
Abstract
Background:
The COVID-19 pandemic severely impacted mental health, including that of gay, bisexual, and other sexual minority men (SMM). Few studies in the US have assessed stigma’s role in shaping the mental health of historically marginalized populations during crises.
Methods:
An online sample of 10,130 SMM completed the 2019 American Men’s Internet Survey; of these, 1,051 completed a follow-up survey in April, and 572 completed a second follow-up survey in July 2020, meaning 572 completed all three surveys. Using this analytic sample (N = 572), we examined the association between sexuality-based stigma (stigma from family and friends, anticipated healthcare stigma, general social stigma) in the preceding 6 months and increases in anxiety symptoms from April to July 2020 in linear regression models. Economic insecurity and pre-existing psychological distress were considered potential moderators, and we used stratification to examine differences in associations by age.
Results:
Mean age was 42 years; 74% of participants (n = 425) were non-Hispanic white, and 84% (n = 482) identified as gay. Greater pre-pandemic general social stigma predicted an increase in anxiety symptoms among SMM overall (adjusted-beta[95% CI] = 0.65[0.26, 1.04]). This increase was amplified among those with greater pre-pandemic psychological distress (adjusted-beta = 0.08[0.01, 0.16]) and specifically among those aged 25 to 44 (adjusted-beta = 0.11[0.01, 0.22]) and 45 to 64 (adjusted-beta = 0.32[0.13, 0.51]). Among SMM aged 16 to 24, greater pre-pandemic stigma from family and friends augmented increases in anxiety among those with greater pre-pandemic psychological distress (adjusted-beta = 0.13[0.03, 0.23]).
Conclusions:
During the initial COVID-19 lockdown, sexuality-based stigma predicted anxiety increases among SMM, increases that were amplified by pre-existing psychological distress and that varied by age. Linking SMM with these vulnerabilities (recent stigma, current distress, young age) to services now and making preparations to link SMM to services later may help mitigate the adverse mental health effects of future national crises.
Introduction
Concerns about the psychological effects of surviving COVID-19 have proliferated, given elevated prevalence of mental health difficulties worldwide during the pandemic (Hossain et al., 2020; Płomecka et al., 2020; Ren et al., 2020; Zhou et al., 2020). Increases in psychological distress from March to April 2020 coincided with the emergence of COVID-19 and subsequent lockdowns (Daly & Robinson, 2021). A report from the Centers for Disease Control and Prevention demonstrated that, among adults in the United States (US), June 2020 anxiety and depression prevalence were roughly three (25.5% vs. 8.1%) and four times (24.3% vs. 6.5%) what were reported in the second quarter of 2019, respectively, with suicidal ideation increasing from 4.3% in 2018 to 10.7% in 2020 (Czeisler et al., 2020). Risk factors for general psychological distress during the early phase of the pandemic included pre-existing psychiatric conditions and reduced social interactions (Hossain et al., 2020; Płomecka et al., 2020; Ren et al., 2020), as well as economic insecurity (e.g., unemployment, food insecurity, housing instability; Mojtahedi et al., 2021; Posel et al., 2021; Ruengorn et al., 2021).
Gay, bisexual, and other sexually minoritized men (SMM) comprise one of the communities at risk for increasing health inequities during COVID-19 (Pan et al., 2021; Santos et al., 2021). Though COVID-19-related job loss (11%) and food insecurity (19%) among SMM have been comparable to that of other adults (Czeisler et al., 2020; Wohl et al., 2013), risk for adverse mental health outcomes has been exacerbated by SMM-specific risk factors, such as reduced coping resources secondary to minority stress, disrupted social support secondary to social distancing measures, and higher pre-existing prevalence of mental disorders (Batchelder et al., 2021; Charlton et al., 2018; Sanchez et al., 2020; Santos et al., 2021).
Additional SMM-specific risk factors include experiences of stigma and associated poor mental health (Babel et al., 2021; Stahlman, Sanchez, et al., 2016; Wiginton, Murray, Augustinavicius, et al., 2022). Sexuality-based stigma, which can be internalized (e.g., one may adopt a negative view toward SMM and turn that view inward, toward themselves), anticipated (e.g., one may expect to be judged or ridiculed upon disclosure or discovery of their sexuality), perceived (e.g., one may believe that they and other sexual minorities like them are devalued in the community in which they live), or enacted (e.g., one may be denied services or physically attacked on account of their sexuality) as a result of one’s sexual identity, behavior, or attraction (Stahlman et al., 2017), is a strong predictor of high vulnerability for adverse mental health outcomes in this community (Hatzenbuehler & Pachankis, 2016; Stahlman, Grosso, et al., 2016; Wohl et al., 2013). However, few studies have examined how past experiences of stigma may shape mental health responses to crises such as COVID-19. Elucidating these associations can inform efforts on strategic population targeting for intervention strategies to mitigate negative mental health impacts in the early phase of future crises.
