
Abstract
Background:
People with mental disorders (PMD) not only face difficulties related to their mental health problems, but also suffer from the stigma and discrimination associated with them. Research on social stigma in the educational setting has been mainly focused on health sciences students.
Aims:
The main objective was to compare the level of social stigma toward PMD among university students, categorized by their fields of study. Additionally, the analysis considered gender, knowledge about mental health, familiarity, and contact.
Methods:
A cross-sectional study was conducted among all first-year undergraduate students during the 2023–24 course at the University of Valencia, who were enrolled in five study fields: Engineering and Architecture (EA), Arts and Humanities (AH), Social and Legal Sciences (SL), Sciences (SC) and Health Sciences (HS). All students completed online an initial questionnaire with socio-demographic items, as well as the following questionnaires: The Mental Health Knowledge Schedule (MAKS), the Reported and Intended Behaviour Scale (RIBS), the Scale of Community Attitudes toward Mental Illness (CAMI), and the Attribution Questionnaire (AQ-27).
Results:
The final sample comprised 2,693 students. The EA students scored highest in authoritarianism and social restrictiveness, and lowest in benevolence and CMHI. Students from SL had higher levels of public stigma than those from AH, SC and HS. Considering only women, EA had the highest scores in authoritarianism. EA men had lower benevolence and lower CMHI.
Conclusion:
These findings suggest that anti-stigma programs conducted at higher education institutions, in addition to traditional health sciences students, should target students from other study fields. This paper goes a step further by proposing that university curricula should include activities to improve understanding of mental health problems and reduce social stigma associated with PMD.
Background
People with mental disorders (PMD) face not only the challenges posed by their condition, but also the associated stigma and discrimination (World Health Organization [WHO], 2024). This stigma can delay help-seeking behavior, violate fundamental rights, and exacerbate marginalization and social exclusion. Indeed, many individuals report that the experience of stigma is more distressing than the mental health condition itself, as it hinders recovery and makes it difficult to normalize their lives (National Academies of Sciences, Division of Behavioral, Social Sciences, Board on Behavioral, Sensory Sciences, & Committee on the Science of Changing Behavioral Health Social Norms, 2016; Thornicroft et al., 2022).
The literature identifies four main types of stigma: social or public stigma, self-stigma, structural stigma, and stigma by association. Social stigma refers to the negative attitudes that society holds toward PMD (Thornicroft et al., 2022) and encompasses stereotypes (cognitive beliefs), prejudices (emotional reactions), and discrimination (behavioral responses) directed at a specific group (Muñoz, 2025; Muñoz et al., 2009). Research on social stigma has explored several contexts, including healthcare, education, the media, and the workplace (Azcoitia et al., 2025; Balasch et al., 2016; Muñoz et al., 2009). In the educational setting, studies have primarily focused on secondary and university students (Corrigan et al., 2016; Fuentes-Durá et al., 2025).
Several studies have documented the presence of social stigma among university students (Gervas et al., 2020; Lyndon et al., 2019; Pranckeviciene et al., 2018; Ruiz et al., 2022). Atienza-Carbonell et al. (2024) reported that stigma levels among university students are comparable to those observed in the general population. Factors such as female gender, older age, prior personal contact with individuals experiencing mental health issues, and greater knowledge about mental health have been associated with lower levels of stigma (Ruiz et al., 2022; Saavedra et al., 2021; Sandhu et al., 2021). Most research in this area has focused on students enrolled in healthcare programs, and stigma has been documented among students in medicine (Atienza-Carbonell et al., 2022; Brahmi et al., 2022; Gervas et al., 2020), nursing (Giralt Palou et al., 2023; Martínez-Martínez et al., 2019), pharmacy (Bazzari & Bazzari, 2023; Shehata & Abdeldaim, 2020), psychology (Lyndon et al., 2019; Pranckeviciene et al., 2018), and occupational therapy (Gajardo et al., 2022). Studies comparing stigma across different university programs typically consider only a limited number of degrees. For example, at the University of Valencia (Spain), Ruiz et al. (2022) found that medical, psychology, and education students exhibited less stigma than economics and data science students. Moreover, linguistics students showed higher levels of stigma than psychology and engineering students (Arnáez et al., 2023). Some research has adopted a broader perspective, examining stigma across a wide range of university programs. This approach is particularly valuable given that all students may interact with PMD either directly (e.g. healthcare professionals) or indirectly in the future. For instance, Sandhu et al. (2021) reported that social science students at McMaster University in Canada exhibited lower stigmatizing attitudes than their engineering peers. Similarly, at the University of South Florida, STEM students scored lower on positive attitudes and help-seeking intentions compared to non-STEM students (Rafal et al., 2018). A multicenter study in China by Li et al. (2024) also found that students in healthcare programs demonstrated less stigma and a greater willingness to help than those in non-healthcare fields.
