
Abstract
Background:
Schizophrenia is a severe mental disorder associated with a significant burden of care. Approximately 30% of patients have treatment-resistant schizophrenia (TRS), characterized by persistent psychotic symptoms, being clozapine the antipsychotic of choice for these individuals.
Aims:
To assess whether caregivers of patients on clozapine experience a higher burden of care compared to caregivers of patients on other antipsychotics.
Methods:
We conducted a post-hoc analysis of a cross-sectional study. Sixty caregiver-patient dyads were included (45 on clozapine; 15 on other antipsychotics). Caregivers were assessed using the Family Burden Interview Schedule – Short Form (FBIS-SF). Patients were evaluated using the Clinical Global Impression – Schizophrenia (CGI-SCH) and the Personal and Social Performance (PSP) scales.
Results:
Patients on clozapine exhibited more severe positive symptoms (3.96 ± 1.22 vs. 2.40 ± 1.40; p < .001) and higher total CGI-SCH scores (13.67 ± 3.32 vs. 11.33 ± 3.52; p = .024). No significant differences were found in total FBIS-SF scores between the groups. In the clozapine group, caregiver burden was associated with female patient gender, lower social functioning (PSP), and receiving social benefits. In the non-clozapine group, an earlier age of onset correlated with increased burden.
Conclusions:
Despite greater clinical severity in the clozapine group, the overall burden was comparable to the non-clozapine group, suggesting that clozapine treatment may help stabilize the impact on families. Factors such as female gender, low functioning, and receiving social benefits (a proxy for illness severity) are correlated with specific burden domains. Due to the small size of the non-clozapine subgroup, these associations should be interpreted with caution.
Introduction
Schizophrenia is a severe mental disorder associated with functioning impairment, often causing loss of independence, associated with a high personal, societal, and family burden (Chong et al., 2016).
Family members who live with and care for a relative with treatment-resistant schizophrenia (TRS) patients often report high levels of burden caused by persistent symptoms, poor functioning, and severity of illness (Velligan et al., 2019). The concept of “family burden” encompasses a broader scope than “caregiver burden,” as it includes the consequences for family members beyond the main caregiver. This broader perspective considers interpersonal relationships within the family, the effects on the children of patients, and the social network of the entire family (Schene et al., 1994). Many studies tend to use “caregiver burden” and “family burden” interchangeably, but they represent different aspects of the challenges faced by families.
Caregiver burden has both objective and subjective aspects. The objective burden involves changes in the home environment, finances, employment status, social life, and leisure activities. In contrast, the subjective burden relates to the emotional responses of caregivers as they cope with the demands of providing care (Velligan et al., 2019).
Schizophrenia is one of the leading causes of disability worldwide, even though effective antipsychotic treatments are available (Haro et al., 2015; Marder & Cannon, 2019). Despite the advances in pharmacological treatment, approximately 30% of patients with schizophrenia develop treatment-resistant schizophrenia (TRS), which is characterized by persistent positive and negative symptoms (Kennedy et al., 2014). TRS is defined as the lack of clinical response to at least two different antipsychotics, despite adequate treatment duration and dosage (Howes et al., 2017). Currently, clozapine is the only drug approved for the treatment of TRS (Kane et al., 2019).
In people with TRS, the persistent positive symptoms may increase the caregiver burden (Brain et al., 2018). We conducted a cross-sectional study to evaluate the burden of care among caregivers of patients taking clozapine and those on other antipsychotics, considering the use of clozapine as an indicator of treatment resistance. We hypothesize that TRS is associated with increased levels of caregiving burden.
Methods
Participants
A post-hoc subgroup analysis was conducted on patients taking and not taking clozapine, using data from a cross-sectional observational study that evaluated the burden on caregivers of outpatients with schizophrenia treated at a tertiary center specializing in schizophrenia (Di Sarno et al., 2022).
We analyzed 60 caregiver-patient dyads, consisting of 45 patients on clozapine (as a proxy of TRS) and 15 on other antipsychotics.
Patients were adults of both sexes, clinically stable, aged 18 to 60 years, and diagnosed with schizophrenia according to DSM-5 criteria (American Psychiatric Association, 2013).
All patients taking clozapine had been on a stable dose for at least 1 year and had TRS. In our service, we adhere to the TRRIP (Treatment Response and Resistance in Psychosis) criteria for TRS, which includes having two or more adequate treatments with different antipsychotic medications, assessments using validated rating scales (such as the PANSS), comprehensive information from past treatments, and ensuring adherence to their current treatment plan (Howes et al., 2017). Clinically stable patients on other antipsychotics were classified as non-TRS.
To be qualified as a caregiver, the participant should have provided direct care to the patient for over 1 year, averaging at least 30 hr/week.
Caregivers who were currently participating in any psychosocial intervention programs or who had language difficulties were excluded from this study.
Assessments
Caregivers
Sociodemographic variables were collected with a questionnaire that included questions about age, gender, family relationship, education, family income, marital status, number of hours/week in contact with the patient, and receipt of social benefits. Family income was defined as the total monthly household income, including all sources of income from individuals living in the household. When applicable, the patient’s income (from employment or government support) was included in the total household income.
The primary outcome of this analysis is the caregiver burden, as assessed through the Family Burden Interview Schedule – Short Form (FBIS-SF; Tessler & Gamache, 1996), Brazilian adapted version (Bandeira et al., 2008). The FBIS-SF is a multidimensional, structured personal interview developed in the United States to evaluate both objective and subjective burden. Objective burden items are scored on a Likert scale ranging from 1 to 5, where 1 indicates “never,” and 5 indicates “every day.” Subjective burden items are also assessed on a Likert scale, but this one ranges from 1 to 4, with 1 meaning “not at all” and 4 meaning “very much.” When evaluating the objective subscales A and B, if the caregiver answers “1” on an objective item, it is interpreted as indicating no subjective burden. In this case, the subjective response is left blank because it cannot be scored as 0.
