
Abstract
Background:
Further research is crucial to clarify the factors associated with mental disorders that directly impact the well-being of medical students.
Aims:
To investigate the various stressors experienced by medical students and the longitudinal association between these stressors and mental health outcomes (depression, anxiety, and stress).
Method:
A two-year longitudinal study was conducted with medical students completing questionnaires at baseline and after 2 years of follow-up. Mental health outcomes (depression, anxiety, and stress) were assessed using the depression, anxiety, and stress scale – 21 items, while stressors were assessed using the Medical Student Stress Factor Scale. Structural equation modeling (SEM) was employed for statistical analyses.
Results:
The study included 231 participants, of which 45.9% reported depression in 2016, rising to 48.9% in 2018. Anxiety decreased from 52.8% to 48.9%, whereas stress increased from 56.7% to 59.7% over the same period. The most prevalent stressors were related to “lack of time” and “learning environment/academic performance.” SEM analyses revealed that follow-up depression was linked to the “learning environment/academic performance,” baseline depression, and “relationships”; follow-up anxiety was associated with “learning issues,” “health,” and baseline anxiety; and follow-up stress correlated with “learning environment/academic performance,” “learning issues,” “health,” and baseline stress.
Conclusions:
The high prevalence of mental health symptoms and the identification of specific stressors associated with these symptoms call for urgent action by medical schools. Interventions should focus on establishing psychological support programs, promoting a balance between academic and personal lives, and reducing the stigma surrounding mental health help-seeking.
Introduction
Mental health is a growing global concern. According to the Global Burden of Disease study, which covered 204 countries and territories, depression is the 13th leading cause of disability-adjusted life years (DALY) worldwide. The number of DALYs attributed to depression is projected to increase by 35.4% by 2050, making it a critical public health concern (GBD 2021 Forecasting Collaborators, 2024). In this context, the mental health of students in health-related fields, particularly those studying medicine, has become an increasing concern because of competitive and demanding academic environments. One systematic review (Rotenstein et al., 2016) found that approximately 27% of medical students worldwide exhibit depressive symptoms. Similarly, the prevalence of other mental health issues is also high among these students, with anxiety rates ranging from 7.7% to 65.5% and stress levels ranging from 12.2% to 96.7% (Hope & Henderson, 2014).
Therefore, identifying the factors contributing to mental health issues among students is essential for addressing their root causes. Major factors identified as detrimental to students’ mental well-being include academic pressures resulting from the need to meet high performance standards, excessive workloads, tight deadlines, and long study hours (Puthran et al., 2016). Additionally, financial concerns, family issues, and peer competition significantly affect emotional well-being, heightening daily stress (Zeng et al., 2019). The lack of time for leisure and self-care activities due to academic demands, also exacerbates psychiatric disorders (Damiano et al., 2020).
Further research is crucial to clarify the factors associated with mental disorders that directly impact the well-being of medical students. Longitudinal studies, rather than the commonly used cross-sectional designs, are needed to bridge this gap and identify epidemiological, curricular, and social factors influencing the mental health of medical students. Understanding these factors is essential for developing effective interventions and support strategies that promote healthy habits, enhance the quality of the learning environment, and positively impact medical training.
Thus, recognizing the need to re-evaluate medical education to not only help produce competent professionals but also mitigate its adverse effects on students’ mental health, this study aims to explore the various stressors medical students encounter during their training. It also examines the longitudinal associations between these stressors and mental health outcomes (depression, anxiety, and stress) using structural equation modeling (SEM).
Methods
Study Design and Period
This longitudinal, observational, and quantitative study involved medical students from a Brazilian public university. Data were collected in 2016 and 2018. The study was approved by the institution’s Research Ethics Committee (approval numbers 1.089.047/2015 and 2.742.787/2018), and all participants provided informed consent.
Setting
The study was carried in a medical school from a public university located in a middle-sized city of Brazil (550,000 inhabitants). This medical school has a predominantly traditional curriculum, which is combined with active learning strategies, such as team-based learning, flipped classroom, problem-based learning and jigsaw, among others. The medical training spans for 6 years and is divided into basic (first and second years), clinical (third and fourth years) and clerkship years (fifth and sixth years).
Participants and Inclusion and Exclusion Criteria
The study included all students regularly enrolled in the medical program in 2016 and 2018 and were present during the in-person data collection. These students completed both phases of data collection (baseline and follow-up) and agreed to participate in this study. Students on international exchange programs or internships in other municipalities were excluded. For the longitudinal follow-up, students who did not complete the questionnaire at both data collection points, such as those who joined the medical program after 2016 or graduated between the two collection periods, were excluded. Consequently, the final sample consisted of students enrolled in the first four years of the medical program in 2016.
Instruments
(a) Sociodemographic Data: Age (in years), sex (male, female), ethnicity (White, Black/Brown/Asian/Indigenous), family income (minimum wages, in Brazilian currency), marital status (single, married/separated/widowed), and year of medical program (1–4).