Despite these insights, most of the evidence relies on comparisons of two groups of students, such as health sciences versus non–health sciences or STEM versus non-STEM. Only a few studies have examined stigma across all students at a single university and this remains a significant gap in the literature. Typically, universities offer a large number of degrees, for example the University of Valencia offers 58, making it necessary to group them into broader categories. In our study, we have chosen to follow the categorization structure established by current Spanish legislation and have worked with five knowledge branches, also known as study fields.
The primary objective of this research is to compare levels of social stigma toward PMD among university students according to their field of study. A secondary objective is to examine the relationship between stigma and several variables including gender, mental health knowledge, and prior familiarity or contact with PMD.
Methods
Study Design and Participants
This study has a cross-sectional design. The study population included all first-year undergraduate students from the University of Valencia (UV) during the academic year 2023 to 2024. In Spain, university-level study fields are organized according to Royal Legislative Decree 1393/2007, which is based on international frameworks developed by UNESCO, the OECD, and the ISCED. This decree classifies study fields (also referred to as branches of knowledge) as: Engineering and Architecture (EA); Arts and Humanities (AH); Social and Legal Sciences (SL); Sciences (SC); and Health Sciences (HS) (see Supplemental Material).
All students were invited to complete an electronic online questionnaire using the survey application tool LimeSurvey (https://www.limesurvey.org/es/). To ensure a minimum number of responses, one group from each degree was invited in person to complete the survey. These groups were not chosen randomly. The staff at each center selected the most suitable group to minimize interference with other ongoing academic activities. Before accessing the questionnaire the participants gave their informed consent to participate. The online survey lasted approximately 15 min and was completed between September 20 and November 30, 2023. Only students aged 17 to 25 were included in the analyses. The rationale behind the choice of this age range was that it corresponds to the emerging adulthood development period (ages 18–25; Arnett, 2000). This is a period between adolescence and young adulthood that fits within the age range of most first-year university students in Spain. Seventeen years-old students were also included in our sample because they turn 18 before the end of the calendar year (the university course begins in September).
Study Instruments
All participants were asked to provide socio-demographic variables, age, gender, and degree course, as well as to complete the following questionnaires.
Mental Health Knowledge Schedule (MAKS) (Evans-Lacko et al., 2010)
The MAKS consists of two parts: the first covers six areas of stigma-related mental health knowledge: help-seeking, recognition, support, employment, treatment, and recovery; and the second consists of six items assessing knowledge of mental health conditions. Only the first part of the MAKS, focussing on the areas of mental health knowledge related to stigma, was used (Sayols-Villanueva et al., 2015).
The items are scored on a 5-point Likert scale, ranging from 1 (=strongly disagree) to 5 (=strongly agree). Total scores are calculated by adding up the response values for each item (“Don’t know” score is coded as neutral = 3). Item 6 is reverse-coded. Overall, higher scores indicate greater knowledge. Because the MAKS scale was not designed to be used as a functional scale, Cronbach’s alpha is not a reliable indicator (Evans-Lacko et al., 2010).
Reported and Intended Behaviour Scale (RIBS) (Evans-Lacko et al., 2011)
This scale consists of eight items, divided into two groups, that measure familiarity with, contact with, and intention to have contact with PMD. The first four items ask participants about their familiarity with and contact with PMD using yes/no responses. We used these four items to identify and assess the percentage of students who have known or know someone with a mental disorder (RIBS Familiarity) and the percentage of students who have lived/worked or are living/working with a PMD (RIBS Contact).
Scale of Community Attitudes Toward Mental Illness (CAMI) (Taylor & Dear, 1981)
This scale assesses the attitudes of the general population toward PMD, focusing on opinions about their integration into the community. This study used the Spanish adaptation validated by Ochoa et al. (2016), with a reliability of 0.86. It consists of 40 items with a five-point Likert scale, grouped into four dimensions: authoritarianism (the belief that PMD are inferior and should be treated coercively); benevolence (a compassionate view of those experiencing mental disorder based on humanistic parameters); social restrictiveness (the view that PMD are a threat to society); and community mental health ideology (concerned with the therapeutic value of the community and the acceptance of de-institutionalized care).