The financial burden is evaluated through five questions that do not contribute to the overall burden score; these questions are meant to provide additional information. The interview lasts approximately 60 min, and interviewers do not need any special qualifications.
All questions refer to the caregiving experience over the last 30 days before the interview, except for the financial burden items, which consider the past 12 months.
The FBIS-SF has five domains related to the family aspects of caregiving: assistance to the patient in daily life (objective and subjective burden), supervision of troublesome behaviors (objective and subjective burden), financial burden (objective and subjective burden), impact on family routine (objective burden), and degree of worry with the patient’s present and future life (subjective burden).
Patients
Sociodemographic characteristics were collected using a questionnaire that included monthly income, marital status, age at diagnosis, disease duration, and the number of psychiatric hospitalizations.
The severity of illness was assessed through the Clinical Global Impression – Schizophrenia (CGI-SCH), which evaluates five dimensions of schizophrenia: positive, negative, depressive, cognitive, and global (de Lima et al., 2007; Haro et al., 2003).
Personal and social functioning was measured with the Personal and Social Performance scale (PSP), a 100-point rating scale divided into four domains. The social activities domain (A) consists of “work and school” and “other socially useful activities (housework, volunteer work, or useful hobbies such as gardening).” The personal and social relationships domain (B) consists of “relationship with a partner,” “family relationships,” and “social relationships.” The self-care domain (C) consists of “personal hygiene” and “care for appearance and clothing.” Finally, “inconvenient and aggressive behaviors” are categorized in the domain (D; Morosini et al., 2000). The patient’s total PSP score should be consistent with the following benchmarks: scores 71 to 100 reflect no dysfunction or “mild” difficulties known only to those familiar with the person; scores 51 to 70 reflect dysfunction or difficulties ranging from “manifest” in one or more domains to “marked” in one domain and scores 1 to 50 reflect “marked” to “very severe” difficulties in two or more domains, where scores ⩽30 demonstrate such poor social function as to require intensive support or supervision (Patrick et al., 2009). The PSP was translated and adapted to Brazilian Portuguese (Menezes et al., 2012).
Ethics
The study was approved by the Institutional Ethics Committee. All participants provided written informed consent after the purpose of the study was explained to them.
Statistical Analysis
All variables were analyzed descriptively. For quantitative variables, means, standard deviations (SD), and medians were calculated. Qualitative variables were expressed as absolute and relative frequencies. To compare means between the two groups (Clozapine vs. Non-clozapine), Student’s t-test was used. The normality of data distribution was assessed using the Shapiro-Wilk test, and the homogeneity of variances was evaluated using Levene’s test. For variables that did not meet the assumption of normality (e.g. patient income and duration of illness), the non-parametric Mann-Whitney U test was employed. The homogeneity of proportions was tested using the chi-squared test or Fisher’s exact test. Correlation studies used Pearson’s coefficient for normally distributed data or Spearman’s correlation for non-normal data. Multivariate analysis was performed using a stepwise linear regression model, including variables with p < .10 in univariate analyses. Analyses were conducted using SPSS 17.0, with a significance level of 5%.
Bivariate analyses were performed to identify factors associated with caregiver burden. It is important to note that these associations do not imply causality due to the cross-sectional nature of the study.
Results
Caregivers
Sixty caregivers were included: 45 provided care to patients taking clozapine and 15 to patients taking other antipsychotics. Most caregivers were family members, particularly mothers. The sociodemographic characteristics are described in Table 1. Family income was also converted to USD purchasing power parities (PPP) exchange rates (OECD, 2021).
Sociodemographic Characteristics of Caregivers (n = 60).
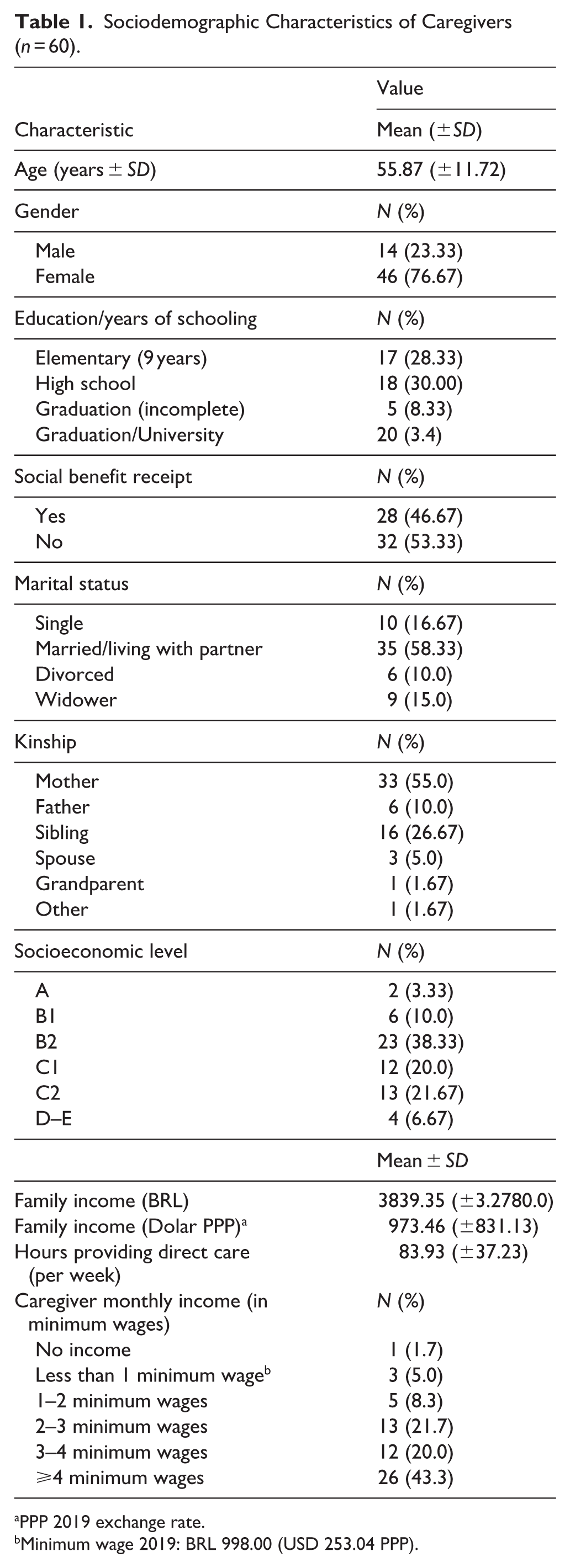
PPP 2019 exchange rate.