(b) Depression, anxiety, and stress scale – 21 items (DASS-21): This 21-item scale assesses and differentiates symptoms of depression, anxiety, and stress (Lovibond & Lovibond, 1995). Each subscale includes seven items rated on a five-point Likert scale, with higher scores indicating greater symptom severity. The scale has been translated into Portuguese and validated for use in Brazil (Vignola & Tucci, 2014).
(c) Medical Student Stress Factor Scale (MSSF): This 28-item scale identifies stressors experienced by medical students during their academic pursuits and is divided into 5 different domains: (1) “Learning Environment/Academic Performance” (12 items, e.g. “Excessive self-pressure for good grades,” “Lack of time to study”); (2) Relationships (5 items, e.g. “Family relationships,” “Faculty relationships”); (3) Health (4 items, e.g. “Physical health,” “Concern about my diet”); (4) Lack of time (3 items, e.g. “Lack of leisure time,” “Lack of time with friends and family”); and (5) Learning issues (4 items, e.g. “Difficulty understanding the content,” “Lack of motivation to learn”). Students assessed these stressors using a seven-point Likert scale to indicate the degree of stress caused by each situation. The total score reflects the students’ overall perceived stress levels, with higher scores indicating greater stress. This instrument was developed and validated in Brazil specifically for medical students (Damiano et al., 2020).
Procedures
Data were collected through self-administered questionnaires, ensuring voluntary participation and anonymity. Interviewers received training on how to approach students for participation and the techniques for administering the instruments. The questionnaires were administered at two distinct time points: initial collection in 2016 and follow-up in 2018. The questionnaires were administered during class sessions, with students placing their completed questionnaires in a collection box, avoiding weeks when they were engaged in summative assessments.
