
Abstract
Italy and Spain were the first countries affected by the shift of the pandemic epicentre from east to west. The rapid spread of the virus in allegedly similar social settings, the relatively high numbers of cases and casualties, and the adoption of drastic containment measures were similar in the two countries during the first wave of the pandemic. Both countries are enmeshed in an unstable political equilibrium at the centre, governed by recently established national political coalitions that have continuously been called into question and exposed to significant public debt. The two countries differ in the role of the executive vis-a-vis the legislative, and the tensions between central coordination and regional centrifugal forces. To improve the understanding of how the pandemic has influenced decision-making and crisis management, this article explains the relevance of institutional veto points, as well as differences between the two countries. There is room to match coordination, policy capacity and shared accountability through more collaborative governance.
Points for practitioners
Governing a transboundary crisis that involves different governmental levels is about creating an effective coordination mechanism that clarifies responsibilities, avoiding those who may block decision-making processes (veto players) through being incentivized to do so due to the absence of adequate shared accountability systems. National and regional managers should realize that the separation of territorial powers not accompanied by political coordination jeopardizes policy capacity in both the short and long term.
Introduction 1
To address the health emergency created by COVID-19, many governments have combined ordinary and extraordinary tools to implement decisions that affect the lives of thousands of people (Bouckaert et al., 2020). In normal times, veto points (Immergut, 1992) play roles in decision-making processes and their outputs. It is expected that during crises, veto points, through the analytical framework used in this article, can foster or hamper joint decision-making processes by different governmental levels. This framework has been used to analyse health and welfare reforms (Ha, 2008; Natali and Rhodes, 2004) and economic policy (MacIntyre, 2001); however, an application of the approach to crisis management in multi-level polities is lacking.
We try to fill this gap by analysing four key moments of the pandemic response during its first six months where the most severe lockdown measures were adopted in several countries. This article attempts to answer the question of whether veto points at different territorial levels of government played a role in slowing down or changing the policy response. Italy and Spain are two multi-level polities that are adequate for this analysis, with power in health decisions being shared between the regions and central government, which increases the potential number of veto points and veto players (Bonoli, 2001).
By focusing on four decision/veto points (the declaration of the state of emergency, the adoption of lockdown measures, the definition of healthcare measures, and the reopening and first economic measures) faced by the two countries during COVID-19, we enquire about the potential to veto policy decisions during transboundary crises. By using veto-point theory (Immergut, 1992), we highlight the interplay between the national government (in charge of supervising the system) and regional veto players (Tsebelis, 2011) in multi-level accountability arenas in the face of crises.
After the COVID-19 outbreak in Wuhan in December 2019, Italy and Spain were the first two European countries to be rapidly and extensively affected by the pandemic. On 31 January 2020, both countries officially registered the first cases. On the same day, the Italian government declared a state of emergency, while Spain proclaimed a state of alarm on 11 March. Both countries experienced an explosion of cases in the highly interconnected areas of Northern Italy, Madrid and Cataluña. The growth of detected cases in the early weeks of the outbreak was also related to the growing test capacity. It brought about a strong sense of urgency, which was further reinforced by the constant increase in the number of pandemic-related deaths.
Italy and Spain have similar productive structures characterized by small- and medium-sized enterprises, pronounced territorial cleavages, the notable presence of a shadow economy, a strong role played by the state in the economy, and welfare systems that are heavily reliant on families (Burroni et al., 2019). Both countries were hit considerably by the global financial and economic crisis of 2008, which led to a rising public debt ratio (Perez and Matsaganis, 2018), reaching 137.3% and 97.9% of gross domestic product (GDP) in Italy and Spain, respectively, in the third quarter of 2019. With the incoming economic crisis, their sovereign debts might not be viable, and the moderate economic growth forecasted at the end of 2019 by the Organisation for Economic Co-operation and Development (OECD, 2019) will be offset considerably. For economic recovery, both countries count on tourism, which represents 13% and 14.3% of GDP in Italy and Spain, respectively. 2 Despite these similarities, both countries present institutional contrasts in intergovernmental relationships and the regulation of lockdown, as explained later.