Attribution Questionnaire (AQ-27) (Corrigan et al., 2004)
This questionnaire briefly describes a man diagnosed with schizophrenia. Its 27 items assess stereotypes, prejudices and discrimination using a 9-point Likert scale. Nine subscales are used to group responses: responsibility, pity, anger, dangerousness, fear, help, coercion, segregation, and avoidance. The total score of the scale is obtained by summing the scores of the nine subscales, taking into account that the items on the help factor are reversed. Higher scores indicate higher stigma. This study used the Spanish adaptation validated by Muñoz et al. (2015), with a reliability of 0.86.
Statistical Analyses
Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) version 28.0. Category variables were described using frequencies and percentages, and quantitative ones were described using means and standard deviations (SD). For inferential statistics, χ2, independent samples t-test, ANOVA, MANOVA and Pearson’s correlations were used. Post hoc comparisons were performed with Tukey or Games-Howell depending on variance homogeneity.
Results
Description of General Characteristics of the Sample
Of the 8,111 first-year students enrolled at the UV, 2,693 (33.2%) completed the socio-demographic questions, as well as the MAKS, the RIBS, and at least one of the two stigma-assessment scales (CAMI, AQ-27). The number of students between the ages of 17 and 25 who made up the study sample was 2,420.
The mean age for the whole sample was 18.41 years (SD = 1.37). The total percentage of women was 65.37%, men 33.10%, and 1.53% selected the option non-binary. Regarding familiarity with PMD, 80.37% know/had known PMD, and 50.62% live/had lived or work/had worked with PMD. Regarding mental health knowledge, the mean MAKS score was 22.99 (SD = 2.72). Table 1 shows the results for these variables for each of the five study field groups.
Demographic Characteristics and Scores in MAKS and RIBS in the Five Study Field Groups.
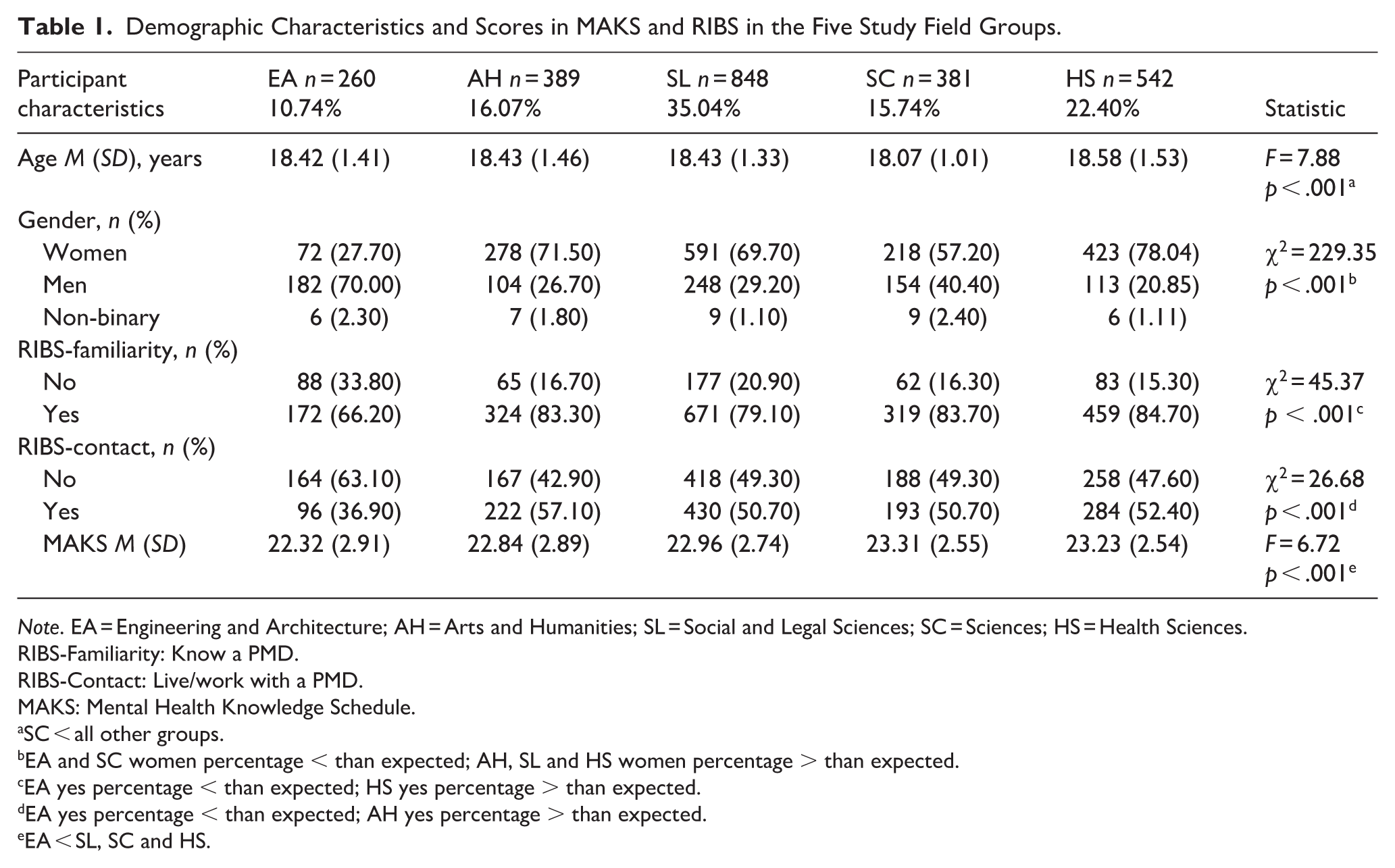
Note. EA = Engineering and Architecture; AH = Arts and Humanities; SL = Social and Legal Sciences; SC = Sciences; HS = Health Sciences.
