
Abstract
Introduction:
Night Eating Syndrome (NES) is a distinct psychopathological entity variously considered as a mental health disorder, eating disorder or circadian rhythm disorder. Medical students are faced with hectic schedules, sleep interruptions and high-stakes exams as they become healthcare providers. Such social factors coupled with poor dietary practices may impact their mental health and biological clocks, leading to NES amongst this population. However, the magnitude of its occurrence and the associated factors are still not well understood, especially in an Indian context. The present study was planned to determine the prevalence of NES and to explore the association between NES and selected psychosocial health profiles amongst undergraduates.
Methodology:
An observational, analytical cross-sectional study was undertaken in a tertiary care hospital in Central India. The study included a total of 414 medical students representing all academic years. The data collection tool comprises a structured questionnaire comprising socio-demographic information, the Night Eating Diagnostic Questionnaire (NEDQ), Insomnia Severity Index (ISI), Simple Lifestyle Indicator Questionnaire (SLIQ) and Patient Health Questionnaire-2 (PHQ-2).
Results:
The overall prevalence of Night Eating Syndrome is 13.8% and the majority are mild NES syndrome (mild: 10.1%, moderate: 1.7% and severe: 1.9%). Participants with depressive symptoms were 12.8%. In unadjusted analysis, participants having insomnia (OR = 3.16, 95% CI [1.7, 5.7]) and depression (OR = 2.05, 95% CI [1.0, 4.2]) were found to be predictors of night eating syndrome. After adjusting for age, presence of depression, personal history of chronic disease, insomnia and current year of education in medical school, insomnia (OR = 3.08, 95% CI [1.6, 5.7]) was the only predictor independently associated with NES among college-going students. BMI was not found to be a predictor of NES amongst the study participants.
Conclusion:
Night Eating Syndrome has a significant association with insomnia when adjusted for concomitant depression implying the need to tackle sleep and mental health as lifestyle factors; which play a role in the development of NES and to elucidate further on this association, emphasising its circadian impact leading onto Non-Communicable Diseases.
Introduction
The age group of 15 to 24 years, defined as youth (Dwivedi et al., 2020), is the period of significant career development and psychosocial stress. Its impact on one’s behaviour to cope with the surroundings leads to poor attention paid to meal choices. Besides quality and quantity, timing of the meals plays a significant role. Aberrant timing of food intake leading to psychological afflictions may predispose the youth to such dysfunctional chrono-disruptive behaviours which come under the Night Eating Syndrome, which had its recent inclusion in the Diagnostic and Statistical Manual 5th Edition (DSM-5) under ‘Other Specified Feeding or Eating Disorder (OSFED) in 2013 (American Psychiatric Association, 2013).
NES has significant associated psychopathological morbidity. A myriad of studies have explored associations between NES and psychiatric conditions (Hamdan et al., 2023) and sleep disturbances (Gan et al., 2019; Matsui et al., 2021; Nolan & Geliebter, 2012). With positive correlations between insomnia, depression and anxiety (even attachment anxiety, Wilkinson et al., 2022, and food addictions, Nolan & Geliebter, 2016), these psychiatric manifestations have possible links with the serotonergic system (Cleator et al., 2012). Through its neurohumoral disturbances in the levels of cortisol, leptin and melatonin with autonomic system derangements (Cleator et al., 2012; Garaulet et al., 2010), a distinct mental health disorder manifests.
The NES could potentiate behaviours that may culminate in the occurrence of Non-Communicable Diseases (NCDs). This chrono-disruption attacks the synchronisation and entrainment of internal biological clocks. It is well proven that these practices perpetuate circadian misalignment, an increased total daily calorie intake (Basdeki et al., 2022; Reid et al., 2014) and decreased energy expenditure (Chaput et al., 2023). This creates altered metabolic physiology with impaired glucose tolerance and insulin sensitivity (Garaulet et al., 2010; Reid et al., 2014) potentiating metabolic syndrome and its components of obesity and dyslipidaemia (Yoshida et al., 2018), as evidenced by raised triglycerides and waist circumference in night eaters (Gallant et al., 2014).
In addition to the above, subclinical vascular damage has been reported in these individuals as carotid plaques (Basdeki et al., 2022) and faster progressive arterial stiffening in habitual night eaters (Zhang et al., 2020). Cohort studies corroborate the habit of late-night overeating and later meals to be associated, and an independent risk factor for all-cause cardiovascular mortality (Palomar-Cros et al., 2023; J. B. Wang et al., 2023). There is evidence of a higher risk of diabetes and cancer mortality due to late-night eating, with more risk with more frequent, more energy-dense foods (P. Wang et al., 2024).
A total of 80% of mortality from NCDs are derived from four major diseases with two of them being cardiovascular diseases (CVDs) and diabetes, the latter being strongly intertwined with metabolic syndrome. With the global rapid epidemiological transition of disease burden to NCDs, especially in low- and middle-income countries like India, (NCD Countdown, 2018) an urgent need to elucidate further upon the link between NES and NCDs is crucial. With WHO’s best buys strategy to reduce burden by working on risk factor exposure, timely intervention upon these simple lifestyle behaviours may prove greatly helpful in reducing NCDs.
With one of the major behavioural risk factors of NCDs as an unhealthy diet, evaluation of NES in youth is imperative, as it is in these formative years the disease begins to evolve. A timely focused intervention at this stage, equipped with adequate evidence-based data, would hinder the disease progression.
