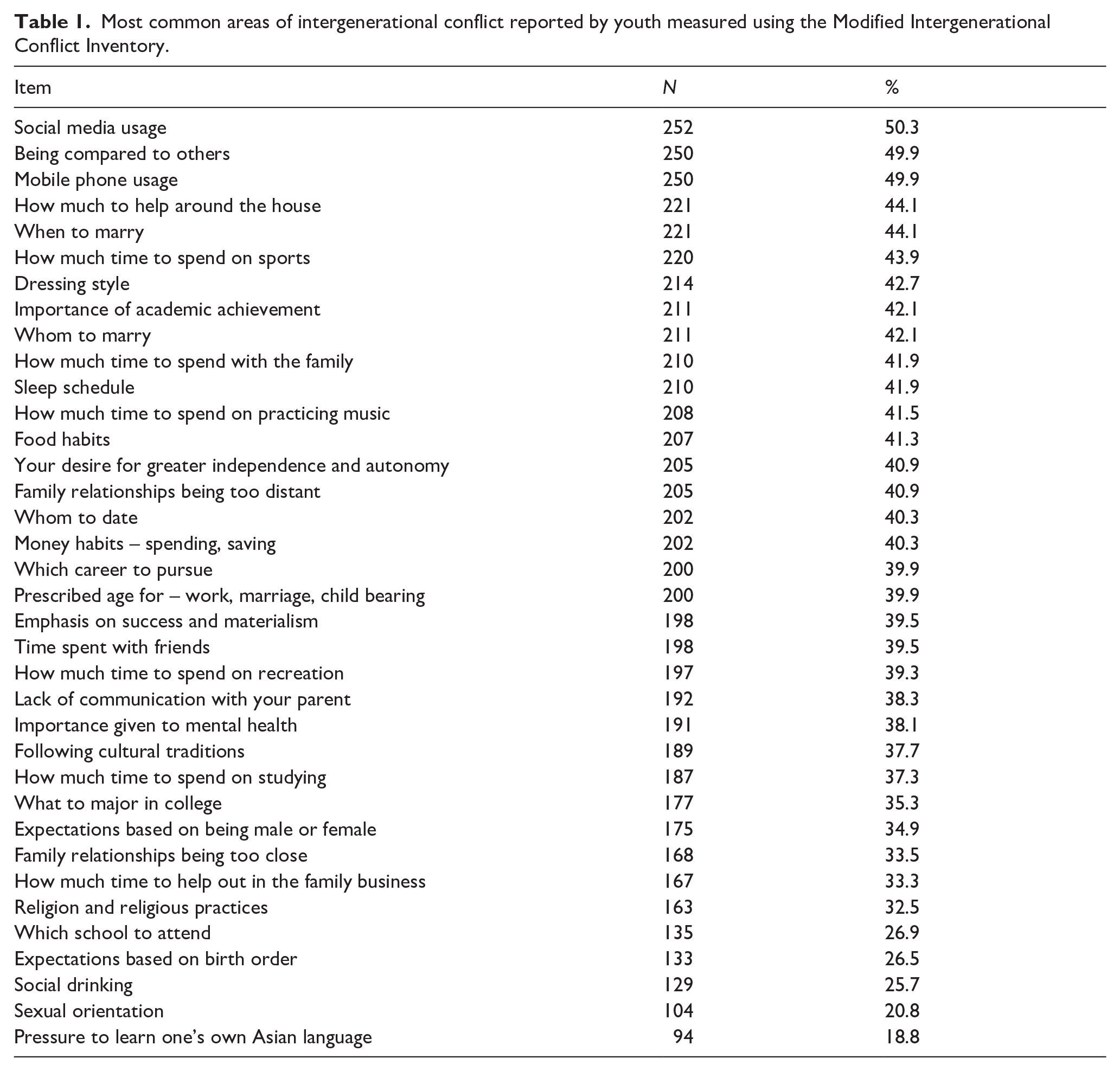
The family environment proved to be a major source of stress in many cases. Whether it was because of constant criticisms from parents and grand-parents (to study better, earn better, behave and dress appropriately) or feeling constrained to express themselves freely or to be understood; of differences of opinions; of perceptions of poor familial support, to incompatibility between parents contributing to frequent arguments and fights, the atmosphere at home, as reported by several participants was unpleasant, even ‘toxic’. We present first the quantitative results from the ICI showing areas of conflict as reported by the youth (Table 1) followed by the findings from the IDIs.