RIBS-Familiarity: Know a PMD.
RIBS-Contact: Live/work with a PMD.
MAKS: Mental Health Knowledge Schedule.
SC < all other groups.
EA and SC women percentage < than expected; AH, SL and HS women percentage > than expected.
EA yes percentage < than expected; HS yes percentage > than expected.
EA yes percentage < than expected; AH yes percentage > than expected.
EA < SL, SC and HS.
The percentage of women students was significantly lower in EA and SC compared to the other groups. RIBS results showed that EA was the study field with the lowest familiarity with PMD (χ2(4, N = 2,420) = 45.37; p < .001; Adjusted Standardized Residuals = 6.1), whereas HS students had the highest (Adjusted Standardized Residuals = 2.9). The EA group had the lowest scores on RIBS Contact (χ2(4, N = 2,420) = 26.68; p < .001; Adjusted Standardized Residuals = 4.7) while AH had the highest (Adjusted Standardized Residuals = 2.8). MAKS scores were also significantly lower in EA than in SL, SC, and HS.
Scores on the MAKS and RIBS were compared by gender. Women scored significantly higher than men on the MAKS (23.27 + 2.61 vs. 22.45 + 2.88; t1472 = 6.75; p < .001). Women also had a higher percentage on both the RIBS-Familiarity (χ2(1, N = 2,383) = 101.47; p < .001) and the RIBS-Contact (χ2(1, N = 2,382) = 45.41; p < .001) compared to men.
Analysis of Stigma Scores by Gender, Familiarity, Contact, and Study Fields
Table 2 shows the scores on the CAMI and AQ-27 questionnaires by gender, familiarity, contact, and study field. Compared to women and non-binary students, men scored higher on authoritarianism and social restrictiveness and lower on benevolence and CMHI. Men also scored higher on the AQ-27, indicating a greater presence of stereotypes, prejudice, and discrimination than women and non-binary students. A higher degree of familiarity and contact with PMD, as measured with the RIBS, were associated with lower scores on the AQ-27 and on authoritarianism and social restrictiveness, and with higher scores on benevolence and CMHI dimensions of the CAMI.
Means, Standard Deviations and Differences as a Function of Gender, Familiarity and Contact With Mental Illness, and Study Fields in CAMI Scale Dimensions (n = 2,405) and AQ-27 Total Score (n = 2,244).