In the next section, we describe the framework of veto points in connection with crisis management. The third section compares Italian and Spanish healthcare institutions. The fourth section analyses four main decision points related to the management of the COVID-19 crisis and summarizes the roles played by national and regional governments. Finally, we present a discussion of the results and conclusions, including practical and theoretical implications.
Approach: the role of veto points in the management of the crisis
Transboundary crises like pandemics spill over different policy sectors, levels of government and national and transnational actors, and may endure over time (Boin, 2009). These crises are likely to demand energetic governmental reactions, which cannot easily be predicted by traditional policy theories (Wenzelburger et al., 2019), in order to issue disaster relief and return to previous conditions.
Beyond these potential enduring changes, crises compel governments to react promptly. They must set the agenda and display policy capacity to implement effective policies that require a good understanding of the problem, its causes and the choice of the most adequate instruments (Bali et al., 2019). Although there is no optimal formula for harmonizing competing interests and tensions, or for overcoming uncertainty and ambiguous government structures (Christensen et al., 2016), flexibility and adaptation represent key assets that are constrained by the political, administrative and situational context. In fragmented institutional contexts, the conditions for effective nationwide crisis management seem to be threatened by the roles played by national and regional governments.
Veto points are moments of strategic uncertainty at which different veto players may formally hamper or overturn the implementation of nationwide policies (Wenzelburger et al., 2019). Veto points (Immergut, 1992) depend on constitutional rules and electoral results, which apply to different governmental arenas in multi-level polities. Therefore, institutional provisions and the configuration of party representatives are relevant. Veto players (Tsebelis, 2002) are actors that have to agree to the proposed policy change. Institutional veto players are defined by the constitutional-level regulations and include the legislative chambers and intergovernmental bodies, as well as comprising territorial actors. Partisan veto players are the party members of the coalition government or the parliamentary groups in the chambers. Immergut (1992), unlike Tsebelis (2002), stated that interest groups may play a role in influencing the decisions of political party representatives at veto points.
Veto players can only be successful if there are decision-making structures with veto points in which actors can influence policymaking (Immergut, 1992). The analysis of Immergut was restricted to the national level of government and the role played by the legislature when the executive tries to enact policy changes. In multi-level policies, veto points for nationwide decisions may include the national parliament and regional governments, with their parliaments. In these arenas, veto players have context-based (and not universal) preferences across countries, as well as different degrees of leverage in decision-making (Ganghof, 2003), but the political struggles are ‘about means rather than ends’ (Ganghof, 2012). Furthermore, as suggested by Immergut (1992), the number and sequence of veto points might influence the direction of decisions.
According to Chowanietz (2011), crises might help decision-makers to surmount the resistance of veto players when ‘rallying around the flag’; however, political parties from the opposition might use the opportunity in the legislature and other levels of government to veto the decisions of central government (Davidsson and Marx, 2013). The transboundary crisis provoked by COVID-19 links decision-making arenas (territories and sectors), fostering juxtaposed and cross-cutting actors, institutions and preferences. The unfolding of the crisis has shown that national governments have faced multiple trade-offs between public health and economic issues, as well as between regional governments unevenly affected by the pandemic. To understand how veto players have influenced decisions, we analyse the constitutional rules and informal practices linked to the decisions made to avert the pandemic, following Immergut’s (1992) veto-point theoretical approach.
The case selection of Italy and Spain: similar fates with dissimilar institutions
This section focuses on the Italian and Spanish multi-level polities, with a territorially layered configuration of veto points. The regions and central powers share decision-making powers on health policies and their intergovernmental arenas set the configuration of veto points that veto players may exploit. Although the systems seem similar, there are institutional differences in the relevance of the comparison (see Table 1).
Main features of the Italian and Spanish institutional systems.
