
Abstract
Background:
Complex post-traumatic stress disorder (C-PTSD) has been included in the International Classification of Diseases 11th Revision (ICD-11) to capture symptomatology caused by extreme, prolonged, or multiple forms of trauma.
Aims:
The present systematic review and meta-analysis sought to assess the one-month prevalence of this disorder in the community setting.
Method:
A systematic search was conducted in four databases (Google Scholar, PubMed, Web of Science, and Scopus) where relevant studies were subjected to explicit eligibility criteria, resulting in 16 included studies and 22 effect sizes. Study characteristics were tabulated, their methodological quality was assessed and findings were synthesized using a random-effects meta-analysis.
Results:
Findings indicated overall that C-PTSD has a moderate prevalence in this population (PREV = 8.59%, 95% CI [5.84%, 11.34%], I2 = 98.6%). Moderator analyses indicated that prevalence differed significantly by continent, scale, sample type, country, and language.
Conclusions:
The results of this study strongly indicate that 9 out of 100 people in the community are at risk for C-PTSD, making it a primary focus of attention and the public policies that it represents. Future research should further explore the prevalence of C-PTSD among specific population groups who experienced specific episodes of trauma.
Introduction
The Relevance of Knowing the Prevalence of Mental Disorders in the Community
Mental disorders currently represent a significant challenge to public health worldwide. The World Health Organization (WHO, 2022) estimates that a large proportion of the population will experience some form of mental disorder in their lifetime. Given this scenario, knowing the prevalence 1 of these disorders in the community setting is essential for the development of effective prevention, intervention and treatment strategies. One of the main benefits of knowing the prevalence of mental disorders in the community is the possibility of designing more effective public health policies. Through epidemiological studies, authorities can identify which disorders are more common in certain populations and adapt the available resources to meet those specific needs (Kessler et al., 2005). For example, if a high prevalence of depression is detected in adolescents, psychological support programs can be implemented in schools and youth centers.
Furthermore, collecting data on the prevalence of mental disorders contributes to reducing the stigma associated with these conditions. Viewing mental health as a common problem in society promotes greater understanding and acceptance by the community, fostering an environment in which affected people feel safer when seeking professional help (Corrigan & Watson, 2002). Another relevant aspect is that knowing the prevalence of mental disorders allows health professionals to better plan their services. By having up-to-date and accurate information, health systems can ensure a more equitable distribution of resources, such as training more mental health specialists and creating accessible care centers for the population at risk (Patel et al., 2018). Finally, analyzing the prevalence of mental disorders in the community setting helps to identify associated risk factors, such as socioeconomic status, access to education, and domestic violence. With this information, prevention strategies can be implemented aimed at reducing the incidence of these disorders and improving people’s quality of life (Lund et al., 2010).
C-PTSD as a New Diagnostic Entity in ICD-11
C-PTSD is an emerging diagnostic entity in the ICD-11 and includes additional symptoms to PTSD in people who experienced extreme, prolonged, or multiple forms of trauma (Reed et al., 2022). That is, to the three main symptoms of PTSD (avoidance, re-experiencing, and sense of threat), three other symptoms are added: affective numbing (or over-reactivity), persistent negative self-concept, and difficulty in interpersonal relationships (Maercker et al., 2022). Specifically, in the ICD-11 C-PTSD is defined as follows:
. . .is a disorder that may develop following exposure to an event or series of events of an extremely threatening or horrific nature, most commonly prolonged or repetitive events from which escape is difficult or impossible (e.g. torture, slavery, genocide campaigns, prolonged domestic violence, repeated childhood sexual or physical abuse). All diagnostic requirements for PTSD are met. In addition, Complex PTSD is characterized by severe and persistent 1) problems in affect regulation; 2) beliefs about oneself as diminished, defeated or worthless, accompanied by feelings of shame, guilt or failure related to the traumatic event; and 3) difficulties in sustaining relationships and in feeling close to others. These symptoms cause significant impairment in personal, family, social, educational, occupational or other important areas of functioning. (WHO, 2024a)
The main difference between PTSD and C-PTSD lies in the depth and breadth of the impact of the trauma (Hyland et al., 2017). While PTSD is generally associated with isolated events, C-PTSD is linked to prolonged experiences of victimization, leading to alterations in identity and sense of self. Furthermore, C-PTSD tends to be more resistant to treatment and is often accompanied by comorbidities such as depression, anxiety, and dissociative disorders (Fung et al., 2023; Karatzias et al., 2019; Reed et al., 2022). C-PTSD develops in individuals who have been exposed to repeated and inescapable traumas, such as severe and ongoing childhood abuse, recurrent intimate partner violence, human trafficking or exploitation, and prolonged imprisonment under abusive conditions. Furthermore, certain factors may increase vulnerability, such as lack of social support, history of childhood trauma, and genetic predisposition to mood disorders (Karatzias et al., 2019).