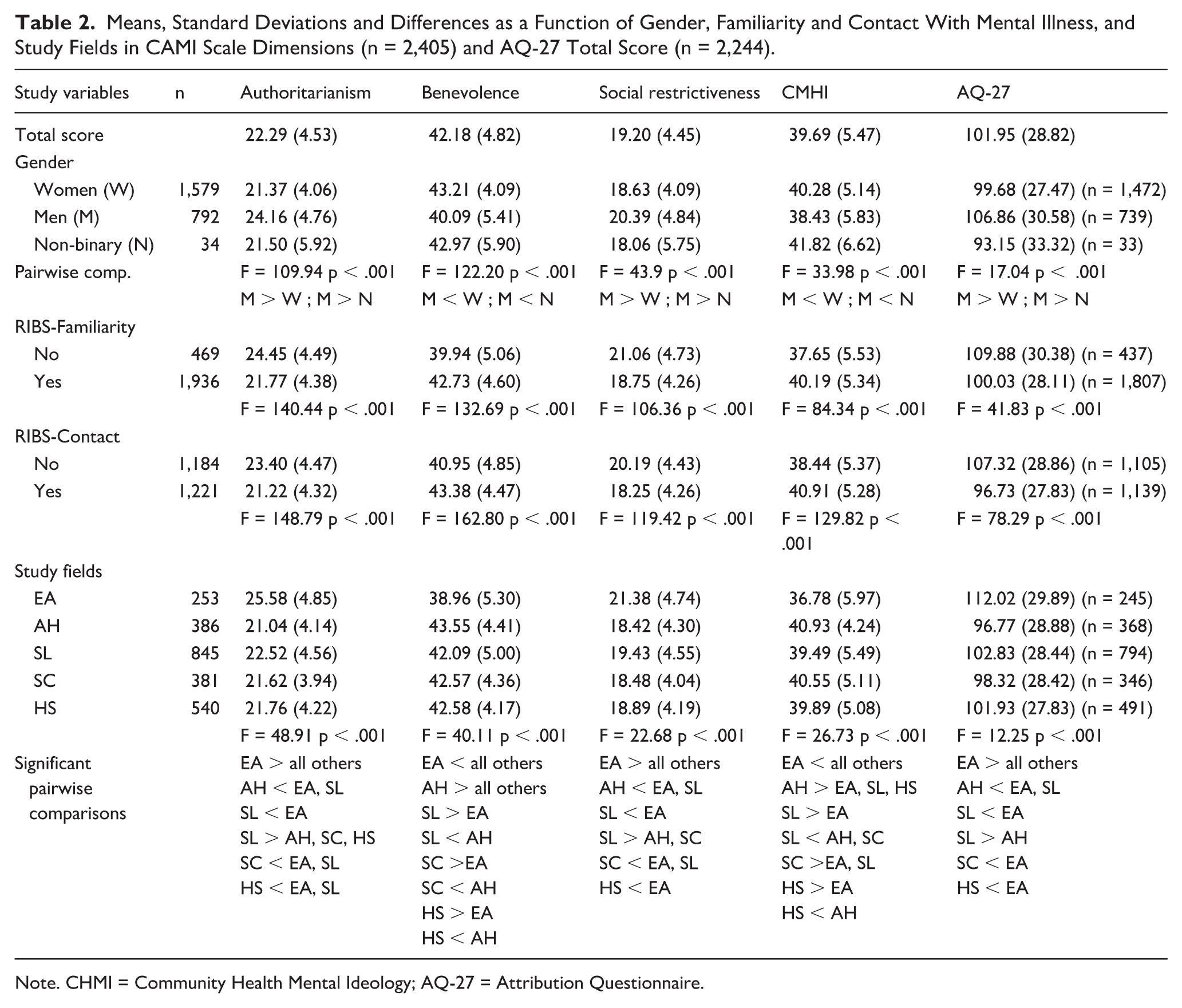
Note. CHMI = Community Health Mental Ideology; AQ-27 = Attribution Questionnaire.
Regarding the different study fields, the most relevant finding was that EA students scored higher on stigma, with high authoritarianism and social restrictiveness but lower on benevolence and CHMI compared to the other four fields. They also scored higher on the AQ-27 (see Table 2). Secondly, it should be noted that SL students also showed high levels of stigma compared to the other three study fields. They scored higher than AH, SC, and HS students on authoritarianism, and higher than AH and SC on social restrictiveness, while scoring lower than AH and SC on CMHI.
The reliability (Cronbach’s α) of the CAMI subscales was .59 for authoritarianism; .78 for benevolence; .70 for social restrictiveness; and .83 for community perception. The overall reliability of the AQ-27 scale was .90.
Gender Analysis by Study Fields
Since the percentage of women is lower in EA and SC (see Table 1), a separate analysis was conducted for women and men in the different study fields. The non-binary group was not included in the analysis because its percentage was very small and did not differ between fields. Table 3 shows complete descriptive statistics and comparisons between study fields, means on CAMI subscales and AQ-27 total score. For women, EA students showed higher scores on authoritarianism and social restrictiveness, and lower scores on benevolence and CMHI than AH students. EA students showed higher scores on authoritarianism than women in the other study fields. On the AQ-27, although the ANOVA was significant, post hoc tests showed no differences. For men, the differences between study fields were more marked. EA students showed lower scores on benevolence and CMHI than students from the other fields. Furthermore, they were more authoritarian and more socially restrictive. SL students showed higher scores than AH and SC students on authoritarianism and lower scores on benevolence and CMHI. As in the case of women, AH students showed lower stigmatizing scores than EA students in all variables.
Comparison of stigma levels between study field groups (separate analyses by gender).