The demanding nature of medical education drives these budding professionals to navigate irregular study schedules, sleep disturbances and a need to prove themselves in high-stakes examinations. These factors make this subpopulation highly prone to the development and perpetuation of NES. Despite its growing recognition as a distinct clinical entity, there is a notable scarcity of research on NES within the Indian context – fewer than five studies exist, and only one has focused on university students. Even among these, only a single study has employed the standard DSM-5 diagnostic criteria, and that too among engineering students. To date, no study has specifically examined NES in Indian medical students, highlighting a significant gap in the existing literature. Our study aims to bridge this gap by being the first of its kind in India to assess the prevalence of NES and explore its associated psychosocial factors among medical undergraduates. It would serve to shed light from an Indian perspective, aiding in delineating this entity globally. As understanding of this relatively new disorder continues to evolve, our study would attempt to contribute to building a holistic interpretation of the same.
Materials and Methods
Study Design & Setting: It was an Institution-based observational analytical cross-sectional study conducted in a tertiary care medical teaching institute in Central India. Every year 125 students gain admission to this Institute pursuing the medical undergraduate course.
This medical teaching institution serves as a pan-country representation, admitting students from diverse regions. Institutional policy mandates that all students reside in the hostel.
The study was carried out for 6 months from September 2023 to February 2024. Only those Undergraduate students who came under the age range of 18 to 24 years were included. There were no specific exclusion criteria. Whomsoever gave the consent to be a part of this research, were included.
Sample Size: Assuming a 12% prevalence of NES reported in a study conducted in Malaysia adherent to the diagnostic criteria (Anthonisamy et al., 2023), with 5% absolute precision, a design effect of 2 (to account for the clustering effect) and an expected response rate of 80%, a sample size of 406 medical students with a 95% confidence interval was calculated for the present research. Statulator, an online software was used for calculating sample size (Statulator, n.d.). However, upon approaching all the medical students, 414 agreed to participate in this research.
Sampling: The intake capacity of the chosen medical college is 125 students per year with around 500 students studying any time during a year. We got the list of all the then-enrolled students from the first year to the final year from the concerned authorities. From this sampling frame, all students were approached from each year. All the participants were approached in person by the researcher, who explained in detail the purpose of the research and distributed the questionnaire. The questionnaire did not have any personal identifiers. The data collected was stored in a password-protected computer with access to only researchers involved in the study.
Operational Definition and Tool for Data collection
A pretested structured questionnaire was used for data collection. A pilot test was done to understand the comprehension and relevancy of the questionnaire. Changes were made based on the inputs from pilot test participants and the final tool was administered which comprised the following sections:
The first part of the questionnaire comprises demographic information like age, gender, current year of MBBS course, father’s and mother’s occupation, family history, and personal history of chronic diseases. Self-reported weight and height were recorded, and body mass index (BMI) (in kg/m2) was calculated and classified according to the WHO Asian classification (The Asia-Pacific Perspective: Redefining Obesity and Its Treatment, 2000).
The second part assesses the night eating patterns for which a 22-item NEDQ (Night Eating Diagnostic Questionnaire) tool was used. It is a self-reported tool, consisting of the clinical diagnostic criteria (Allison et al., 2010; Nolan & Geliebter, 2019):
1. The daily pattern of eating demonstrates a significantly increased intake in the evening and/or nighttime, as manifested by
a. At least 25% of food intake is consumed after the evening meal
b. At least two episodes of nocturnal eating per week
2. Awareness and recall of evening and nocturnal eating episodes are present.
3. The clinical picture is characterised by at least three of the following features:
a. Lack of desire to eat in the morning and/or breakfast is omitted on four or more mornings per week
b. Presence of a strong urge to eat between dinner and sleep onset and/or during the night
c. Sleep onset and/or sleep maintenance insomnia are present four or more nights per week
d. Presence of a belief that one must eat in order to initiate or return to sleep
e. Mood is frequently depressed and/or mood worsens in the evening.
4. The disorder is associated with significant distress and/or impairment in functioning.
5. The disordered pattern of eating has been maintained for at least 3 months.
6. The disorder is not secondary to substance abuse or dependence, medical disorder, medication or another psychiatric disorder. (this criterion has not been assessed by questionnaire but noted down in the study tool)
The NEDQ tool showed positive convergent validity with NEQ (Night Eating Questionnaire) in university students and the community sample. (rs = 0.25, rs = 0.54 with p < .001). While NEQ attempts to screen independently of diagnosis, NEDQ establishes a diagnosis based on the proposed DSM criteria; segregating individuals into clinically useful diagnostic groups (Nolan & Geliebter, 2017).
Based on the above diagnostic criteria, two systems were used to categorise the participant as having the Night Eating Syndrome. A hierarchical scoring system categorised based on the following:
Non-NE = normal (does not meet any criteria)
N = mild night eater has 1 criterion from 1 (but does not meet criteria NE or NES)
NE = moderate night eater has 1 criterion from 1 plus >2 of 5 qualifiers from criteria 3 (but does not meet criteria NES)
NES = full syndrome Night Eater has 1 criterion from 1 plus >2 of 5 qualifiers from Criteria 3 plus 4 and 5
Another one is dichotomous, Normal or Non-NES if does not meet any of the parameters above and NES or full syndrome if Night Eater has 1 parameter from 1 plus >2 of 5 qualifiers from Criteria 3 plus Criteria 4 and Criteria 5.