Most common areas of intergenerational conflict reported by youth measured using the Modified Intergenerational Conflict Inventory.
Quantitative
The most frequently reported areas of IGC were with regard to social media usage (252, 5.3%), being compared to others and mobile phone use (250, 49.9%), undertaking household work and when to get married (221, 44.1%). Additionally, issues like dressing style (214, 42.7%) importance of academic achievement (211, 42.1%) and time spent with family (210, 41.9) were also major sources of conflict (Table 1).
Qualitative
We describe the theme on family environment and IGC in terms of three sub-themes, namely, family dynamics/relationships, role expectations, friendships and marriage.
Family dynamics/relationships
Constant criticisms often left participants doubting and questioning their own abilities. One participant, who, following her parent’s divorce, had to move in with her maternal grandparents, spoke of having to listen to her grandmother’s taunts and criticisms almost on a daily basis, eroding her self-esteem and triggering thoughts of wanting to end her life. Another, described feeling disturbed by the loud arguments between her parents at home which was also affecting her studies. When she pointed this out to them, they told her not to find refuge in such excuses. The result was that the participant stopped communicating with her parents widening the chasm between them. In another case, a 24-year-old participant, felt that she had no voice in her family. Their failure to recognise her individuality was distressing to her and resulted in arguments and quarrels. Others spoke of not getting the support they needed from their parents as in one case where a participant described being physically and verbally abused by his father when he was a child while his mother played a passive role neither protecting him nor consoling him. A male participant spoke of having no communication with his father, whose addiction to alcohol resulted in fights and arguments at home disrupting the atmosphere. The absence of a supportive home environment which was sometimes even hostile, contributed to some participants feeling ‘empty’ even afraid ‘to take life forward’ (ID 003, female, 24 years).
Role expectations
Stereotypical role expectations with girls having to cook, manage household chores and get married and boys having to take on family responsibilities, obtain respectable jobs and eventually get married were other areas of stress for the youth. One male participant spoke of the pressure put on him by his family to get a job and start providing for the family owing to their straitened economic conditions. A female participant, in turn described the pressure put on her by her mother to conform and be ‘like a girl’ a phrase that annoyed and angered her leading to frequent arguments. Many female participants additionally, spoke of having to abide by a dress code prescribed by the family which was frustrating and annoying to them. Such curbs and restrictions imposed on young people exacerbated tensions within families often resulting in angry outbursts by both parties, disrupting relationships. In some cases, participants spoke of towing the line in the interest of avoiding such confrontations, often at great cost to their own sense of self.
Friendships and marriage
Having friends of the opposite gender was frowned upon, more so for girls. Some female participants whose parents were very strict spoke of not being allowed to even go out with their female friends and of having to return home at specified times. Failure to comply resulted in major fights and arguments. Boys too, reported facing some restrictions but perhaps not to the extent that girls did. A few spoke of being denied pocket money or were provided very low allowances affecting their ability to spend when they went out with their friends. This served to effectively discourage them from going out. Engaging in long conversations over the phone was also discouraged by many parents and was a frequent cause of conflict between parents and their wards, often resulting in participants using it surreptitiously. Participants attributed this behavior of their parents to a basic distrust of their friends combined with the fear that these friends would have a negative influence on them and would misguide them. Similar issues arose with the use of social media with participants reporting that their parents saw its use as a waste of time and one that ate into their focus on studies – concerns, which the youth disagreed with.
The issue of marriage was another major source of conflict and stress as reported by many participants. Many female participants spoke of being explicitly told by their parents not to date or have boyfriends and that their parents- having their best interests at heart- would find a suitable boy and arrange their marriages for them. Participants spoke of wanting to make their own choices, of being allowed to date and get to know the person before entering into marriage – practices that were not acceptable to most parents. Even male participants were dissuaded from meeting with girls or even having them as their friends and spoke of their parents urging them to get married once they were in stable jobs and were around 27 to 28 years of age. In this context, one female participant indicated that her parents were not averse to her dating, provided this would lead to marriage with that individual, a guarantee she was unable to give.
Thus, the family environment was not always perceived as a nurturing and caring space in which young people could feel safe and secure and grow to their full potential. For many youths, it turned out to be a source of great stress leaving them feeling stifled, unhappy and depressed.
