
Abstract
Background:
Parenting plays a critical role not only in supporting children’s healthy growth and development but also in contributing to a meaningful and fulfilling life.
Aims:
This study evaluates how parents’ self-compassion levels, which significantly influence their well-being, affect their parenting styles.
Methods:
The research was conducted using a cross-sectional and descriptive design. Data were collected through an online form between April and October 2024, using a general information form, the Self-Compassion Scale, and the Multidimensional Parenting Styles Scale. Data analyses were performed using SPSS 25.0. Descriptive statistics, including mean, standard deviation, minimum/maximum values, frequency, and percentage, were used to summarize the findings.
Results:
The effect of parents’ self-compassion levels on parenting styles was analyzed using one-way analysis of variance (ANOVA). The results indicate that most parents exhibit high levels of self-compassion and positive parenting behaviors. Additionally, as self-compassion levels decrease, negative parenting behaviors tend to increase.
Conclusion:
These findings suggest that self-compassion is a key factor in the parenting process, and supporting parents’ self-compassion levels may contribute to developing more positive parenting behaviors. Therefore, it is recommended that psychosocial support and awareness programs be developed to enhance parents’ self-compassion levels.
Background
Parenting is a multidimensional and dynamic process that significantly affects children’s development and well-being. The attitudes and behaviors exhibited by parents during this process play a crucial role in shaping children’s emotional, social, and cognitive development (Żmuda, 2024). Parents’ attitudes toward their children and their attitudes toward themselves are critically important in the parenting process. In this context, self-compassion is essential to healthy and balanced parenting. Self-compassion refers to parents’ ability to develop a compassionate, understanding, and supportive attitude toward themselves (Neff & McGehee, 2010). A self-compassionate approach enables parents to be more patient, empathetic, and understanding toward their children. Moreover, it strengthens the parent-child relationship and significantly contributes to children’s well-being (Moreira et al., 2015; Stenz et al., 2023; Żmuda, 2024). Since self-compassion is also learned through modeling, the importance of parental attitudes becomes even more apparent (Bayar & Dost, 2018; Neff & McGehee, 2010). Furthermore, parents’ self-compassion levels can influence their parenting styles and the quality of their interactions with their children (Liang et al., 2024; Moreira et al., 2015; Stenz et al., 2023). Therefore, understanding the impact of parents’ self-compassion on parenting styles is a crucial area of research.
Parenting styles encompass parents’ overall attitudes toward their children, significantly influencing children’s emotional, social, and cognitive development (Avdiu & Hyseni Duraku, 2024; Baumrind, 2012; Kuppens & Ceulemans, 2019). These attitudes reflect parental behaviors aimed at creating an emotionally meaningful environment for their children (Avdiu & Hyseni Duraku, 2024; Kuppens & Ceulemans, 2019). The development of healthy and positive parenting approaches not only fosters a peaceful family environment but also supports children’s socialization and peer relationships (Kol, 2016; Li et al., 2025). Additionally, parenting styles play a vital role in raising physically and psychologically healthy individuals with high self-confidence. Independent, self-reliant, and responsible individuals often emerge from positive parenting practices (Tripathi & Pandey, 2018).
Children shape the future of societies, and their well-being is closely tied to how they are raised. Parents, serving as caregivers and role models, play a decisive role in this process. Their well-being directly influences their parenting attitudes. Given this, evaluating the relationship between parents’ self-compassion and parenting styles is very important. However, a direct examination of this relationship remains largely unexplored in the existing literature. Therefore, this study aimed (1) to describe the levels of self-compassion and parenting styles among parents, and (2) to examine the relationship between parents’ self-compassion levels and their parenting styles. It is expected that the findings of this study will contribute significantly to interventions aimed at enhancing parental psychological resilience, promoting more positive parenting practices, and supporting children’s health and well-being.
In this context, the research questions are as follows:
Are there significant differences in parenting styles depending on parents’ self-compassion levels?
Materials and Methods
Study Design
This study was conducted using a cross-sectional and descriptive design to evaluate the relationship between parents’ self-compassion levels and their parenting styles.
