
Abstract
Depression is a significant risk factor for suicidal ideation, yet the mechanisms underlying this relationship remain unclear. Experiential avoidance and interpersonal needs, particularly perceived burdensomeness and thwarted belongingness, have been proposed as key mediators, but their relative roles in psychiatric inpatients are not well established. The objective of this study is to investigate whether experiential avoidance and interpersonal needs mediate the relationship between depression and suicidal ideation among psychiatric inpatients. This cross-sectional study included 151 psychiatric patients aged 18 years or older. Inclusion criteria were defined as recent suicide attempts accompanied by ongoing suicidal ideation or significant suicidal ideation. Data were collected using the Sociodemographic Form, Hospital Anxiety and Depression Scale, Acceptance and Action Questionnaire, Beck Scale for Suicide Ideation, and Interpersonal Needs Questionnaire with two subfactors: Perceived burdensomeness and thwarted belongingness. All measures showed statistically significant correlations with each other. The parallel three-mediator model further highlighted that the mediating role of perceived burdensomeness was more prominent than that of experiential avoidance, whose indirect effect alone was not significant. The results of this study may suggest that perceived burdensomeness is key to linking depression to suicidal ideation. Therapeutic approaches that strengthen social connectedness and reduce interpersonal distress may be particularly effective for managing suicidal ideation in psychiatric inpatients.
Introduction
The term suicide is derived from the Latin “sui caedere” (to kill oneself) and is defined as a destructive attempt aimed at ending one’s own life (Beck et al., 1979). Suicide is defined as death caused by self-directed injurious behavior with the intent to die because of the behavior. Suicidal ideation (SI) involves thinking about, considering, or planning suicide and refers to ending one’s life; it is a critical mental health concern with potentially fatal consequences if not promptly recognized and managed (NIMH, 2026; Rizvi et al., 2024; WHO, 2026). Suicide is often perceived as an escape from profound hopelessness, unmet needs, overwhelming stress, and helplessness. Suicidal experiences exist along a continuum, ranging from passive thoughts about death to active planning and impulsive actions (Naghavi, 2019). SI ranges from passive thoughts, such as wanting to be dead, to active thoughts, such as wanting to kill oneself (Liu et al., 2020). The severity of lifetime SI is a strong predictor of future suicide, which is understood as part of a continuum ranging from suicidal thoughts to completed suicide, making ideation an important clinical warning sign. A continuum extending from SI to completed suicide can be understood as a maladaptive, self-destructive coping mechanism (Chammas et al., 2022; Mundt et al., 2013). Most people cope effectively, but vulnerable individuals with poor coping skills favor escape-avoidance and confrontive strategies over problem-solving. Suicide cases show extreme avoidance and minimal problem-solving, linked to adverse childhood experiences and recent stressors. Maladaptive coping strategies escalate suicidality and worsen symptoms like distress, crisis risk, isolation, burdensomeness, rigid thinking, helplessness, and impaired problem-solving (Castillo et al., 2023; Liang et al., 2020; Pompili, 2024; Werbart Törnblom et al., 2021). SI is not limited to a Depressive Episode; it can be linked to suicide as a diagnostic criterion. Patients with many psychiatric disorders have higher SI rates and an increased risk of death by suicide. Bipolar disorder, psychotic disorders, and depressive disorder all show an increased suicide risk compared to the general population (Baldessarini & Tondo, 2020; Kim et al., 2025; Kang et al., 2024; Xu et al., 2023). Depressive symptoms were strongly linked to SI in individuals with bipolar disorder (Baldessarini et al., 2020; Macellaro et al., 2025). Suicide is a leading cause of death among individuals with schizophrenia, and the lifetime risk of suicide in this group is estimated to be 10 times higher than in the general population. SI is more prevalent in schizophrenia compared to the general population, especially among inpatients (Aytac et al., 2020; Bai et al., 2021). Depressive symptoms were strongly linked to SI in individuals experiencing psychosis (FitzPatrick et al., 2025).
Suicide and Experiential Avoidance
Experiential avoidance (EA), defined as the unwillingness to confront distressing internal experiences, has been identified as a key factor in SI. Suicide can be viewed as the most extreme form of EA, representing a final attempt to escape unbearable psychological pain, and reflecting a severe cognitive fusion where individuals believe their lives are not worth living (Ducasse et al., 2018). Studies show that individuals with higher EA are more likely to engage in experiencing suicidal thoughts. The entrapment or “cry of pain” model of suicide highlights escape from emotional pain, known as EA, as a central factor (Tighe et al., 2018). For example, Angelakis and Gooding found a strong link between EA and suicidality (Angelakis & Gooding, 2021). SI can be understood as a form of EA, highlighting the potential value of therapeutic approaches that focus specifically on reducing such avoidance (Ellis & Rufino, 2016). Greater psychological flexibility was associated with a lower risk of suicide and significantly moderated how depression influenced suicidal thoughts over time, while EA was found to predict SI (Krafft et al., 2019).