IGC and suicidal ideation/behaviour
Quantitative
Table 2 depicts the association between IGC and suicidal ideation/behaviour among the participants. Participants with suicidal ideation had significantly higher ICI scores (Mean = 99.1, SD = 24.1) compared to those without suicidal ideation (Mean = 74.1, SD = 25.3), with a p-value of .001. Similarly, participants with suicidal behaviour had higher ICI scores (Mean = 98.5, SD = 24.6) compared to those without suicidal behaviour (Mean = 76.5, SD = 26.3), with a p-value of .001. These results suggest that higher ICI scores were strongly associated with both suicidal ideation and behaviour.
Association between intergenerational conflict (measured by Modified Intergenerational Conflict Inventory) and suicidal ideation and behaviour measured by Columbia Suicide Severity Rating Scale).
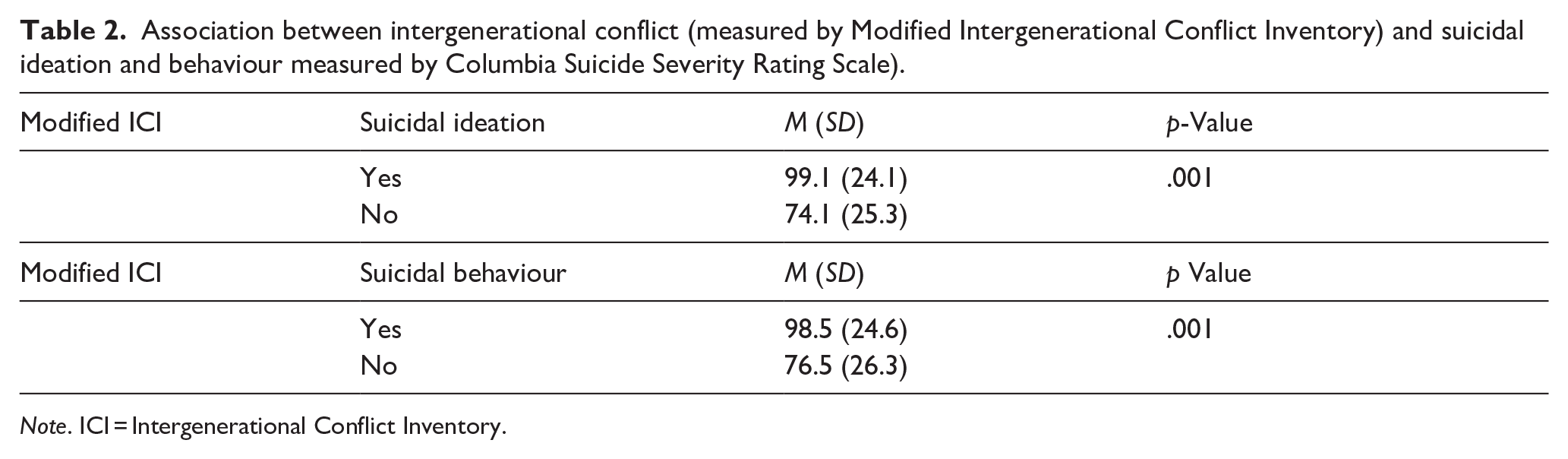
Note. ICI = Intergenerational Conflict Inventory.
Qualitative
Our qualitative analysis also revealed that persistent conflicts with parents such as those described earlier, contributed to several participants reporting feelings of sadness and depression, of low self-esteem, of feelings of loneliness and of harbouring suicidal thoughts. Some had even attempted suicide in a desperate attempt to escape and free themselves of their emotional burden. One young girl spoke of wishing she had not been born at all while another, a young man, described driving his motor bike at high speed, possibly at great risk to his life. A few participants said that they had been experiencing suicidal thoughts for several years but had either not acted on them or else the fear of pain and the sight of blood acted as deterrents. The presence of these negative feelings and thoughts severely compromised their sense of self, leaving them feeling unsupported and unloved. In other narratives, participants described the critical role played by parents in nurturing their children and their failure to understand and support them often drove young people to self-harm or suicide.
Coping with IGC
This theme has been divided into two sub-themes: (i) ways of coping with conflicts and (ii) conflict resolution.