Treatment for C-PTSD is more complex than for standard PTSD due to the breadth of its symptoms (Brewin et al., 2017). Some key strategies include: (a) tailored cognitive-behavioral therapy (CBT), to address negative self-image and dysfunctional beliefs (Rajkumar, 2025); (b) cognitive processing therapy (CPT), effective in restructuring negative thoughts about the trauma (LoSavio et al., 2024); (c) mentalization-based therapy (MBT), to improve emotional regulation and interpersonal relationships (Smits et al., 2024); (d) EMDR (eye movement desensitization and reprocessing), focused on processing traumatic memories (De Jongh & Hafkemeijer, 2024); and (e) pharmacological intervention, with antidepressants or mood stabilizers in cases of severe symptoms (Bisson et al., 2020).
The Current Review
To determine the prevalence of a disease across diverse geographic and cultural settings, prevalence meta-analyses are conducted. Prevalence meta-analysis serves to obtain a more accurate estimate of disease frequency based on prevalence proportions (Barendregt et al., 2013). In prevalence meta-analyses, the summary estimate represents an average prevalence across the included studies (Borges Migliavaca et al., 2022). This estimate allows researchers to assess disease burden; that is, who in the population is experiencing a particular disease, at a very specific point in time (Borges Migliavaca et al., 2020). It is critical to examine this metric and confirm whether there are differences between the frequency of C-PTSD across cultures, so that researchers and clinicians can have a clear picture of the presence of this disorder in the population. This information creates an empirical foundation to support better management and planning for the burden of C-PTSD.
Certainly, some systematic reviews have examined in depth the prevalence of C-PTSD in: serving military personnel and veterans (Grinsill et al., 2024), survivors of human trafficking and modern slavery (Evans et al., 2022), refugees and asylum seekers (de Silva et al., 2021; Lechner-Meichsner et al., 2024; Mellor et al., 2021), and foster children (Czerwińska & Kucharska, 2024). There was also one narrative review that mentioned a possible general prevalence of C-PTSD (Maercker et al., 2022). However, no review has looked at the prevalence of C-PTSD in the community. This is important, as this new condition included in the ICD-11 will be of special attention at the community level and in the public health policies of WHO member states in the coming years.
Therefore, the aim of this systematic review was to determine the 1-month prevalence of C-PTSD in the community. We also aimed to determine whether this prevalence varies by continent, sample type, country, language, age and gender of participants, country vulnerability, and study quality.
Method
Eligibility Criteria
The protocol of this systematic review was registered in OSF (doi: https://osf.io/zjx2d/?view_only=96505b6204b446c9b74086ebc077abf4). The acronym PICOS (population, instrument, construct, outcome, and type of studies) suggested by COSMIN (Gagnier et al., 2021; Prinsen et al., 2018) was used to define the inclusion criteria. (P): Individuals from the community, (I): The International Trauma Questionnaire and others (see Sarr et al., 2024), (C) ICD-11 C-PTSD, (O): 1-month prevalence, (S): Cross-sectional and longitudinal studies.