Interpersonal Needs and Suicide
The Interpersonal Theory of Suicide aims to explain previously unclear aspects of suicide and its etiology. It proposes that lethal suicide occurs when individuals both desire and are capable of suicide. The theory emphasizes that desire and capability are distinct, with only a small subset of people exhibiting both. The Interpersonal Theory addresses this by providing testable hypotheses linking risk factors, suicidal desire, and capability, thereby advancing scientific understanding and clinical utility. This theory focuses on explaining why most people with suicidal thoughts do not act on them. Perceived burdensomeness (PB) and thwarted belongingness (TB) are key predictors of suicidal ideation. TB is the unmet human need to belong, as central to suicidal desire. TB is a multidimensional, dynamic construct comprising loneliness (few meaningful interactions) and the absence of reciprocally caring relationships, and ongoing TB increases the risk for suicidal thoughts. PB is the belief that one is a liability or burden to others, often accompanied by self-hatred. Extreme perceptions of burdensomeness, particularly when extended across multiple relationships, can heighten suicidal ideation. TB and PB are related but distinct constructs. Empirical studies show that both constructs independently predict SI and highlight that the overlap of these factors greatly predicts suicidal desire (Park & Kim, 2019; Van Orden et al., 2010). It was the first theoretical framework to include the concept of the capability for suicide explicitly. According to the theory, the ability to engage in suicide develops through repeated exposure to physically painful or fear-inducing experiences (Baumeister & Leary, 1995).
EA is significantly associated with increased perceptions of unmet interpersonal needs and higher levels of suicidal ideation. Several studies have demonstrated that EA is related to PB and TB, two core interpersonal needs implicated in suicidal desire (Espinosa-Salido et al., 2025; Hapenny & Fergus, 2017). So, combining the interpersonal theory of suicide with the psychological flexibility model could provide a more comprehensive framework for understanding and evaluating suicide risk in psychiatric inpatient populations. Both EA and IN may serve as factors related to coping that are closely linked to suicide or suicidal thoughts, as mentioned above. The conceptual framework of this study aims to integrate EA and interpersonal processes to explain suicide risk across psychiatric disorders. Elevated suicidality in psychiatric inpatients with bipolar, psychotic, and depressive disorders forms the clinical basis. As a coping strategy, EA can intensify emotional pain and hinder problem-solving, increasing risk. EA models suicide as an extreme attempt to escape distress. The Interpersonal Theory of Suicide adds PB, TB, and acquired capability as key factors. Together, these elements describe how psychological distress, avoidance, and unmet needs interact to influence SI and the progression to suicide. In short, EA, PB, and TB are interconnected mechanisms through which dysfunctional coping may contribute to depression and SI in psychiatric inpatients (Kurşuncu & Baştemur, 2024; Roush et al., 2019). This study aims to examine the psychological and interpersonal factors that lead to SI among psychiatric inpatients. Specifically, this study aims to examine the mediating roles of EA and IN—conceptualized as PB and TB—in the relationship between depression and suicidal ideation. Assessing EA with TB and PB together may yield a more nuanced, process-oriented understanding of SI. The study aims to clarify the possible intermediary role between PB, TB, and EA and how depression links to suicidal thoughts. It hypothesizes that EA, PB, and TB mediate the connection between depression and suicidal thoughts among psychiatric inpatients. Additionally, increased levels of depression may be associated with higher SI in the inpatient psychiatric population, involving relationships with EA, TB, and PB.
Methods
Patients and Design
This study uses a cross-sectional observational design with mediation analysis to explore how EA and IN mediate the relationship between depression and SI among psychiatric inpatients. The study involved 151 individuals aged 18 and older who were admitted to the inpatient psychiatry clinics at Cam and Sakura City Hospital in Istanbul, Türkiye, due to recent suicide attempts with ongoing SI without suicide attempt, as evaluated by a psychiatrist. The study sample comprised individuals who had formulated suicidal plans and/or needed inpatient treatment after a suicide attempt. All patients underwent a psychiatric assessment by a psychiatrist to confirm the diagnoses. The study included individuals diagnosed with psychotic disorders, bipolar disorder, and unipolar depression. Psychiatric diagnoses in this study were determined using the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10), which is the standard classification used in Türkiye, as per the Ministry of Health. Accordingly, diagnoses included schizophrenia (F20), schizoaffective depressive disorder (F25.1), and non-organic psychotic disorders (F28–F29), including bipolar depressive episode (F31.3–F31.5), depressive disorder subtypes (labeled as unipolar depression) such as mild, moderate, severe, and severe with psychotic features (F32.0–F32.3). In the inpatient clinic where the study was conducted, a structured inpatient clinical interview form is routinely used. This form includes a specific section for assessing suicidal ideation, including current thoughts, planning, and a history of suicide attempts. It is completed for all hospitalized patients. Therefore, suicidal ideation in this study was based on the presence of active suicidal thoughts as documented in this standardized clinical assessment.
Exclusion criteria included conditions such as intellectual disability or dementia that could impair the ability to provide reliable responses. Additionally, the decision-making capacity of suicidal inpatients was assessed by experienced psychiatrists through a clinical examination before obtaining consent. Patients who refused to participate were also excluded from the study.