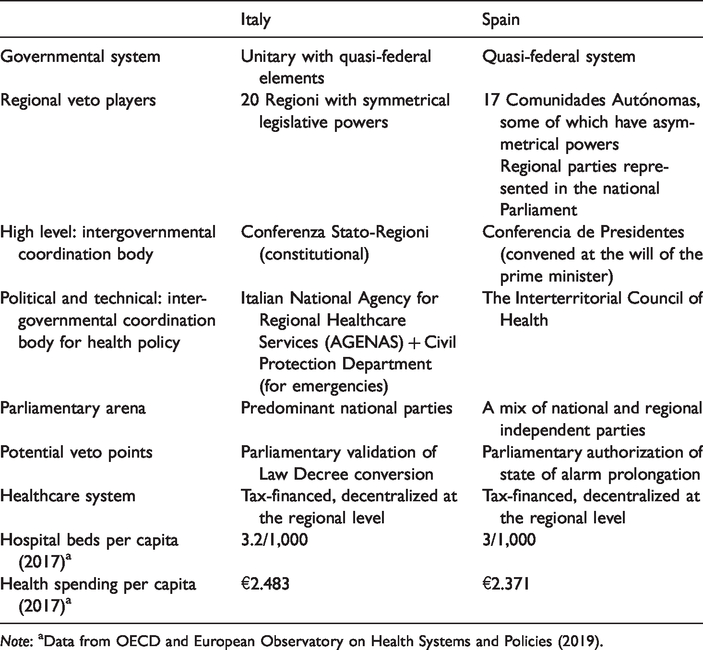
Note: aData from OECD and European Observatory on Health Systems and Policies (2019).
The increasing regionalization of power has softened over recent decades as a result of the centralizing features of the ‘Napoleonic state tradition’ (Ongaro, 2008) assigned to both countries. Yet, Spain is one of the most decentralized countries in the European Union (EU), with only 45.7% of government expenditure being at the central level (Eurostat) and 19.7% of staff working in the centre (with 58% working in the regions) (Ministerio de Política Territorial y Función Pública [MPTFP], 2020b). However, Italy presents almost reverse numbers, with 61.5% of government expenditure at the central level in 2018 (Eurostat) and 54.6% of staff working at the centre (with 21.8% working in the regions) (Istituto Nazionale di Statistica [ISTAT], 2017).
Italy has gradually decentralized since the 1970s, when the regions with ordinary statutes established by the Republican Constitution of 1947 were finally created (Palermo and Wilson, 2014). The 2001 constitutional reform and subsequent laws in 2003, 2005 and 2009 provided the regions with decisional capacity on local policies, favouring a federalist arrangement (Lippi, 2011). Furthermore, since 2000, the directly elected regional presidents (governors) have transformed the regional executives into political actors of relevance (some of which have national relevance).
Permanent intergovernmental conferences facilitate policy coordination. The national government and governors have met at the Conference of Regions and Autonomous Provinces since 1981. The regions must be consulted when developing draft laws, legislative decrees or government regulations on regional-related matters. In this regard, regions and their conferences can represent veto players that can slow down, and sometimes block, the implementation of national government policies.
In healthcare, the Ministry of Health coordinates the national health plan and sets the basic healthcare levels. Other national bodies are the Higher Health Council, the Higher Health Institute and the National Agency for Regional Health Services. Regional health systems, which are heterogeneous despite financial standardization, include local health authorities and hospitals. The decision-making processes in the health system are, then, fragmented but the national government may play a political role in defining a unitary approach to problem-solving.
Currently, Spain shows elements of both dual and cooperative federal systems. The state has exclusive powers in social security and international relations, for instance, and the Comunidades Autónomas have power in health, education and social services, though the government can issue basic legislation in those areas. However, power is shared in most sectors (Aja and Colino, 2014). The evolution of the system has ended up, paradoxically, in too much centralization (the regions complain that they lack resources and autonomy) and too much decentralization (the central government objects to the gradual loss of power and the difficulties in implementing national-level goals) (Colino and Hombrado, 2015). Furthermore, some regions have power in different areas than the rest, with responsibility for regional police, the power to call for regional elections (not on the same day as municipal elections in the rest of the regions) and different, more advantageous, financial systems (Navarra and the Basque Country). The asymmetrical institutional configuration of the regions and high political mistrust among authorities from different territorial levels have converted some regional authorities into veto players at relevant veto points, and this has entailed high political-level conflict since the late 1980s through cases filed at the constitutional tribunal (MPTFP, 2020a).