The third part is a screening tool for detecting depression, for which the Patient Health Questionnaire-2 (PHQ-2) was used. This tool has been effective with reasonably good sensitivity and specificity of 61% and 92% respectively for detecting major depression based on the cutoff score of 3 or greater in primary care patients (Arroll et al., 2010).
The fourth part was the Insomnia Severity Index (ISI), administered to detect insomnia in study participants over the last 2 weeks. It is a Likert-type scale composed of three sleep-related and four wake-related items, each item score ranging from 0 to 4. A total score of ⩾15 corresponds to moderate to severe insomnia which is clinically significant. The scale has been proven to be a reliable instrument to screen for insomnia in the general population, with its Cronbach’s alpha coefficient of 0.90 when tested over 959 community participants (Morin et al., 2011) and 0.95 when tested amongst a group of obese veterans (Dorflinger et al., 2017).
The last part of the tool consists of evaluating the lifestyle factors using the Simple Lifestyle Indicator Questionnaire (SLIQ) (Godwin et al., 2008), which includes diet, exercise, smoking, alcohol consumption and perceived stress with relevant questions for the same. It assigns category scores to each which range from 0 to 2. A higher score predicts a category score indicative of a healthy lifestyle. It then computes a total score ranging from 0 to 10 wherein 0 represents unhealthy and 10 represents healthy. This score is used to classify individuals into healthy, intermediate and unhealthy. This scale has shown a validity correlation coefficient of 0.77. (Godwin et al., 2008) It has also shown good convergent and concurrent validity to briefly assess an individual’s lifestyle in research (Godwin et al., 2013).
Data Analysis: JAMOVI 2.3.28 solid version was used for the statistical analysis. The proportion of Night eating syndrome, depression, categories of insomnia, categories of lifestyle indicators and other background characteristics are presented as frequencies and percentages (%). To assess the effect of various psychosocial factors recorded in this research on Night Eating Syndrome. Binary logistic regression was employed to identify factors associated with the outcome variable. Prior to model building, collinearity among independent variables was assessed using the Variance Inflation Factor (VIF) for continuous and ordinal