
Abstract
Background:
One of the sections of the International Classification of Diseases 11th Revision (ICD-11), which focuses on the diagnosis of personality disorder (PD), has received great support from the scientific community for dimensionally focusing on its functioning instead of categories of low validity and utility for daily clinical practice.
Aims:
The goal of this paper is to provide a positive framework to complement the personality spectrum, and thus, with a comprehensive approach, strengthen the usefulness of the ICD-11-PD model.
Methods:
This is a narrative review focused on primary literature identified through searches conducted in PubMed and Web of Science in April 2024. The keywords used were “personality disorder,” “dimensional models of personality disorders,” and “ICD-11 personality disorders.” Given the nature of the review, we included studies employing diverse diagnostic criteria for personality disorders, as well as those based on the new ICD-11 definition.
Results:
Despite the promising benefits of this new model, preliminary evidence has highlighted several shortcomings, including low discriminant validity, weak latent structures, and a lack of clarity in distinguishing between PD and normal personality. From this perspective, complementary positive framework is proposed, which designates happiness and social well-being as determinants of the clinical importance of personality functioning in the new ICD-11-PD model.
Conclusion:
With this integrative model, such deficiencies could be better addressed by providing a personalized and empowering assessment and intervention approach that can obtain cost-effective results in primary and specialized care.
Introduction
Personality disorder (PD) is one of the most common mental health conditions, with prevalence rates ranging from 7.8% in community samples (Winsper, 2021) to 12.16% in the general population (Volkert et al., 2018). Although there are effective interventions for PD, they have a long duration; for example, for borderline personality disorder (BPD; Tyrer & Mulder, 2022a). Moreover, the diagnosis of PD usually has shortcomings when they are already applied in routine clinical practice because of widespread prejudices causing demoralization and feelings of helplessness among doctors, patients, and their families (Herpertz et al., 2022). In the International Classification of Diseases 11th Revision (ICD-11), PD follows a dimensional model mainly diagnosed by its severity in five levels (normal, difficult, mild, moderate, and severe), of which the last three constitute the clinical threshold. This dimensional model can help improve clinical utility; however, its conceptual foundations seem incomplete, since evaluation and treatment, focused on the patient’s problem, do not necessarily imply an increase in well-being, and vice versa (Greenspoon & Saklofske, 2001).
This approach in evaluation and diagnosis, which is promoted by actual nosological systems, possibly initiates stigmatization through a vicious circle transmitted to the entire community and social actors. To address these limitations, some researchers (de la Iglesia & Castro Solano, 2018) proposed the Positive Personality Model (PPM). In their study, it was found that positive traits are positively and moderately related (which denotes closeness, but not equality) to the traits of the normal range of the five-factor model (FFM). Furthermore, that positive traits negatively associated with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) maladaptive trait domains. In other words, positive traits have been shown to have a greater ability to predict positive mental health than FFM traits (de la Iglesia & Castro Solano, 2018) and adequately predict therapeutic progress (Eidman & de la Iglesia, 2021).
Another study, considering the bipolar continuum between health and illness, found that the positive traits of serenity, moderation, sprightliness, and integrity occurred more frequently in people with complete mental health than in those with problems, vulnerability, or ambivalence (de la Iglesia & Castro Solano, 2019). In this sense, the goal of this paper is to provide a positive framework to complement the personality spectrum, and thus, with a comprehensive approach, strengthen the usefulness of the ICD-11-PD model. With this in mind, (a) this model and its limitations are analyzed; additionally, (b) the positive perspective of personality is described and a guideline is proposed to incorporate the positive framework in the ICD-11-PD model. Finally, the implications of this integrative personality model for the evaluation, treatment, and clinical management provided by healthcare providers are discussed.
Methods
This is a narrative review focused on primary literature identified through searches conducted in PubMed and Web of Science in April 2024. The keywords used were “personality disorder,” “dimensional models of personality disorders,” and “ICD-11 personality disorders.” Given the nature of the review, we included studies employing diverse diagnostic criteria for personality disorders, as well as those based on the new ICD-11 definition. These articles were complemented with reviews and book chapters, with an emphasis on replicated findings.