Informed and Ethical Approval
Informed consent was obtained from all patients/their guardians. This study was approved by the ethics committee (Date: 17/07/2023; No.: 09-02). The ethical procedures implemented included ensuring participants’ privacy and anonymity, obtaining informed consent, securely storing data, and conducting the study in accordance with established ethical guidelines. Additionally, the data were stored in hospital information systems and ethics committee archives, and unauthorized access by unauthorized individuals was not possible.
Measurement Tools
The Sociodemographic Form: This form, developed by researchers for the current study, collects essential demographic and psychosocial information, including age, marital status, education, occupation, psychiatric history, psychiatric diagnoses, and alcohol and substance use.
Hospital Anxiety and Depression Scale (HAD): The scale is a self-administered tool with 14 items, which screens for anxiety and depression symptoms separately. The scale demonstrates good psychometric properties, including strong internal consistency, high correlations with clinical ratings (r = .54–.79), and clear discrimination between the anxiety and depression constructs (Zigmond & Snaith, 1983). Aydemir et al. validated the Turkish version. The scale demonstrated good reliability after establishing translation equivalence and testing across different samples, with Cronbach’s alpha coefficients of .85 for the anxiety subscale and .78 for the depression subscale (Aydemir, 1997).
Beck Scale for Suicide Ideation (BSSI): The scale developed by Beck et al. is a 21-item self-assessment scale evaluating current suicidal ideation and past suicidal behavior. The Scale showed high internal consistency in a clinical sample, with most items having significant positive item-total correlations and a strong reliability coefficient (Cronbach’s alpha) of .89 (Beck et al., 1979). Özçelik et al. validated the Turkish version. Cronbach’s alpha value for the BSSI was .84, indicating good internal consistency (Ozcelik et al., 2015).
Acceptance and Action Questionnaire (AAQ-II): The 7-item scale is a 7-point Likert-type measure that assesses experiential avoidance and psychological inflexibility, with higher scores indicating greater levels. The measure showed good reliability and validity, with a mean Cronbach’s alpha of .84 (Bond et al., 2011). The Turkish version was validated by Yavuz et al. in 2016. The Turkish version of the AAQ-II demonstrated good internal consistency, with a Cronbach’s alpha of 0.84 (Yavuz et al., 2016).
Interpersonal Needs Questionnaire (INQ): The 15-item scale, developed by Van Orden et al., comprises two subscales measuring perceived burdensomeness and thwarted belongingness, each rated on a 7-point Likert scale. The INQ demonstrated good internal consistency, with Cronbach’s alpha coefficients of .85 for perceived burdensomeness and .87 for thwarted belongingness (Van Orden et al., 2012). Kursuncu and Bastemur validated the Turkish version. The Turkish INQ-15 demonstrated strong internal consistency, with Cronbach’s alpha and McDonald’s omega coefficients of .92 for perceived burdensomeness and .86 for thwarted belongingness (Kurşuncu & Baştemur, 2022).
Statistical Analysis
The statistical analyses were conducted using Jamovi software (version 2.6). First, descriptive statistics were calculated to summarize the demographic and clinical characteristics of the sample. The distributional properties of all study variables were assessed by skewness and kurtosis coefficients, along with visual inspection of histogram density plots, confirming that the assumptions of approximate normality were met. Internal consistency of all scales and subscales was evaluated using Cronbach’s alpha coefficients, which indicated acceptable to excellent reliability within the current sample. Pearson correlation analyses were performed to examine the bivariate relationships among depression, EA, PB, TB, and SI. To further investigate the underlying mechanisms linking depressive symptoms to suicidal ideation, a multiple parallel mediation analysis was conducted. In this model, depression (HAD-D) was specified as the independent variable, suicidal ideation (BSSI) as the dependent variable, and EA (AAQ-II), PB (INQ-PB), and TB (INQ-TB) as simultaneous mediators. Prior to the mediation analysis, multicollinearity assumptions were assessed using Variance Inflation Factor (VIF) and tolerance values, as well as intercorrelations among variables; all indicators suggested that multicollinearity was not a concern. The significance of direct and indirect effects was evaluated, and indirect effects were tested using confidence intervals. Statistical significance was set at p < .05 for all analyses.
Results
The research sample consisted of 73 (44.5%) males, and the mean age of the sample was 34.0 (SD: 11.7). Unipolar depression -any depressive disorders without manic/hypomanic symptoms (in ICD-10 F32.0–F32.3) was the most common diagnosis, observed in 112 participants (71.3%), followed by bipolar disorder in 36 participants (22.9%) and psychotic disorders in 9 participants (5.7%). For all scales and subscales, skewness values ranged from −0.303 to 0.813, and kurtosis values ranged from −1.20 to 0.549, indicating that all variables were within acceptable limits for approximate normality. Additionally, visual inspection of histogram density graphics showed that the distributions were approximately normal. All scales and subscales show acceptable to excellent internal consistency, with Cronbach’s α values ranging from .743 to .888, indicating generally reliable measurements across instruments. Demographic and clinical data, along with Cronbach’s α values, are shown in Table 1.
Demographic and Clinical Characteristics of the Participants.