variables, and the Chi-square test of independence for nominal variables. For inclusion in the multivariable logistic regression model, a liberal p-value threshold of <0.2 in the bivariate analysis was adopted. This approach ensures that potentially relevant variables are not excluded prematurely. The Hosmer-Lemeshow goodness of fit test was employed to assess how well the model fits the data.
Ethical Consideration: The study was initiated after obtaining ethical clearance from the Institutional Ethics Committee and necessary permission from college authorities (IEC approval number: IEC/Pharma/2023/672, dated 2nd November 2023). The research was carried out without affecting the academic activities of the participants. Informed written consent was obtained from the participants.
Results
Participant Characteristics: A total of 414 students enrolled in the study. The mean age was 19.93 ± 1.51 years and the majority were males (68.8%). The students comprising the population were from the first year (26.8%), second year (25.4%), third year (26.6%), and fourth year (21.3%) studying in the undergraduate curriculum respectively. 5.8% of the total had a self-history of chronic diseases while 47.1% had a family history which included Diabetes, Hypertension, Thyroid disorders, and Asthma (Table 1).
Sociodemographic and Risk Factors of the Study Participants.
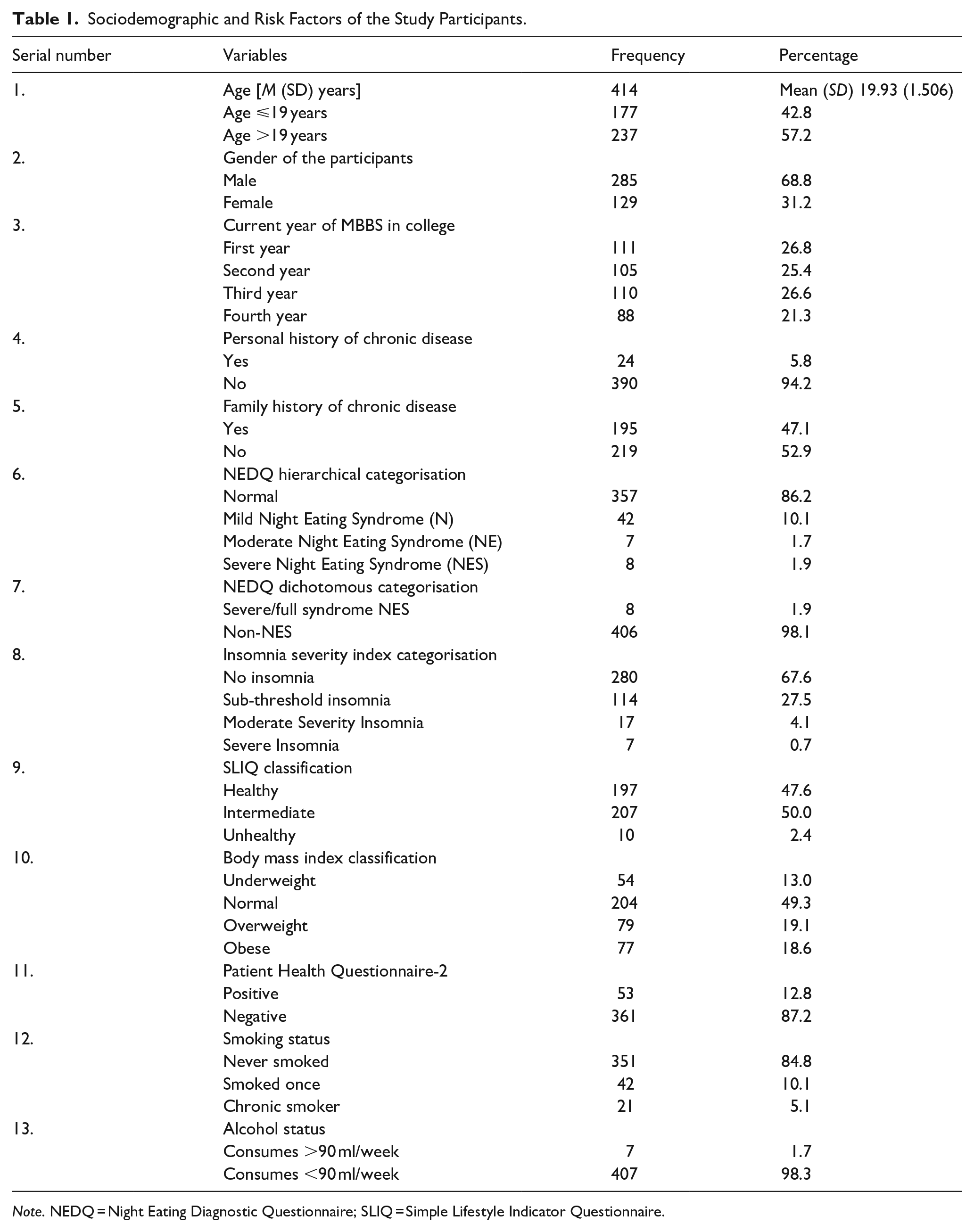
Note. NEDQ = Night Eating Diagnostic Questionnaire; SLIQ = Simple Lifestyle Indicator Questionnaire.
Night Eating Syndrome: Applying the hierarchical categorisation for NES, participants were placed under four categories consistent with the standard diagnostic criteria formulated in the scale as follows: severe NES (1.9%); moderate NES (1.7%); mild NES (10.1%) and normal or without any NES (86.2%). 1.9% of the participants complied with the criteria for full syndrome NES. For analysis, stratification was done into two groups with group 1 labelled non-NES (normal, does not meet any criteria) and group 2 labelled having NES or presence of night eating (combination of mild, moderate and severe syndrome). The NES group comprised 13.8% of the sample population while 86.2% had no NES (Figures 1 and 2).
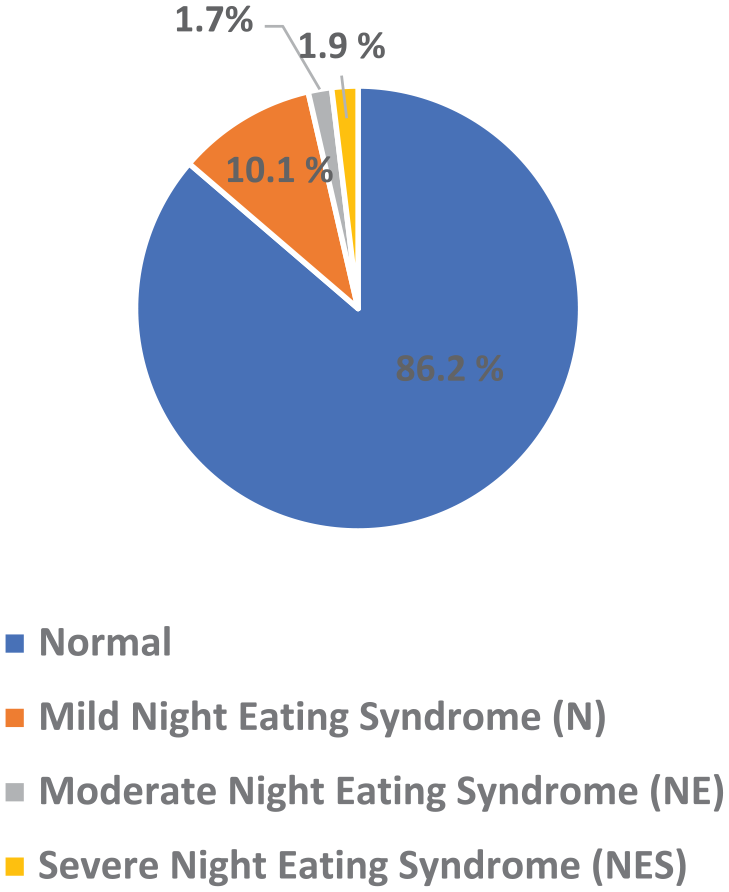
Proportion of Night eating syndrome based on NEDQ hierarchical categorisation.
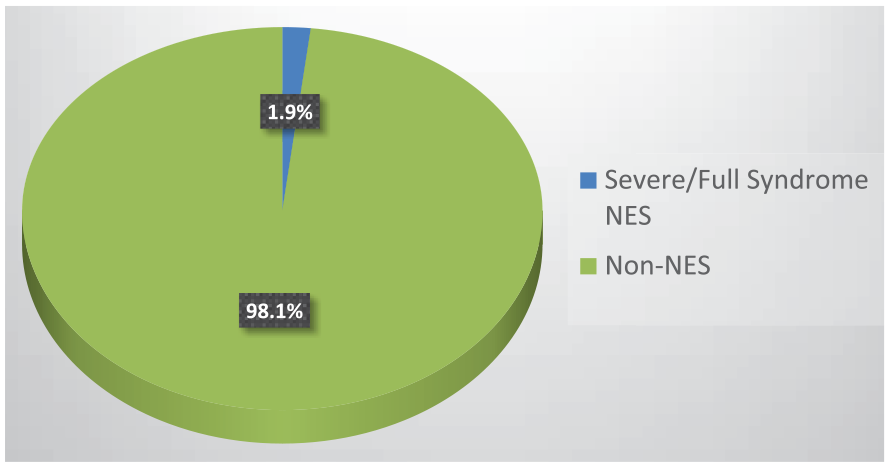
Proportion of Night eating syndrome based on NEDQ dichotomous categorisation.