Factors such as pre-existing mental distress and pandemic-related economic insecurity that have been found to shape pandemic mental health in the general population may also shape how stigmatized populations experience mental health impacts in COVID-19-like crises, as these factors may create different levels of preparedness to cope with emerging economic and psychological challenges (Sanchez et al., 2020; Santos et al., 2021). Age may similarly affect coping preparedness. Sexuality-based stigma has been shown to negatively correlate with age in some research with SMM (Wohl et al., 2013), while younger age has been associated with poorer mental health due to less access to supportive resources and a relative lack of experience coping with stressful situations (Ferraz et al., 2021).
We sought to answer the following research questions: (1) Were pre-pandemic experiences of sexuality-based stigma associated with anxiety symptom changes during the early course of COVID-19 among SMM in the US? (2) If so, was this association moderated by economic insecurity and pre-existing psychological distress, and (3) do these associations vary by age? We hypothesized that past experiences of sexuality-based stigma would predict increases in anxiety symptoms and that these associations would differ by pandemic-related economic insecurity and pre-existing distress, as well as across age strata. Findings can facilitate pandemic preparedness and response by supporting tailored, targeted, and evidence-based intervention and programming efforts, including making mental health support services accessible to SMM.
Methods
Recruitment and Participants
The American Men’s Internet Survey (AMIS) is an annual cross-sectional web-based behavioral survey of SMM in the US. SMM are recruited through convenience sampling using banner advertisements and email blasts (Sanchez et al., 2020; Wiatrek et al., 2021; Zlotorzynska et al., 2017). Eligibility criteria included being cisgender male, being ⩾15 years, US residence, and past oral or anal sex with a male partner or gay/bisexual-identification if a minor. SMM who participated in the 2019 round of AMIS data collection (August-December 2019) and provided an email address for being re-contacted were invited via email to participate in a COVID-19 impact survey in April 2020. A survey link in the email re-assessed eligibility and obtained informed consent. April 2020 participants who provided an email address for additional follow-up were contacted in July 2020 to complete a second COVID-19 impact survey, before which eligibility was confirmed and consent was obtained again. The same consent procedures were followed for those under 18 years, as the process of assent plus adult consent was waived by the institutional review board given the sensitive nature of the survey. No incentives were provided. This secondary analysis of de-identified data was deemed exempt by the Johns Hopkins University Institutional Review Board.
It is important to note that AMIS is not a longitudinal survey. We implemented the COVID-19 follow-up surveys rapidly in response to the emerging pandemic with participants from our existing convenience sample from the 2019 cycle of AMIS. Therefore, we did not perform a formal a priori sample size calculation. The analytic sample size reflects all eligible participants who agreed to be re-contacted and who completed the follow-up surveys during the study period.
Measures
Anxiety During COVID-19
Study outcome was change in anxiety level from April to July 2020, which was assessed via the Generalized Anxiety Disorder assessment (GAD-7; Spitzer et al., 2006). The GAD-7 consists of seven items that ask about frequency of occurrence of symptoms over the past 2 weeks with a 4-point Likert type response scale: “Not at all” (0), “several days” (1), “over half the days” (2), and “nearly every day” (3). The GAD-7 has been validated in the general US adult population (Löwe et al., 2008). Internal consistency was excellent (α = .91, April; α = .93, July). We calculated sum scores in April and July, with values ranging from 0 (no anxiety experienced) to 21 (highest level of anxiety), and used the difference to reflect anxiety change (assessed April, July 2020; see Table S1).
Pre-Pandemic Sexuality-Based Stigma
Sexuality-based stigma was measured during the 2019 AMIS data collection cycle using 13 items (e.g., “Have you been excluded from family activities because you have sex with men?”; see Appendix A for all items). The answer of “Yes, experienced in the past 6 months” was assigned a score of 1, while “Yes, but not in the past 6 months” and “No” were assigned a score of 0. Items were separated into three subscales: stigma from family and friends (items 1–3); anticipated healthcare stigma (items 4–5); and general social stigma (items 6–13; Augustinavicius et al., 2020; Wiginton, Murray, Algarin, et al., 2022; Wiginton, Murray, Augustinavicius, et al., 2022). Mean stigma subscale scores were calculated, and to increase interpretability, we scaled-up the scores by a factor of 10 resulting in values from 0 to 10, with higher values indicating greater pre-pandemic sexuality-based stigma (assessed 2019).
Pre-Pandemic Psychological Distress
Pre-pandemic psychological distress was measured by the Kessler-6 (K6) scale. The K6 asks about frequency of occurrence of six symptoms (e.g., “feeling nervous”) in the past 30 days (Furukawa et al., 2003). Answers were coded from 0 to 4: “None of the time” (0), “A little of the time” (1), “Some of the time” (2), “Most of the time” (3), and “All of the time” (4). A K6 sum score was calculated to represent the psychological distress level for each participant (range = 0–24), with higher scores indicating greater distress. Internal consistency was excellent (α = .90; assessed 2019).