Study Population and Sample
The required sample size was determined a priori using G*Power 3.1.9.7 for a one-way analysis of variance (ANOVA). Assuming a small effect size (Cohen’s f = 0.10), a significance level of α = .05, a desired power of 1 − β = .90, and three groups (low, medium, and high self-compassion), the minimum required sample size was calculated as 252 participants. Participants were recruited through a Non-probability sampling snowball sampling approach, whereby initial respondents were invited to refer other eligible parents. To compensate for potential data loss and to maintain sufficient statistical power, all parents who consented to participate were included, resulting in a final sample of 385 participants (Chatzi & Doody, 2023).
Study Setting and Duration
The study was conducted between April and October 2024 using an online survey. Participants were recruited through the non-probability snowball sampling method.
Data Collection Instruments
The study data were collected using the General Information Form, the Self-Compassion Scale (SCS), and the Multidimensional Assessment of Parenting Scale (MAPS). The General Information Form was developed to assess participants’ sociodemographic characteristics, including age, gender, education level, occupation, and income level.
The Self-Compassion Scale (SCS); developed by Neff (2003) and adapted into Turkish by Akın et al. (2007), consists of 26 items on a 5-point Likert scale and includes six subdimensions: self-kindness, self-judgment, common humanity, isolation, over-identification, and mindfulness. Higher scores in each subscale indicate a more substantial presence of the corresponding trait. Negative subscales (self-judgment, isolation, and over-identification) are reverse-scored, and the total self-compassion score is calculated as the mean of the six subscale scores. Based on the total score, self-compassion levels are classified as low (1.0–2.49), moderate (2.5–3.49), or high (3.5–5.0). The internal consistency reliability (Cronbach’s α) of the scale ranged from .72 to .80, and the test-retest reliability coefficients were found to be between .56 and .69 (Akın et al., 2007). The Cronbach’s α value for the Self-Compassion Scale (SCS) was .779.
The Multidimensional Assessment of Parenting Scale (MAPS); developed by Parent and Forehand (2017) and adapted into Turkish by Karababa (2019), consists of 34 items across seven subdimensions: proactive parenting, positive reinforcement, close relationship, supportive approach, hostility, low control, and physical control. The scale allows for calculating two composite scores: comprehensive positive parenting, which includes proactive parenting, positive reinforcement, close relationship, and supportive approach subscales, and comprehensive negative parenting, which includes hostility, low control, and physical control subscales. The scale is structured using a 5-point Likert rating system (1 = Never, 5 = Always) and includes no reverse-scored items. The possible score ranges are 16 to 80 for comprehensive positive parenting and 18 to 90 for comprehensive negative parenting. The Cronbach’s α reliability coefficients were reported as .80 for proactive parenting, .83 for positive reinforcement, .83 for close relationship, .77 for supportive approach, .85 for hostility, .85 for low control, and .91 for physical control. The overall reliability was .90 for comprehensive positive parenting and .88 for comprehensive negative parenting (Karababa, 2019). The Cronbach’s α value for the Multidimensional Assessment of Parenting Scale (MAPS) was .763.
Data Analysis
Statistical analyses were conducted using SPSS 25.0. Descriptive statistics for continuous variables were presented as mean, standard deviation, minimum, and maximum values, while categorical variables were reported as frequency and percentage. Given the large sample size (n = 385), normality was evaluated using skewness, kurtosis, and Q–Q plots, as the Shapiro–Wilk and Kolmogorov–Smirnov tests were overly sensitive. The data were found to be approximately normally distributed, supporting the use of parametric tests. The internal consistency of the scales was evaluated using Cronbach’s α. The effect of parents’ self-compassion on parenting styles was examined through one-way ANOVA and ANCOVA, with the significance level set at p < .05.
Ethical Considerations
Prior to the study, ethical approval was obtained from the Ethics Committee for Social and Human Sciences Research of a State University (Approval Date: May 26, 2023, Approval Number: 2023-516). Permission for the use of the measurement scales was obtained via email correspondence. Informed consent was obtained from all participants in accordance with the principles of autonomy, voluntary participation, and confidentiality. Participants were fully informed about the study before providing their consent. All procedures followed the principles of the Declaration of Helsinki.