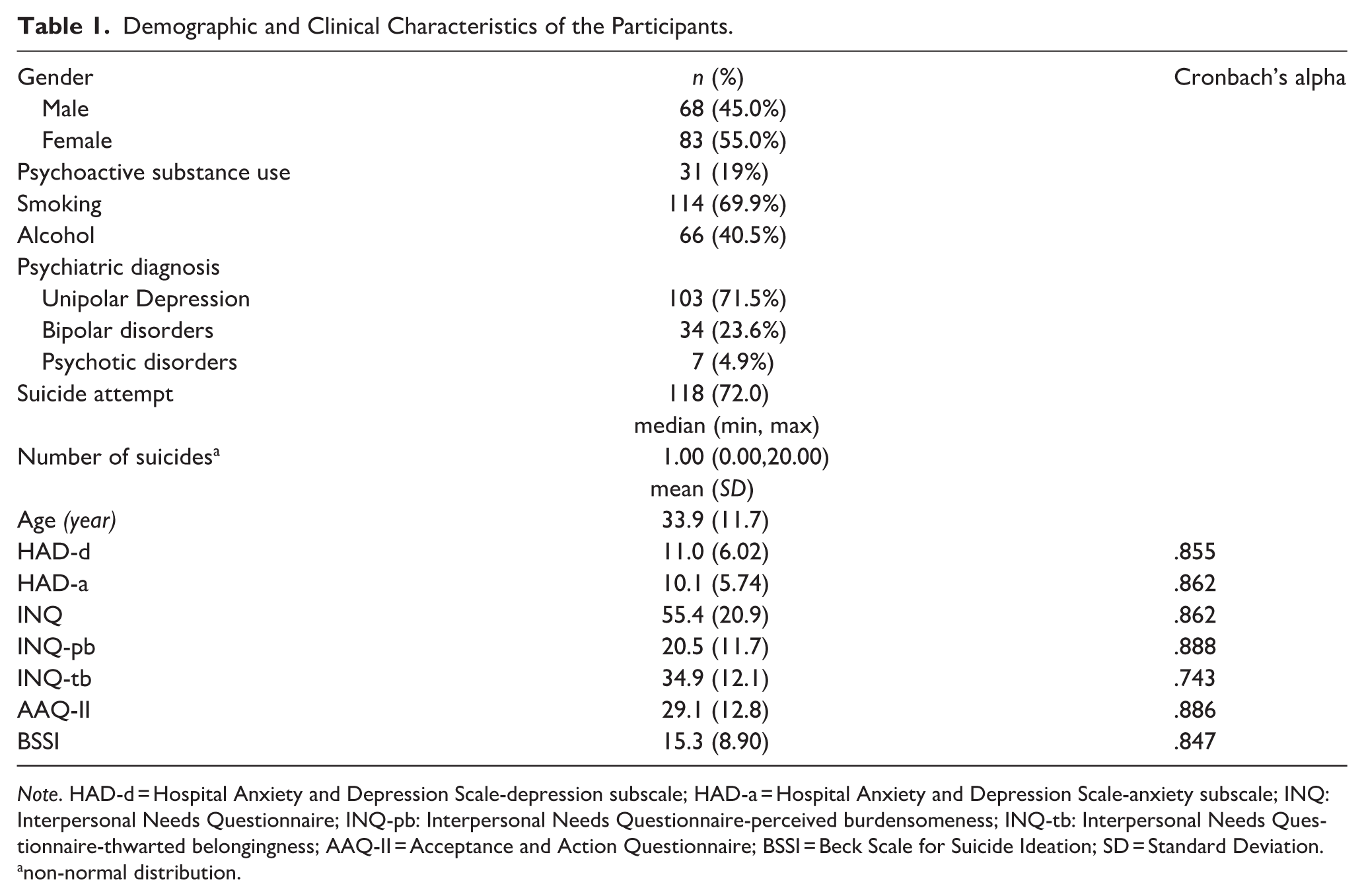
Note. HAD-d = Hospital Anxiety and Depression Scale-depression subscale; HAD-a = Hospital Anxiety and Depression Scale-anxiety subscale; INQ: Interpersonal Needs Questionnaire; INQ-pb: Interpersonal Needs Questionnaire-perceived burdensomeness; INQ-tb: Interpersonal Needs Questionnaire-thwarted belongingness; AAQ-II = Acceptance and Action Questionnaire; BSSI = Beck Scale for Suicide Ideation; SD = Standard Deviation.
non-normal distribution.
Pearson correlation analyses revealed significant positive relationships between depression, EA, IN, and suicidal ideation. Depressive symptoms were associated with greater EA and IN, PB, and TB. These interpersonal and psychological factors were also closely linked to suicidal ideation. All the p-values were below .001, indicating highly significant associations (Table 2).
Pearson Correlations for Scores (r) of Scales and Subscales.