Economic Insecurity
Participants were asked three questions to evaluate COVID-19’s impact on financial stability: (1) Do you feel that difficulty buying food has changed during COVID-19? (2) Do you feel that difficulty paying rent has changed during COVID-19? (3) Have you lost your job, or one of your jobs because of COVID-19? For the first two questions, participants could select among three answer choices: “has decreased because of COVID-19,” “has not changed or changed for reasons other than COVID-19”, and “has increased because of COVID-19.” For the job loss item, participants could select from “Yes, because of COVID-19,” “No,” and “Yes, but because of something other than COVID-19.” We recoded all three questions as binary variables that took values of “increased difficulty due to COVID-19” versus “decreased or unchanged” (for food and rent), or “lost job due to COVID-19” versus “no or lost for other reasons” (for job loss). In case these challenges were rarely endorsed, the three items were combined into one binary variable, indicating whether participants “experienced any financial challenges due to COVID-19” versus “not experienced any challenges or challenges were due to other reasons” (assessed April 2020).
Demographics
We included age, race/ethnicity, and annual household income reported in April 2020 as potential confounders. Race and ethnicity were combined into one categorical variable that took one of four values: non-Hispanic Black, Hispanic or Latinx, non-Hispanic white, and another race or multiracial. In the stratified analysis, we categorized the study population into four age groups (16–24, 25–44, 45–64, and ⩾65) to represent generations with potentially different work experience and mental health status. We also collected data on sexual identity, which we provide descriptively.
Analysis
A directed acyclic graph (DAG) illustrating hypothesized associations among constructs of interest is presented in Figure 1. We used separate bivariate and multivariable linear regression models to assess unadjusted and adjusted associations between past experiences of each sexuality-based stigma domain and change in anxiety symptoms. Next, we added interaction terms between each stigma subscale score and the two potential moderators to the adjusted models to determine the extent to which economic insecurity and pre-existing distress moderated stigma-anxiety change associations. Lastly, we stratified the study population by age group and re-examined the same associations in the former multivariate models (with and without interaction terms) to assess whether associations varied by age. As not all participants who took the COVID-19 survey in April re-took the survey in July, we performed a sensitivity analysis using inverse probability weighting (IPW) to adjust for the probability a participant took part in the July survey. The significance threshold for all analyses was α = .05. Missingness was low for all variables (<5% for income; <2% for GAD-7; <1% for all other variables); no data were imputed. Data cleaning was conducted in Stata 14.1 (StataCorp LLC, College Station, TX), and analyses were performed in R Statistical Software (version 4.1.2; R core Team, 2021).
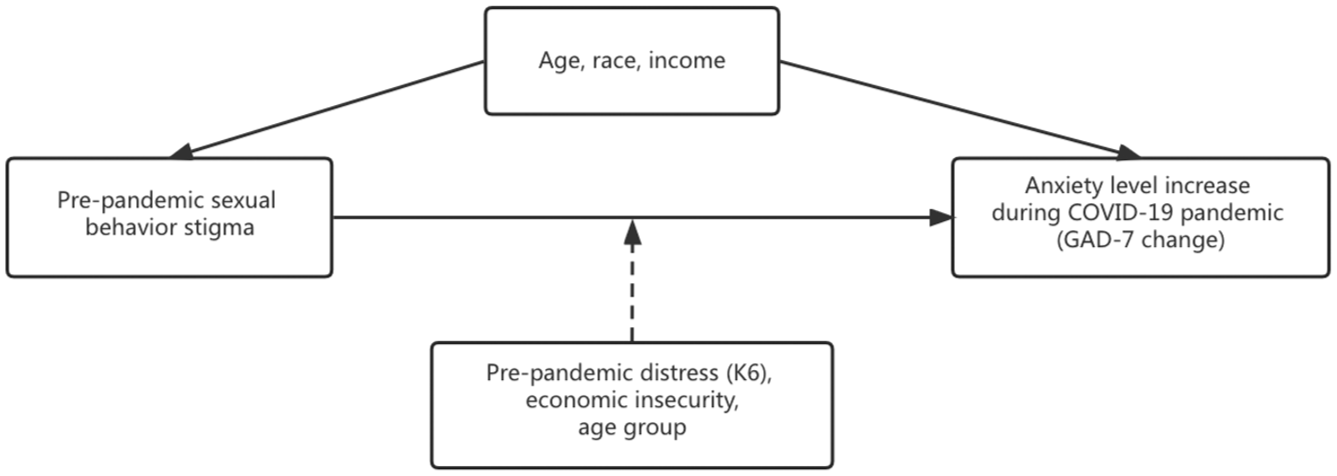
Directed acyclic graph (DAG) depicting the analytic relationships of interest.
Results
Sample Characteristics
Of the 10,130 SMM in the 2019 AMIS cycle, 1051 (10.4%) completed the April 2020 COVID-19 survey, among which 572 (54.4%) were surveyed again 3 months later (Table S2). Compared with those lost to follow-up after the April survey (n = 479, 45.6%), SMM retained in the July survey tended to be older and non-Hispanic white, with fewer pandemic-related financial challenges and sexuality-based stigma experiences. We included only SMM who took the April and July COVID-19 survey in the main analysis for this study and linked them with their 2019 survey data (N = 572).