Records identified in PubMed and Web of Science were merged into a single database, and duplicates were removed using a combined automated procedure followed by manual verification, comparing titles, authors, year of publication, and DOI. In cases of discrepancies, the most complete version of the record was retained. All members of the research team contributed to the literature review. The search yielded 114 records in Web of Science and 98 in PubMed, while manual searching identified 16 book chapters and 6 reviews.
The sole inclusion criterion was that the texts detailed at least one maladaptive and/or adaptive aspect of personality. These texts were operationalized through a two-phase process. First, an initial screening of titles and abstracts was conducted to identify potentially relevant studies based on the explicit presence of personality constructs (both adaptive and maladaptive). Subsequently, the preselected articles were assessed in full text to confirm that they substantively addressed these aspects of personality, excluding those that mentioned them only tangentially or did not develop them analytically. Documents providing exclusively categorical descriptions of personality disorders were excluded. The quality of the included texts was not assessed, as this is a narrative review (Pae, 2015). The included documents are cited in the Results section and discussed in the Discussion section.
Results
The Promising Utility of the ICD-11-PD Model, But What’s Missing?
PD is a common condition (Somma et al., 2022), that affects 7.8% of the world’s population (Winsper et al., 2020); prevalence that can extend up to 12.16% in Western countries (Volkert et al., 2018). The ICD-11-PD model is primarily dimensional, focusing on severity, and largely replicates the Alternative DSM-5 Model for PDs (AMPD) framework with three guidelines: (a) identification of the presence of PD, (b) assigning a degree of severity (normal, difficulty, mild, moderate, or severe) in self and interpersonal (dys)functioning, (c) and optionally, rating the prominence of maladaptive traits —continuous with normal traits— and the borderline pattern (World Health Organization [WHO], 2022). Certainly, categorical evaluations facilitate referral decision-making, as well as help establish the intensity and duration of treatment (Bachet al., 2021) and dimensional assessments help identify underlying symptomatology, thus refining treatment; thus, a gradual approach of dimensional expansion within the diagnostic category is more appropriate (Gaebel et al., 2020).
However, the approach to PD from the ICD-11 mentioned above seems incomplete, as the positive spectrum of personality has not been considered (de la Iglesia & Castro Solano, 2018). This situation increases the practical limitations of evaluation and intervention, and reduces the scope and effectiveness of public health policies. For example, adherence to treatment and patient rehabilitation would be hindered. That is, the person upon receiving a (negative) diagnosis of severe PD based on personal and social deterioration may feel demoralized to begin therapeutic work. It may also happen that the individual receives a subsidy from the state (i.e. for disability based solely on this severity diagnosis); which can be a reinforcer to hold on to the disease and not seek treatment. In contrast, a comprehensive approach that includes the PPM to the current nosology of PD would reinforce the patient’s strengths, who would value and use these for their own improvement and that of the people around them, feeling useful, integrated, and with a deep meaning of their sense of life. Likewise, in the diagnostician, this comprehensive approach would forge the need to learn to contemplate the human being not only with an essential or recuperative focus, but also with an empowering and prosocial focus.
Another concern arises when incorporating a severe level of PD, whose threshold still does not show diagnostic accuracy, because of the few cases present at this level (Bachet al., 2021; Olajide et al., 2018). Likewise, it does not justify the usefulness of the most extreme threshold, since the therapeutic plan for severe PD is similar to the therapeutic management provided to moderate PD. Although the PD diagnostic model, based on its severity, has shown (in its measurements) preliminary results of cross-cultural validity and utility (Ayinde & Gureje, 2021; Bach & Tracy, 2022) —not without limitations (L. Hualparuca-Olivera, 2022)—, it has also shown low discriminative validity with weak latent structures (Sleep et al., 2021). In addition, because there is no clear boundary between PD and normal personality (Gamache et al., 2021; Jang & Vernon, 2018), the circumscribed threshold (i.e. personality difficulty) can be confused with other difficulties commonly diagnosed in primary care (e.g. stress, not classified elsewhere), generating false negatives for mild PD. According to prominent authors, for several decades there has been a protest against the desire of clinical psychology and psychiatry to medicalize human difficulties (Stein et al., 2020), and their strengths and virtues have not been considered (Messias, 2020; Seligman, 2019; Yang et al., 2022). Therefore, the incorporation of a positive framework may be more useful.