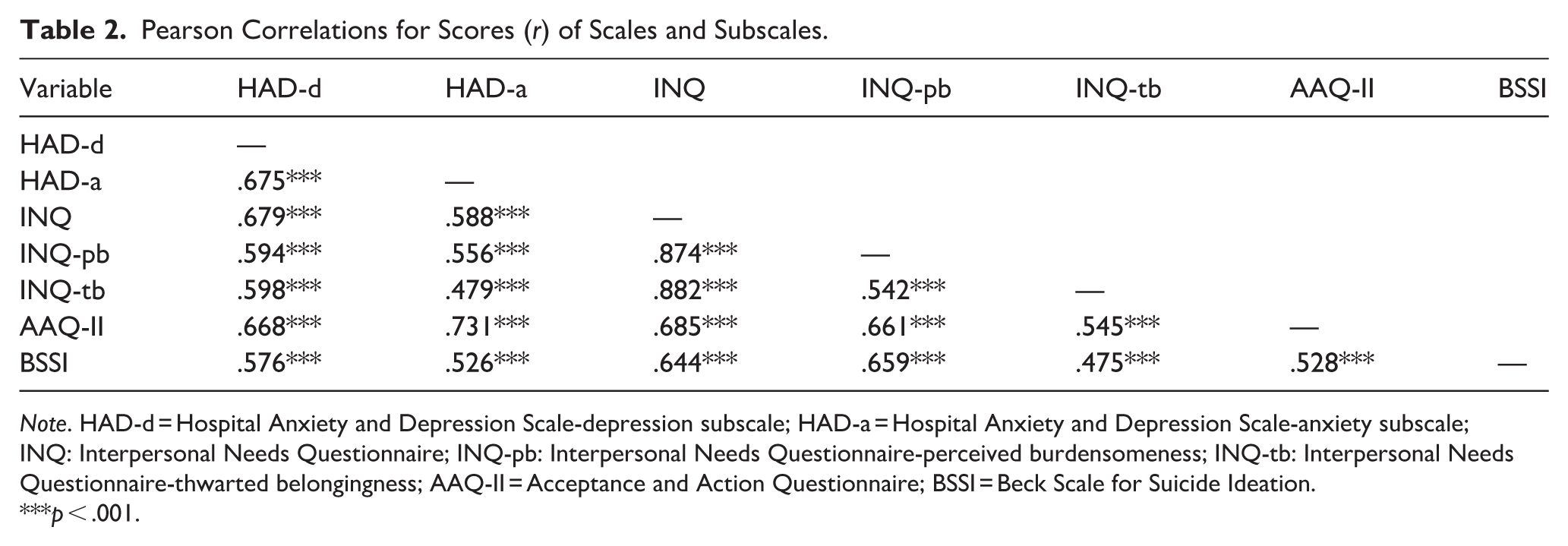
Note. HAD-d = Hospital Anxiety and Depression Scale-depression subscale; HAD-a = Hospital Anxiety and Depression Scale-anxiety subscale; INQ: Interpersonal Needs Questionnaire; INQ-pb: Interpersonal Needs Questionnaire-perceived burdensomeness; INQ-tb: Interpersonal Needs Questionnaire-thwarted belongingness; AAQ-II = Acceptance and Action Questionnaire; BSSI = Beck Scale for Suicide Ideation.
p < .001.
To examine the the relationship between depression (HAD-d) and SI (BSSI) furthermore, a multiple parallel mediation analysis was conducted, including EA (AAQ-II), PB (INQ-pb), and TB (INQ-tb) as simultaneous mediators. Variance Inflation Factor (VIF) values ranged from 1.74 to 2.47, and tolerance values ranged from .405 to .576; additionally, intercorrelations among HAD-d, INQ-pb, INQ-tb, AAQ-II, and BSSI were all below .70, indicating that there was no evidence of multicollinearity among the variables. Depression was significantly associated with EA (β = .668, p < .001), PB (β = .594, p < .001), and TB (β = .598, p < .001). In this model, only PB was significantly associated with SI (β = .477, p < .001), whereas the paths from EA (β = −.018, p = .839) and TB (β = .068, p = .376) to SI were not significant. Consistent with these findings, the indirect effect of depression on SI through PB was significant (Estimate = 0.419, 95% CI [0.251, 0.588], p < .001), while the indirect effects through EA (Estimate = −0.018, [−0.187, 0.152], p = .839) and TB (Estimate = 0.060, [−0.073, 0.193], p = .379) were not significant. Depression remained directly associated with SI after accounting for all mediators (β = .264, p = .002), and the total effect of depression on SI was significant (Estimate = 0.852, [0.659, 1.046], β = .576, p < .001). The findings indicate that, among the examined mediators, PB plays a dominant role in explaining the association between depressive symptoms and SI when all mediators are modeled simultaneously (Table 3).
Mediation Analysis.