Ways of coping with conflicts
In terms of how young people t coped with conflicts faced by them in their families, a number of different ways were reported which included sharing problems with friends, seeking help from a mental health professional, introspecting as a way of understanding oneself better and working towards self-improvement by adopting a disciplined lifestyle. Talking to friends or someone with whom they were close, was a strategy reported by many study participants. Those who reported seeking care from a mental health professional found this helpful but, in some cases, felt forced into being secretive about doing it as their parents believed it to be indicative of a mental illness and therefore not seen as an acceptable strategy. Smoking and eating more than usual were other strategies described by a few. In one instance, a participant strongly believed that attempting suicide or even thinking about it was not the way to go about dealing with conflicts. It only resulted in causing pain to one’s family. Most participants stated that the best way to handle family conflicts was through open communication and understanding which they believed was central to better family relationships.
Conflict resolution
These family conflicts as described by the participants had been happening for a considerable length of time, but their resolution rarely ever happened. Usually, following the outburst or the heated arguments, participants reported a stand-off like situation with neither party talking to each other, even avoiding each other. This would continue for a few days after which a semblance of outward normality would return but the simmering discontent remained. Attempts at referring or bringing up the issue of conflict was seen to only accentuate and worsen matters. In some cases, participants said that they made adjustments or acquiesced to their parent’s wishes to keep the peace in the home and to avoid further altercations. Another, explained that the only way out was to reduce one’s expectations from family, avoid thinking about the events that had happened and move on. But, for the most part, these conflicts were rarely ever discussed and were just set aside only to surface again on another occasion.
Quotes supporting each theme/sub-theme are presented in Supplemental Table 3.
The conceptual framework, derived from our findings, shown in Figure 1, displays the relationship between IGC and suicidal ideation/behaviour among youth.
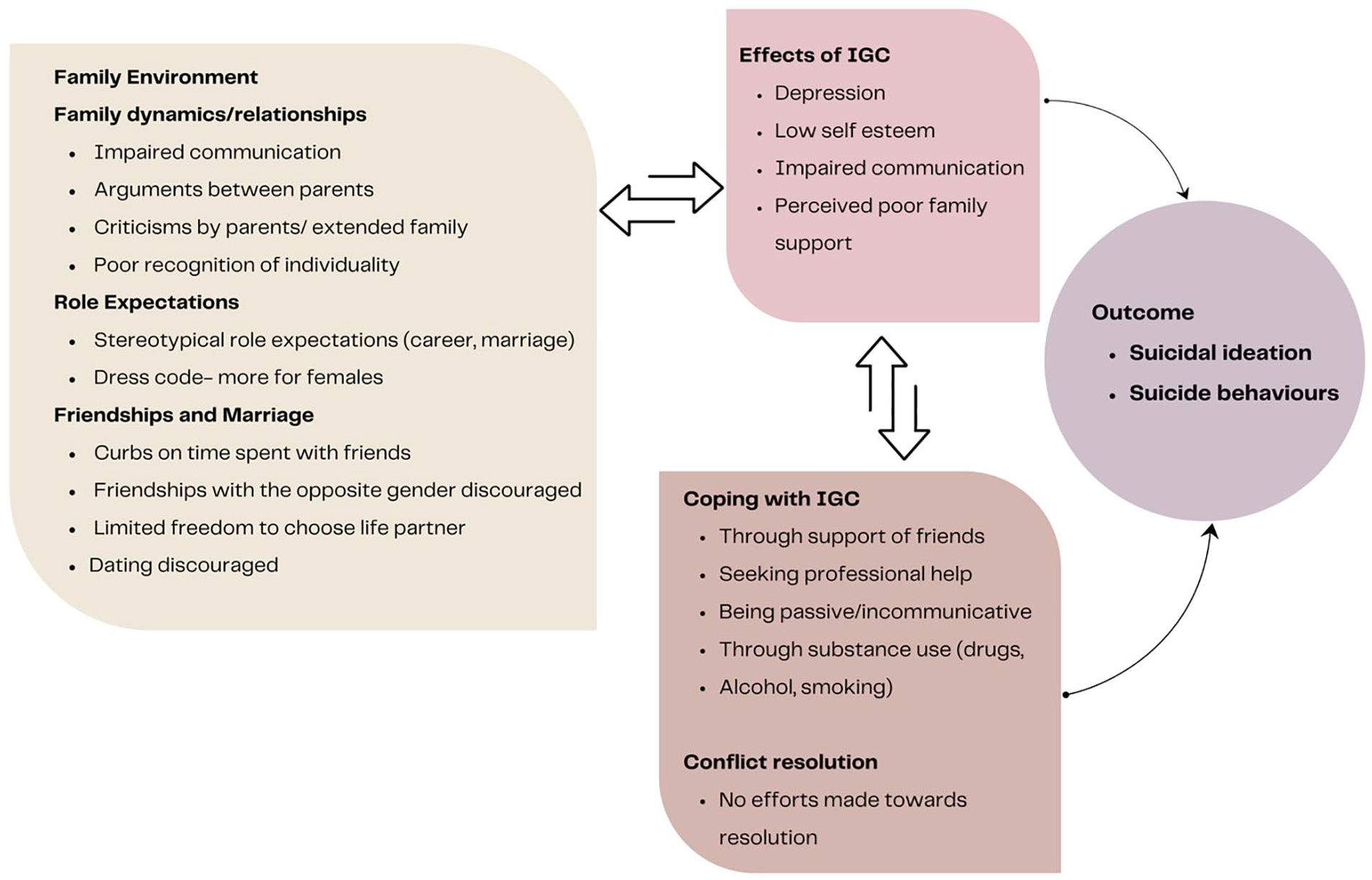
Conceptual framework of intergenerational conflict and suicidal ideation/behaviour among youth.
Discussion
The key findings from our study contextualised in an urban setting in south India that highlight the core components of a CF to explain the phenomenon of IGC can be summarised as; poor family dynamics affecting relationships and creating an atmosphere with little to no scope for open communication, thereby contributing to depression, suicidal thoughts/attempts; restrictions and curbs imposed on various spheres leading to resentment and widening of the generational divide and with no conflict resolution happening, coping with IGC not always helpful. Through the development of the CF, we have sought to provide an understanding of the complex interplay between IGC and suicidal behaviour among the youth in Chennai.