At baseline, age ranged from 16 to 83 years, with a mean of 41.9 years (SD = 15.9) and with 44.1% aged between 25 to 45 years. A substantial proportion of the participants (n = 425, 74.3%) reported being non-Hispanic white, followed by 74 (12.9%) who reported being Hispanic or Latinx and 38 (6.6%) who reported being non-Hispanic Black (Table 1). Most identified as gay or homosexual (n = 482, 84.3%), with a minority identifying as bisexual, pansexual, or queer (n = 84, 14.7%; not displayed).
Characteristics of the Study Population, Overall and Stratified by Age Group.
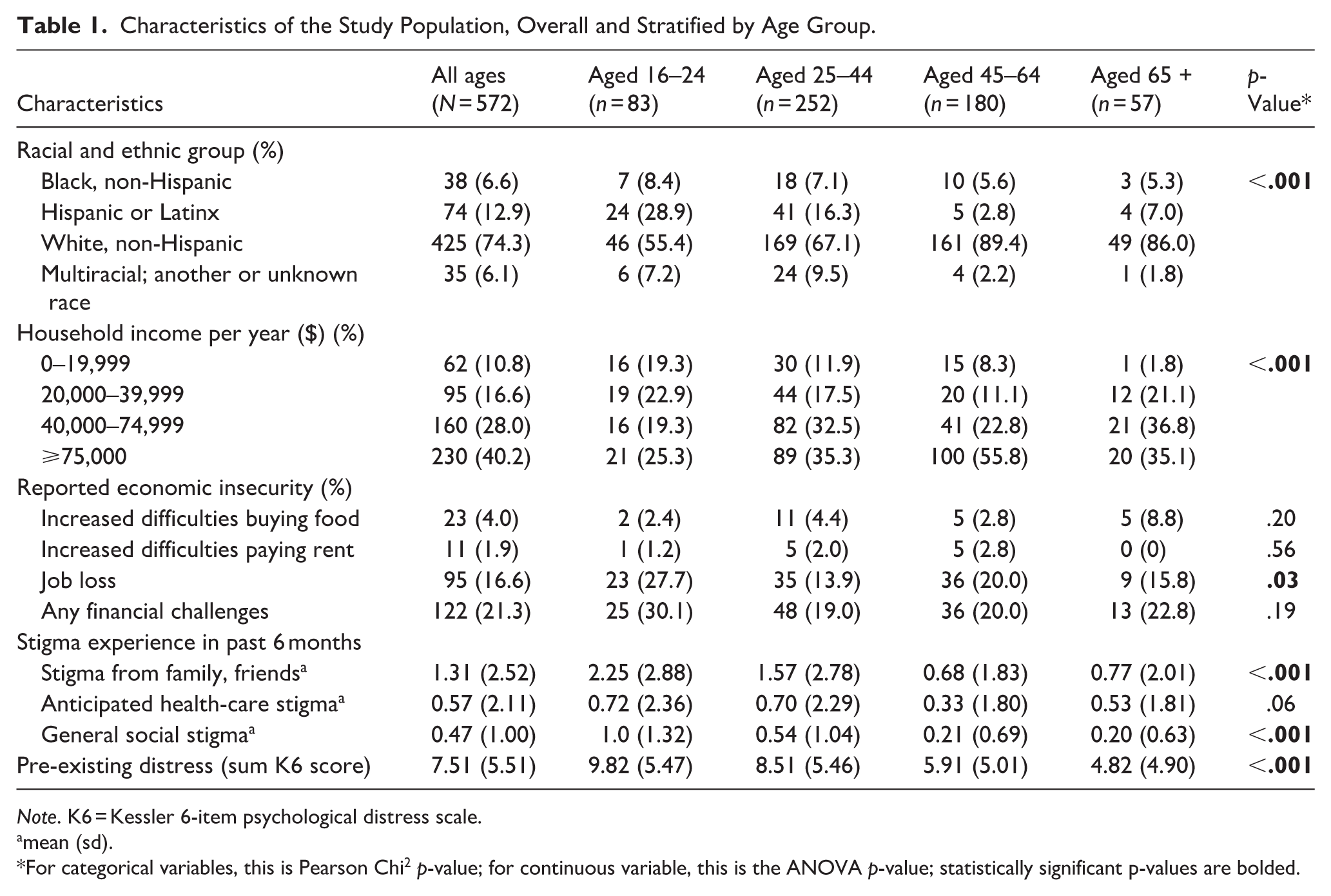
Note. K6 = Kessler 6-item psychological distress scale.
mean (sd).
For categorical variables, this is Pearson Chi2 p-value; for continuous variable, this is the ANOVA p-value; statistically significant p-values are bolded.