Psychosocial Profile: Analysis of the ISI scores showed that 4.8% had clinically significant insomnia, 27.5% had sub-threshold insomnia, and 67.6% had no insomnia. Based on PHQ-2, 12.8% of the participants were screened as depressed while the rest 87.2% had no depression. The composite SLIQ score separated the participants as 2.4% being healthy, 50.0% being in the intermediate category and 47.6% being healthy. Asia-Pacific BMI Classification of Body Mass Index segregated participants into 13% as underweight, 49.3% as normal, 19.1% as overweight and 18.6% as obese.
Predictors of Night Eating Syndrome: There were no significant differences between NES and non-NES groups concerning demographic factors including sex, age or year of study in the institution; or alcohol consumption, smoking status, BMI classification, SLIQ score, self- or family history of chronic diseases.
However, insomnia categorisation was significantly associated with Night eating presence categorisation, with all p-values<.001. Those having some form of night eating behaviour had 3.200 times higher unadjusted odds of suffering from clinically significant insomnia than those not having any form of night eating behaviour. Also, the group having NES had 2.055 times more unadjusted odds of being depressed than those free of night eating (p-value <.045) (Table 2).
Distribution of Night Eating Diagnostic Questionnaire (NEDQ) Hierarchical Classification With Other Sociodemographic and Risk Factors.
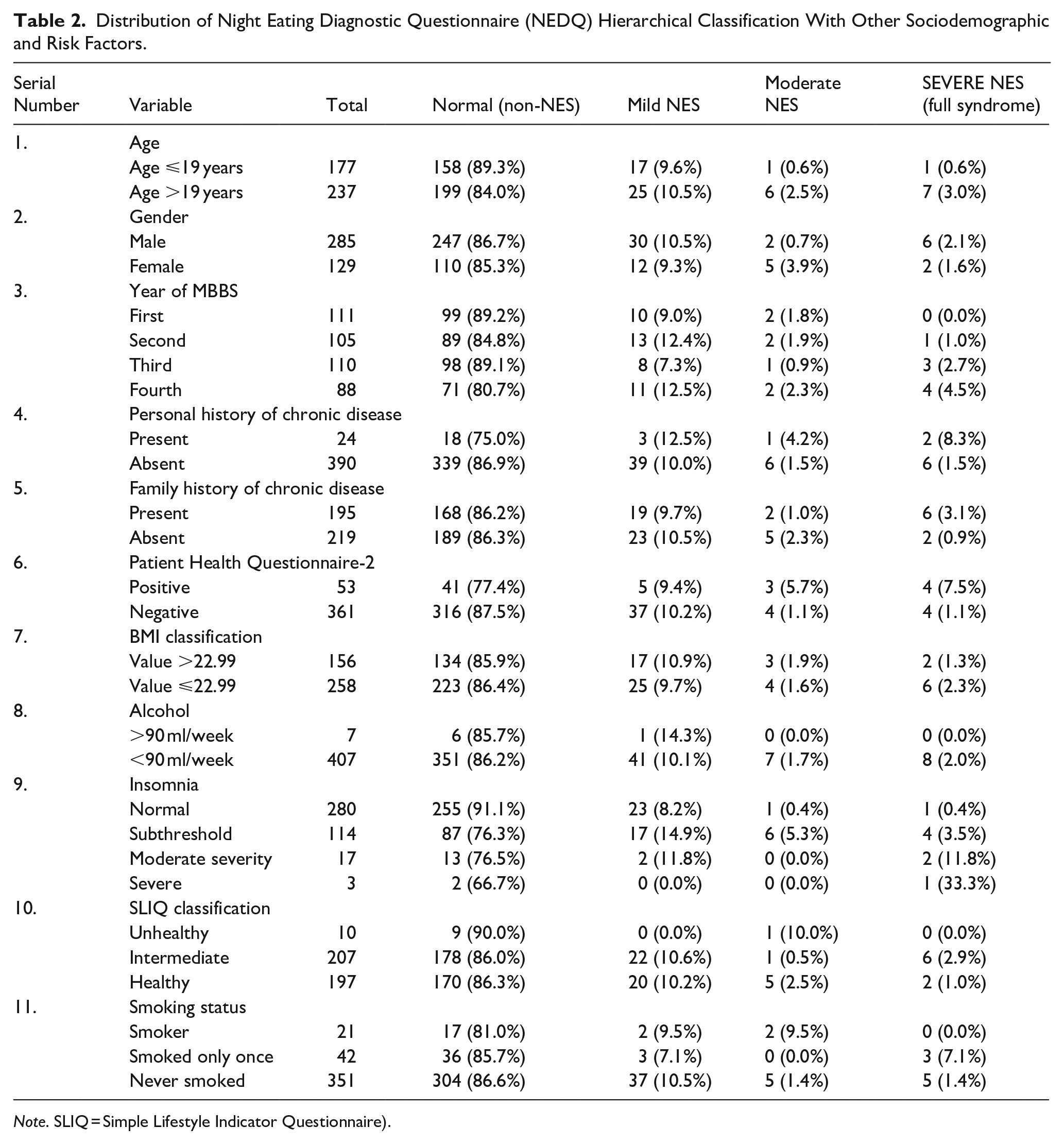
Note. SLIQ = Simple Lifestyle Indicator Questionnaire).