Minimum wage 2019: BRL 998.00 (USD 253.04 PPP).
Family Burden Interview Schedule
Table 2 describes the FBIS-SF scores of caregivers. There were no differences between the groups in either objective or subjective burden.
FBIS-SF Scores of Caregivers of Patients on Clozapine and Other Antipsychotics.
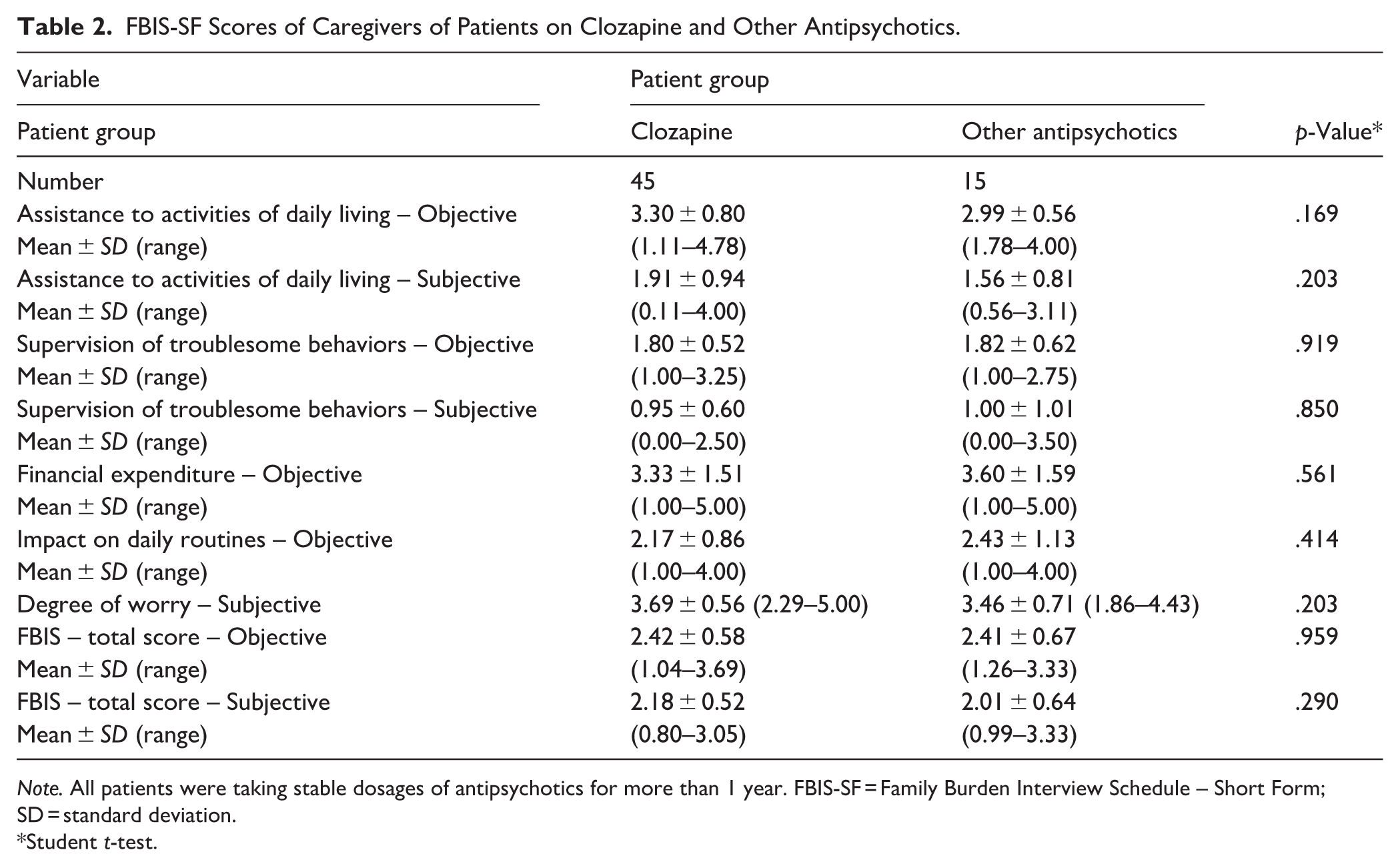
Note. All patients were taking stable dosages of antipsychotics for more than 1 year. FBIS-SF = Family Burden Interview Schedule – Short Form; SD = standard deviation.
Student t-test.
Patients
Forty-five clozapine patients and 15 non-clozapine patients were included; no sociodemographic differences were observed between groups; the majority were male and single (Table 3).
Sociodemographic Characteristics of Patients.