Statistical Analysis
Descriptive statistics included absolute and relative frequencies for categorical variables and means and standard deviations for continuous variables. Pearson correlation coefficients were calculated for mental health outcomes and stress factors, with significance set at p < .05.
Finally, causal models were estimated using SEM, a method that examines hypothetical interrelationships among latent constructs through factor and path analysis techniques (Violato & Hecker, 2007). We specified three theoretical models to assess the longitudinal impact of stressors on medical students’ depression, anxiety, and stress (see Figure 1). These models were based on a previous cross-sectional study carried out by our group (Damiano et al., 2020) showing that different types of medical school’s stressors could have important associations with mental health. These relationships were later supported by another Turkish study using the same MSSF instrument (Akova et al., 2025). Based on this evidence, we hypothesized that baseline mental health and stressors factors could have a longitudinal influence on the stressors factors, as well as aggravate depressive, anxiety and stress symptoms at follow-up. Identifying such predictors could have important educational implications to healthcare providers and educators. Overidentified models were then refined using fit indices, theoretical foundations, and statistical significance. Model adequacy was evaluated using the following benchmarks: Root Mean Square Error of Approximation (RMSEA) <0.08, Standardized Root Mean Square Residual (SRMR) <0.08, Comparative Fit Index (CFI) ⩾0.95, and Tucker–Lewis Index (TLI) ⩾0.95 (Kyndt & Onghena, 2014). All variables included in the SEM models used continuous scores.