Results
The participants had a mean age of 41.2 ± 7.72 years, with 80.5% being female and 93.8% being married. Regarding educational background, 64.2% held a university degree, while 57.7% were employed as civil servants. Additionally, 56.1% reported that their income was equal to their expenses. Participants with two children comprised 50% of the sample (Table 1).
Participant Features.
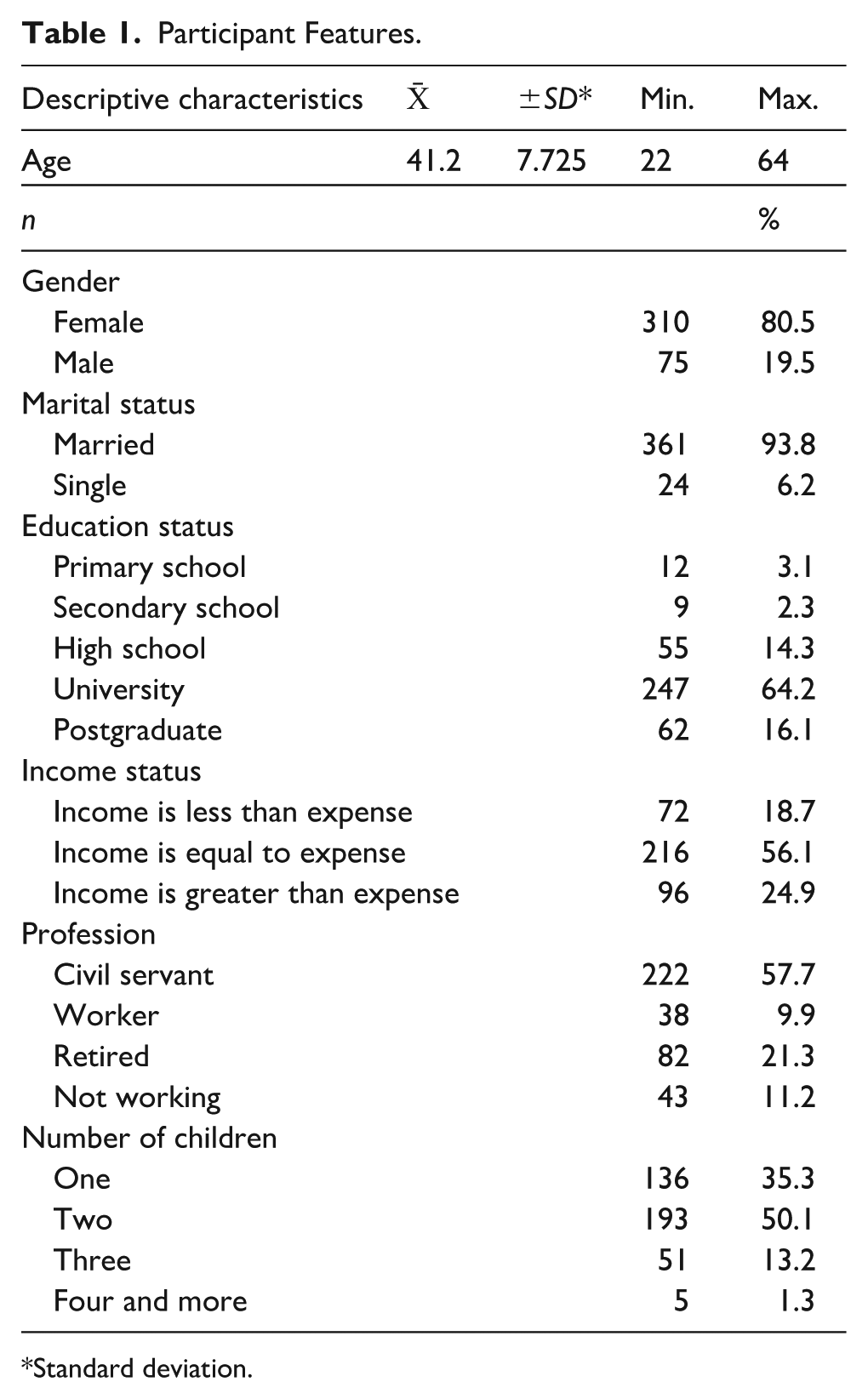
Standard deviation.