Additionally, the Conferencia de Presidentes, attended by the Spanish prime minister and all regional prime ministers, convenes for cross-cutting events of relevance, like environmental issues or terrorism. These conferences do not have any bearing on the formal decision-making process. In the absence of a proper territorial chamber to introduce regional demands and solve conflicts, intergovernmental relations are channelled through the executives. The lower chamber may become an arena where regional interests can be voiced. Regional parties may have the chance to influence the formation of central government and support (or veto) the main laws and the annual budgetary laws at the national Parliament.
Concerning the healthcare system, the Spanish government has some exclusive power over the regulation and general coordination of health, and each region issues development legislation and manages and finances health. The Interterritorial Council of Health (ICH), a political intergovernmental body composed of the national and regional ministers of health, ensures the coordination of the system for all health-related issues, including public health, except for national emergencies, where the central government may issue overarching decisions. As in Italy, Spain is a fragmented system where regional parties from particular regions may play considerable roles. To conduct the analysis of the institutional structures and the decision-making processes during the first three months of managing the crisis in Italy and Spain, we carried out a documentary analysis (McNabb, 2015; Tight, 2019) of the information provided by national and regional governments, as well as of the legislation that shapes the institutional configuration of both systems.
Dealing with the crisis in the intergovernmental arena
This section analyses the phases in the management of the COVID-19 crisis where veto points can be observed. The effective management of a crisis requires swift detection of the crisis, understanding of respondents of what is happening, critical decisions being made by the right people, orchestration of the efforts of respondents and communication of governments with citizens, while the aftermath of a crisis is also marked by having proper accountability procedures (Boin et al., 2016). To provide an understanding of the management of the COVID-19 crisis in Italy and Spain, we focus on the following four phases, which span the first 100 days of the pandemic: declaration of a state of emergency; lockdown (and its prolongation) as a critical decision; the definition of healthcare measures to orchestrate efforts; and the reopening of the economy as one of the relevant features of the aftermath.
Declaration of a state of emergency
Italy and Spain differ in the regulation of the state of emergency, a key element involved in issuing lockdown measures and placing health institutions under a single command. In Italy, the declaration of a state of emergency lasted six months. Following the Civil Protection Code (Legislative Decree 1/2018), the declaration did not require parliamentary validation, that is, there was no veto point. Thereby, the head of Civil Protection acquired extraordinary powers that were exercised through ordinances. This agency operates under the supervision of the Prime Minister’s Office. The state of emergency declaration does not itself constitute a legal basis for any further governmental act. The Italian constitution uses the Law Decree for emergencies. It allows the government to issue legislative acts without prior parliamentary authorization, though under the scrutiny of the head of the state. Each Law Decree must be converted into law by Parliament within 60 days (veto point). During the first 100 days of the crisis, the Italian Parliament validated the 13 Law Decrees adopted by the government.
In Spain, the Organic Law 4/1981 regulates the state of alarm, sets conditions for the duration of the declaration and strengthens Parliament’s role in its prolongation. Under the state of alarm, which can be used for epidemics, the affected area can be placed under the coordination of the central or any regional government (if the state of alarm affects one region). During this period, public authorities can restrict circulation in specific areas and at certain times, commandeer industrial properties (like putting private hospitals under public health authorities’ command), and ration or fix prices of basic articles. The Spanish Parliament must authorize the prolongation of the state of alarm within 15 days of the first declaration. The Parliament can approve the duration of the state of alarm for more than a fortnight but the government did not request a longer period than that during the first wave given the uncertain parliamentary support for this request. This veto point was not initially used by the national opposition parties or by the regional parties with parliamentary representation given the seriousness of the situation.