The Positive Framework of Personality: Implementation in the ICD-11-PD Model
This positive perspective establishes that every human being seeks to grow, provide, and find satisfaction and happiness, even when he or she experiences a mental disorder (Messias, 2020). From the beginning of the understanding of the mind, Greeks studied the wisdom of the human being as a virtue; and positive psychology rescued this idea of studying the characteristic virtues and strengths of individuals, even in clinical practice (Kanellakis et al., 2022; Lambert et al., 2023; McTiernan et al., 2022; Sarı & Schlechter, 2020; Stemmler et al., 2021; Wood & Tarrier, 2010). Newly born positive psychiatry seeks to extend this knowledge, even toward biological markers (Jeste et al., 2015; Ruini, 2017), to promote wellness in people with mental and physical illnesses (or at risk of developing them). Likewise, given the limitations of diagnostic systems, positive psychiatry it seeks to generate a nosological taxonomy that not only focuses on symptoms and dysfunctions but also on physical and mental health (Jeste et al., 2015; Johnson & Wood, 2017; Messias, 2020; Tyrer & Mulder, 2022b). Magyar-Moe et al. mentioned the following:
“Putting the client first (i.e., ‘a client with borderline personality disorder’) and seeing their disorder as only one aspect of who they are as a person is much more humane and sets the stage to introduce strengths theory and balanced conceptualizations of clients” (Magyar-Moe et al., 2015, p. 526)
Two integrative models have emerged in recent years that fit the psychiatric nosology of PD: the integrative model of personality strengths and weaknesses (Widiger, 2016) and the integrative dimensional model, based on the previous work of other authors (de la Iglesia & Castro Solano, 2018). The first model does not exploit the potentialities of the positive frame of personality by locating it as a contiguous range of neutrality for dysfunctional extremes. The second model places the positive range at one extreme and the maladaptive range at the other; however, it does not disaggregate the levels in the positive range. This last model has emerged as an alternative to incorporating a positive range without affecting the practicality (ease) of evaluation at the cost of limiting its potential. It is important to understand that, from the positive approach, personality encompasses more than normality and abnormality because functioning is centered on values, virtues, and strengths (de la Iglesia & Castro Solano, 2018). As some authors mention (e.g. Widiger, 2016), a person with high levels of extraversion, agreeableness, conscientiousness, openness, and emotional stability performs positively in his personality. However, to a lesser extent, people with high levels of introversion, antagonism, disinhibition, closedness, and neuroticism can still function in a satisfactory manner in a parsimonious way. This statement is key to understanding the spectrum of personality functioning, and how traits interact within this spectrum.
As a first deduction, it can be stated that a “negative” or “maladaptive” trait does not necessarily imply impaired functioning (Regier et al., 2020); and as a second deduction, a “positive” trait does not necessarily imply a resilient performance that generates well-being (Wood et al., 2016). Both the first and second deductions are supported by previous studies, which have been understood in clinical practice (Widiger, 2016). A third deduction implies that people who have a mental illness, in this case PD, definitely have more dysfunctional traits, but they also have functional traits (adaptive) and, to a lesser extent, positive (or resilient) traits (de la Iglesia & Castro Solano, 2018; Widiger, 2016). This indicates that the general functioning of an individual’s personality is the sum of the valence of each trait. Therefore, a comprehensive examination of these valences is necessary (L. M. Hualparuca-Olivera et al., 2022; Widiger, 2016). Figure 1 illustrates, in a general way, an integral framework of personality adjusted to the ICD-11 nosology.