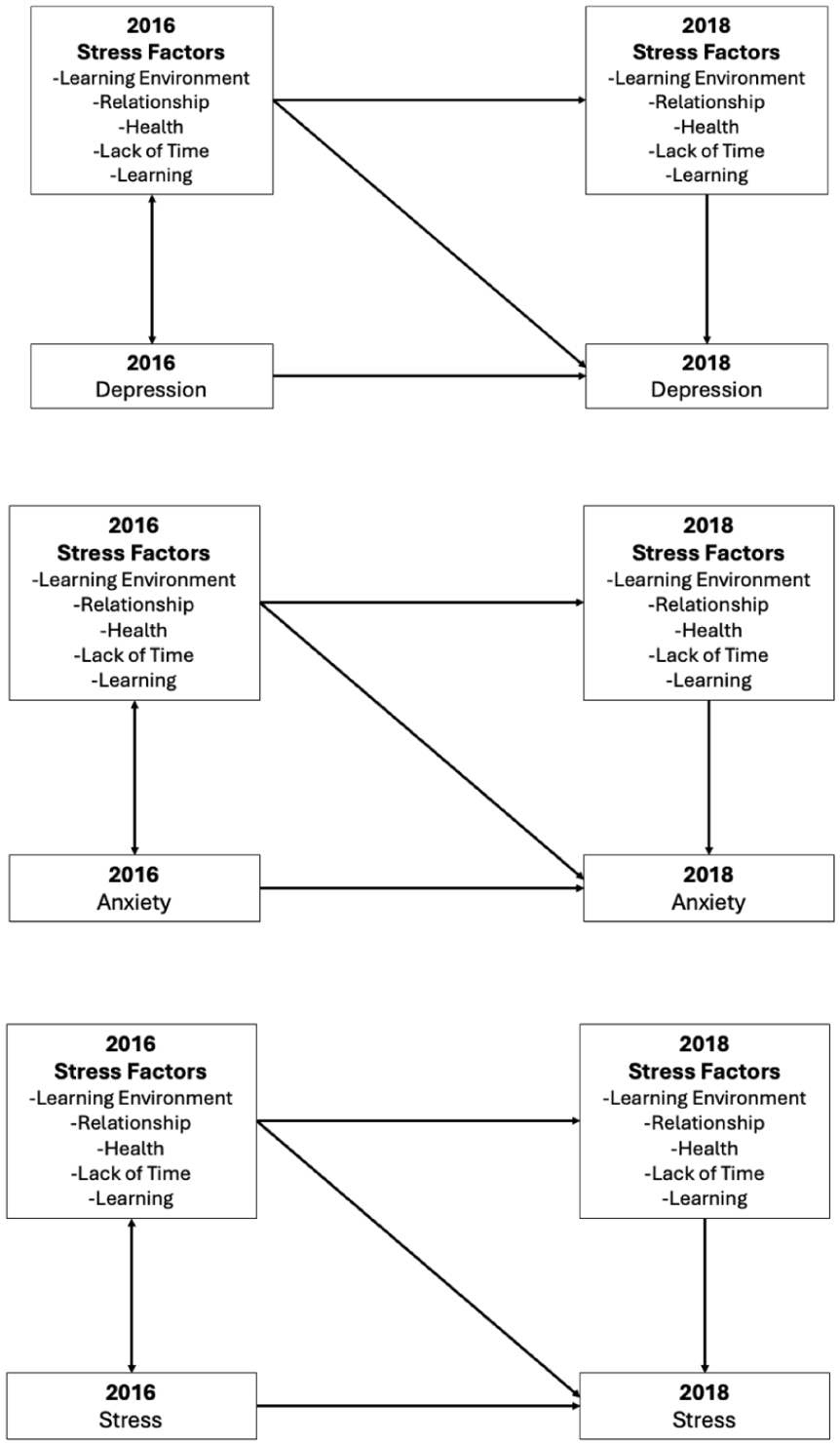
Theoretical models for the longitudinal influence of medical students’ stressors on depression, anxiety, and stress.
Results
A total of 231 medical students completed all questionnaires on stress factors and mental health at both time points (the response rate was 44% from the total population of students registered at the medical school and 46.3% from those who answered the baseline questionnaire). Participant’s sociodemographic characteristics, presented in Table 1, show that their average age was 20.4 years (SD 2.4), with 54.1% being females, 98.7% single, and 68.4% being White. They were distributed across the first to fourth years of study. The table comparing those who responded only the baseline and those who responded both timepoints is presented in the Supplementary Material. Non-respondents had significantly lower levels of stress and anxiety, while presented greater age and were from later years of medical training as compared to respondents.
Baseline Characteristics of Participants.
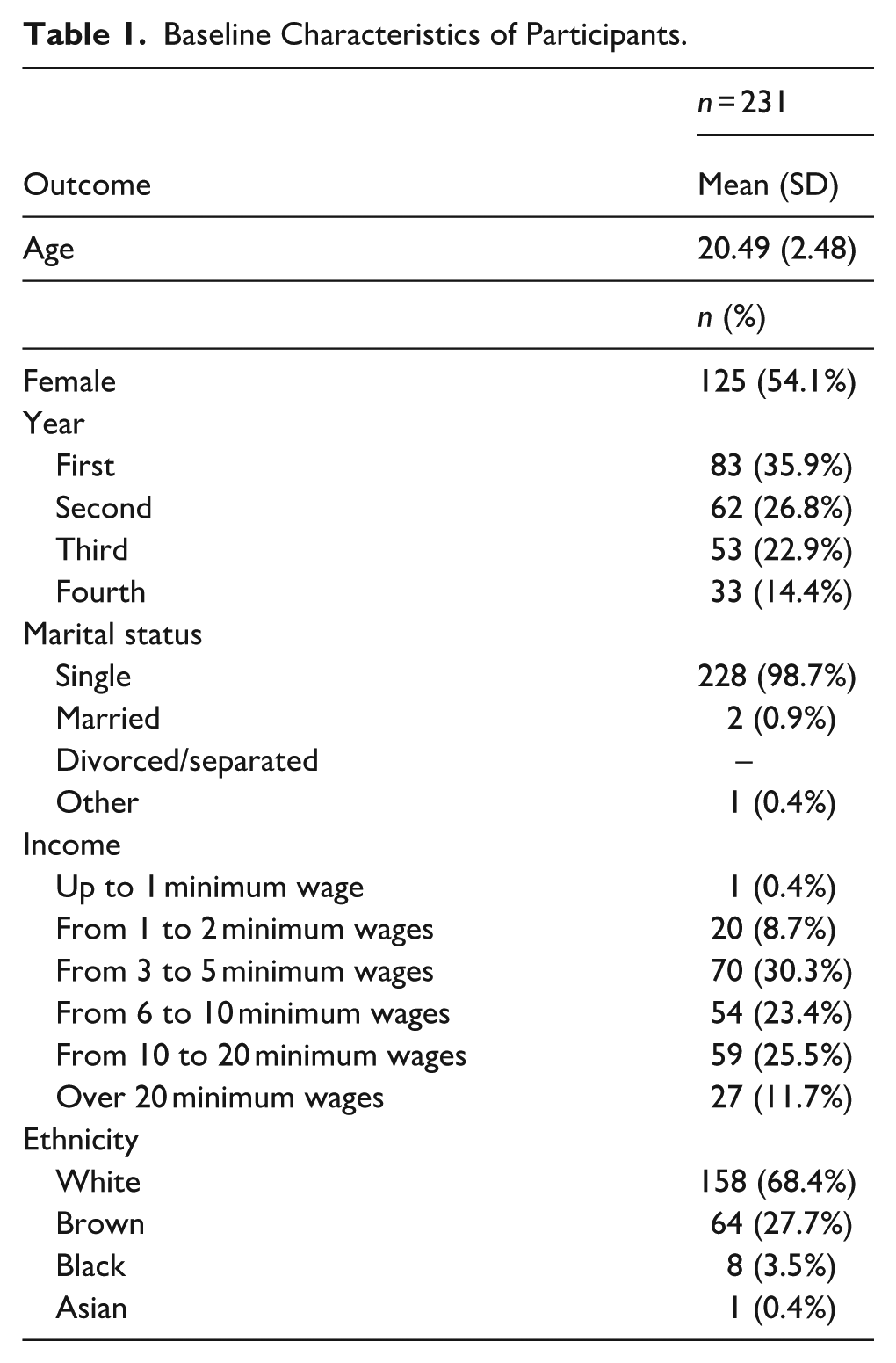
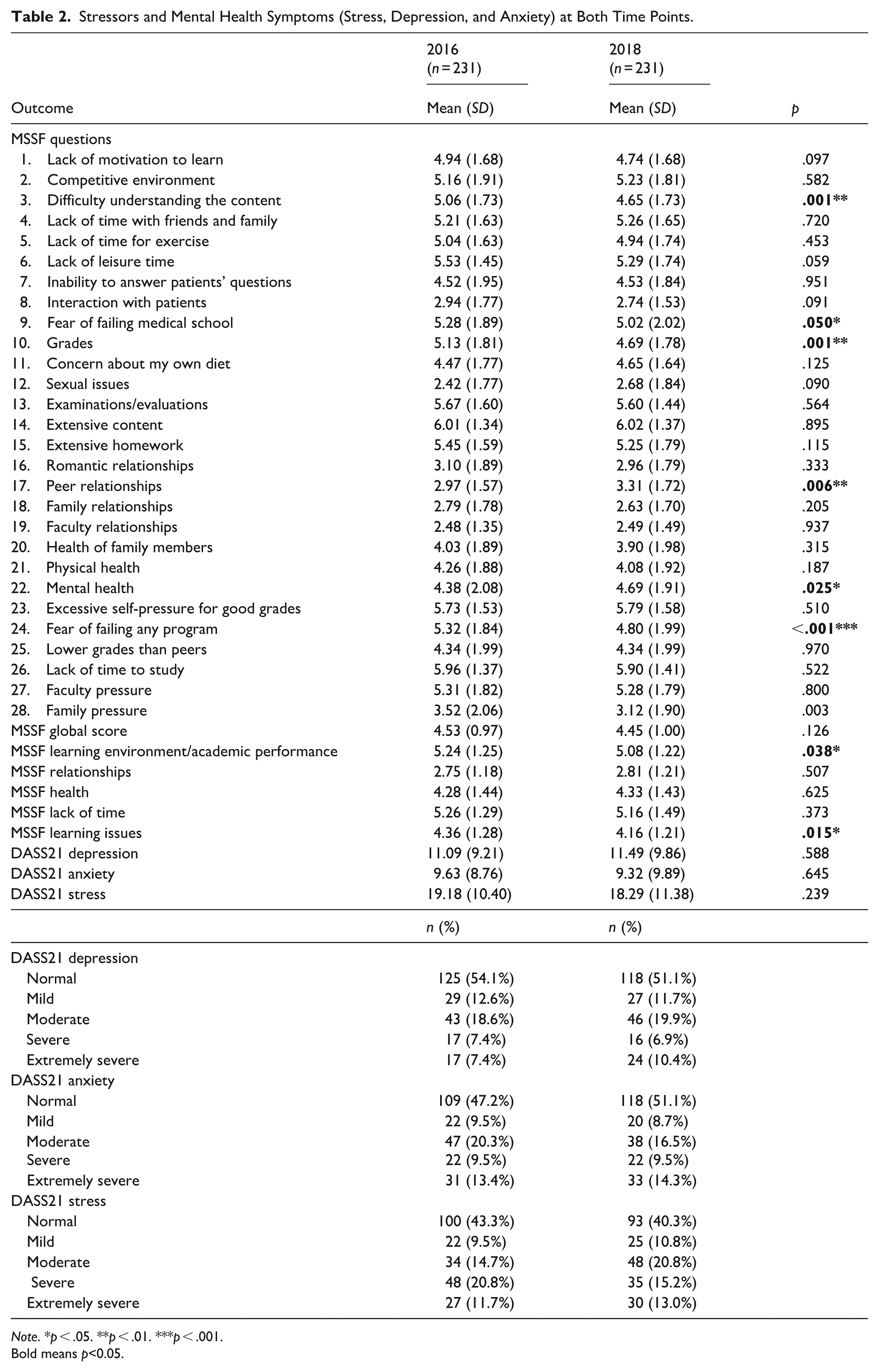
Table 2 presents stressors and mental health symptoms (stress, depression, and anxiety) at both time points. The prevalence of depression increased from 45.9% in 2016 to 48.9% in 2018. Anxiety was reported at 52.8% in 2016, decreasing to 48.9% in 2018, whereas stress levels increased from 56.7% to 59.7% during the same period. The primary stressors remained consistent across both time points and were ranked as follows: extensive content, lack of time to study, excessive self-pressure for high grades, and examinations or evaluations. The MSSF dimensions with the highest scores in both 2016 and 2018 were “lack of time,” “learning environment/academic performance,” “learning issues,” “health,” and “relationships.”