Lockdown measures
On 23 February, the Italian government established urgent measures and set the first lockdown areas in the North (Law Decree n. 6). In normal times, regulation of health protection is shared between the central government, which establishes the key principles, and the regions, which manage the healthcare service. During the management of COVID-19, this system has been partially altered. The directing role of the central government was enhanced, and the Premier coordinated the interactions with governors and the public. The cautious line maintained by the government, supported by the experts of the National Institute for Health, extended the lockdown nationwide on 10 March.
Regions and municipalities had the power to adopt additional containment measures during this period but the framework of competences remained confusing until the adoption of Law Decree n. 19 on 25 March. Therewith, the central government constrained the power of sub-national governments, and different regions reacted to this. Northern regions, led by the major opposition party (Lega Nord), contested governmental decisions, while the central and southern regions, controlled in some cases by the majority parties, alternated between supportive and antagonistic positions. Some regions made decisions without consulting the central government (e.g. Lombardy created a COVID-19 hospital) and simultaneously claimed that they could not independently adopt containment measures (the failure to establish a red area in Lombardy was under judicial investigation). Some southern regions requested the restriction of population mobility. The antagonistic positions of some regions, in the mass media or inside the Permanent Conference, did not change the government’s decisions, which were unrestricted in the absence of a formal veto point.
To fight the COVID-19 pandemic, the Spanish government proclaimed a state of alarm on 14 March (RD463/2020), commanding a nationwide lockdown except for in areas of health and essential economic activity. Overall, the state of alarm was extended six times 3 for consecutive 15-day periods, and it finished on 21 June, 105 days later. The extensions were authorized in Parliament, though each time with a smaller majority in support of the government. Voting represented a considerable veto point for governmental decisions, though the actual veto was only exerted in the last extension. At the declaration of the state of alarm, the central government centralized decisions on the specific restrictions to be applied in each of the clinical phases of the evolution of the pandemic, with an initial consultation (not shared decision-making) with regional authorities until the end of the fifth extension on 7 June.
The central government can endow the presidents of the regional governments with the authority to issue orders under the state of alarm. This only happened after the sixth extension of the state of alarm, that is, 75 days after the lockdown started. Before handing over the power to the regions, the Premier held 13 weekly videoconferences with the regional presidents until 7 June. This is a very intense interaction considering that between 2004 and 2019, such conferences with the presidents were held only six times.
These meetings represented an opportunity for co-joint decision-making but the polarized climate of party politics and the centrifugal forces exerted by the Catalonian and Basque authorities weakened this potential. The Premier used this forum as an information platform. The governmental strategy encountered considerable opposition from the Madrid regional authority (governed by a right-wing coalition, as opposed to central government), Catalonia (governed by secessionist forces) and also the Basque Country (governed by a regionalist party with representation in the national Parliament). The conference of regional and national prime ministers could have been used as a political instrument to soften the veto positions of regional leaders at the national Parliament but this was thwarted by the unilateral position of the central government.
These meetings did not constitute a formal veto point. However, the opposition of some influential regions permeated the national parliamentarian elites that had to authorize successive extensions of the state of alarm. The negotiations about regional singularities (in the Basque Country and Catalonia), as well as the opposition of the conservative party to victimizing regions seen as being punished by the pandemic (Madrid) or successful in taming it (Galicia), set the tone for highly contested parliamentary sessions. From the fourth to the sixth extensions, parliamentary authorization was not granted until the last minute, with only one or two votes over the needed majority. The expert argument for keeping the lockdown, mostly agreed in technical intergovernmental forums like the Commission for Public Health, was not a battleground for supporting the government with the state of alarm. Instead, political argumentation of different sorts, rather than scientific evidence, was used as justification for not supporting the state of alarm.