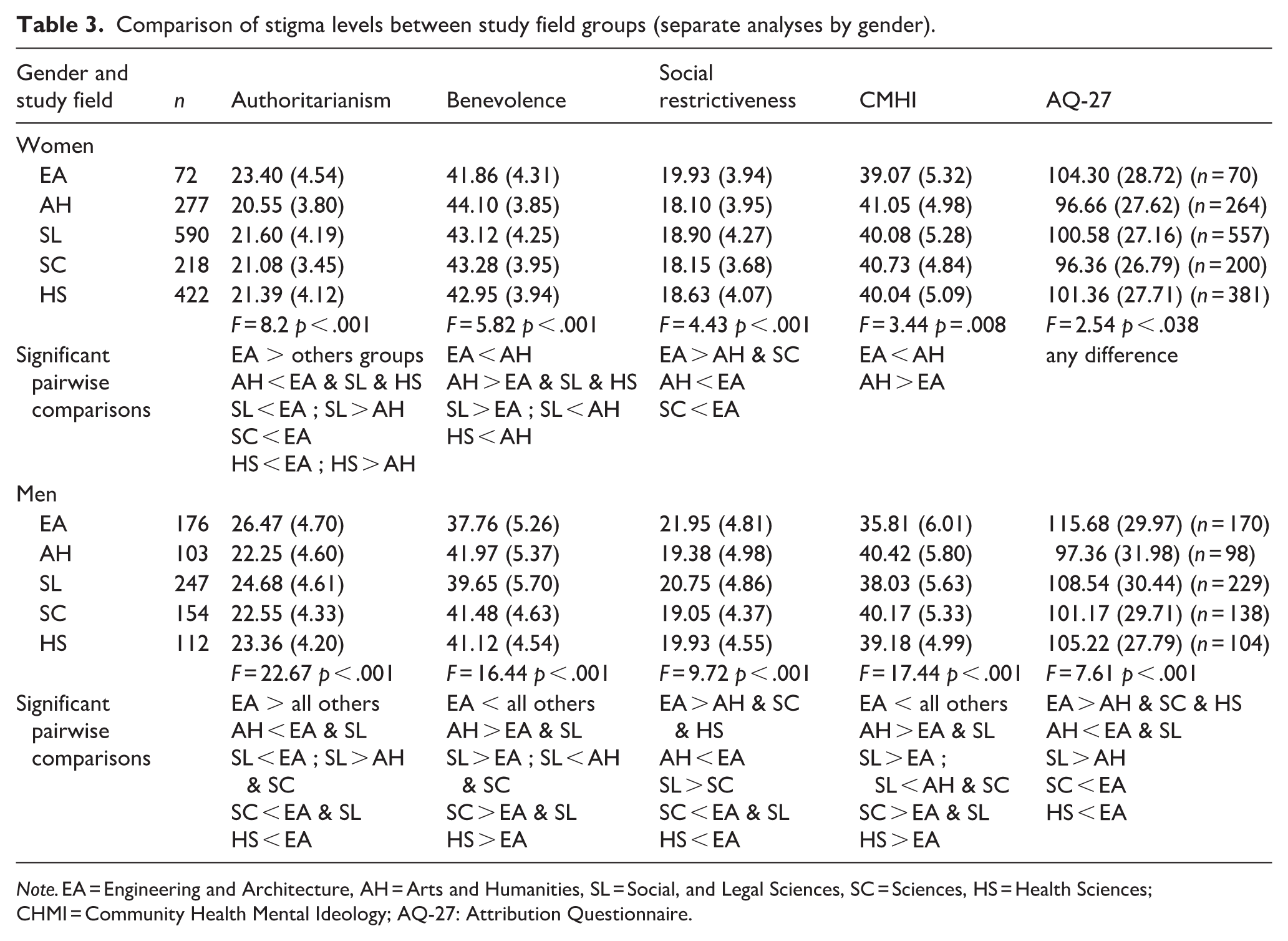
Note. EA = Engineering and Architecture, AH = Arts and Humanities, SL = Social, and Legal Sciences, SC = Sciences, HS = Health Sciences; CHMI = Community Health Mental Ideology; AQ-27: Attribution Questionnaire.
Correlational Analysis
After graphically checking for linearity, the Pearson correlation coefficient was calculated between the outcome variables and mental health knowledge (MAKS) scores. All correlations were significant (see Table 4). Students with higher levels of knowledge on mental health showed less authoritarianism, social restrictiveness, and stigmatizing attributions while showing greater benevolence and willingness to integrate PMD into the community. Effect sizes were intermediate for the CAMI subscales and small for the AQ-27. As expected, correlations between the CAMI subscales and the AQ-27 had a large effect size.
Linear Correlations Between MAKS, CAMI Subscales and AQ-27.