The total and subscale scores of the scales were assessed for normality using skewness–kurtosis values and Q–Q plot analyses. Since all skewness and kurtosis values ranged between −2.5 and +2.5, and the points on the Q–Q plots closely followed the diagonal line, the data were considered to be normally distributed.
The scoring of the Self-Compassion Scale (SCS) was conducted in accordance with the guidelines provided in the scale description. The mean total score from the scale was calculated as M = 3.43. Based on this mean score, the scale scores were converted into categorical data. As a result, 49.6% of the participants were classified as having high self-compassion, while 39.5% exhibited moderate self-compassion (Table 2).
Self-Compassion Scale (SCS) Mean and Frequency Values.
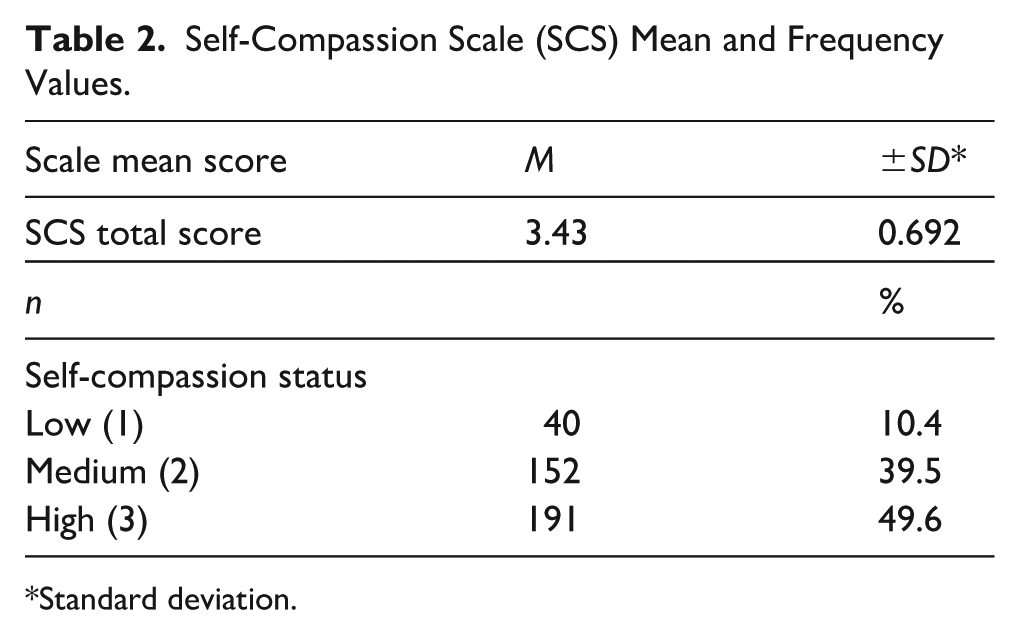
Standard deviation.
The Multidimensional Assessment of Parenting Scale (MAPS) scoring was conducted according to the guidelines provided in the scale description. Two types of scores were obtained: positive parenting attitudes and negative parenting attitudes. The mean total score for positive parenting attitudes was calculated as 68.67 ± 6.99 (min = 18, max = 80), while the mean total score for negative parenting attitudes was 35.00 ± 9.418 (min = 18, max = 87; Table 3).
Multidimensional Assessment of Parenting Scale (MAPS) Total Score and Frequency Values.