The last extension that we consider (on 7 June 2020) was accepted by the authorities because some regions that were threatening to veto the full lockdown were granted the power to issue measures in their territories. After 21 June, the central government was not able to issue inter-regional mobility restriction orders as a declaration of a state of alarm is required. The presidents of these regions were in charge of determining the containment measures, and they very often collided with the judiciary, which led to some decisions being overturned.
Healthcare emergency and governance
In Italy, operational coordination at the national and inter-regional levels has been entrusted to the Civil Protection Department and the Ministry of Health. Despite the presence of regional representatives in some nationwide consultation and decision-making bodies, the central government issues the main health policy decisions through different executive orders. Regions have always managed regional services without any possibility of attributing direct responsibility to the government, except for technical indications from the coordination bodies.
The situation in Spain was more nuanced. During the state of alarm, the Ministry of Health centralized all (health- and non-health-related) decisions, with the capacity to commandeer the resources of all private hospitals. However, given that central powers were restricted to issuing basic legislation and lacked management experience in normal times, the ministry did not have the skills and resources to properly source needed equipment (the Ministry of Finance had to assume this task) and steer the system. Some regional leaders and their assessors questioned national policies and requested full control over the measures to be taken. However, the central decision to pass the steering functions of the pandemic to the regions so that they could be adapted to local situations came late, after the fifth extension on 7 June, once the threat of a veto was apparent. The relatively slow devolution of power to the regions on the matter might have been because the pandemic, by and large, cross-cut the borders of different regions with similar impacts, though the health data did not show this and there were disparities in the incidence of COVID-19. Only the central government was able to set limits on inter-regional mobility, for instance. Another possible explanation is the distrust of the centre regarding the handling of the pandemic by regional authorities.
At the same time, the regions benefited from their lack of accountability since everything that went wrong could be pinned on the central government. The lack of effective political cooperation among territorial levels opened a window of opportunity to create an inter-territorial agency for public health with shared governance principles and responsibility, and joint accountability, a gap that the intergovernmental Commission for Public Health does not seem to fulfil. In the absence of such a body, political struggles may considerably influence the decision-making of different bodies. A central agency (Centro Estatal de Salud Pública) was foreseen in Law 33/2011 but never implemented. The new agency (announced as being finally created by the Health Minister on 18 June 2020) might need to expand the share of ownership with the regions to achieve joint governance and to limit the opportunistic political behaviour of regions when vetoing national decisions. The Interterritorial Council for Health could take up that role but disagreement on how to implement localized lockdowns following scientific knowledge has proven that this council cannot authoritatively assume the coordination of the system.
The heterogeneous capacity of the 20 Italian regional health systems – efficient and effective but expensive in the North and subject to severe cuts and commissioners in the Centre and South – influenced the regional dynamics triggered by the pandemic. Northern regions that boasted better health systems were the first to be severely affected. Some of these regions, however, adopted a containment approach in the early stages, which was not effective, generating a wider debate on the opportunity of entrusting public health to the sub-national level. The Civil Protection Department supported the regions in the procurement of equipment and personnel by setting procedures. A specific national commissioner was created for coordinating procurement.
The 17 regional Spanish health systems faced the challenge separately by buying medical equipment on the market (sometimes with disappointing results) and denying access to this equipment to patients from other regions (though with time, cooperation started to work). Thus, each region had a different capacity to face the pandemic. Big disparities in beds, staff and testing capacity were present before the crisis and remained throughout it. The rigidity of contracting healthcare personnel did not allow some regions to contract healthcare staff from other regions in which they were in excess.
Reliable information on cases, deaths, the recovery rate and the R number (related to the infection potential of the virus) was key among the scientific community to offer advice on policy options. In Italy, the Civil Protection Department shared a unitary system of classification and transmission of information with the Ministry of Health and Regions, assuming final responsibility for communicating the data. In Spain, the gathering of data was flawed at times. Comparative data were full of regional exceptions, and considerable distrust in the reliability and timeliness of the data surfaced now and then. This hampered the day-to-day follow-up and prognosis of the situation.