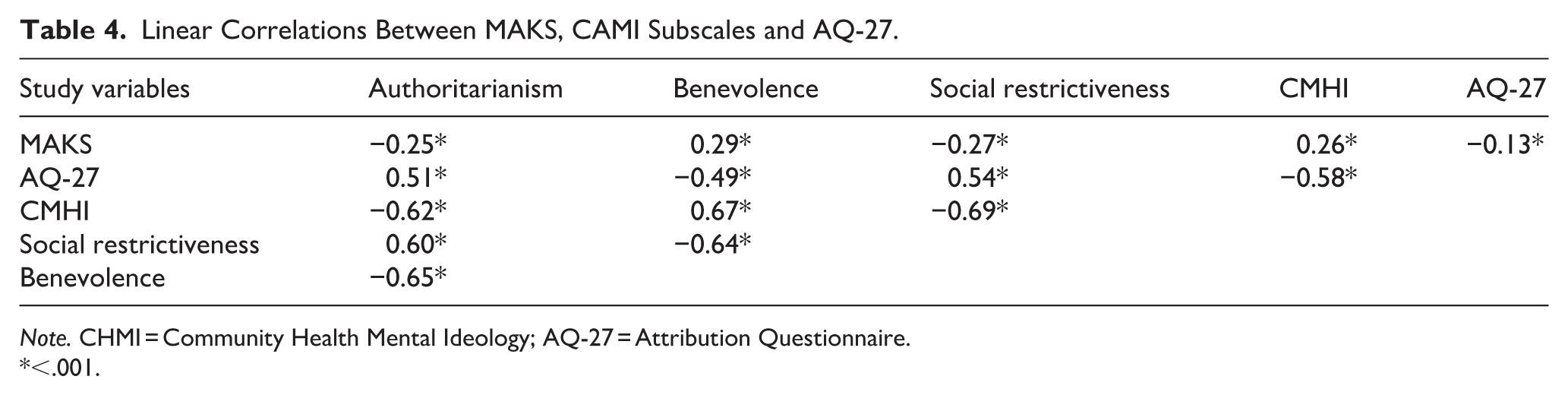
Note. CHMI = Community Health Mental Ideology; AQ-27 = Attribution Questionnaire.
<.001.
Discussion
To date, few studies have examined social stigma toward PMD across an entire university student body. Most existing research relies on dichotomous comparisons, such as health sciences versus non–health sciences students (Li et al., 2024) or STEM versus non-STEM students (Rafal et al., 2018; Zabaleta-González et al., 2023).
This study is among the first to compare social stigma levels in first-year students across the five official university study fields in Spain (encompassing 58 degree programs), and to analyze their associations with several predictors of stigma. This innovative approach has the advantage of creating five analytically comparable groups, allowing a more comprehensive and nuanced assessment of stigma levels across the entire university population than other comparisons based on only two broad and dichotomous categories.
The main finding related to the primary objective of this study is that students enrolled in EA reported the highest levels of social stigma. It is also important to highlight that SL students showed high stigma levels relative to AH, SC, and HS. The field with the lowest stigma levels was AH. Regarding gender differences within study fields, it is notable that women in EA showed higher stigma scores than women in AH, while men in EA exhibited higher stigma scores than men in all other fields.
Consistent with the second objective, the analysis of stigma predictors (gender, mental health knowledge, familiarity, and contact) showed that women exhibited lower social stigma than men across the first-year student body and demonstrated greater mental health knowledge, familiarity and contact. Previous literature similarly reports that women tend to display lower stigma in both Western and non-Western contexts, a pattern partly attributed to their higher mental health literacy (Al Omari et al., 2023; Li et al., 2024).
EA students reported the lowest levels of familiarity and contact with PMD, as well as the lowest mental health knowledge. Greater mental health knowledge, familiarity and contact are associated with less stigma (Arnáez et al., 2023; Li et al., 2024; Saavedra et al., 2021). These variables may help to explain why EA students displayed the highest level of stigma in this study.
For SL students, the second group with the highest stigma levels, there were no notable differences from most other fields in terms of mental health knowledge, familiarity, or contact (with the exception of EA). Conversely, the group with the greatest amount of contact, AH students, also reported the lowest stigma levels.
Prior research suggests that contact reduces prejudice by decreasing contact-related anxiety and increasing empathy toward PMD and perspective-taking (Pettigrew & Tropp, 2008). Improving mental health literacy and promoting familiarity and meaningful contact with PMD should therefore be central goals for universities, as suggested by Thornicroft et al. (2022). Fresán et al. (2012) emphasize the importance of addressing both factors simultaneously; noting that providing information alone, without incorporating contact strategies, may actually increase rather than decrease stigma. According to our findings, these efforts may be particularly relevant for students in the EA and SL fields.