Stressors and Mental Health Symptoms (Stress, Depression, and Anxiety) at Both Time Points.
Note. *p < .05. **p < .01. ***p < .001.
Bold means p<0.05.
Although most stressors remained consistent after the 2-year follow-up, the scores for difficulty in understanding content, fear of failing medical school, grades, and fear of failing the course decreased. Conversely, mental health and peer relationship stress increased. Most MSSF dimension scores remained stable, except for “learning environment/academic performance” and “learning issues,” which showed a decline.
Table 3 Presents the correlation matrix for the mental health and stressor dimensions.
Correlation Matrix for Mental Health and Medical Students’ Stressors Dimensions.
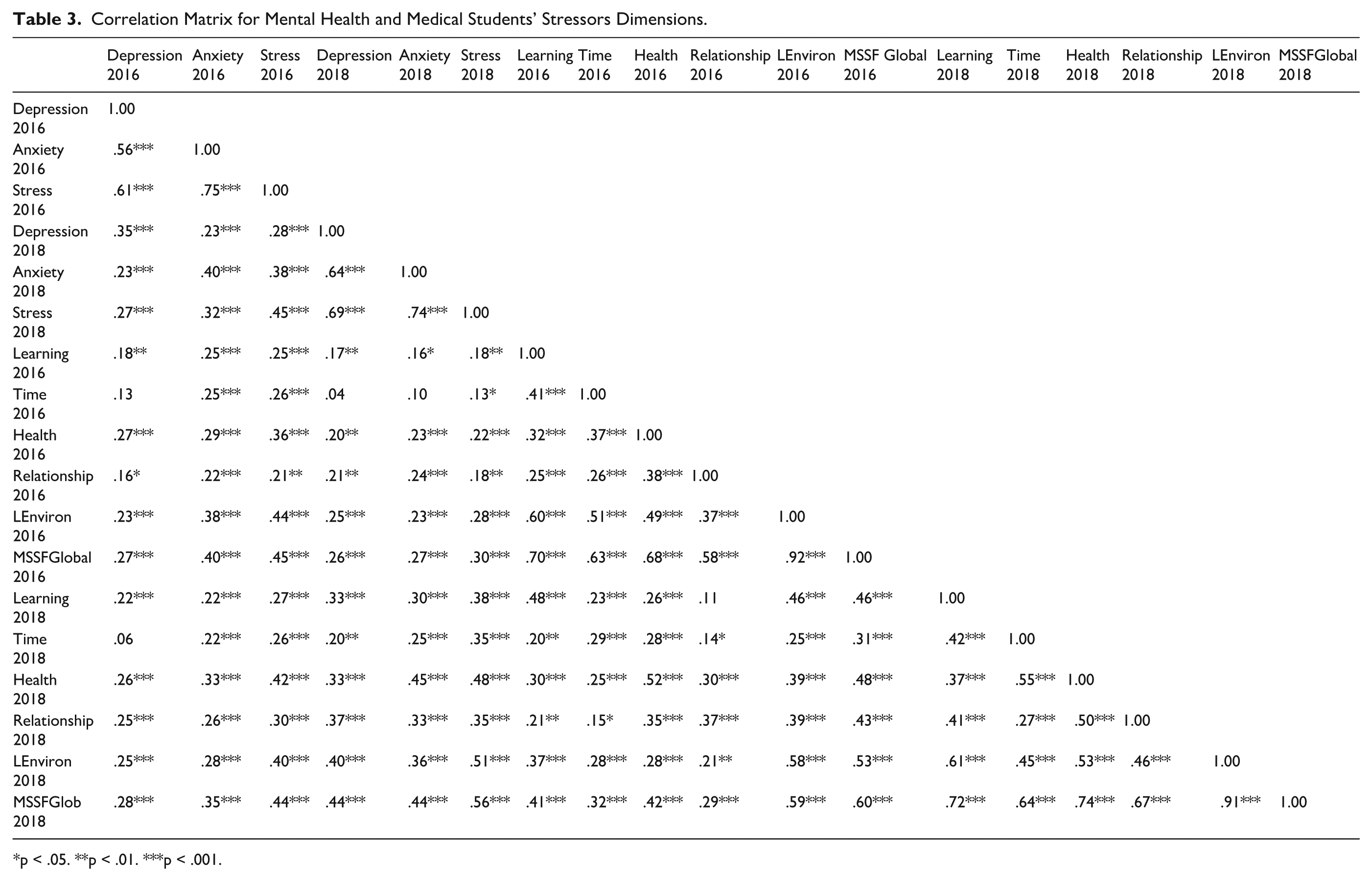
*p < .05. **p < .01. ***p < .001.