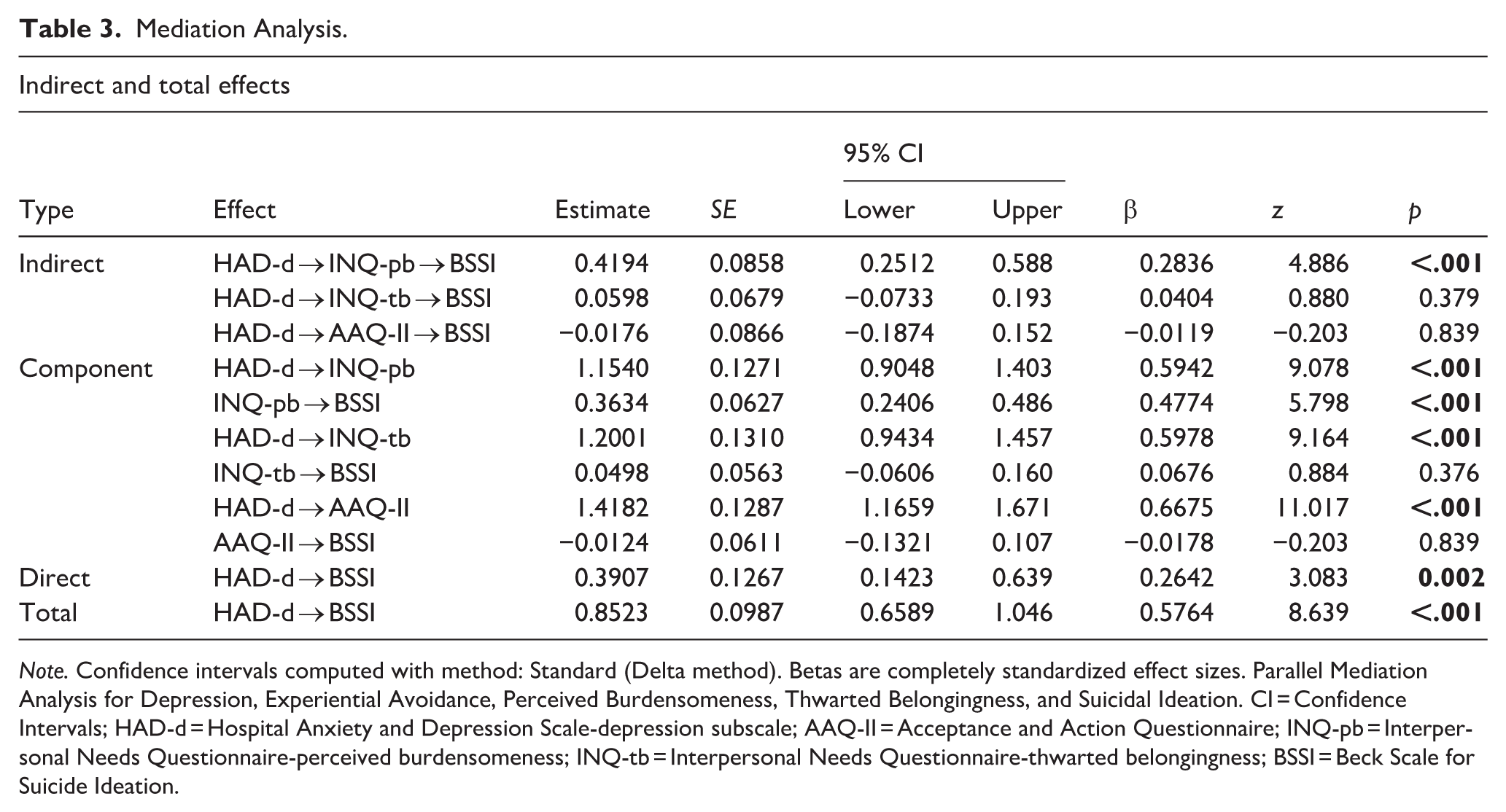
Note. Confidence intervals computed with method: Standard (Delta method). Betas are completely standardized effect sizes. Parallel Mediation Analysis for Depression, Experiential Avoidance, Perceived Burdensomeness, Thwarted Belongingness, and Suicidal Ideation. CI = Confidence Intervals; HAD-d = Hospital Anxiety and Depression Scale-depression subscale; AAQ-II = Acceptance and Action Questionnaire; INQ-pb = Interpersonal Needs Questionnaire-perceived burdensomeness; INQ-tb = Interpersonal Needs Questionnaire-thwarted belongingness; BSSI = Beck Scale for Suicide Ideation.
Discussion
Suicide and SI have always been intensively studied because of their significance for both societal and individual mental health, especially because psychiatric inpatients are at higher risk. Understanding and predicting the impact of SI is an important area of suicide research. The current study aimed to better understand SI among psychiatric inpatients by leveraging the interpersonal theory of suicide and the EA. Demographic data from the current research indicated no significant gender differences among patients hospitalized for suicide.
Major depressive disorder is a primary driver of suicide, particularly when left untreated, and is commonly identified in patients hospitalized for suicidal thoughts (Rihmer & Kiss, 2002; Wasserman, 2016). The prevalence of SI across different populations has consistently shown a strong association with mental health problems. In general, SI appears to be less common in the general population than in clinical samples. Among individuals receiving outpatient psychiatric care, both current and lifetime experiences of SI are relatively frequent, while even higher rates are observed among psychiatric inpatients. SI is closely linked to a wide range of mental health disorders, and its prevalence varies considerably across diagnostic categories. It is particularly common among individuals with mood, personality, adjustment, psychotic, and substance use disorders. Furthermore, studies consistently report a higher prevalence of SI among females than among males across different settings and populations (Furnes et al., 2021). People who had expressed SI showed a clearly higher risk of dying by suicide than those who had not, although this risk varied across populations and was greater in psychiatric patients during the first year of follow-up than in non-psychiatric groups (Hubers et al., 2018).