These findings highlight the importance of targeting students from non-health-related degrees on top of the traditional approach involving health sciences students (e.g. Atienza-Carbonell et al., 2022), as priority groups for anti-stigma initiatives in higher education.
Further comparative research is needed to identify specific university degree programs that may be at greater risk of fostering stigmatizing attitudes toward PMD, bearing in mind that cultural and regional contexts are likely to shape these patterns. This need is particularly evident within the Social and Legal Sciences field as it encompasses a diverse array of degrees which may result in considerable internal heterogeneity. Given the relatively high levels of stigma observed in this group, more detailed analyses are needed in the future.
Strengthening collaboration among universities, for example, through the exchange of effective interventions and evidence-based best practices, could support the development of more inclusive and less stigmatizing academic environments, ultimately contributing to more equitable and inclusive societies (Thornicroft et al., 2022).
Limitations
According to the classification used, EA, SC, and HS can be considered homogeneous groups, AH displays relative heterogeneity, and SL is the most diverse, encompassing 21 degree programs (see Supplemental Material). Although some are still heterogeneous, this seems to be a better approach than grouping all students into only two categories (STEM vs. non-STEM or health sciences vs. non-health sciences). The SL group includes degrees in: Economics; Law; Physical Activity and Sports Science; Audiovisual Communication; and Primary School Education. AH includes degrees such as: Classical Philology; History; or Philosophy.
Additionally, only first-year undergraduates have been included in this study sample and the findings are based on self-reported questionnaires which inherently have a risk of response bias, including social desirability. Given that participation was voluntary, self-selection bias cannot be entirely ruled out. Finally, the design of this research does not allow for causal inferences.
Strengths
In this population-based study, all students were invited to participate in the survey via the university intranet. A group from each grade was invited in person by a member of the research team during one of their classes to complete the survey in order to ensure a minimum participation per grade. This resulted in a high response rate of 33.20%, which is noteworthy given that no academic or monetary incentives were offered to students for participation. In addition, this study is among the first to compare stigma levels across several study fields while examining the relationship with several common predictors of stigma. Furthermore, a comprehensive assessment of social stigma was employed.
Conclusion
The importance of stigma reduction for HS students who will be the future care providers for people with mental disorders is obvious, but it should not be forgotten that this is not the only group interacting with such people throughout their lives. Stigma reduction assessment and intervention in other future professionals is also important because we can all influence the stigmatization process. Students will also play important roles in building inclusive societies (Chiu et al., 2022). The results of this study support the recommendations proposed by The Lancet Commission on Ending Stigma and Discrimination in Mental Health (Thornicroft et al., 2022) in the education sector. This paper goes a step further and proposes that university curricula should include sessions to improve mental health literacy and contact with PMD in order to reduce social stigma.
Supplemental Material
sj-docx-1-isp-10.1177_00207640261456751 – Supplemental material for Uncovering Mental Health Stigma in Undergraduates From Different Study Fields
Supplemental material, sj-docx-1-isp-10.1177_00207640261456751 for Uncovering Mental Health Stigma in Undergraduates From Different Study Fields by Inmaculada Fuentes-Durá, Carmen Dasí, Juan C. Ruiz, Lucía Fau-Camarasa and Vicent Balanzá-Martínez in International Journal of Social Psychiatry
Footnotes
Acknowledgements
The authors would like to thank all the students who participated in the study. We would also like to thank the vice-rectorate for Sustainability, Collaboration and Healthy Living, the Dean’s teams of the 18 Centers of the University of Valencia, the professors who opened the doors of their classrooms to us, and Lynne Coppillie for her help with the language of the manuscript.
Ethical Considerations
The study was reviewed and approved by the Ethics Committee at the University of Valencia (reference number 2023-MED-2736351).
Consent to Participate
All participants gave informed consent to take part in the research.
Author Contributions
IF-D: Substantial contributions were made to the following: conception and design, data acquisition, drafting the article, approval of the final version to be published, and obtaining funding. CD: Substantial contributions were made to the following: conception and design, data acquisition, data analysis, and interpretation, drafting the article, approval on the final version to be published. JCR: Substantial contributions were made to the following: conception and design, data acquisition, data analysis, and interpretation, drafting the article, approval on the final version to be published. LF: Substantial contributions were made to the following: drafting the article or revising it critically for intellectual content, approval on the final version to be published. VB-M: Substantial contributions to conception and design, data acquisition, drafting the article, approval on the final version to be published, and obtaining funding.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Conselleria d’Educació, Universitats i Ocupació de la Generalitat Valenciana (CIAICO/2022/232).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.