About half of participants (n = 264, 46.2%) reported experiencing any sexuality-based stigma from family and friends, 93 (16.3%) reported any anticipated healthcare stigma, and 277 (48.4%) reported any general social stigma in the 6 months prior to the 2019 AMIS survey. Stigma from family and friends was highest (mean = 1.31, SD = 2.52) among the three subscales, followed by anticipated health-care stigma (mean = 0.57, SD = 2.11) and general social stigma (mean = 0.47, SD = 1.00).
Job loss was the most commonly endorsed of the three economic challenges caused by COVID-19 (n = 95, 16.6%), followed by increasing difficulties buying food (n = 23, 4.0%) and paying rent (n = 11, 1.9%). Approximately one out of five participants (n = 122, 21.3%) reported at least one economic challenge.
Compared to older participants, younger participants were comprised of a higher proportion of Hispanic or Latinx men and a lower proportion of non-Hispanic white men, a higher proportion of those earning <$40,000 annually, and higher pre-pandemic sexuality-based stigma scores (all p < .001).
Stigma as a Predictor of Change in Anxiety Symptoms
In the full, non-stratified sample, GAD-7 scores increased on average from 6.11 in April to 6.26 in July (p > .05). GAD-7 increases for 16 to 24, 25 to 44, 45 to 64 and 65+ age groups were 0.52 (95% CI = [−0.45, 1.50]), 0.08 [−0.48, 0.63], 0.13 [−0.52, 0.78] and 0.02 [−1.04, 1.09], respectively.
In non-stratified models, greater pre-pandemic general social stigma predicted significant anxiety increases (adjusted-beta[95% CI] = 0.65[0.26, 1.04]; Table 2). In age-stratified models, greater pre-pandemic general social stigma predicted significant anxiety increases among 25 to 44- and 45 to 64-year-olds, with adjusted-betas of 0.62 [0.08, 1.15] and 1.28 [0.33, 2.24], respectively. Greater pre-pandemic stigma from family and friends predicted non-significant anxiety increases overall (adjusted-beta = 0.09[−0.07, 0.25]), which was also observed across age strata (adjusted-betas = 0.06 to 0.57[−0.10, −0.34] to [0.33, 1.26]). Greater pre-pandemic anticipated healthcare stigma predicted non-significant anxiety decreases overall (adjusted-beta = −0.13[−0.31, 0.05]) and in most age strata (adjusted-betas = −0.35 to 0.01[−0.85, −0.33] to [0.14, 0.60]; Table 2).
Associations Between Increase in Anxiety Symptoms April to July 2020 and Past Experience of Sexuality-Based Stigma Among SMM in the US.

Note. SMM = sexual minority men; US = United States; b = beta; CI = confidence intervals.
Adjusted for confounders (age, race and ethnicity, and household annual income).
p-Value < .05; Bold indicates significant values.
In non-stratified interaction models, greater pre-pandemic general social stigma amplified anxiety increases among SMM with greater pre-pandemic psychological distress (adjusted-beta = 0.08[0.01, 0.16]). This trend was also observed among SMM aged 25 to 44 (adjusted-beta = 0.11[0.01, 0.22]) and 45 to 64 (adjusted-beta = 0.32[0.13, 0.51]), but the reverse was seen among SMM aged 16 to 24 (adjusted-beta = −0.35[−0.65, −0.06]), such that pre-pandemic general social stigma tempered anxiety increases among SMM with greater pre-pandemic psychological distress. Among SMM aged 16 to 24, greater pre-pandemic stigma from family and friends augmented anxiety increases over time among those with greater pre-pandemic psychological distress (beta = 0.13[0.03, 0.23]), but tempered anxiety increases among those experiencing pandemic-related economic insecurity (beta = −1.65[−2.73, −0.58]; Table 3).
Associations Between Increase in Anxiety Symptoms April to July 2020 and Past Experience of Sexuality-Based Stigma Among SMM in the US.