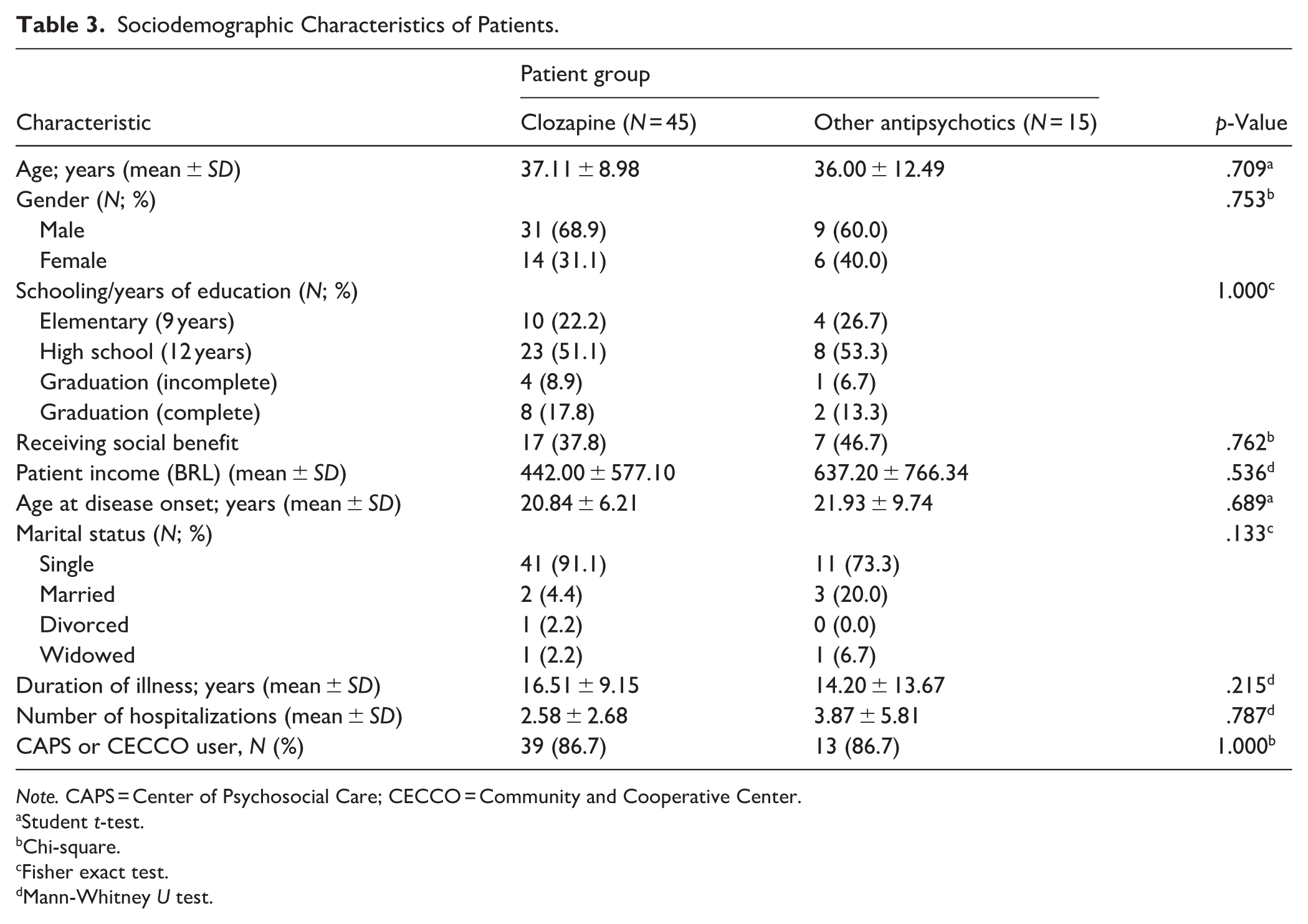
Note. CAPS = Center of Psychosocial Care; CECCO = Community and Cooperative Center.
Student t-test.
Chi-square.
Fisher exact test.
Mann-Whitney U test.
Psychopathology
According to the CGI-SCH, patients taking clozapine had higher positive and total scores (Table 4), although the mean scores in all five domains could be classified as mild disease (less than 4, moderately ill; Haro et al., 2003).
CGI-SCH Assessment.
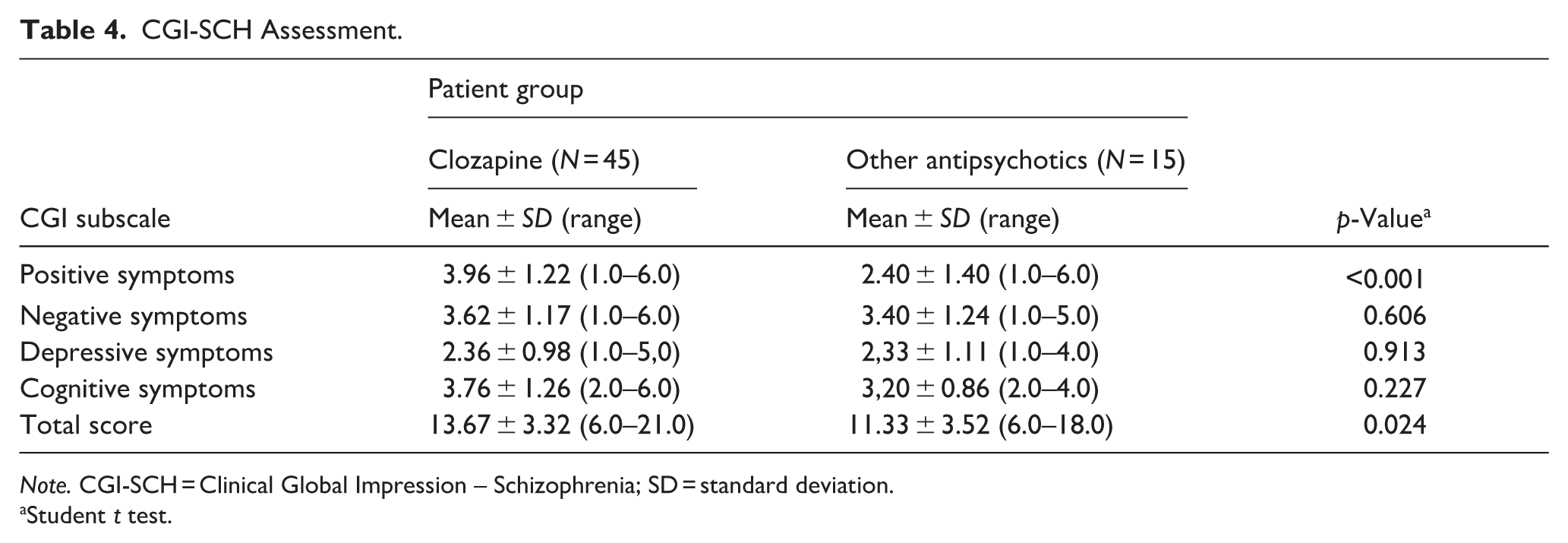
Note. CGI-SCH = Clinical Global Impression – Schizophrenia; SD = standard deviation.