We excluded studies with individuals from clinical, medical, psychiatric, or correctional settings. We also excluded studies with selective samples of trauma-exposed individuals (e.g., serving military personnel and veterans, survivors of human trafficking and modern slavery, refugees and asylum seekers, homeless people, prison staff, and foster children). We also excluded research with fewer than 100 participants. We also excluded studies that adopted a retrospective diagnostic approach based on previously recorded data from primary or secondary care records or national registries. Finally, we excluded those studies that presented prevalence data overlapping with larger studies (e.g., Ben-Ezra et al., 2018; Cloitre et al., 2019; Hyland et al., 2021).
Search Strategy
We conducted a systematic literature search, without language restrictions, using four databases: Google Scholar, PubMed, Web of Science, and Scopus (on January 30, 2025), employing the following keyword formula: (Prevalence OR epidemiology) AND ((Complex PTSD) OR (CPTSD) OR (C-PTSD)) AND ((community) OR (general population) OR (population) OR (student*) OR (healthy sample) OR (normal population) OR (representative sample)). For this meta-analytic review, we followed the guidelines of Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA; Page, McKenzie, et al., 2021; Page, Moher, et al., 2021). Supplementary Table S1 shows the PRISMA checklist for this systematic review.
Study Selection and Data Extraction
Figure 1 illustrates the study selection process. The search yielded 230,214 results (229,000 from Google Scholar, 600 from PubMed, 357 from Web of Science, and 257 from Scopus). There were no restrictions regarding study design, age, sex, sample type, country, and language because several of these variables were used as moderators in the analysis. Only studies that presented 1 month prevalence estimates in percentages or decimals were included; these were designated as effect sizes for subsequent analysis.
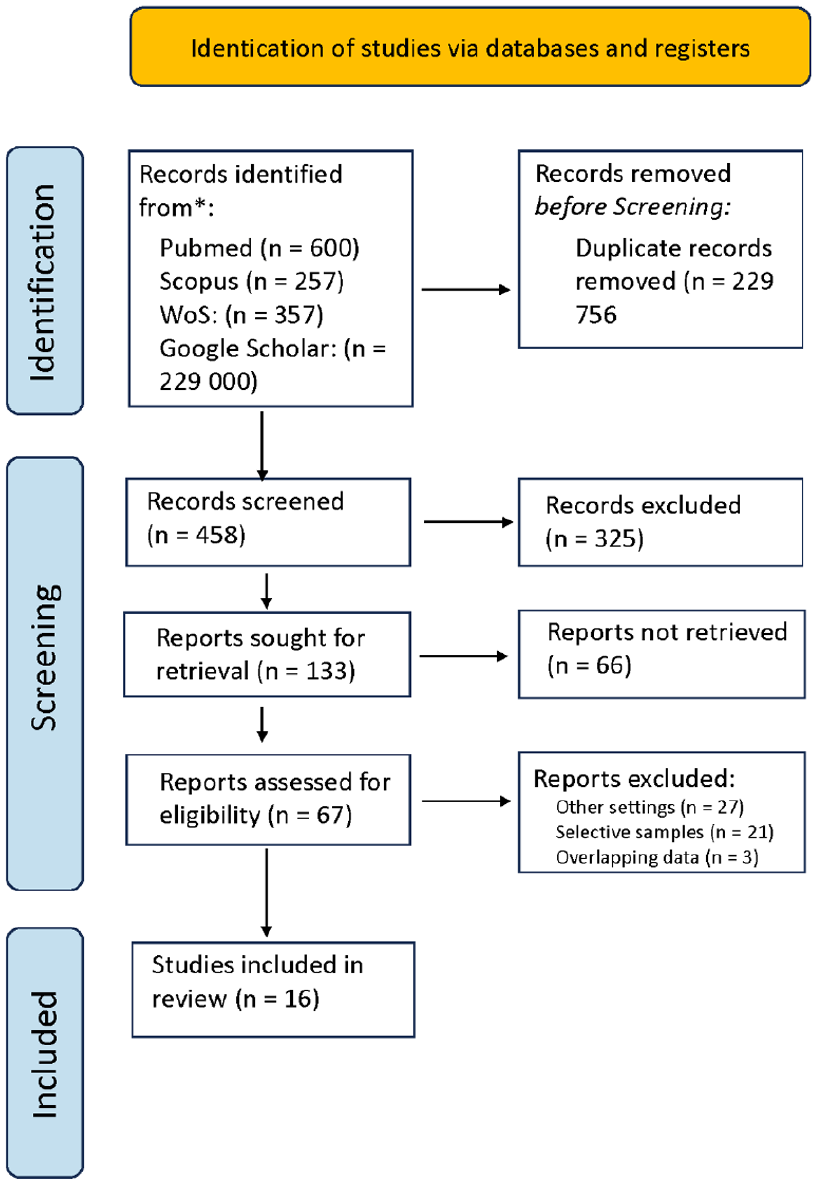
Study selection flowchart.