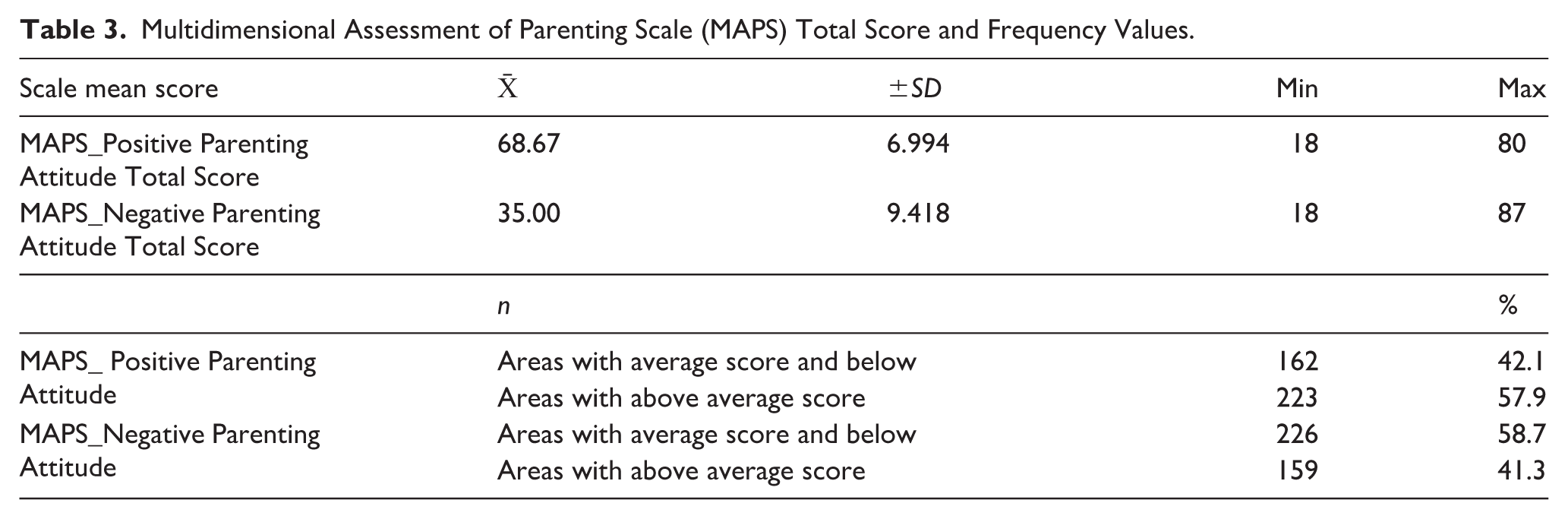
A frequency analysis was conducted based on the MAPS scoring, categorizing participants into those scoring below, at, or above the mean for positive and negative parenting attitudes. The results showed that 57.9% of the participants scored above the mean for positive parenting attitudes, while 41.3% scored above the mean for negative parenting attitudes (Table 3).
The evaluation of positive and negative parenting attitudes based on self compassion levels (1 = low, 2 = medium, and 3 = high) was conducted using one way analysis of variance (ANOVA). The results indicated that self compassion levels did not show a statistically significant difference in positive parenting attitudes (p > .05); however a statistically significant difference was found in negative parenting attitudes (p < .05; Table 4).
Comparison of Positive and Negative Parenting Attitudes According to Self-Compassion Variable (ANOVA).
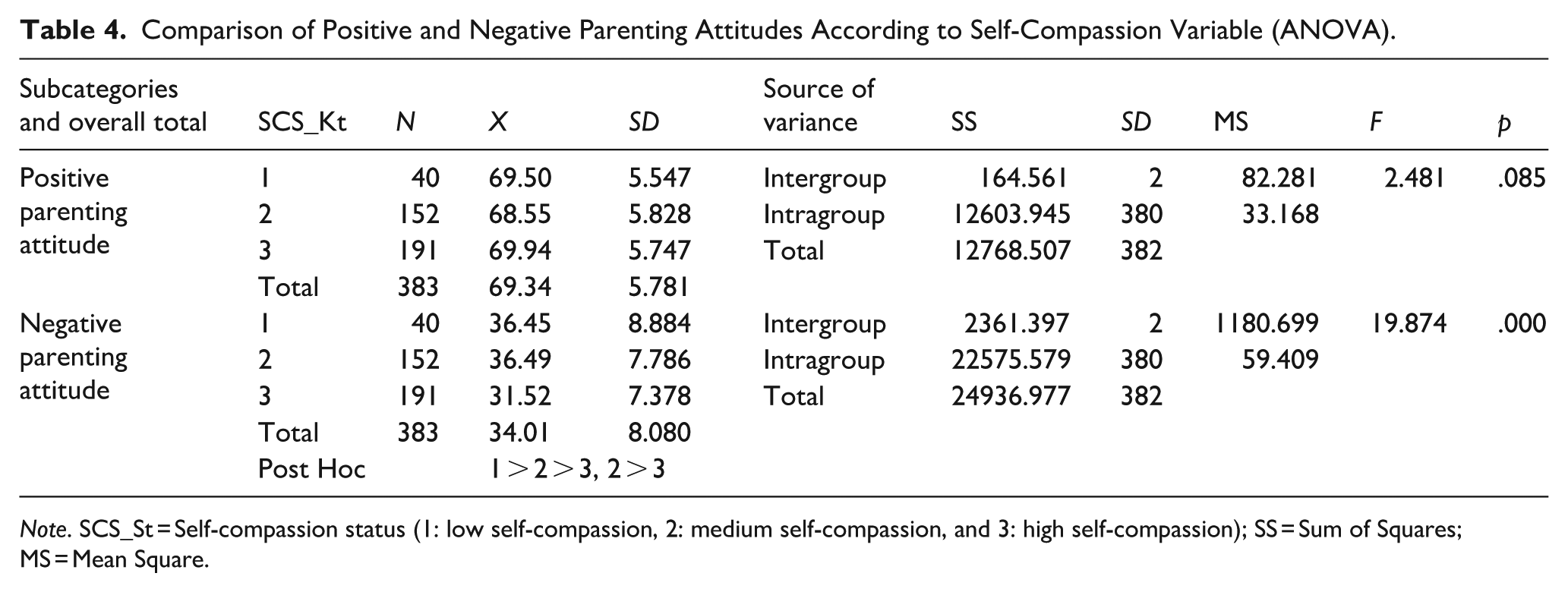
Note. SCS_St = Self-compassion status (1: low self-compassion, 2: medium self-compassion, and 3: high self-compassion); SS = Sum of Squares; MS = Mean Square.
To identify the origin of this difference, a post hoc LSD test was conducted. Post-hoc analyses revealed that participants with low (M = 36.45) and medium (M = 36.49) self-compassion scored significantly higher on negative parenting than those with high self-compassion (M = 31.52), indicating that higher self-compassion was associated with lower negative parenting attitudes (1, 2, and >3; Table 4). However, when the effects of covariates such as age, gender, education level, income status, occupation, marital status, and number of children were controlled for in an ANCOVA, the previously significant difference became non-significant (p > .05). This finding suggests that the observed differences in negative parenting attitudes across self-compassion levels may be attributable more to demographic factors than to self-compassion itself.
Discussion
Parenting plays a critical role not only in supporting children’s healthy growth and development but also in contributing to a meaningful and fulfilling life. In this context, parents’ well-being emerges as a significant factor. This study examined the relationship between self-compassion—which has been shown to have a decisive impact on individual well-being and can be enhanced through various intervention programs—and parenting attitudes.