The results of this study showed that depressive symptoms were strongly and positively correlated with PB, TB, EA, and SI. A study conducted among 402 psychiatric inpatients, like this study, also supports these findings, showing that feelings of TB and PB are significant predictors of SI (Brown et al., 2021). The other two studies also found that EA, PB, TB, depression, and SI were moderately to highly correlated, consistent with the present study’s findings (Hapenny & Fergus, 2017; Roush et al., 2019). These results reinforce the importance of focusing on these core interpersonal experiences when assessing and addressing suicide risk in clinical settings, particularly among high-risk inpatient populations (Beautrais, 2006; Chu et al., 2017; Parrish et al., 2026).
Interpersonal difficulties are more often found in people with depressive symptoms and are directly associated with an increased risk of suicidal thoughts, highlighting their crucial role in the development of suicidality. Feelings of alienation and being a burden in family and social settings raise suicidal thoughts, in line with the interpersonal theory of suicide and supported by numerous studies (Conner et al., 2007; Hallensleben et al., 2019; Joiner et al., 2010; Van Orden et al., 2010). Interpersonal difficulties weaken important protective factors against suicidal ideation. Social support proved to be a strong protective factor against suicidal ideation, with suicidal thoughts decreasing as social connectedness increased (Selak et al., 2024; Stoms et al., 2025). When individuals experience strain or a sense of absence, they may feel alienated and unimportant. Shame can hinder disclosure of suicidal ideation, while depression increases withdrawal. Growing isolation can deepen hopelessness and elevate the risk of suicidal ideation. Overall, findings of this study also may highlight the importance of addressing both depressive symptoms and their impact on interpersonal needs to better understand and prevent SI among psychiatric patients.
In the parallel mediation model, only PB uniquely predicted SI and showed a significant indirect effect, whereas EA and TB were not significant. Depression was significantly associated with all three mediators. Overall, PB emerged as the strongest variable linking depressive symptoms to suicidal ideation. These findings are consistent with prior literature. A study reported moderate-to-high correlations among EA, PB, and TB; however, structural equation modeling indicated that PB was the predominant predictor of suicidality (Kurşuncu & Baştemur, 2024). In a similar study, Espinosa-Salido and colleagues evaluated the relationships among EA, PB, and TB and suicidal ideation. They found that PB, but not TB, mediated the relationship between EA and SI when both were tested simultaneously. Together with the present results, these studies highlight PB as a central interpersonal mechanism linking psychological distress to SI (Espinosa-Salido et al., 2025). Across studies, PB consistently shows a stronger association with SI than TB, or it emerges as significant while TB does not (Bhargav & Swords, 2022; Ko & Park, 2025; Martin et al., 2021). PB may be more influential than TB in SI because it may directly target how individuals evaluate their own worth and impact on others. Feeling like a burden can create intense guilt, shame, and self-blame, which may transform emotional distress into the belief that one’s absence would benefit others. This can make suicidal thoughts seem like a solution rather than just an escape. In contrast, TB reflects unmet social needs and loneliness, which are painful but do not necessarily imply that one should disappear. Thus, interpersonal burden may more strongly transform psychological pain or depressive status into suicidal ideation.
EA is the tendency to avoid unpleasant internal experiences and is linked to higher levels of depression and suicidal ideation. Research indicates that reductions in EA are associated with decreases in both depressive symptoms and suicidal thoughts, suggesting that EA may mediate the relationship between depression and suicidal ideation. Across various populations—such as psychiatric inpatients and university students—EA has been found to partly mediate the effect of depression or related stressors on suicidal ideation, emphasizing its significant indirect role in the development of suicidal thoughts (Ellis & Rufino, 2016; Wang et al., 2023). Bryan et al. examined the effect of EA on the emergence of post-traumatic stress, depressive symptoms, and suicidal thoughts involving 168 participants. The findings indicated that those with higher psychological flexibility experienced significantly less post-traumatic stress and depression, and a reduced risk of suicide (Bryan et al., 2015). This study showed a relationship between EA and depression and SI. However, EA did not demonstrate a mediating effect. The lack of a mediating effect may be due to the magnitude of the PB.
These results may underscore the importance of assessing the awareness of one’s interpersonal values at risk for suicidal ideation. Roush and colleagues find that greater valued living and life fulfillment are each associated with lower levels of thwarted interpersonal needs and suicidal ideation, suggesting that integrating the psychological flexibility model with the interpersonal theory of suicide may improve the conceptualization, assessment, and treatment of suicide risk among psychiatric inpatients (Roush et al., 2019). This study establishes that EA and IN partially mediate the relationship between depression and suicidal ideation. Integrating findings from the second study could emphasize the potential benefit of interventions that enhance psychological flexibility and address unmet IN. Moreover, clinical interventions could benefit from addressing how EA and IN interact in real-world psychiatric settings and how these mediators might serve as early intervention targets to prevent the escalation of SI in depressed patients. Mental health providers should also include the assessment of TB and PB in a comprehensive suicide risk evaluation since these factors may significantly influence the connection between psychological flexibility and SI.