Citations obtained from the search in the above-mentioned databases were managed using Mendeley Desktop v. 1.19.8. Titles and abstracts were then filtered after removing duplicates. Once important citations were identified, the full text was searched. In case access to the study articles was restricted, the authors were contacted to obtain the full text through ResearchGate.
The data extracted were: (a) authors, (b) year of publication, (c) scale, (d) C-PTSD prevalence, (e) cases, (f) sample size, (g) sample type, (h) country, (i) vulnerability score (j) language, (k) percentage of women, (l) average age of participants, and (m) quality score. At both the study selection stage and the assessment of risk of bias of the included studies, TC-R and EV-A acted as blinded reviewers and any discrepancies were resolved by a third reviewer, LH-O.
Quality Assessment
Study quality was assessed using the JBI Critical Appraisal Checklist for studies reporting prevalence data (Munn et al., 2015). This tool covers nine questions: Q1 = Was the sample frame appropriate to address the target population? Q2 = Were study participants sampled in an appropriate way? Q3 = Was the sample size adequate? Q4 = Were the study subjects and the setting described in detail? Q5 = Was the data analysis conducted with sufficient coverage of the identified sample? Q6 = Were valid methods used for the identification of the condition? Q7 = Was the condition measured in a standard, reliable way for all participants? Q8 = Was there appropriate statistical analysis? and Q9 = Was the response rate adequate, and if not, was the low response rate managed appropriately? The following options are available for these questions: 1 = “Yes” and 0 = “No/Unclear.”
Procedure for Synthesis
For the synthesis of evidence, the “meta” package version 8.0-1 of the RStudio 2024.09.1 software was used. A meta-analysis (using a random effects model) was performed to determine the prevalence of C-PTSD (and how it varies) with heterogeneity analysis, average prevalence, sensitivity analysis (Egger regression test and funnel plot), and moderator analysis (subgroup analysis for categorical variables and meta-regression for continuous variables 2 ).
Results
Description of Included Studies
Supplementary Table S2 shows the characteristics of the 16 included studies that covered the C-PTSD prevalence literature over the past 10 years. The analyzed studies included samples from four continents (Africa, Asia, Europe, and North America) and 16 countries (11 Western countries: Denmark, Germany, Ghana, Ireland, Lithuania, Netherlands, Northern Ireland, Poland, Switzerland, United Kingdom, and United States; and five non-Western nations: China, Israel, Kenya, Nigeria, and Taiwan). The C-PTSD prevalence was reported in eight languages in these studies: Cantonese, Danish, Dutch, English, German, Hebrew, Lithuanian, and Mandarin Chinese.
The sample type distribution was as follows 3 : A total of 78.6% of the studies included community-dwelling adults (Ben-Ezra et al., 2020; Fung et al., 2022, 2024; Ho et al., 2024; Hoeboer et al., 2025; Jørgensen et al., 2024; Maercker et al., 2018; McGinty et al., 2021; Po et al., 2023; Robinson et al., 2025; Rzeszutek et al., 2024; Truskauskaite et al., 2023; Wolf et al., 2015), 21.4% community-dwelling adolescents (Chiu et al., 2023; Maercker et al., 2018; Redican et al., 2022), and 14.3% community-dwelling older adults (Maercker et al., 2018; Thoma et al., 2025).