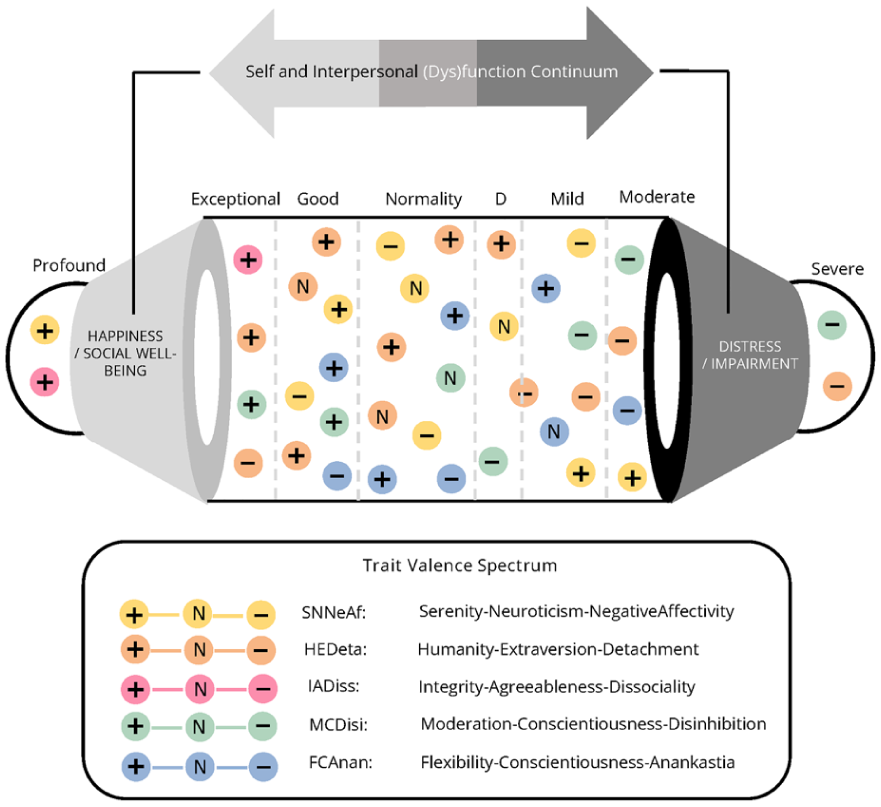
New comprehensive model of personality functioning and traits.
For assessment, however, it is first necessary to evaluate what is manifested—namely, personality functioning (after verifying the general and positive clinical requirements)—in order to determine the level and intensity of intervention required (Figueroa-Cave, 2018; World Health Organization, 2024). Subsequently, the constellation of traits, or more specifically their facets, is identified to determine the particular characteristics that may constitute therapeutic targets (to be reduced or enhanced; Bach & First, 2018; Tyrer et al., 2015).
For example, within this model, the borderline pattern is retained in ICD-11. However, it is considered a heterogeneous and unstable construct, and its specialized interventions have not demonstrated superiority over the core components of structured clinical management (Tyrer & Mulder, 2022c). This suggests that an intervention focused on specific domains, rather than on a heterogeneous category—as is the case with specialized treatments for borderline personality disorder—may be more effective and potentially of shorter duration (Tyrer & Mulder, 2022c).
For comparison, Figures 2 and 3 illustrate the assessment approach of the current ICD-11 personality disorder model and the proposed integrative model, respectively.