Three SEMs were developed to assess depression, anxiety, and stress at both time points (Figure 2a–c). All variables included in these models were treated as continuous scores as reported previously. First, the longitudinal SEM constructed for depression (Figure 2a) demonstrated a good fit (CFI = 0.998, TLI = 0.994, RMSEA = 0.021, and SRMR = 0.023). In this model, the baseline variables indicated that “learning environment/academic performance” in 2016 was associated with both “learning environment/academic performance” and “relationships” in 2018, depression in 2016 was associated with depression and “relationships” in 2018, and “relationships” in 2016 was associated with “relationships” in 2018. Regarding the follow-up variables, both “relationships” and “learning environment/academic performance” in 2018 were associated with depression in 2018. The model explained 23.3% of the variance in depression, 21.8% in relationship stress, and 32.5% in learning environment stress in 2018.
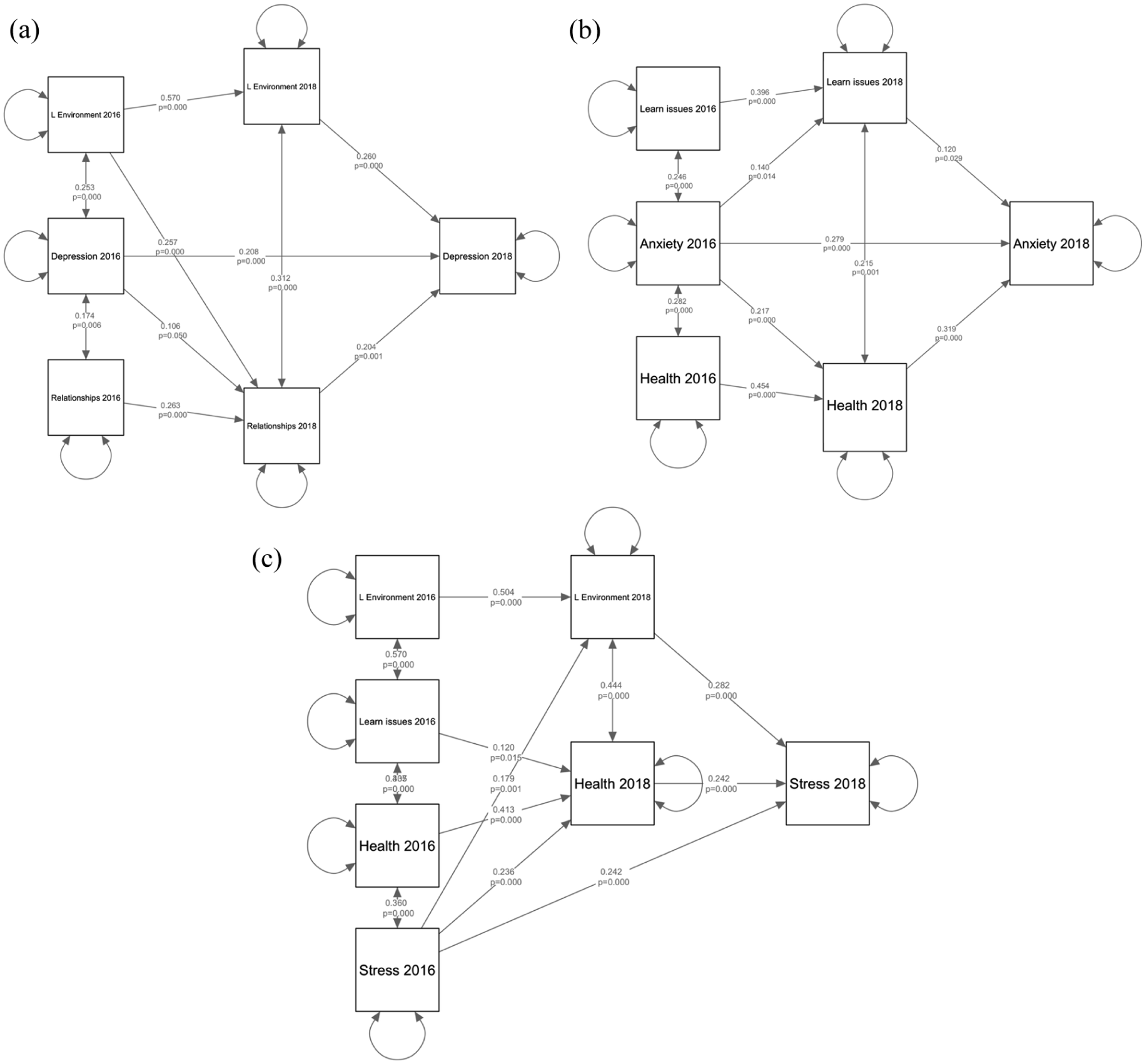
Structural equation models investigating the dynamic relationship between variables at both time points: (a) depression, (b) anxiety, and (c) stress.