To measure C-PTSD, 13 studies used the International Trauma Questionnaire (ITQ), one study used the International Trauma Questionnaire for children and adolescents (ITQ-CA, one study used the Child and Adolescent Trauma Screening (CATS), and one study used the National Stressful Events Survey (NSES). Only one study used a longitudinal design (Po et al., 2023). The vulnerability score of countries, according to the World Risk Report 2023, ranged from 0.99 to 27.1. The 16 studies recruited a total of 27,288 participants. Except for one study that only used female samples (Fung et al., 2024), 58.7% of participants were female, with a mean age of 40.2 years for adults and 14.5 years for adolescents. The 1-month prevalence of C-PTSD ranged from 0.50% to 19.60%.
Quality of Studies
After assessing the 16 studies using the JBI Critical Appraisal Checklist for studies reporting prevalence data (see Supplementary Table S3), most studies were considered to be of good quality (QS average = 8). For the first question, 100% of the studies were rated as “Yes.” For the second question, 43.75% of the studies met the requirement. For the third question, 100% of the studies were rated as “Yes.” For the fourth question, 100% of the studies met the requirement. For the fifth question, 100% of the studies were rated as “Yes.” For the sixth question, 93.75% of the studies met the requirement. For the seventh question, 100% of the studies were rated as “Yes.” For the eighth question, 100% of the studies met the requirement. Finally, for the ninth question, 62.5% of the studies were rated as “Yes.”
Synthesis of the Evidence
One study included four prevalence estimates, resulting in a total of 22 effect sizes (k) included in the meta-analysis. A significant degree of heterogeneity was found, with τ2 = 0.0042, 95% CI [0.0024, 0.0089], implying significant variance in the actual effects between these studies. The I2 coefficient also supported this claim (I2 = 98.6%, 95% CI [98.4%, 98.8%]), as did Cochrane’s Q (Q = 1530.18 (21), p < .0001). The estimate of the group effect size (prevalence) was moderate (PREV = 8.59%, 95% CI [5.84%, 11.34%]). Using Egger’s regression test, a significant level of publication bias was found (t = 8.52 (20), p < .0001), see funnel plot (Supplementary Figure S1). Prevalence varied by continent (Q = 57.51 (3), p < .0001) (see Figure 2), scale (Q = 74.31 (3), p < .0001), sample type (Q = 64.38 (3), p < .0001), country (Q = 734.58 (15), p < .0001), and language (Q = 301.41 (8), p < .0001). However, prevalence did not vary according to percentage of female gender (β = 0.0010, p = 0.3202), mean age (β = -0.0010, p = 0.3418), vulnerability score (β = 0.0020, p = 0.2318), and quality score (β = -0.0093, p = 0.5530) of the studies.
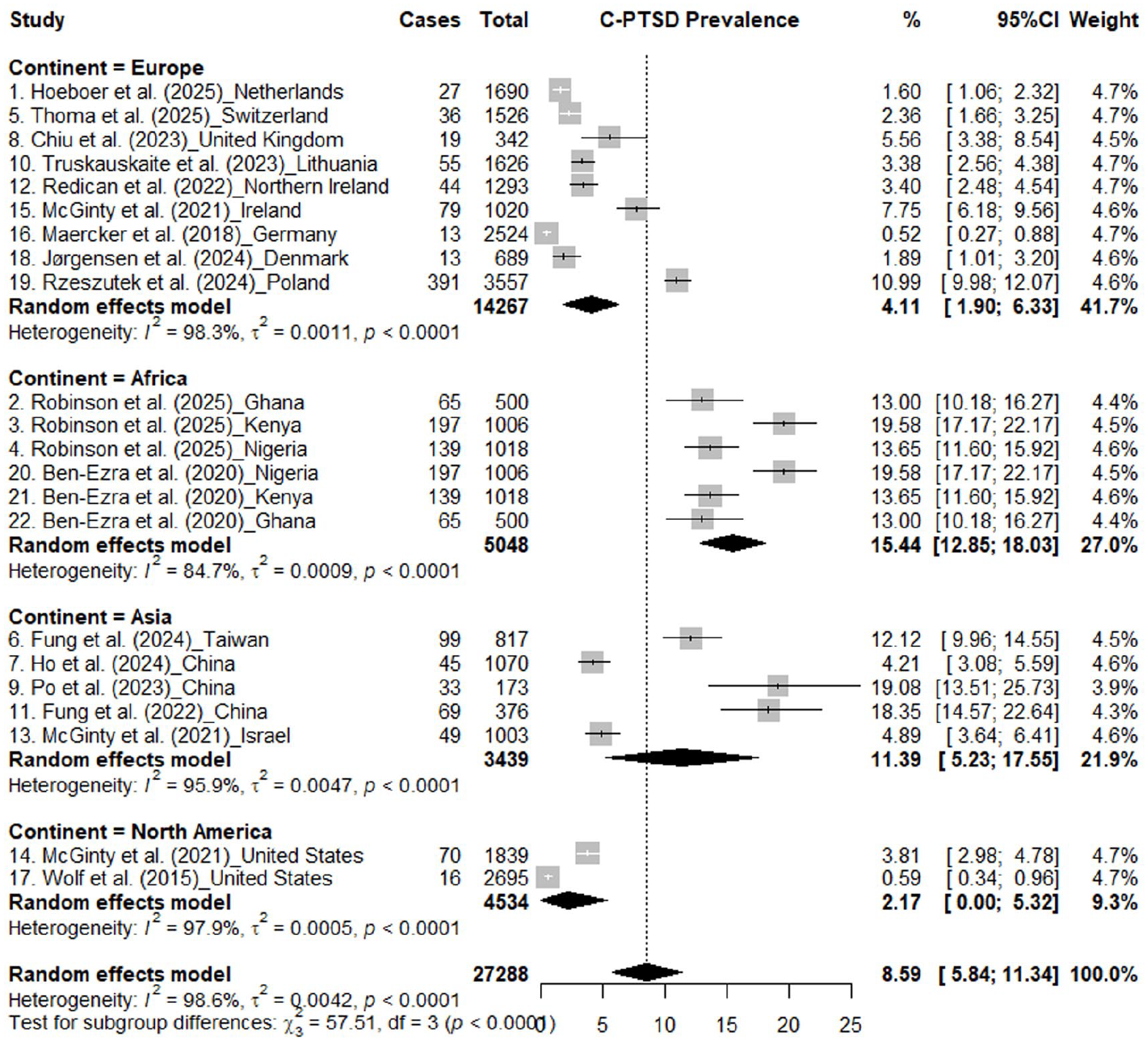
Forest plot of C-PTSD prevalence studies (grouped by continent).
Discussion
The developers of the ICD-11 mental, behavioral and neurodevelopmental disorders chapter included C-PTSD in the hope that it might capture the symptomatology of extreme, prolonged or multiple forms of trauma (Reed et al., 2022). To date, this is the first study to comprehensively examine the global prevalence of C-PTSD in the community. Overall, the findings of this review indicate that the prevalence of C-PTSD in this population is moderate (6.72%).
Similar preliminary findings have been found in narrative reviews on the prevalence of C-PTSD in the general population (Maercker et al., 2022). This result is also similar to that found in non-treatment seeking refugee population samples (de Silva et al., 2021; Lechner-Meichsner et al., 2024). This prevalence is far below that of treatment seeking populations exposed to horrific trauma (Czerwińska & Kucharska, 2024; de Silva et al., 2021; Evans et al., 2022; Grinsill et al., 2024; Lechner-Meichsner et al., 2024).
Furthermore, heterogeneity in the characteristics of the included studies may affect estimates related to publication bias (Oltmanns & Oltmanns, 2021). This type of bias, common in most studies, may be associated with factors such as sample size, magnitude and direction of the effect, as well as statistical significance (Sánchez-Meca et al., 2021).