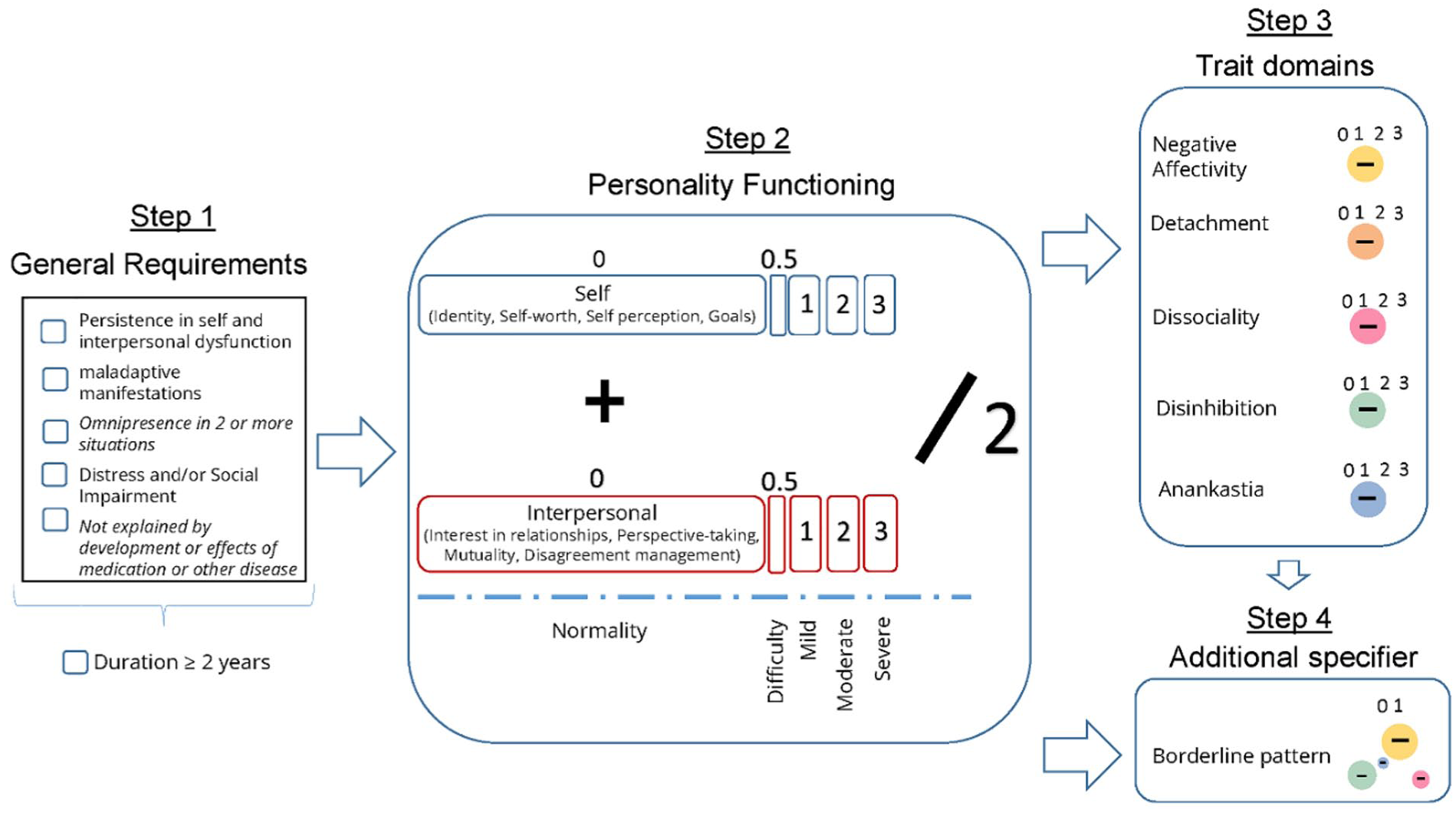
Current evaluation model of the ICD–11–PD.