Studies have highlighted the bidirectional nature of communication patterns, whereby conflicts exacerbate poor communication, leading to misunderstandings and strained relationships (AM et al., 2022), features evident in the narratives of our study participants also. Several participants in our study described being poorly understood by their parents, of a failure by parents/elders to recognise their individuality and of restrictions and curbs imposed on them that only exacerbated conflicts when resisted. These restrictions extended to various aspects of their lives including the friends they had and the time spent with them, the kind of clothes they wore- more so for girls- and more important, on decisions regarding marriage and career. The tensions accruing from such arguments and dissensions, where participants felt that their ideas and thoughts were neither recognised nor valued left many feeling sad and some suicidal (Sayed & Sinha, 2024). The psychological repercussions of IGC on our study participants included heightened levels of depression, anxiety and low self-esteem that compromised their sense of well-being. Such psychological factors serve as proximal risk factors for suicidal behaviour, underscoring the need for early identification and intervention strategies targeting mental health issues arising from familial conflicts (Lin & Guo, 2024). It also underscores the importance of addressing familial dynamics as a potential precursor to understanding suicidal behaviour among young people.
Our study also identified coping mechanisms, social support and access to mental health services, which could modulate the impact of familial conflicts on suicidal ideation and attempts. This nuanced understanding underscores the multifaceted nature of suicidal behaviour, necessitating a holistic approach (Gupta et al., 2024; Yang et al., 2022). Important to note here is that in most cases participants in our study reported no resolution of conflicts which were simply set aside, only to re-surface on another occasion. This does not augur well either for the youth or for the parent and suggests the need for counselling services to help families more effectively resolve such issues.
From a developmental perspective, the framework recognses the unique challenges faced by young individuals navigating the transition from adolescence to adulthood. It acknowledges the role of IGC as normative developmental challenges, which, when exacerbated, can disrupt the developmental trajectory and increase vulnerability to suicidal behaviour (Goldston et al., 2016). This developmental lens underscores the importance of targeted interventions tailored to the specific needs of young individuals (Wood et al., 2018).
The quantitative finding that social media and mobile phone use are among the top sources of IGC highlights the unique challenges youth face in the digital age, aligning with global concerns about the negative impact of social media on mental health (Khalaf et al., 2023). Qualitative data further revealed parental anxieties over excessive phone use, online interactions, and exposure to unfamiliar values, often rooted in protective or traditional motives. Their concerns, though well-intentioned, tend to be perceived by the youth as being restrictive contributing to anger and annoyance, misunderstandings, and, in some cases, suicidal ideations among youth (Marsh et al., 2024).