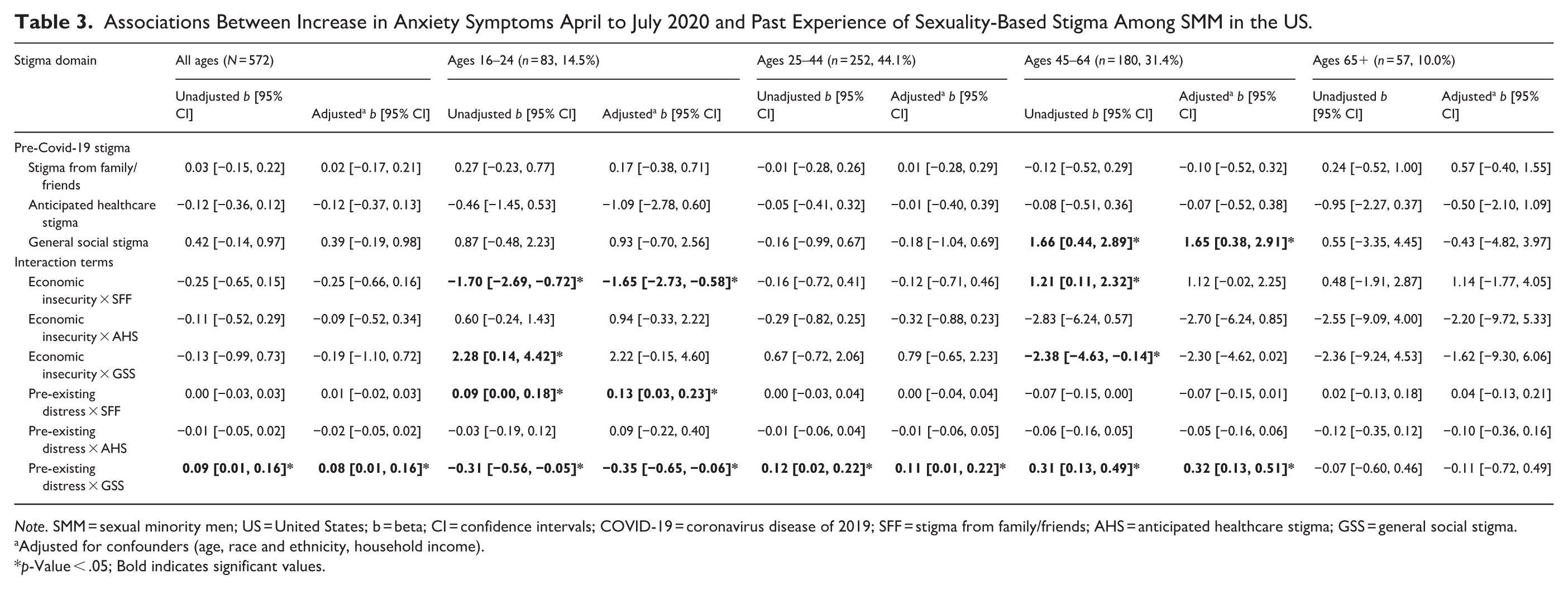
Note. SMM = sexual minority men; US = United States; b = beta; CI = confidence intervals; COVID-19 = coronavirus disease of 2019; SFF = stigma from family/friends; AHS = anticipated healthcare stigma; GSS = general social stigma.
Adjusted for confounders (age, race and ethnicity, household income).
p-Value < .05; Bold indicates significant values.
Sensitivity Analysis
After adjusting for the probability that a participant took the July survey, the results were comparable to those in the main analysis (Tables S3–S4).
Discussion
We sought to examine whether pre-pandemic sexuality-based stigma predicted anxiety changes, whether pre-existing psychological distress and pandemic-related insecurity moderated this association, and whether these associations differed by age. We found that pre-pandemic experiences of sexuality-based stigma were associated with increases in anxiety symptoms during the initial lockdown period (April–July, 2020). We further found that these associations were moderated by pre-existing psychological distress and pandemic-related economic insecurity, and that the magnitude and significance of these associations differed across age strata. Importantly, these findings reflect the small proportion of participants who self-selected to complete all three surveys and should be considered in light of this information. While numerous other studies have examined the impact of COVID-19 on the mental health of SMM and other queer populations in the US (Fish et al., 2021; Ruprecht et al., 2021; Salerno et al., 2020), ours is among the first to examine the role of sexuality-based stigma in this context.
Greater pre-pandemic general social stigma predicted anxiety increases overall and among those aged 25 to 44 and 45 to 64 years specifically. Greater pre-pandemic psychological distress amplified anxiety increases overall and among those aged 25 to 44 and 45 to 64 years. These findings may reflect interconnected aspects of the same phenomenon. That is, experiences like those comprising general social stigma – healthcare mistreatment, police refusal to help, harassment, violence – can generate psychological distress (Marti-Pastor et al., 2020; Wiginton, Baral, et al., 2025; Wiginton et al., 2023) that could have heightened vulnerability to further adverse psychological reactions or to an exacerbation of pre-existing distress in the face of major stressors like COVID-19 (Hatzenbuehler, 2009; Meyer, 2003; Murphy et al., 2021). The same participants who endorsed both pre-pandemic general social stigma and psychological distress may have experienced this psychological distress in response to general social stigma, which may be the source of the observed associations. This would help explain why the stratified (i.e., greater experiences of pre-pandemic general social stigma predicting anxiety increases among those aged 25–44 and 45–64 years) and moderated associations (i.e., amplified anxiety increases in these age strata among those with greater pre-pandemic psychological distress) remained in the same age groups.
That this effect was confined to the two middle age groups may reflect the lack of statistical power in strata with smaller sample sizes. Alternatively, for the oldest SMM in this sample, this effect could be due to this group’s having the smallest increase in anxiety symptoms compared to all other age groups (+0.02 vs. +0.08–0.52). For the youngest SMM, the lack of an effect of pre-pandemic general social stigma on anxiety increases could indicate reduced salience of general social stigma experiences compared to other stigma experiences (e.g., stigma from family and friends; see below) consistent with the relative influence of family and peers during this developmental period versus other interactions (Fish et al., 2021; Gonzales et al., 2020; Hanna-Walker et al., 2023). SMM in the middle age groups may have had more opportunities to encounter general social stigma in the previous 6 months than the youngest and oldest SMM and had less direct exposure to family interactions than the youngest SMM.