Student t test.
Functioning
The patients had no differences in social functioning, as assessed with the PSP. The mean total PSP scores were (mean ± SD) 61.02 (±11.32) in the clozapine group and 60.13 (±14.91) in the other antipsychotics group (p = .809). The PSP values ranged from 41 to 80 in the clozapine group and from 41 to 90 in the non-clozapine group. The scores indicate a moderate functioning impairment.
Correlation Analyses
Although the caregivers of patients taking clozapine and those taking other antipsychotic medications had similar total scores on the FBIS-SF, and the patients did not show any differences in functioning according to the total scores on the PSP, we conducted correlation analyses. These analyses aimed to determine whether sociodemographic factors and functioning aspects of the patients correlated with specific aspects of caregiver burden in both groups of patients and their caregivers.
In the clozapine group, the age of onset of illness had a correlation with the FBIS-SF in the subjective and objective burden in the supervision of troublesome behaviors and the impact of daily routine (the earlier the onset of illness, the higher the burden). The patient income correlated with the impact on daily routines; higher incomes were correlated with higher burden (Table 5).
Pearson and Spearman Correlation Analyses Between FBIS-BR Scores and Sociodemographic and Clinical Data of Patients Taking Clozapine (n = 45).
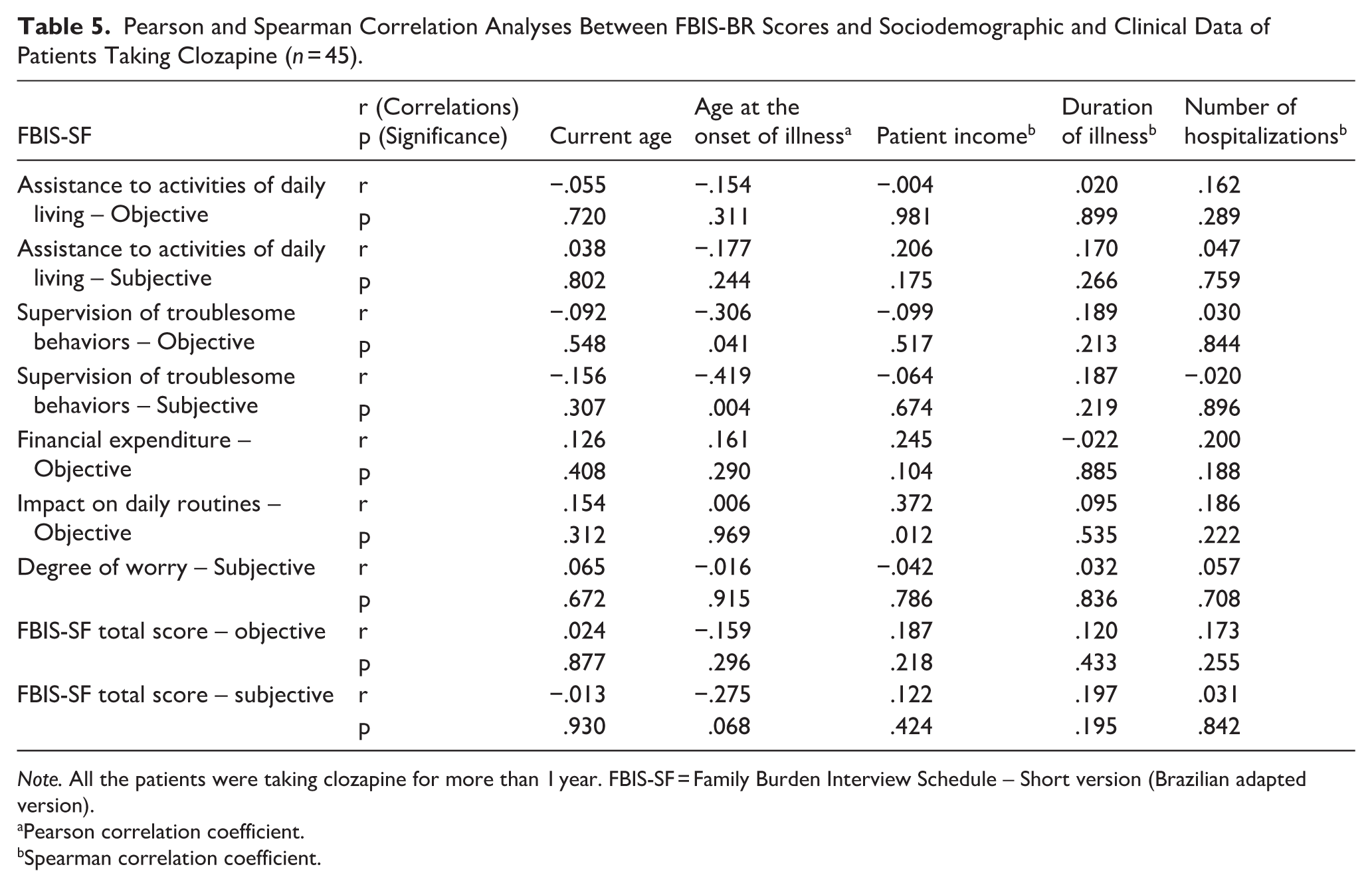
Note. All the patients were taking clozapine for more than 1 year. FBIS-SF = Family Burden Interview Schedule – Short version (Brazilian adapted version).