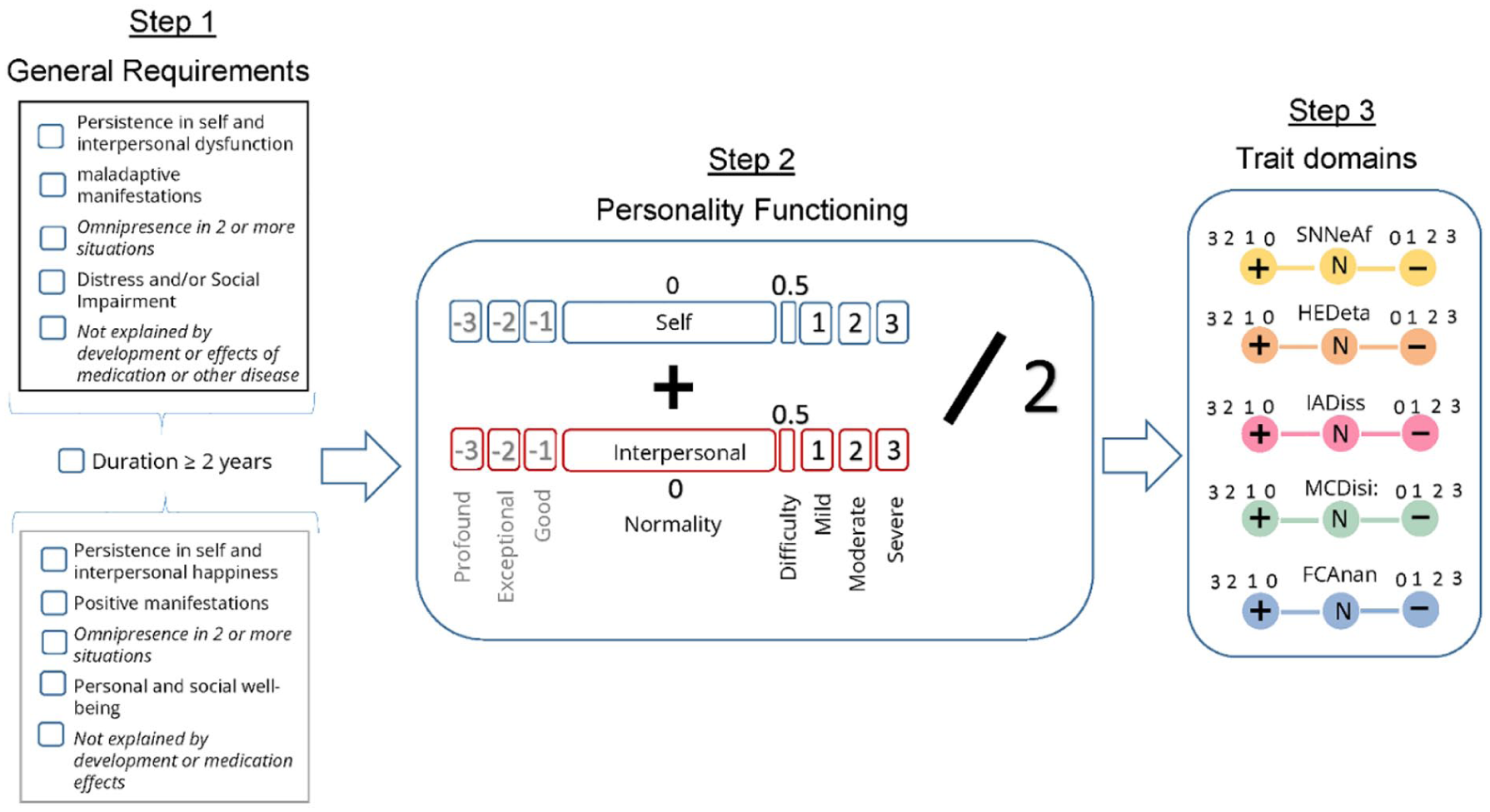
Assessment of PD using an integrative model of psychopathology and health.
Discussion
Although the study and application of the positive perspective has a promising future for all psychiatric conditions, its usefulness is particularly important in the field of PD. Both positive clinical psychology and positive psychiatry have a precise historical basis in the study of personality (Wood & Johnson, 2016), and researchers have provided important evidence to support the usefulness of this perspective in the evaluation and treatment of PD and other conditions in clinical practice (Duckworth et al., 2005; Widiger, 2016; Yang et al., 2022). According to leading researchers, the usefulness of the ICD-11-PD model in clinical management implies (a) the reduction of stigma in communication between health providers, patients, and their families; (b) favoring the differential diagnosis and assignment of the most relevant mental disorders; and (c) making it possible to predict future treatment needs (assault, suicide, or other morbid conditions), in addition to specifying the expected degree of disability leave (see Bach et al., 2022).