Adjusted Predictors of Night Eating Syndrome: In unadjusted analysis, participants having insomnia (OR = 3.16, 95% CI [1.7, 5.7], OR = 3.4, 95% CI [1.14, 10.1]) and depression (OR = 2.05, 95% CI [1.0, 4.2]) were found to be predictors of NES. Variables associated with p-value <0.2 were entered into the final model to see the effect of various variables on NES after adjusting the confounding effect. Age, history of depression, personal history of chronic disease, insomnia and current year of education in medical school were entered into a final model. After adjusting for all these factors, insomnia (OR = 3.08, 95% CI [1.6, 5.7]) is the only predictor which remained significant explaining NES among college-going students (Table 3).
Predictors of Night Eating Syndrome Among the Students -Logistic Regression Analysis (Univariable and Multivariable Analysis).
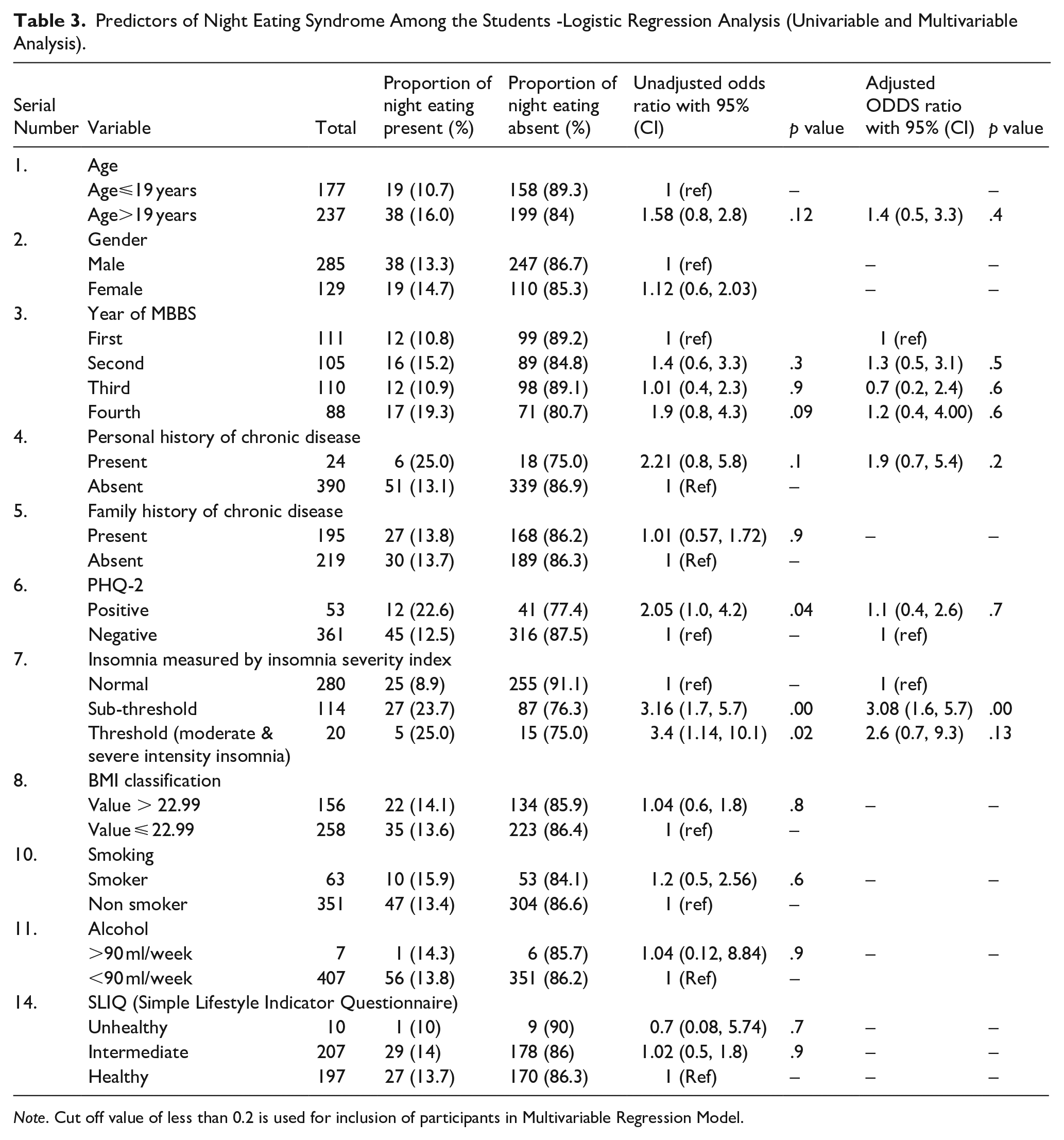
Note. Cut off value of less than 0.2 is used for inclusion of participants in Multivariable Regression Model.