As a psychotherapeutic intervention based on the psychological flexibility model, Acceptance and Commitment Therapy (ACT) may be a practical treatment approach for psychiatric inpatients with elevated suicidal ideation. Preliminary findings suggest that ACT is effective in reducing suicidal thoughts and treating depression among psychiatric inpatients. By emphasizing values and committed action, ACT may indirectly affect SI through its impact on IN (Petersen & Zettle, 2009; Tighe et al., 2018). Several studies have reported a connection between EA—or psychological flexibility—and IN. TB and PB mediate the link between psychological inflexibility (including EA and cognitive fusion) and suicidal ideation. This suggests that ACT may help reduce SI by improving IN (Baer et al., 2022; Roush et al., 2019; Van Orden et al., 2012). Intervention studies demonstrate that approaches focusing on interpersonal relationships may be effective and feasible in reducing suicide risk among both older adults and adolescents (Heisel et al., 2015; Zullo et al., 2021).
This study is limited by its focus on psychiatric inpatients at a single hospital, thereby restricting the generalizability of its findings to outpatient or community populations. The sample comprises individuals with relatively severe symptoms and acute presentations, who may differ in key psychological traits from those in less severe cases. Self-report measures, although validated, may be affected by social desirability or recall bias. The small sample size may also reduce the statistical power required to test more complex mediation models, potentially affecting the generalizability and strength of the results. Larger and more diverse samples are needed in future studies to confirm and extend the mediation effects observed in this study. Another limitation is the absence of data on patients’ previous psychiatric or primary care history, which could provide important context for understanding the development of suicidal ideation. While much research has examined suicide ideation in the inpatient population, it has not specifically focused on individuals with suicide ideation in the general population. Also, some specific groups like refugees, low-income individuals, those living alone, and the unemployed face higher stress and limited support, increasing their vulnerability to suicide (Berkelmans et al., 2021; Burhan et al., 2024). Therefore, specific populations may require separate review. The cross-sectional design limits the ability to determine causality between depression, EA, IN, and suicidal thoughts. Additionally, biological factors were not assessed, which may play a vital role in SI and suicidal risk (Aytac et al., 2020; Gokcay et al., 2025). Future research should employ longitudinal designs and multimodal approaches that combine biological, psychological, and social factors to gain a more complete understanding of SI.
Conclusion
This study highlights the roles of EA, TB, and PB in understanding SI among psychiatric inpatients and suggests that PB may be more influential than TB in suicidal ideation (Figure 1). Both factors partly mediate the association between depression and suicidal ideation, supporting the integration of the Interpersonal Theory of Suicide with the EA Model. Including severe cases, such as individuals with concrete suicidal plans or recent attempts, is a significant strength. Despite some limitations, the study uniquely combines psychological flexibility and interpersonal theories. The findings highlight the importance of evaluating EA, burdensomeness, and belongingness, and suggest that interventions like ACT or those addressing IN might help lower suicide risk.
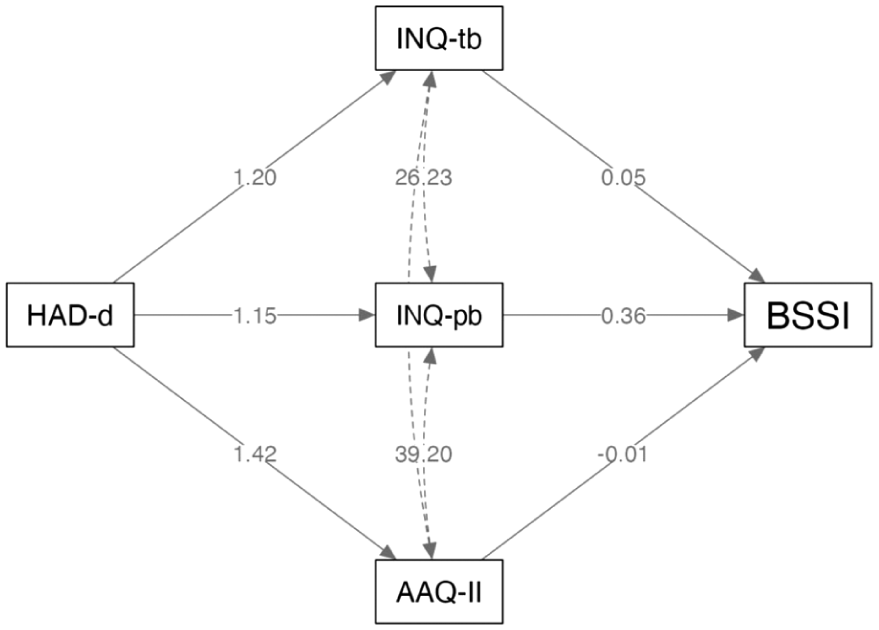
Parallel mediation analysis for depression (predictor), experiential avoidance (mediator), perceived burdensomeness (mediator), thwarted belongingness (mediator), and suicidal ideation (dependent variable).
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.