The diagnosis of PD is stigmatized more than many other mental disorders (Tyrer & Mulder, 2022c), and the dimensional model, which highlights the recuperative approach to this condition, may not generate a significant change in the entrenched perception of the diagnostician or patient if there is no adequate training (Baker et al., 2022). Consequently, the positive personality perspective can be used to further change the categorical clinical perspective toward a more complete dimensional model. There are several measures for evaluating positive personality characteristics: the Inventory of Strengths and Values in Action (VIA Inventory of Strengths; Peterson & Seligman, 2004), and the Positive Traits Inventory-5 (PTI-5; de la Iglesia & Castro Solano, 2018). Furthermore, the integrated measures of the maladaptive range of personality include the five-factor form (FFF; Widiger, 2016) and the Integrative Dimensional Personality Inventory for ICD-11 (IDPI-11; L. M. Hualparuca-Olivera et al., 2022); the latter includes the positive ranges of personality traits and their functioning.
The fundamental difference between the comprehensive framework proposed in this paper and the previous ones is that this model disaggregates and assesses the different levels of the positive range of personality. This distinguishes it from the conventional measures of the normal or maladaptive range of the five-factor model. This is because it is only possible to assert a low or high functioning of the trait domain, but not to identify them with precision when their location is outside their thresholds. By having a more precise location of personality functioning in the positive range, decisions can be made about the intensity of interventions to promote positive traits. Furthermore, it allows to specifying which of these to promote in the patient (Levak et al., 2011), and avoiding contraindications to the PD of the evaluated person, as described in previous studies (Hervás, 2017).
Using an approach from positive psychology interventions (PPIs; Smirnova & Parks, 2018) and positive therapy (PPT; Peseschkian & Remmers, 2020), the practitioner can provide psychotherapy and treatment of PD using a therapeutic approach. Furthermore; carry out counseling, prevention, and education from a preventive-pedagogical approach; promote cross-cultural understanding from a social approach; and establish the cooperation and integration of different therapeutic methods from an interdisciplinary approach (Peseschkian & Remmers, 2020). That is, with an explicit positive framework within the ICD-11-PD model, objective guidelines can be established to prevent these conditions and promote multidisciplinary and multi-sectoral work (Wood & Johnson, 2016). This allows for the inclusion ofthe human virtues of the person who suffers from it by qualifying categorically or dimensionally between normality and abnormality (de la Iglesia & Castro Solano, 2018; Widiger, 2016).
In this sense, personality should not be seen only as the absence or presence (graded or not) of the disorder but as a bipolar spectrum between well-being and illness. For example, in specialized care, it may be useful to intervene in the conative domains of the patient (e.g. volitional, ethical; see Liutsko, 2019). In this way, an integration of their identity can be promoted, since the person not only experiences a pathogenic agent or environment but also of pathogenesis and salutogenesis (Bach & Mulder, 2022; Johnson & Wood, 2017). Moreover, with the support of the World Health Organization, incorporating a positive framework for personality disorders into the diagnostic classification system could enable research on personality disorders to advance in diverse directions and help reduce methodological biases in this field, by enriching studies with a more comprehensive and precise assessment of the full spectrum of personality.