According to the study, most parents exhibited high self-compassion and positive parenting attitudes. Similarly, Smane and Svence (2021) reported that parents with higher self-compassion levels were more inclined to create a supportive environment for their children and were more likely to adopt positive parenting practices. In line with this, Patsakos (2024) found that higher self-compassion levels were associated with lower stress and depression levels, particularly among parents of children with disabilities. Self-compassion enhances parents’ psychological resilience against psychological challenges such as self-criticism and isolation (Patsakos, 2024). Furthermore, Hendry et al. (2022) identified a negative correlation between self-compassion levels and parenting stress, demonstrating that parents with higher self-compassion experienced less stress, regardless of their children’s psychological conditions. Similarly, Gois et al. (2023) emphasized that self-compassion was a buffer against negative emotions during stressful periods, such as the COVID-19 pandemic. Their study revealed that parents with higher self-compassion levels managed parenting-related guilt and anxiety more effectively. Żmuda (2024) also highlighted the positive impact of self-compassion on parenting quality, reporting that parents with higher self-compassion showed improvements in self-regulation and coping skills. Additionally, Nguyen et al. (2023) emphasized that self-compassion reduced parental burnout and promoted positive parenting practices. In a similar vein, Cheung et al. (2022) reported a negative correlation between self-compassion and depressive symptoms, suggesting that as self-compassion increased, overall well-being improved. Moreover, parents with higher self-compassion levels were found to use emotion regulation strategies more effectively, displaying greater tolerance, warmth, and understanding toward their children (Avdiu & Hyseni Duraku, 2024; Li et al., 2025). They were also more attuned to their children’s needs and developed appropriate responses to meet these needs (Avdiu & Hyseni Duraku 2024; Fernandes et al., 2022; Gois et al., 2023; Hong et al., 2022; Smane & Svence, 2021). These findings suggest that higher levels of self-compassion and positive parenting behaviors among parents may be related to their educational background. Parents with higher education levels are likely to have a stronger sense of self-actualization and greater life satisfaction, which may explain their higher self-compassion levels and more positive parenting practices.