Pearson correlation coefficient.
Spearman correlation coefficient.
In the other antipsychotics group, the age at onset of illness had a negative correlation with the subjective burden in the assistance to daily life, subjective and objective burden of supervision of troublesome behaviors, and impact on the daily routines: younger ages were correlated with higher burden. Eventually, the age at onset of the illness correlated with both subjective and objective total scores (Table 6).
Pearson and Spearman Correlation Analyses Between FBIS-BR Scores and Sociodemographic and Clinical Data of Patients Taking Other Antipsychotics (n = 15).
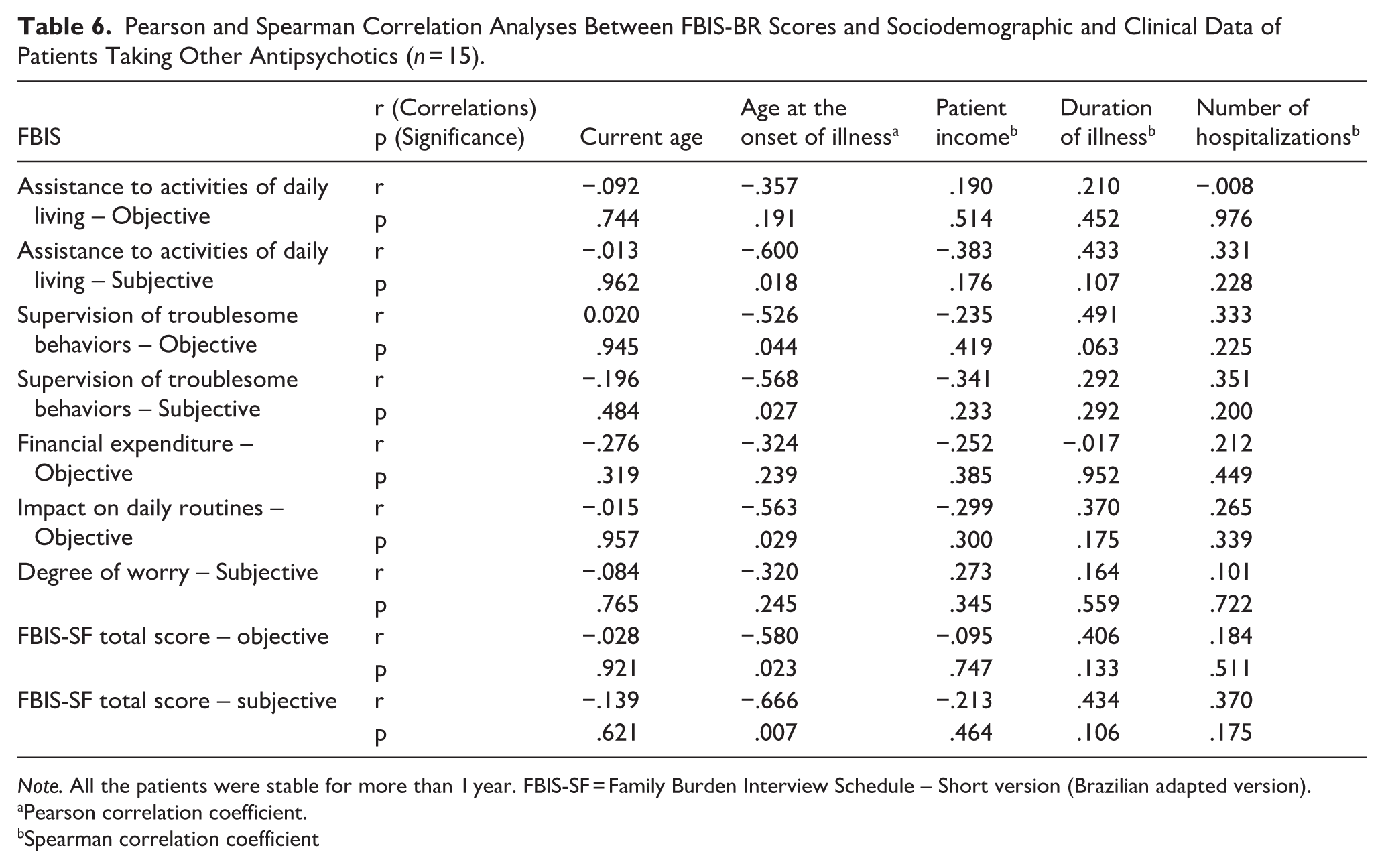
Note. All the patients were stable for more than 1 year. FBIS-SF = Family Burden Interview Schedule – Short version (Brazilian adapted version).
Pearson correlation coefficient.
Spearman correlation coefficient
In the clozapine group, the female gender correlated with the financial caregiver burden (Table 7), and among the other antipsychotics group, the female gender was correlated with a higher objective burden in the supervision of troublesome behaviors and the total objective score (Table 8).
FBIS-SF Scores by Gender in Clozapine Patients (Mean ± SD).