Within a positive personality framework (i.e. individual positive traits), the management of disability in health services may be improved by integrating the other two levels of subjective well-being: positive subjective states and positive groups and institutions (Dunn, 2018). In this regard, the rehabilitation of chronic mental and physical conditions—for example, through the development of positive disability identities (Dunn, 2018)—may be cost-effective compared with purely traditional clinical interventions (Johnson & Wood, 2017). Similarly, in both primary and specialized care, it may be useful to identify individuals with positive levels of personality (including virtuous characteristics) who can act as agents of positive change (i.e. positive transformers of their environment) and contribute to health promotion. Governments and health authorities should establish policies and investments to facilitate these initiatives. The positive paradigm may have substantial impact in primary care and could help alleviate pressure on specialized services. This would be particularly beneficial in low- and middle-income countries (LMICs), where access to higher levels of care is often limited and inefficient. It is important to note that traditional clinical practice has primarily focused on symptom reduction, thereby alleviating distress and impairment; however, patients not only seek medication or psychotherapy to reduce discomfort, but also guidance to achieve well-being and happiness (Johnson & Wood, 2017; Messias, 2020).
A meta-analysis (Cobben, 2017) showed that BPD symptoms decreased after PPIs based on mindfulness, acceptance and commitment therapy (ACT), and loving-kindness and compassion meditation (CM/LKM), in addition to increasing well-being. Similarly, it has been shown that individuals with severe dissocial tendencies can benefit from treatment based on Risk-Need-Responsivity (R-N-R; Andrews & Bonta, 2010) complemented by the Good Lives Model program (Ronel et al., 2013), or its variant Positive Re-Entry in Corrections Program (PRCP; Huynh et al., 2015), within the multidisciplinary framework of Positive Criminology (Lindley, 2022). Emphasis can be placed on interventions based on mindfulness, self-training, hetero-compassion (Hervás, 2017; Olsen, 2021), reintegrative shame, self-help groups, social acceptance, and exposure to kindness (Lindley, 2022), which promote the development of positive personality traits such as moderation, humanity, and integrity. Likewise, specific PPIs have recently been provided from art therapy, combined with schema therapy, to strengthen a healthy adult self (Haeyen, 2019). These techniques can address all six healthy ego functions of maladaptive personality performance through exercises that promote self-acceptance, expression of the experiential world, compassion, mindfulness, appreciation of artistic images, expressive representation of various modes, and healthy adult patterns, as well as address limited reparenting (Haeyen, 2019).
Finally, the alternatives mentioned in this paper to improve clinical management through a positive expansion of the ICD-11 PD model are based on indirect evidence —as science begins—. Therefore, it is necessary for future research to delve more deeply into confirming the viability of these hypotheses. Scientific interest and funding has focused on the study of pathological biomarkers and their domains (Seligman, 2019). Nevertheless, support for the perspectives, models, and methods available and with demonstrable evidence is needed to address such a complex construct. Thus, a comprehensive perspective linking psychopathological performance with virtuous functioning would be useful (Christy et al., 2018; Jeste et al., 2015).
Conclusions
This paper aimed to provide a perspective to incorporate a positive paradigm that favors the usefulness of the ICD-11-PD model in clinical practice, as well as a potential framework susceptible to improvement, for future models of psychiatric nosology. With ICD-11, the WHO has shown interest in prioritizing clinical usefulness and cross-cultural applicability over the inter-rater reliability of its constructs (Keeley et al., 2016) and despite its Kraepelinian ontological (categorical) foundations. For example, there has been an initiative for the dimensional diagnosis of some mental disorders and the incorporation of traditional medicine in one of its chapters. This comprehensive and inclusive approach can also support the incorporation of a salutogenic perspective: mental disorders, and even more so PD, constitute a complex entity compiled from multiple vulnerabilities (Livesley & Larstone, 2018; Regier et al., 2020; Somma et al., 2022). Although the PD has effective evidence-based interventions, it cannot be denied that there are cases that do not respond to treatment (Somma et al., 2022). These individuals tirelessly seek relief from the distress and frustration generated by their personality dysfunction. The authors of this paper believe that in such situations, a positive approach provides greater shelter to those in whom the purely clinical categorical/dimensional approach does not rescue the potential of their humanity.
Footnotes
Ethical Considerations
Due to the study design, no ethics committee approval was required.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The database is available with a request to the corresponding author*.