Formally, the management of the emergency during the first months in both countries did not register the activation of veto points; this only occurred at the end in Spain. The governance of health systems, already regionalized, adapted to the mandates of the national government. The transition from central coordination to the regional handling of the pandemic in Spain seeded the path to regional veto points over national interests.
Reopening and economic measures
The softening of the lockdown can be contextualized at two levels. At the international level, both countries progressively followed other governments by reducing the containment pressure while maintaining significant limits to the mobility between states. Furthermore, the European bond eased due to the suspension of the Stability Pact, and the European Central Bank purchased massive Italian and Spanish securities. These circumstances increased the space for governmental public spending choices.
At the national level, the resumption of parliamentary debate and political activities in Italy at the end of April reduced central governmental autonomy in making decisions, and veto points became more available than before. Due to the frequent interactions with Parliament, the opposition parties and the regions, the Premier made decisions considering the country’s economic needs. The regions maintained a divided approach, characterized by local demands and a common request to reopen activities but not the inter-regional borders. The Head of State and the government promoted a unitary national path, keeping the tools for the rapid activation of red areas active if necessary. The government postponed the reduction of containment measures due to the opposition of the scientific community, which suggested an extension of the lockdown until May. In the same period, the government set up an after-emergency commission, effectively creating an additional body to gather the requests of the various stakeholders. Subsequently, the demands of the economic world prevailed, vetoing the continuation of the lockdown.
The Spanish Premier firmly maintained the closure of the borders until 1 July (then set for 22 June for EU members), even though this would impose irreversible damage to tourism. This decision lagged three weeks behind that of Italy, which was next in the world ranking for attracting tourists. The government planned to reopen the economy and follow de-escalation according to a preset plan established by government experts. The government negotiated the de-escalation phase with the regional authorities based on scientific evidence and testing capacity. However, given the fragile majority in Parliament supporting the declaration of the state of alarm, the central government had to sacrifice some decision-making power to reopen the economy on behalf of the regions in the final stage.
In Italy, the economic power put pressure on easing the lockdown without the existence of a veto point. However, in Spain, the national Parliament became the veto point that limited the goal of the national government to guide lockdown decisions by scientific evidence.
Discussion
This article has focused on the role of institutional veto points in policy decisions during transboundary crises. The main institutional instances where veto points could be located concerning the management of a pandemic may appear during the declaration of emergency, the issuance of lockdown measures, healthcare emergency and governance, and the reopening of the economy. Veto points represent formal instances in which actors may block decisions. Actors functioning as veto players are, in this context, opposing political parties, regional parties and regional authorities.
During the first three months, the Italian regions did not become effective veto players, and the central government managed to set nationwide policies without restrictions. During the veto-point situations, regional requests were uneven or discordant, and this may have favoured the unrestricted decision-making powers of the government. The regions had different claims on whether to open up the economy in terms of protecting themselves from an influx of citizens from other regions highly affected by the pandemic. In the early stages, the call for national unity by the Head of State was key in this response. The central government was made accountable for the decisions, and regional accountability was diffused.
In Spain, the veto points were influential in two intertwined areas: the relations between the executive and the legislature regarding the maintenance of the emergency rules; and the intergovernmental system. The real veto took place in the parliamentary negotiations to extend the state of alarm. Once the veto players forced the central government to share responsibility for making confinement decisions with the regions, some regional authorities backed off and asked the central government to delay the sharing of responsibilities, or played blame games (as in the region of Madrid during the October lockdown), in order to avoid rendering direct accountability. Once regional actors are made accountable, they cannot blame the central government, and it has been shown that a different government strategy earlier on could have drawn more support for nationwide strategies. The crisis has paved the way for reforms where joint collaborative governance with shared accountability can be framed for future episodes of this or other pandemics.