Second, the longitudinal SEM for anxiety (Figure 2b) also demonstrated a good fit (CFI = 0.986, TLI = 0.948, RMSEA = 0.065, and SRMR = 0.035). Analyzing the baseline variables, “learning environment/academic performance” in 2016 was associated with “learning environment/academic performance” in 2018. Anxiety in 2016 was associated with anxiety in 2018, “health” in 2018, and “learning issues” in 2018. Additionally, “health” in 2016 was associated with “health” in 2018. Regarding the follow-up variables, both “learning issues” and “health” in 2018 were associated with anxiety in 2018. This model successfully explained 29.3% of the variance in anxiety, 30.9% in health stress, and 20.4% in learning issue stress in 2018.
Finally, the longitudinal SEM for stress (Figure 2c) also exhibited a good fit (CFI = 1.000, TLI = 1.005, RMSEA = 0.000, and SRMR = 0.020). Analyzing baseline variables, the “learning environment/academic performance” in 2016 was associated with the “learning environment/academic performance” in 2018, the “learning issues” in 2016 was associated with the “learning issues” in 2018, and stress in 2016 was associated with stress, “health,” and “learning environment/academic performance” in 2018. “Health” in 2016 predicted “health” in 2018. Regarding the follow-up variables, both “learning environment/academic performance” and “health” in 2018 were associated with stress in 2018. This model successfully explained 37.4% in stress, 35.6% in health stress, and 36.4% in learning environment stress in 2018.
Discussion
This study examined the complex longitudinal relationships between the various stress factors experienced by medical students and their mental health symptoms. Mental health symptoms were prevalent, with the most common stressors being “lack of time” and the “learning environment/academic performance.” Our SEM analyses indicated that the “learning environment/academic performance,” baseline depression, and “relationships” were associated with follow-up depression; “learning issues,” “health,” and baseline anxiety were associated with follow-up anxiety; and “learning environment/academic performance,” “learning issues,” “health,” and baseline stress were associated with follow-up stress. These findings can assist medical school administrators and educators in understanding the stress factors contributing to mental health problems and aid in developing prevention and intervention strategies to overcome these challenges.
Our findings revealed persistent mental health issues, with rates of depression increasing from 45.9% to 48.9%, anxiety decreasing from 52.8% to 48.9%, and stress increasing from 56.7% to 59.7% between 2016 and 2018. These results are higher than those of previous global systematic reviews (Hope & Henderson, 2014; Rotenstein et al., 2016) and other studies in which depression rates ranged from 20% to 40% (Matar Boumosleh & Jaalouk, 2017; Moutinho et al., 2019; Nyer et al., 2013). Additionally, mental health problems displayed a noticeable upward trend over time, which is consistent with previous Brazilian findings indicating worsening levels of anxiety, depression, and stress as students progress through medical school (Moutinho et al., 2017, 2019). The high prevalence observed at both data collection points underscores the critical need for educators to pay attention to these issues throughout students’ academic journeys.
The major stressors identified – extensive content, lack of time to study, excessive self-pressure for good grades, and examinations/evaluations – persisted across both time points. The MSSF scale identified “lack of time” and the “learning environment/academic performance” as the most significant stress factors. Although a range of factors can be considered as potential causes of impaired mental health among medical students, our data emphasize that conditions related to the curriculum and student learning are perceived as more stressful by students. Entering university can represent a new reality and requires routine adjustment, with a need for self-affirmation and professional development (Moutinho et al., 2017). In the specific case of medical schools, given the highly competitive and individualistic nature of the profession, many students gradually develop a tendency toward isolation as a means of self-protection against the intense competition inherent in academic and professional environments (Bert et al., 2020). Additionally, students may face academic and financial difficulties that increase their stress levels (Liu et al., 1997; Salam et al., 2013). Excessive content and examinations, which also impact time availability, have been highlighted in the literature as important factors affecting student well-being (Brown, 2015; Damiano et al., 2020; D’Eon, 2023). In this context, curriculum reform and better adaptation of teaching methods focusing on active learning methodologies can be important education tools.
The complex relationship between stressors and mental health was elucidated through SEMs, which enhanced our understanding of these findings. These models revealed that baseline depression symptoms predicted depression at follow-up. Similar trends were observed for anxiety and stress models. Although anticipated, as students with poor mental health are more likely to experience these issues (Castro Pecci Maddalena et al., 2025; Quince et al., 2012), this finding underscores the importance of early detection. Moreover, owing to the persistent nature of these conditions, identification and intervention may mitigate long-term mental health problems.
Regarding the various MSSF stressor dimensions, the learning environment – a detrimental aspect of student life, closely tied to their well-being (Damiano et al., 2019, 2020), encompassing factors such as excessive content, examinations/assessments, and competitiveness – was associated with follow-up depression and stress. Previous studies have indicated that an unfavorable learning environment can lead to poorer academic and mental health outcomes (Damiano et al., 2019) which aligns with our findings. Despite this evidence, medical schools often fail to address the issue of an overloaded curriculum (D’Eon, 2023) not focusing on reducing the burden of summative assessments and minimizing the competitive student culture.