Discussion
The present study among medical undergraduates aimed to delineate the prevalence of NES in an Indian context and correlate the associated psychosocial factors. The prevalence of NES, including all its forms from mild to severe, was 13.8%, with the remaining 86.2% as normal, having no NES. While those in full syndrome were only 1.9%, the rest 1.7% were in moderate NES and 10.1% were mild NES. Besides NES, alarming rates of psychosocial problems were found, comprising depression, insomnia, unhealthy lifestyle behaviour and overweight or obesity.
The overall prevalence of NES, when compared to studies in India, was comparatively lower, referring to the study on engineering students as 37.3% (Murthy et al., 2024, pp. 1–11) and that on nursing students as 54% (M. Kaur, 2022). While the latter utilised a different scale based on standardised criteria, the former applied the same as our study. This highlights that a medical background confers relatively greater conscience and awareness among students about eating habits.
The prevalence of NES was found to be closest to that of an American study (12.4% for the presence of night eating) (Yahia et al., 2017), with similar proportions in mild, moderate and severe forms of the syndrome; 8.5%, 2.7% and 1.2% respectively (Yahia et al., 2017). The similarity can be attributed to the profile matching amongst the population samples chosen.
The overall prevalence of 13.8% as found in our study correlates with the prevalence found in studies conducted on university students from Malaysia as 12.2% (Gan et al., 2019) and 14% (Mohamad & Mahkota, 2023, p. 133), from Saudi as 10.3% (Ahmed et al., 2019). A study from Pakistan had very high values of prevalence, 49.36% (Zaidi et al., 2020), while those from the West had much lower values of 2.9% (Runfola et al., 2014) and 2% (Nolan & Geliebter, 2016). All the above utilised the Night Eating Questionnaire (NEQ) as their diagnostic tool.
Prevalence is affected by the scale chosen. NEQ is known to assess global symptom severity only, whose positive predictive value varies with the cutoff chosen (Allison et al., 2008; Nolan & Geliebter, 2017). The present study has assessed NES using the Night Eating Diagnostic Questionnaire (NEDQ), a 22-item self-reported questionnaire adherent to the diagnostic criteria as given in DSM-5 (Nolan & Geliebter, 2019). Besides conferring diagnostic precision, this facilitates comparability of our study findings, thereby contributing towards standardising NES research globally.
An Indonesian study utilising NEDQ reported 82% prevalence with a 16% full syndrome NES compared to our 1.9% full syndrome NES prevalence (Djunet, 2023). More females and a narrower age range may be responsible for the disparity. Two systematic reviews placed the prevalence of NES in the range of 3% to 15% (J. Kaur et al., 2021; Muscatello et al., 2022), our value of 13.8% remains concordant with the said range. Amongst various studies globally, diversity and distinctiveness of the prevalence of NES among medical students may be attributed to differences in the diagnostic criteria and scales employed, population socio-demographics, cultural differences, institutional policies and different levels of urbanisation, driven by upcoming industrialisation (Pike & Dunne, 2015), impacting the access to food, local food environments and eating behaviours.
The proportion of NES does not significantly differ with age or gender in our study. With few studies favouring a female preponderance, there has been a consensus amongst studies that neither age nor gender led to any such difference as per the systematic review (J. Kaur et al., 2021).
Additionally, we found that those in the fourth or final year had the highest proportion of night eating behaviour (19.3%) compared to students in other years of the medical undergraduate curriculum, in line with another study (Zaidi et al., 2020). Though not significant, this could be explained by higher levels of stress and pressure to live up to their family’s academic expectations and night study patterns. There is strong evidence of stress precipitating night eating (Gan et al., 2019; McCuen-Wurst et al., 2018), supported by the quantitative data on the disturbed hypothalamic-pituitary-adrenal axis in these subgroups (Birketvedt, 1999; Birketvedt et al., 2002).
There were no significant correlations between NES and BMI amongst our participants. This association, despite having been explored in multiple studies, is complex. Found mostly in an older sample (Meule, Allison, Brähler, & De Zwaan, 2014; Nolan & Geliebter, 2016) or a clinically obese population (Allison et al., 2008; Gallant et al., 2014); with no association among college students (Nolan & Geliebter, 2012; Runfola et al., 2014). Lower age amongst non-obese NES patients implied a possible precession to obesity (Marshall et al., 2004; Spaggiari et al., 1994) with probably an elevated risk of weight gain in the future (Nolan & Geliebter, 2012). These discrepancies may be attributed to gender, age and pre-existing obesity (Meule, Allison, Brähler, & De Zwaan, 2014). There is evidence of emotional eating moderating the relationship between NES and BMI (Meule, Allison, & Platte, 2014) which further needs to be explored.
Upon mental health assessment with PHQ 2, students who screened positive for depression had 2.1 odds of having NES. Studies from India and Pakistan on college students have shown depression to be associated with NES (Zaidi et al., 2020; Murthy et al., 2024, pp. 1–11). Multiple studies have shown samples with NES having significant co-morbid depressive symptoms (Calugi et al., 2009; Colles et al., 2007), negative affect and anxiety disorders irrespective of pre-existing obesity status or age (Muscatello et al., 2022).
However, in our regression model, depression had a confounding effect, with insomnia being the primary predictor of Night Eating Presence. Also, students with any form of night eating behaviour had 3.4 times higher odds of suffering from clinically significant insomnia than those not having any form of night eating behaviour. The confounding effect of depression may be explained by the usage of a screening tool consisting of only two questions, which were self-reported. This may be responsible for masking the association between depression and NES in the final model.