Due to their transversal nature across sectors and territories, pandemics require coordination from a central vantage point that entails policy capacity and shared responsibility, and safeguards territories suffering different impacts from the pandemic. Central coordination has been interpreted as the voice and ‘whip’ of government, but in multi-level polities, a more nuanced joint governance approach is needed. National and regional political elites may veto decisions for which they are not held accountable; in joint decision formulas, this blocking strategy might be minimized. In Italy, the national government does not need to negotiate its centrality to manage the system; in Spain, the central body is hollowed out given the influence of veto players in Parliament. The gradual decentralization in Spain has weakened the ability to produce a coordinated reaction to pandemics.
Another key element of pandemics is the need to set clear accountability in multilevel politics. In Italy, the primary responsibility and related accountability remained with the national government. The Spanish approach of centralized decision-making set the central government as a lightning rod of all critiques. After the first wave of the pandemic, once regions recovered full control over crisis management, they also held individual responsibility; however, they could act irresponsibly and let the central government intervene and take the blame. This shows the weakness of the system and gives room for setting up an intergovernmental agency shielded from political games that can base decisions on scientific evidence.
The veto-point framework is useful for explaining reforms in normal times but it also helps to understand policy decisions during crises. We expanded the framework from Immergut (1992) to include multi-level politics. To the role of the legislature and national parties, we added regional parties and executives as veto players that might exploit decision points. As suggested by Immergut (1992), veto players are only relevant if there are veto points. This shows that formal veto points in Spain hampered the decision-making process during the initial part of the crisis and conditioned further measures thereafter. Regional authorities and political parties have been able to exploit these veto points by reducing the power of the centre and reacting individually to the pandemic, selfishly at times. Furthermore, we enriched the theoretical framework by including the role of accountability in the response of veto players. In traditional scholarly writings on veto players, there is a debate on the role of political parties as veto players. In multi-level polities with parties that only represent the regions in national arenas, these actors must be included. However, accountability towards their constituencies is key to understanding their veto preferences.
This intersection between coordination and shared accountability in multi-level systems opens a window of opportunity for enduring institutional changes in shared governance. However, one can also be pessimistic, as shown by Blyth (2013), regarding the ability of the momentum created by transboundary crises to exert long-lasting changes.
Conclusions
After analysing the management of the COVID-19 pandemic in Italy and Spain, we conclude that regional governments and regional parties at the national level had varying degrees of relevance in vetoing central decisions at particular stages (Immergut, 1992) in multi-level polities. In Italy, the national government, backed by the constitution and the validation of Parliament, issued the main decisions. Regional leaders did not oppose the measures and could not veto them. In Spain, the central government also made decisions but it strived for the parliamentary authorization needed every two weeks to extend the lockdown. Regional and national opposition parties ruling in some regions threatened to veto national government, which might have not requested an additional lockdown period.
Both countries, through different institutional frameworks, used similar policies as their first reaction to the crisis. With different veto-point opportunities, the veto did not materialize at first because of the centrality of the time factor, the uncertainty of decision outcomes, the transboundary dimensions of the crisis and the opportunity to place all responsibility on the central government. These factors fostered similar decisions and outcomes in both countries. The pandemic, in other words, influenced the institutional arena and its veto players by establishing a new strategic context for the actions. However, given the threat of veto players in Spain, a window of opportunity has opened to change the legislation on the state of alarm and create a more effective intergovernmental governance body with the regions.
This analysis contributes to the debate on the roles of institutions in influencing decision-making processes by analysing a specific circumstance in which the existing veto points were not activated. The multi-level institutional arrangements showed a coordinated command (from the centre or jointly with the regions), and particular accountability arrangements may explain how veto players will behave at veto points, if present at all. To understand the relevance of these results, other quasi- or federal policies could be compared with the handling of a trans-regional crisis to look at where vetoes (may) take place.
Through the analysis of how the Italian and Spanish governments managed the first three months of the COVID-19 emergency in 2020, this article has tried to understand whether veto points played a role in slowing down or changing the policy response. Initially, after analysing the documentation on the decision-making processes that reconstructed the dynamics that took place between the national and regional governments, we conclude that the response of the national government was not thwarted by regions, even when there were veto points. However, veto points started to play a role in Spain even when the crisis was far from over.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.