Exposure to less traditional media and globalised perspectives has reshaped the roles and expectations of women which emerged as a significant source of IGC in our study. Qualitative findings highlighted tensions between young women’s aspirations for education, careers, and autonomy, and family expectations around early marriage and traditional gender roles (Raj et al., 2019). Social media further intensifies this divide by shaping youth perceptions of relationships and lifestyles (Wilska et al., 2023). These conflicts can undermine self-esteem, heighten isolation and contribute to suicidal ideation.
While our study focused on the impact of IGC on youth suicidal ideation and behaviour, it is important to acknowledge that IGC can also significantly affect the psychological well-being of parents. Research suggests that parents experiencing ongoing conflict with their children may report increased stress, anxiety and depressive symptoms (Hua, 2023). These conflicts can challenge parents’ sense of competence, identity, and authority, leading to feelings of helplessness and frustration. Furthermore, studies have found that parents’ own attitudes, values, and expectations can play a crucial role in shaping intergenerational dynamics and conflict (Chandrasekara et al., 2024).
While counselling addresses immediate mental health needs, a broader public health approach is essential to prevent and reduce the impact of IGC on youth suicidality. Community-based interventions that promote intergenerational dialogue, positive parenting, and mental health stigma reduction are key (Castillo et al., 2019). Schools and workplaces can support these efforts through programmes on communication, conflict resolution and mental health awareness. Given social media’s role in IGC and youth mental health, public health strategies should also promote responsible digital use through media literacy, parental guidance and collaboration with tech companies to regulate harmful content (Latha et al., 2020). Encouraging positive online communities can further protect youth well-being. A comprehensive public health strategy can foster a more supportive environment for young people, reducing IGC-related distress and enhancing mental health outcomes.
The study has several strengths. Firstly, the use of a mixed-methods approach allowed for both a broad understanding of the prevalence and influence of IGC on suicidal behaviour and a deeper exploration of the lived experiences of young people. Secondly, the CF that is grounded in our study findings, offers a comprehensive understanding of the multifaceted nature of IGC and its impact on young individuals’ mental health and suicidal behaviour. Lastly, is the cultural adaptation of the ICI to the Indian context thereby ensuring that the specific challenges faced by Indian youth are adequately captured.
Some limitations that warrant consideration are the absence of the perspectives of parents that could have helped provide a more holistic understanding of the phenomenon and the fact that the cross-sectional nature of study, limits making any causal inferences. Also, it is important to keep in mind that the CF may present a simplified version of the complexity of familial relationships and may not adequately capture the nuances of individual experiences within diverse cultural and socio-economic contexts. This perhaps, demands deeper exploration.
In conclusion, the CF can be seen to guide interventions aimed at mitigating the impact of IGC on suicidal behaviour among young people in the Indian context and possibly in other southeast Asian countries as both share many common familial and cultural values. It underscores the importance of family-based interventions focusing on enhancing communication skills, fostering familial cohesion and promoting positive coping strategies.
Supplemental Material
sj-docx-1-isp-10.1177_00207640251341063 – Supplemental material for Intergenerational conflict and suicidal behaviour among young people in south India: Development of a conceptual framework
Supplemental material, sj-docx-1-isp-10.1177_00207640251341063 for Intergenerational conflict and suicidal behaviour among young people in south India: Development of a conceptual framework by Lakshmi Vijayakumar, Vijaya Raghavan, Shuba Kumar, Rani Mohanraj, A Akshaya, NP Haritha, Harihara Murthy Subramanian, Jothilakshmi Durairaj, R Padmavati and M Suresh Kumar in International Journal of Social Psychiatry
Footnotes
Acknowledgements
Vijaya Raghavan was supported by the India Health Policy and Systems Research Fellowship (IHPSR) under Health Systems Transformation Platform (HSTP).
Contributors
LV, RP, MSK and VR conceived the study. VR, AA, NPH, SK, RM, SK and HMS collected the data. VR, SK and RM analysed the data. VR, LV, SK and RM wrote the report with contributions from all other authors. LV and VR accessed and verified the underlying data. All authors contributed to writing (review and editing), had access to the data, and were responsible for the final decision to submit for publication.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mariwala Health Initiative (MHI).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.