Night eating behaviour and insomnia may be the manifestation of deep-rooted mental health issues (Babicz-Zielińska et al., 2013). The residential requirement of hostels, combined with the experience of being away from home, may elevate the risk of developing NES among the student population. This socio-cultural prospect of hosteller status in concert with rigorous Indian medical training may add another dimension to NES literature, emphasising occupational identity and academic strain as possible emerging risk factors.
Besides NES, insomnia can also lead to internal circadian desynchrony and delayed timing of calorie intake (Gallant et al., 2014), predisposing to aberrant metabolism (Chaput et al., 2023). When such stressed-out students prefer a worse diet in the form of more high-calorie, high-fat items, particularly at night, it adds to a higher total daily calorie intake (Basdeki et al., 2022). This cumulates to a higher BMI and further increases the risk of NCDs (Gomes et al., 2023), like obesity (J. B. Wang et al., 2014) and metabolic syndrome (Yoshida et al., 2018).
With insomnia being the sole predictor in our adjusted model, sleep and night eating are deeply intertwined. Insomnia patients have more chances of having NES and vice versa with either psychopathology preceding the other (McCuen-Wurst et al., 2018), or even having an additive effect (Muscatello et al., 2022). Characterised by a circadian phase delay, NES is possibly the first to have dissociation of patterns and timing of eating and sleeping (O’Reardon et al., 2004), presumably acting as a peripheral oscillator in humans (Kandeger et al., 2018). This highlights the bidirectional psychopathology between night eating and insomnia, both augmenting the other (Christensen & Short, 2021) through hormonal aberrations (Garaulet et al., 2010). Both independently increasing the risk of weight gain and NCDs, insomnia and alterations in metabolic physiology with circadian disruption due to NES is a complex inter-relationship which needs further exploration.
This bidirectionality may represent a parallel manifestation of an underlying stress-induced circadian disorder. Our findings suggest that an increased stressful environment and educational context of academic pressure amidst separation from home constitute a unique psychosocial strain, besides vulnerability conferred through circadian or metabolic dysfunction. These factors may represent a multifaceted association contributing to the initiation of disease progression, which may begin as a possible maladaptive behavioural change attempting to cope with internal circadian desynchrony. This interaction would likely be such that the contribution of each factor towards disease development is influenced by psychosocial and demographic attributes of each individual. The disease may perpetuate as a maladaptive stress dysregulation compounded with sleep-related circadian strain. This probable integration invites a re-conceptualisation of NES in global literature, expanding from the compartmentalised description as an eating disorder and redefining it in a broader framework as a chronobiological psychosocial dysregulation syndrome with a multifactorial mechanism.
This study has the following strengths. First, to our knowledge, this is the first study in the Indian context which systematically quantifies NES among adults in academic institutional settings, adherent to clinical diagnostic criteria. Besides contextually adding to global epidemiological mapping of the disease landscape, our study facilitates cross-study comparison and delineates possible new socio-cultural influences. Secondly, our study findings encourage the expansion of understanding about NES in global literature. Thirdly, the high response rate may be favourable in precise assessment of the disorder. These findings may be generalised to the medical fraternity across various colleges.
Our study findings must be interpreted with these underlying limitations. Our cross-sectional design hinders ascertaining temporality or any causal inference. We cannot determine whether these psychosocial profiles are exposure or mediator variables related to NES. Self-reporting leads to too much reliance on the sincerity and willingness of participants, leading to information bias; as medical students aware of the stigma associated with mental health disorders might underreport the severity of their symptoms. Some independent variables like tobacco or alcohol may lead to social desirability bias. With questions based on the memory of behaviour over the past months, recall bias sets in. Limited to a single college campus, the voluntary nature of student recruitment may introduce a selection bias; those with disordered eating did not choose to participate, thereby underestimating the prevalence.
The study has the following institutional implications. Medical students who are future healthcare providers must have adequate exposure to healthy lifestyle choices. Incorporating the integrated approach to NES, programmes related to initiatives defining access to different food categories, sleep hygiene and stress management should be considered in these demanding academic environments. Emphasis on health and well-being within the medical education framework would serve as protective factors against NES. Instead of treating NES as an isolated issue, reasons for indulging in NES should be explored with qualitative studies, addressing the perception of students about this issue and its socio-cultural factors. Early identification through heightened awareness with timely intervention is desirable. Besides expanding the scope of study to more university campuses, attributes of students in general may be potential confounding variables. Controlling for these factors in future studies is advisable. As the present study adopts a cross-sectional design, establishing actual causality requires longitudinal or cohort studies that can explore these multifactorial associations in greater depth, clarify the temporal sequence of events, and thereby enhance our understanding of various facets of NES.
Conclusion
Night Eating Syndrome was significantly associated with insomnia. With evidence growing linking this disorder with adverse metabolic outcomes and trends of sleep compromise amongst budding students, emphasis on this vulnerable population would hinder not only these manifested mental health problems but also prevent its evolution and promote a healthy youth. Being an aberrant lifestyle practice, intervention through a simple behavioural modification would go a long way in reducing the disease burden at large. Future studies are warranted to investigate further, elaborating on mechanisms and enhancing a more complete understanding of this disorder from all aspects.
Footnotes
Ethical Considerations
The study was reviewed and approved by the Research Cell and Institutional Ethical Committee of AIIMS, Nagpur (IEC Clearance No- IEC/Pharmac/2023/672.
Consent to Participate
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The data will be available on valid request to authors.