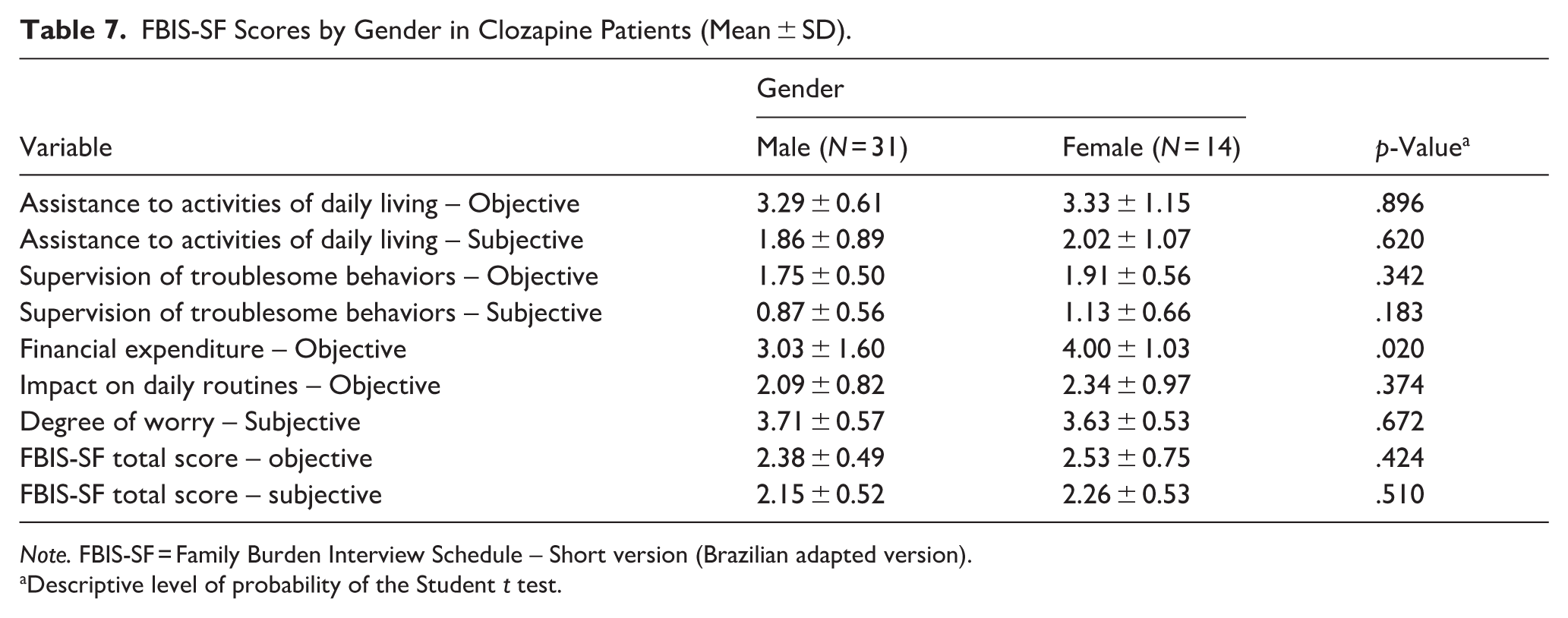
Note. FBIS-SF = Family Burden Interview Schedule – Short version (Brazilian adapted version).
Descriptive level of probability of the Student t test.
FBIS-SF Scores by Gender in Patients on Other Antipsychotics (Mean ± SD).
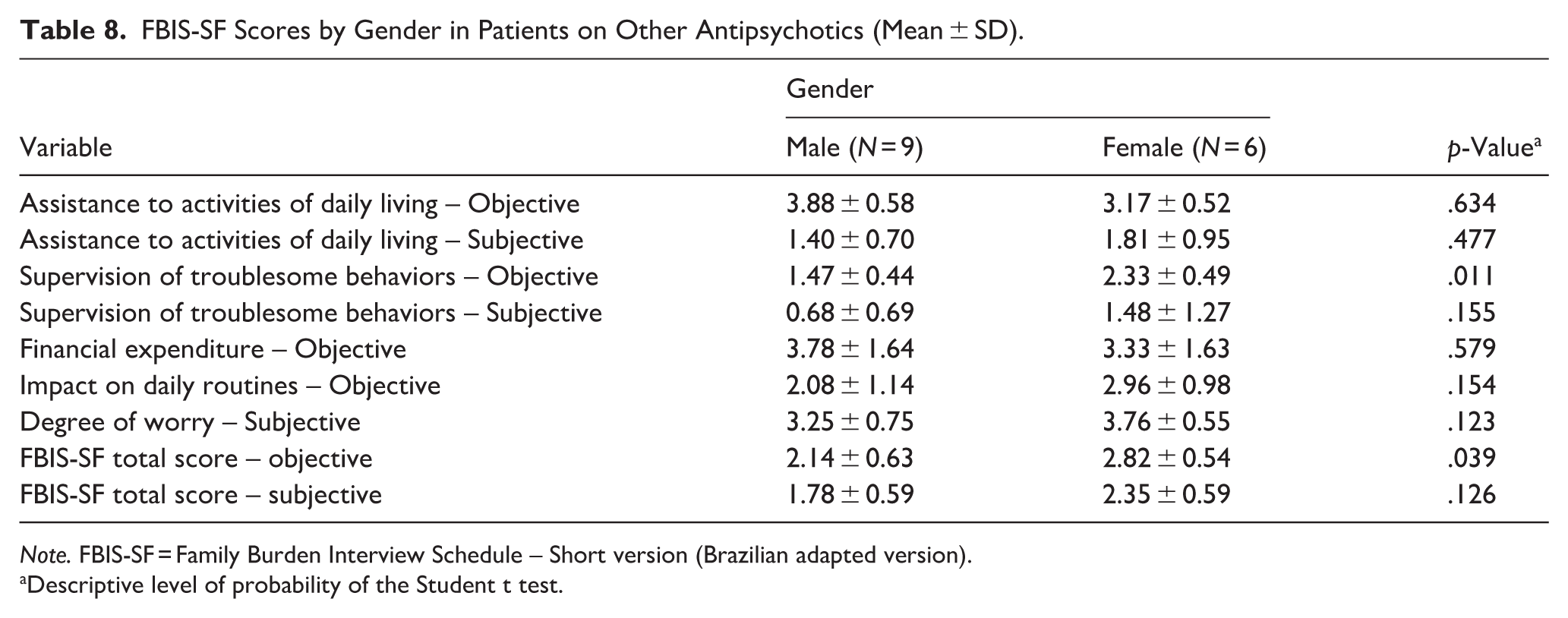
Note. FBIS-SF = Family Burden Interview Schedule – Short version (Brazilian adapted version).