In the meta-analysis carried out, the prevalence of C-PTSD varied depending on the continent, scale, type of sample, country, and language. This was expected since Sánchez-Meca et al. (2021) highlight those sociodemographic characteristics constitute relevant sources of divergence, as evidenced in this study. This result also aligns with the argument that there are methodological differences between the studies, such as the representativeness of the samples included and differences in cultural attitudes when completing the questionnaires (Maercker et al., 2022). In addition, it was expected that in countries with a higher rate of poverty and violence such as those in Africa, higher rates of C-PTSD prevalence would be detected. Also, in contrast with what was mentioned in other reviews/manuals (Lonnen & Paskell, 2024; WHO, 2024b), there was no increased prevalence of C-PTSD as the percentage of the female gender increased.
The sources of variation identified in this review explain the differences in the prevalence of C-PTSD in a significant way. Therefore, it is more appropriate to interpret these results as a set of factors interacting with each other, producing changes in the prevalence of this new disorder.
Limitations and Future Directions
The inclusion of five studies from non-Western countries promotes the generalizability of the findings to cultures where the psychiatric nosology does not seem to conform (or partially conforms) to traditional Western standards of signs and symptoms, which is one of the strengths of this systematic review (Fabrega, 2001). However, this review has some limitations. This concerns the evidence included in this review. All investigations used self-report measures, which could bias the prevalence estimates somewhat. In addition, there were continents with two studies, which makes the interpretation of results difficult. It is still preferable to take them with a grain of salt.
We can say that the overall findings of this review remain valid despite these methodological restrictions. In fact, the prevalence found in this review can serve to guide researchers, clinicians and public policy makers in their work and to obtain more accurate and appropriate results. Much research remains to be done on the prevalence of C-PTSD among specific population groups who suffered specific episodes of trauma.
Final Comments
Knowing the prevalence of C-PTSD in the community setting represents a key tool for formulating health policies, reducing stigma, improving service planning, and identifying risk factors. Promoting gender equality and non-violent and respectful relationships within families, institutions, and communities form the cornerstone of C-PTSD prevention approaches (Salter & Hall, 2020). A society that prioritizes the study and care of mental health is a more just, equitable, and healthy society. C-PTSD is known to be a debilitating condition that deeply impacts the lives of those who suffer from it.
The inclusion of C-PTSD in the ICD-11 allows for a better understanding and treatment of this disorder, differentiating it from classic PTSD and recognizing the need for specific therapeutic approaches. Early diagnosis and access to appropriate interventions can significantly improve the quality of life of those affected. In this research we have accurately identified the prevalence of this disease in the community setting, which will serve for posterity in terms of improving clinical practice, management of health resources and services by authorities, and adequate awareness of users and consumers.
Supplemental Material
sj-docx-1-isp-10.1177_00207640251368064 – Supplemental material for A Systematic Review and Meta-Analysis of the Global Prevalence of ICD-11 Complex Post-Traumatic Stress Disorder in the Community
Supplemental material, sj-docx-1-isp-10.1177_00207640251368064 for A Systematic Review and Meta-Analysis of the Global Prevalence of ICD-11 Complex Post-Traumatic Stress Disorder in the Community by Luis Hualparuca-Olivera, Elsa Vigo-Ayasta, Julio Torales, Cristian Ramos-Vera, Tomás Caycho-Rodríguez, Margarita Calle-Arancibia, Dennis Calle and Antonio Ventriglio in International Journal of Social Psychiatry
Footnotes
Acknowledgements
We thank the reviewers for their comments regarding our paper for its improvement.
Author Contributions
LH-O led the conceptualization of the manuscript, also contributed to the data analysis, and acted as a third reviewer to resolve discrepancies in the study selection and risk of bias assessment stages. TC-R and EV-A acted as blinded reviewers during the search, selection, and risk of bias assessment of the studies. CR-V wrote the article and JT reviewed it critically. JT also assisted in data analysis. MC-A, DC and AV participated in the conceptualization, formal analysis, methodology, and writing the original draft. LH-O performed the final review and revision. All authors approved the final version of the manuscript and share public responsibility for the content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.