The study found that as self-compassion levels decreased, negative parenting attitudes increased. However, when demographic factors such as age, gender, education, income, occupation, marital status, and number of children were controlled in an ANCOVA, the previously significant differences in negative parenting attitudes became non-significant, suggesting that these demographic variables may account for part of the observed relationship.Consistent with previous research, Hendry et al. (2022) reported a negative correlation between self-compassion and parenting stress, indicating that parents with lower self-compassion levels experienced higher stress, which may contribute to negative parenting attitudes. Cheung et al. (2022) found that parents with lower self-compassion levels exhibited more depressive symptoms, potentially impairing parent-child interactions. Similarly, Doo and Kim (2022) observed that decreased self-compassion in parents was associated with a greater likelihood of developing negative parenting attitudes that may prevent children from experiencing a safe and supportive environment. Moreover, Tekin and Kayılı (2023) highlighted that negative parenting attitudes undermine children’s emotional regulation, as harsh and intolerant behaviors can lead to anger control issues and aggression. Similarly, Narvaez et al. (2024) reported that negative parenting attitudes increase the likelihood of substance use among children, emphasizing the long-term behavioral consequences of harsh and neglectful parenting. Conversely, Psychogiou et al. (2016) found that parents with higher self-compassion were less critical and reacted more calmly in parenting situations. Taken together with the current findings, it can be inferred that although self-compassion is associated with negative parenting attitudes, this relationship may be influenced by demographic factors. Parents with lower self-compassion levels may adopt harsher and less tolerant attitudes toward their children, but part of this tendency could be explained by characteristics such as age, gender, or family composition. Therefore, interventions aiming to improve parenting practices may benefit from addressing both parental self-compassion and broader demographic or contextual factors.
Conclusion and Recommendations
This study’s findings indicate that most parents exhibit high levels of self-compassion and positive parenting attitudes. Additionally, as self-compassion levels decrease, negative parenting attitudes increase. However, when sociodemographic variables were controlled for using ANCOVA, this relationship became statistically non-significant. These results suggest that while self-compassion may influence parenting attitudes, its effect can be moderated by sociodemographic factors.
This study highlights the role of self-compassion in parenting processes and provides a foundation for future research. Further investigation of individual, cultural, and socioeconomic factors influencing parents’ self-compassion is warranted. Longitudinal studies with larger samples are recommended to clarify causal relationships between self-compassion and parenting attitudes. Additionally, universal preventive interventions, such as psychoeducational programs delivered by healthcare professionals, may enhance awareness of self-compassion and promote supportive parenting practices.
Footnotes
Acknowledgements
The authors express their gratitude to all participants for their kind acceptance in this study.
Ethical Considerations
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation (Decision No 2023-516, Date 26.05.2023) and with the Helsinki Declaration of 1975, as revised in 2008.
Author Contributions
Conceptualization: S.S. and M.K.Y. Data curation: S.S. and M.K.Y. Formal analysis: S.S. Investigation: S.S. and M.K.Y. Methodology: S.S. and M.K.Y. Project administration: S.S. and M.K.Y. Resources: S.S. Software: S.S. Supervision: S.S. and M.K.Y. Validation: S.S. Visualization: S.S. and M.K.Y. Roles/Writing—original draft: S.S. and M.K.Y. Writing—review and editing: S.S. and M.K.Y.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.