Learning issues, including low motivation and difficulty understanding content, were significant predictors of follow-up anxiety and stress among medical students. These struggles can lead to frustration and adversely impact educational outcomes, resulting in decreased motivation. Motivation is a critical factor in medical education, and students with low motivation tend to have poorer outcomes, such as higher levels of mental health issues and lower academic performance (An & Li, 2021; da Silva Ezequiel et al., 2022). Medical schools should proactively identify underperforming students, investigate the causes of their learning difficulties, and address motivational issues, as these factors may be associated with struggles during follow-up. The literature suggests that interventions to boost motivation and address student challenges are important and should be implemented by medical educators (Hays et al., 2011).
Health issues were also identified as significant stressors related to anxiety and stress at follow-up. The literature indicates that students’ dietary habits, along with their physical and mental health, can significantly influence their overall well-being (AlJaber et al., 2019; McKerrow et al., 2020). Our study corroborates this finding by demonstrating that health problems can lead to distress during follow-up. Medical schools should ensure (or facilitate) access to healthcare for their students as health issues can persist and affect both medical training and future mental health.
Finally, stress factors in relationships (i.e. family, romantic, peer, and faculty relationships) were associated with follow-up depression. Many factors contribute to mental health issues among medical students, including personal matters, such as romantic and family relationships. Previous evidence indicates that social connection problems are strongly associated with depression in the general population (Badri et al., 2021; Sommerlad et al., 2022), which also appears to be true for medical students. However, relationships with peers and faculty members are also crucial in academic life. Previous studies have shown that bullying/hazing, violence, sexual discrimination, homophobia, racism, social discrimination, minority discrimination, and professional misconduct can have detrimental effects on medical students (Cook et al., 2014; Damiano et al., 2019), which aligns with our findings. Early identification of these negative relationships and implementation of educational and preventive interventions can reduce stress during medical training and prevent unprofessional behavior in the future (Lind et al., 2020).
This study has certain limitations. First, being a single-center study limits the generalizability of the findings. It is important to underscore that this study was carried out in a public medical school, which has characteristics that are different from Brazilian private schools. Public medical schools are funded by the government, have no tuition fee for all students and, a portion of their enrollment slots (quotas) are reserve for low-income students and/or those who studied in public high-schools. Therefore, external validity to other private institutions may be limited and should be made with caution. Second, participant loss occurred over the two-year follow-up period. Respondents were different concerning lower age, earlier stage of medical training and higher levels of anxiety and stress. Therefore, it seems that non-respondents probably were less interested in answering the questionnaire for having less mental health symptoms and for being at the end of the course. Third, although the questionnaires used were validated and widely employed in other studies, they relied on self-reporting, which does not provide a definitive diagnosis of mental health issues and may be influenced by social desirability bias. However, the longitudinal design of this study, which involved tracking a cohort of students over 2 years, allows for the exploration of causal relationships between the study variables. A strength of the present study is the fact that the SEM models presented a good percentage of their variance explained (ranging from 23.3% to 37.4%), showing a good model fit and reinforcing the possible clinical relevance and educational implications of our findings.
In conclusion, the high prevalence of mental health symptoms over time, along with the identification of specific stressors associated with these symptoms, highlights the urgent need for medical education institutions to adopt targeted policies and interventions to enhance students’ mental well-being. Implementing psychological support programs, promoting a balance between academic and personal life, and reducing the stigma surrounding help-seeking is essential to ensure that future physicians maintain both their physical and mental health.
Supplemental Material
sj-docx-1-isp-10.1177_00207640251384081 – Supplemental material for Longitudinal Relationship Between Medical Students’ Stressors and Mental Health Outcomes: A Structural Equation Modeling Analysis
Supplemental material, sj-docx-1-isp-10.1177_00207640251384081 for Longitudinal Relationship Between Medical Students’ Stressors and Mental Health Outcomes: A Structural Equation Modeling Analysis by Paula de Moura e Silva Toledo, Giancarlo Lucchetti, Sabrine Teixeira Ferraz Grunewald, Oscarina da Silva Ezequiel and Alessandra Lamas Granero Lucchetti in International Journal of Social Psychiatry
Footnotes
Acknowledgements
We thank the medical students who participated in this study
Ethical Considerations
The study was approved by the institution’s Research Ethics Committee (approval numbers 1.089.047/2015 and 2.742.787/2018)
Consent to Participate
All participants provided informed consent.
Author Contributions
Paula de Moura e Silva Toledo: Writing – original draft, Methodology, Conceptualization.
Giancarlo Lucchetti: Writing – original draft, Methodology, Formal analysis, Conceptualization.
Sabrine Teixeira Ferraz Grunewald: Writing – original draft,
Oscarina da Silva Ezequiel: Writing – review & editing, Methodology, Conceptualization.
Alessandra Lamas Granero Lucchetti: Writing – review & editing, Data curation, Methodology, Formal analysis, Conceptualization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author under reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.