Ensuring that SMM are aware of and can conveniently and affordably access affirmative mental health services, including in-person and telehealth services, before national crises hit is imperative. Scholars, community organizations, and advocates can work together to link SMM to such services, or at least make SMM aware of their existence, and create a partnership of sorts between SMM communities and mental health service organizations to ensure plans for mental health service access and utilization are in place when crises strike. SMM with pre-existing risk factors for distress exacerbation, such as sexuality-based stigma experiences, psychological distress, and middle age, merit special consideration in these efforts. Research is needed with larger samples of SMM younger than 25 years and older than 65 years to help clarify their risk.
Several findings emerged that were particular to the youngest age group only. Pre-pandemic stigma from family and friends amplified anxiety increases among those with greater pre-pandemic psychological distress. These relationships may be explained similarly to those above. Pre-pandemic stigma from family and friends may have caused the pre-pandemic psychological distress that was detected, and it is perhaps this pre-existing distress that heightened this group’s vulnerability to anxiety increases when confronted with the pandemic (Hatzenbuehler, 2009; Meyer, 2003; Murphy et al., 2021). Alternatively, those with pre-pandemic psychological distress may have been more likely to worry about returning to their biological family’s home or spending increased time at that home (due to pandemic-related challenges) where they may have encountered the same family or friends who stigmatized them previously (Fish et al., 2021; Gonzales et al., 2020; Hanna-Walker et al., 2023).
Two unexpected findings in this age group also emerged. First, greater pre-pandemic general social stigma predicted anxiety decreases among those with pre-pandemic psychological distress. It is possible that pre-pandemic general social stigma led to pre-pandemic psychological distress, and that protective isolation from general social stigma led to anxiety decreases, though this cannot be confirmed with the data. It is also possible that these individuals developed coping skills from prior experiences of stigmatization and psychological distress (Aldao et al., 2010; Bonanno et al., 2004; Hatzenbuehler, 2009; Meyer, 2003), which they were able to utilize in the midst of the pandemic to reduce anxiety. The second unexpected finding was that greater pre-pandemic stigma from family and friends predicted anxiety decreases among those who encountered pandemic-related economic insecurity. Stigmatization by family among SMM commonly manifests as or leads to physical and financial rejection (Gattis, 2013; Goldbach et al., 2014; Ryan et al., 2009). SMM accustomed to such stressful scenarios could have already developed strategies and coping skills to manage financial uncertainty and therefore mitigate anxiety caused by pandemic-related economic concerns (Aldao et al., 2010; Bonanno et al., 2004). Our interpretations of these unexpected, perhaps counterintuitive findings should be considered with caution, as they are of course speculative and cannot be proven from the data we have.
The youngest age group endorsed the highest levels of each form of sexuality-based stigma, the lowest income level, the greatest pandemic-related economic challenges, the highest level of pre-existing psychological distress, and the largest increase in anxiety during the early months of the pandemic. These findings reflect growing concerns of a mental health crisis among young SMM and underscore the potential vulnerability to the impacts of major stressful life events in this age group, pointing to a critical need to prioritize mental health and other psychosocial supports for young SMM (Carstensen et al., 2011; Halkitis et al., 2015; Zhou et al., 2020). Targeted interventions dedicated to young SMM – particularly those who may be residing in environments where they could be stigmatized by biological family and/or friends – are warranted, with special consideration needed for ensuring services are affordable and insurance-related challenges are addressed (e.g., avoiding utilization of parents’ insurance; one’s mental health service utilization being billed to parents’ insurance). Pairing economic-programming with mental health intervention efforts would further support this age group, given the likelihood of reduced economic independence. Holistic, person-centered care, such as psychosocial wraparound programming, may be most helpful for this group.
It is important to note that the increases in anxiety we documented, though statistically significant, were below commonly used thresholds indicative of clinical significance (Bischoff et al., 2020; Toussaint et al., 2020), though they do reflect findings from other longitudinal studies tracking anxiety during the early months of the pandemic (Amendola et al., 2021; Essadek et al., 2025). Small mean changes in symptom scores at the individual-level can still have public health relevance, as they could signal an upward shift in the proportion of individuals in a population crossing established clinical thresholds (Raza et al., 2018). That is, for the SMM population, which experiences elevated baseline anxiety on account of minority stress, modest increases in symptom scores may represent an amplification of distress at the population level, potentially increasing the proportion of SMM experiencing clinically significant anxiety. Moreover, from a public health perspective, understanding even small effects of a large-scale crisis on the mental health of a population are important to track, and documenting that these increases are selectively rather than universally experienced in this population provides direction on where to target intervention efforts.