Descriptive level of probability of the Student t test.
Receiving income from a social benefit program had a positive correlation with the burden of the impact on daily routines. The mean score (±SD) of the impact on daily routines was 2.60 ± 0.86 in the clozapine patients who were recipients of social benefits, and 1.90 ± 0.77 in those who did not have any social benefits. The other domains of the FBIS-SF did not correlate with social benefits programs. No correlation between social benefit and caregiver burden was found in the non-clozapine group.
The total PSP score was correlated with the burden of assistance in daily activities and the total objective burden in clozapine patients. No correlation between total PSP and caregiver burden was observed in the non-clozapine group.
Discussion
Our study is limited by the small sample size, particularly in the non-clozapine group, and the use of clozapine as a proxy for treatment resistance, rather than a clinical prospective diagnosis. Also, this was a post-hoc analysis of a cross-sectional study; therefore, we did not evaluate the treatment response. However, it is a specialized schizophrenia service where a standard protocol is followed for introducing clozapine in cases of TRS. Additionally, patients on clozapine exhibited higher scores on positive and total symptom scales, further supporting the diagnosis of TRS. The larger number of patients in the clozapine group reflects the nature of our service, which concentrates more TRS patients. A previous study conducted in our service in 2006 showed the same proportion of TRS patients as in our current sample (Henna Neto & Elkis, 2007).
Considering the use of clozapine as a proxy of treatment resistance, we expected a higher burden of care in this subgroup, caused by persistent psychotic symptoms (Brain et al., 2018; Kamil & Velligan, 2019; Velligan et al., 2019). However, both groups presented a similar level of burden, with a few differences. The factors associated with a higher burden of care in the clozapine group were: earlier disease onset, female gender, patient income, and total PSP score. In the non-clozapine group, the caregiver burden was associated with age at disease onset and female gender.
The caregiver burden associated with earlier disease onset aligns with existing literature (Hajebi et al., 2019; Mantovani et al., 2016; Strunoiu et al., 2019).
We would expect to see a negative correlation between patient income and caregiver burden (Wang et al., 2025; Yazici et al., 2016). However, in the clozapine group, we observed the opposite: higher patient income was associated with higher caregiver burden, particularly in terms of the impact on family routines. This paradox could possibly be explained by the fact that patients with TRS are more likely to qualify for continuous social security benefits due to the severity of illness. Consequently, in this particular cohort, a higher income may indicate a more severe clinical status and greater functional impairment. Moreover, higher income among patients with persistent symptoms could create a false sense of autonomy that is not aligned with their clinical condition. This discrepancy may lead to increased conflicts and a greater need for supervision, ultimately intensifying the burden on these patients compared to non-TRS.
Yazici et al. (2016) found the inverse relationship: an increase in income is generally associated with a decrease in caregiver burden. However, it is important to note that Yazici et al. did not evaluate patients with TRS.
The correlation of female gender with higher family burden was somewhat unexpected and merits further research. In fact, male patients are usually reported to cause more burden (Yu et al., 2017). The factors underlying this finding are unclear; however, we propose several hypotheses for future investigation.
Psychosis affects men and women differently, particularly regarding parenting roles and sexuality (Firmin et al., 2021; Seeman, 2012). Men with schizophrenia often lose their sexual drive and may abstain from sexual activity. In contrast, women with schizophrenia may lead active sexual lives but are particularly vulnerable to sexual abuse and unplanned pregnancies. Additionally, women with schizophrenia face a significantly increased risk of sexual or violent traumatization, both inside and outside their homes (Seeman, 2012). Another possibility is that in Brazil, the home environment often means that care for elderly parents is managed partially or entirely by family members, with women, especially daughters, taking on a prominent role in this caregiving. When these women become ill, their caregiving role may be left unfilled. These gender-specific issues could potentially increase the burden of care on families.
Although females imposed an increased caregiver burden, the small sample size of our study did not allow us to make further stratifications for confounders.
In our study, the majority of caregivers (55%) were mothers and only three were spouses. Previous studies reported that female caregivers have a higher level of burden than male caregivers (Yu et al., 2017).
The lack of a significant difference in burden between the clozapine and non-clozapine groups suggests that long-term stabilization with clozapine may play a role in mitigating the high burden typically expected in treatment-resistant cases. However, this is a speculative hypothesis that should be explored in future studies. Verma et al reported a reduction in the burden of caregivers of patients with TRS treated with clozapine for at least 3 months (Verma et al., 2021).
The high levels of burden observed in our sample align with previous studies in Latin American contexts, which also used the FBIS-BR, where family members often remain the primary source of support for patients with schizophrenia due to cultural values of family cohesion and gaps in formal community care services (Albuquerque et al., 2010; Barroso et al., 2009; Eloia et al., 2018).In addition, the history of adverse life events can be a residual confounder in this study.
In conclusion, caregivers of people with schizophrenia experience a high level of burden; age of disease onset, female gender, low functioning, and receipt of social benefits might be associated with increased caregiver burden among those caring for patients taking clozapine. Further studies with a larger sample size of TRS schizophrenia should shed light on our observations.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MRL has served on advisory boards for Boehringer-Ingelheim, Johnson & Johnson, and Apsen. He has received support for the development of scientific and educational materials from Libbs, Adium, Apsen, EMS, and Takeda, as well as lecture fees from Takeda and Apsen. MK was an employee of M8 Pharmaceuticals during the study and is currently employed by Bristol Myers Squibb (BMS). EDS declares no conflicts of interest. The authors affirm that these interests have no bearing on the present study.