Limitations
The findings of this study should be considered in light of limitations. Timing of the COVID-19 surveys might have been unable to fully capture changes in pandemic mental health. The first survey took place right after lockdown, while the second happened when the initial spike of cases began to level-off and several states were making plans to reopen (Gao et al., 2020; Tang & Wang, 2020). This would possibly miss anxiety fluctuations that may have occurred prior to the initial decline in cases that may have been associated with emotional recovery. Moreover, distress likely fluctuated greatly over subsequent waves, and in the longer term more sustained increases in distress may have occurred. Thus, our study may underestimate increases in anxiety experienced over the broader course of the pandemic. This could have simultaneously been advantageous, providing a glimpse of how SMM reacted and responded during the early stages of a major crisis, yielding insights into how to target resources in crises.
Previous literature has observed a decreasing trend in levels of stress, anxiety, and depression from April to May 2020 in the US (Zhou et al., 2020). However, as the pandemic was evolving quickly during the early months of 2020, factors (lockdown measures, increasing death tolls, increased testing with regularly reported case numbers in neighborhoods and among family members) could have influenced how individuals perceived emerging challenges and risks, causing difficulty in determining what time point should have been used for survey administration. More refined results could be derived from longitudinal studies with more visits over a longer time span. An additional consideration is that this sample was recruited online through convenience, self-selection strategies; thus, the findings might not be generalizable to all SMM, particularly those who may have limited access to or low use of online modalities. Effects may have been attenuated in the current sample, given that stigma levels were higher among those who did not complete both surveys and given research showing SMM with greater stigma may be less engaged in research (Parchem & Molock, 2021; Wiginton, Ortiz, et al., 2024).
Those who participated may have also been more likely to have greater interest in health-related topics or be less occupied by emerging personal challenges and mental health difficulties than those who did not participate. Relatedly, those who were retained in the follow-up survey tended to be older and non-Hispanic white, with fewer pandemic-related economic challenges and stigma experiences. Racial/ethnic minority groups were also under-represented in the sample. These factors severely limit the extent to which our findings may be generalizable. Moreover, this under-representation, combined with the focus on assessing stigma based on sexuality only (rather than also assessing, e.g., racial/ethnic minority stigma or intersecting stigmas), may be particularly consequential for understanding anxiety fluctuations and the relationships examined here for Black and Asian SMM. In the US, Black populations face ongoing racial stigma and stressors, while Asian populations – especially during the pandemic – were subjected to heightened racism stemming from rhetoric and discourse linking them to COVID-19. Our findings may therefore not accurately capture the mental health experiences of these populations. Targeted oversampling of these groups is imperative for better documenting their experiences and challenges so that resources for tailored programming may be allocated more strategically.
Finally, all measures were self-reported and subject to social desirability bias that could have led to underreporting of distress and stigma experiences, and we were unable to assess changes in other relevant outcomes such as depression.
Conclusions
Sexuality-based stigma experiences predispose SMM to adverse psychological reactions when confronted with major stressors, like the COVID-19 pandemic. Such crises that are nationwide in scope will have a wide reach, impacting the mental health of many SMM across the country, necessitating the integration of concrete, targeted programming to support mental health into pandemic- and other crisis-preparedness responses. Given the nature of crises like the COVID-19 pandemic, many marginalized populations may be in turmoil simultaneously and require resources when these crises hit, making it challenging to provide urgent mental health and other services to all in need. It is incumbent upon scholars, community organizers, and advocates to partner with local communities and policymakers to help ensure marginalized groups can access affirming, high-quality psychosocial support and other services in times of crisis.
Supplemental Material
sj-docx-1-isp-10.1177_00207640261456760 – Supplemental material for Pre-COVID-19 Sexuality-Based Stigma Predicts Mid-Pandemic Anxiety Increases in a Cohort of Sexual Minority Men in the United States
Supplemental material, sj-docx-1-isp-10.1177_00207640261456760 for Pre-COVID-19 Sexuality-Based Stigma Predicts Mid-Pandemic Anxiety Increases in a Cohort of Sexual Minority Men in the United States by John Mark Wiginton, Hanmeng Xu, Jason Lo Hog Tian, Qian-Li Xue, Stefan D. Baral, Travis H. Sanchez and Sarah M. Murray in International Journal of Social Psychiatry
Footnotes
Appendix A
Acknowledgements
The authors are grateful to participants for contributing their time and information to the survey.
Ethical Considerations
This secondary analysis of de-identified data was deemed exempt by the Johns Hopkins University Institutional Review Board #7006. Data are housed in a JHU stigma data repository, initially approved 3/23/2016, expiring 9/9/2027.
Consent to Participate
Participants provided online informed consent to complete the survey.
Author Contributions
JMW, supervision, writing – review and editing; HX, conceptualization, methodology, formal analysis, writing – original draft; JLHT, validation and writing – review and editing; QLX, methodology, supervision; SDB, funding acquisition, project administration, supervision, writing – review and editing; THS, funding acquisition, investigation, project administration, writing – review and editing; SMM, conceptualization, methodology, supervision, writing – review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the US National Institutes of Health grants P30MH136919 and R01MH132150. JMW received support from K01MD020565. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data for this study are not publicly available to protect confidentiality. Requests may be made to THS.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.